
Abstract
Background:
The purpose of this study is to evaluate the effects of Florida lae House Bill 21 (HB21) on opioid prescribing patterns by a single orthopedic hand surgeon after outpatient hand and upper extremity surgery.
Methods:
The following variables were evaluated with retrospective chart review before and after implementation of HB21: type of opioid, number of pills, morphine milligram equivalents (MMEs), emergency department visits, and readmissions. In addition, the Florida Prescription Drug Monitoring Program (E-FORCSE [Electronic-Florida Online Reporting of Controlled Substance Evaluation]) was queried to determine the number of pills and MMEs prescribed and sold for the latter cohort. Student t tests, Fisher exact tests, and binary logistic regression were used for statistical analysis. P < .05 was considered significant.
Results:
We reviewed 231 consecutive patients who underwent hand or upper extremity surgery from July 2017 to July 2018 and 207 consecutive patients from January 2020 to January 2021. The average age was significantly different between the cohorts (48.41 vs 44.98 years, P = .025); however, there were no significant differences across other demographic variables. After controlling for age, the average number of pills prescribed per patient decreased significantly after HB21 (25.11 vs 21.6 pills, P < .001). The number of MMEs prescribed per patient decreased as well, but the decrease was not statistically significant (167.8 vs 154.1 MMEs, P = .054). There was an association between preoperative opioid prescriptions filled and prolonged opioid use (odds ratio 6.438, P = .003).
Conclusion:
Florida law HB21 resulted in significantly fewer pills prescribed per patient, suggesting that legislation likely changed prescriber behavior and/or patient demand regarding postoperative opioid prescriptions after outpatient hand and upper extremity surgery.
Introduction
The opioid epidemic has become increasingly prominent in the medical literature in recent years, with an emphasis on decreasing opioid prescriptions across all fields of medicine. Although the United States comprises just 5% of the world’s population, it accounts for nearly 80% of opioids consumed and 99% of hydrocodone use worldwide.1,2 A large percentage of opioid addiction and overdose is attributed to overprescription, with a 111% increase in opioid prescription–related overdose deaths seen from 2004 to 2008. 3 Nearly 500 000 Americans died from opioid overdose between 1999 and 2019. 4 In 2019, opioids accounted for over 70% of all drug overdose deaths in the United States. 5
Orthopedic surgeons commonly prescribe opioids for postoperative pain and may contribute to overprescription. Guy and Zhang 6 found that orthopedic surgeons accounted for the third highest opioid prescription rate per prescriber in the United States. The only specialties found to prescribe a greater amount of opioids than orthopedic surgery were pain medicine and physical medicine and rehabilitation. 6 Furthermore, Kim et al 7 reported overprescription after hand surgery, finding that as few as one-third of pills prescribed may actually be consumed. Furthermore, there are studies which suggest that opioid-based pain control may not be necessary for certain upper extremity and hand surgeries.8 -11
In 2016, the Centers for Disease Control and Prevention issued guidelines highlighting the risks associated with prescribing opioids and encouraging conservative prescribing practices. 12 Subsequently, states began enacting opioid prescribing laws (Supplemental Table 1). On July 1, 2018, Florida implemented House Bill 21 (HB21) in an attempt to reduce opioid prescriptions. This bill limits the supply of Schedule II opioids to 3 days for acute pain prescriptions, with the ability to prescribe a 7-day supply if an exception is documented. 13 Pharmacy prescription claims in the state of Florida were found to significantly decrease in both the days supply and morphine milligram equivalents (MMEs) prescribed after total hip arthroplasty, total knee arthroplasty, and reverse total shoulder arthroplasty after the implementation of HB21.14,15
The effects of HB21, however, have not specifically been studied regarding outpatient hand and upper extremity surgery. Our goal is to evaluate the effects of Florida law HB21 on opioid prescribing patterns by a single surgeon after outpatient hand and upper extremity surgery. We hypothesize that the law will be effective in decreasing the total MMEs and number of pills prescribed per patient.
Materials and Methods
Institutional review board approval was obtained. Patients who underwent outpatient hand or upper extremity surgery by one senior surgeon from July 1, 2017 to July 1, 2018 and January 1, 2020 to December 31, 2020 were eligible for inclusion. These groups each comprise 1 year of consecutive patients before and after implementation of HB21. Two hundred thirty-one consecutive patients from July 1, 2017 to July 1, 2018 and 207 consecutive patients from January 1, 2020 to December 31, 2020 were included for a total of 438 patients. The following patient populations were excluded: pregnant women, prisoners, minors, and patients incapable of giving medical consent. Opioid prescriptions were assessed with retrospective chart review. The Electronic-Florida Online Reporting of Controlled Substance Evaluation (E-FORCSE) Program was used to evaluate opioid prescriptions filled after the implementation of HB21.
The following variables were compared before and after the implementation of law HB21: type of opioid prescribed, number of pills prescribed, MMEs prescribed, unplanned emergency department visits, and unplanned readmissions. Electronic-Florida Online Reporting of Controlled Substance Evaluation was queried to determine the number of pills and MMEs of opioid prescriptions sold but was only used for the latter cohort, as E-FORCSE only contains data for the most recent 2-year period. The following information was also gathered: age, sex, body mass index (BMI), type of procedure, intraoperative and perioperative complications, prior opioid use, and history of prior orthopedic surgery. The number and dose of opioid and benzodiazepine prescriptions were recorded within the first 90 days preoperatively.
Statistical significance for age, BMI, number of pills dispensed, and MMEs was determined using an independent t test. Significance for sex, type of procedure performed, unplanned emergency department visits, unplanned readmissions, and unplanned reoperations was assessed using Fisher exact test. Associations between prolonged postoperative opioid prescriptions were assessed with binary logistic regression. For demographic variables with statistically significant differences in means across cohorts, analysis of covariance (ANCOVA) was assessed with an ANCOVA test. P < .05 was considered significant. All data were collected and stored in Microsoft Excel (Microsoft Corp, Redmond, Washington). All statistical analyses were performed in SPSS Version 28.0 (IBM Corp., Armonk, New York).
Results
There were no differences between the prelaw and postlaw groups with respect to sex (117 women and 114 men vs 112 women and 95 men, P = .503) or BMI (27.2 vs 27.0, P = .639); however, the mean age differed between the 2 cohorts (48.41 vs 44.98 years, P = .025). There were no differences in unplanned postoperative emergency department visits (3 vs 0, P = .250), hospital readmissions (6 vs 3, P = .509), or unplanned reoperations (3 vs 3, P = 1.00; Table 1).
Demographics Between Prelaw and Postlaw Cohorts.
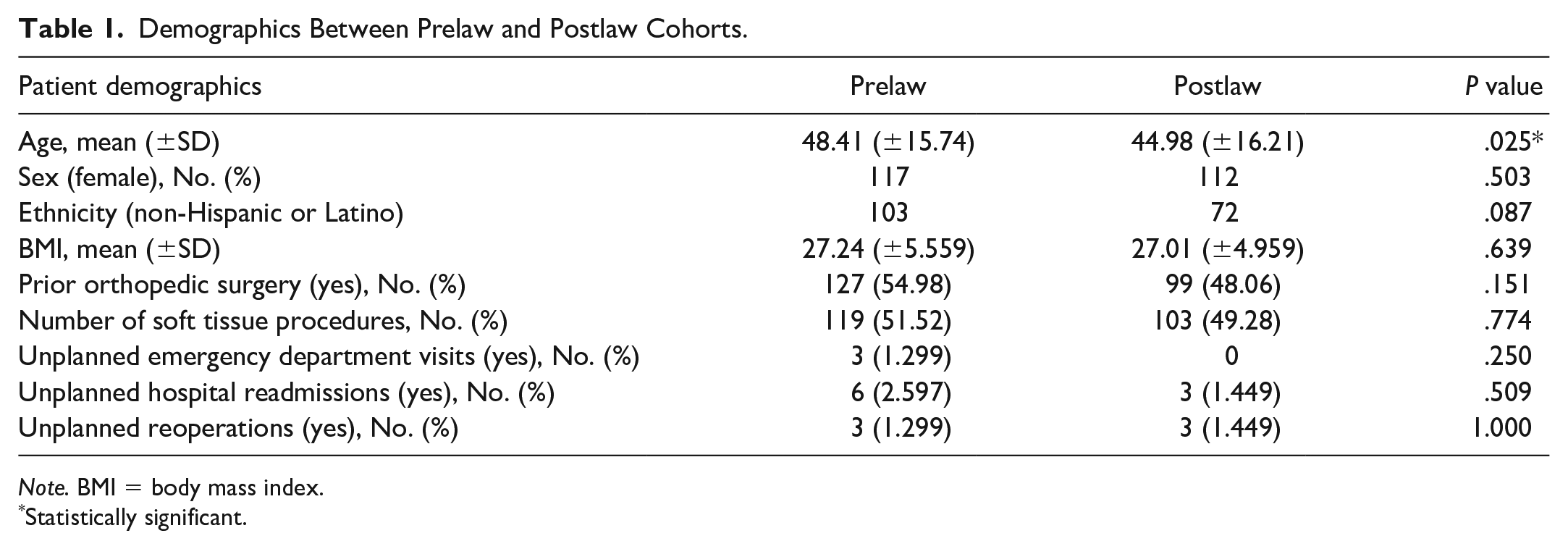
Note. BMI = body mass index.
Statistically significant.
The average number of pills prescribed per patient decreased significantly after the law (25.11 vs 21.61 pills, P < .001). The number of MMEs prescribed per patient decreased as well, but the decrease was not statistically significant (167.8 vs 154.1 MMEs, P = .111; Table 2). When controlling for age, the number of pills prescribed per patient decreased significantly (P < .001; Table 3).
Average Opioid Pill Count per Patient and MMEs Prescribed per Patient.

Note. MMEs = morphine milligram equivalents.
Statistically significant.
Average Opioid Pill Count per Patient and MMEs Prescribed per Patient Controlling for Age.

Note. MMEs = morphine milligram equivalents.
Statistically significant.
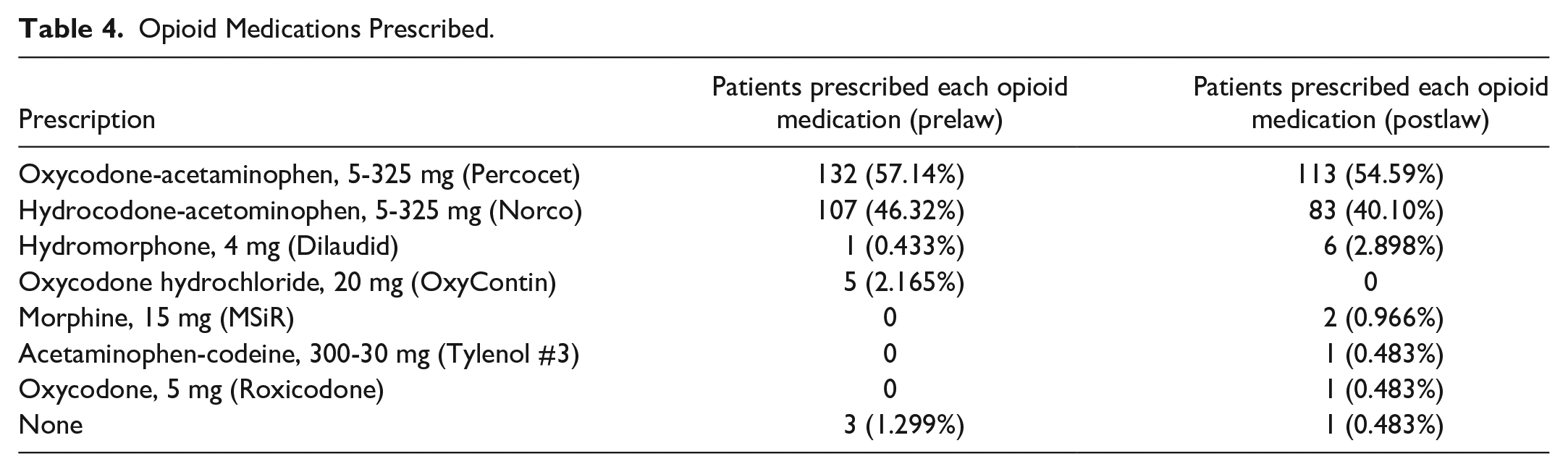
The most commonly prescribed opioids were oxycodone-acetaminophen (Percocet; n = 57.14%, 54.59%) and hydrocodone-acetaminophen (Norco; n = 46.32%, 40.10%; Table 4). There was no association between age (odds ratio [OR] = .996, P = .840), sex (OR = .824, P = .721), procedure type (OR = 1.483, P = .494), or history of prior orthopedic surgery (OR = .454, P = .164) and prolonged opioid prescription use (30-90 days postoperatively). However, there was a significant association between preoperative opioid prescriptions filled (within 30 days preoperatively, from any provider) and prolonged opioid use in the latter cohort (OR = 6.438, P = .003; Table 5).
Opioid Medications Prescribed.
Additional Postoperative Prescriptions Between 30 and 90 Days Postoperatively.
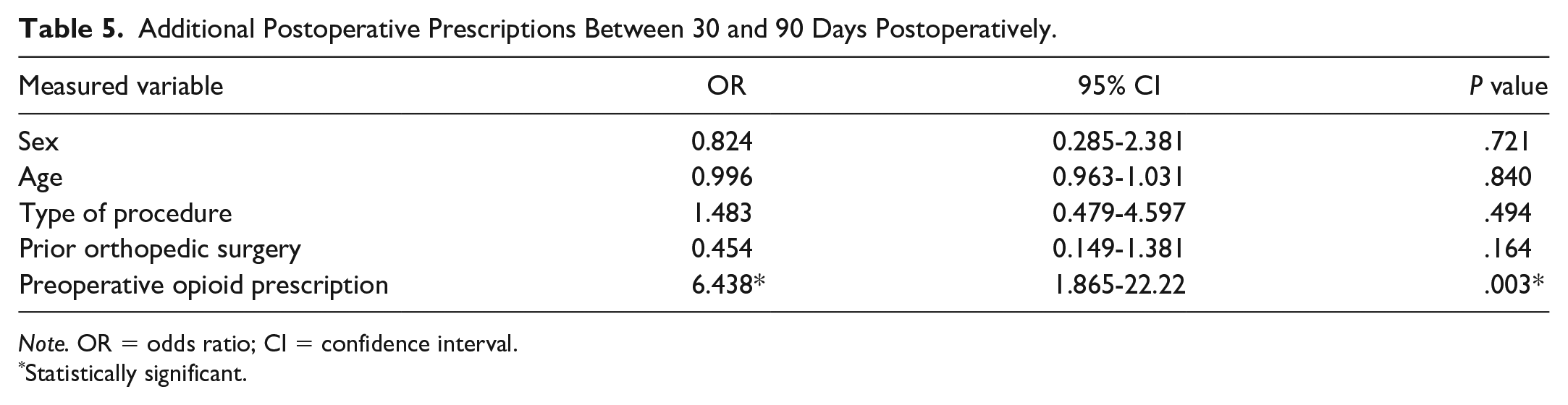
Note. OR = odds ratio; CI = confidence interval.
Statistically significant.
Using E-FORCSE data, we found 28 patients (13.52%) in the postlaw cohort received one or more additional opioid prescriptions in their first 90 days postoperatively, receiving an additional 14.19 pills and 197.82 MMEs in their first 90 days postoperatively on average. However, in the postlaw cohort, just 169 initial perioperative prescriptions (82.0%) were actually obtained by patients, indicating that at least 18% of patients did not require postoperative opioid medications. As a result, there were significantly fewer MMEs (128.8 vs 154.1, P = .006) and pills (18.17 vs 21.61, P < .001) provided to patients than were prescribed in the first postoperative prescription (Table 6).
Postlaw Opioids Prescribed Versus Sold.

Note. MMEs = morphine milligram equivalents.
Statistically significant.
Discussion
Early studies have shown Florida law HB21 to be successful in decreasing opioid prescriptions. A 2020 study performed at the University of Florida examined over 50 000 opioid prescriptions, comparing the incidence of new opioid users and mean days supply of opioids per month before and after HB21. The investigators found that the law reduced the incidence of new opioid users from 5.5 to 4.6 patients per 1000 and the mean days supply from 5.4 to 4.2 days. 16 They concluded that HB21 was successful in reducing the frequency of first-time opioid users and the average days supply of postoperative opioid prescriptions.
Opioid restriction laws have been shown to decrease opioid prescriptions within orthopedic surgery.14,15,17 Pannu et al 15 evaluated opioid prescriptions after total joint arthroplasty before and after HB21, finding a significant reduction in MMEs prescribed postoperatively from 1059.9 to 942.8 MMEs. Sabesan et al 14 assessed the effect of HB21 on opioid prescription patterns for reverse total shoulder arthroplasty, finding significant reductions in both pills (26 vs 18) and MMEs (375.6 vs 199.6) prescribed after HB21.
Although the effects of Florida’s opioid law specifically on hand surgery have not been assessed, Shah et al demonstrated that the Rhode Island Uniform Controlled Substances Act implemented in 2016 was successful in reducing pills prescribed after hand surgery, decreasing the postoperative pills prescribed per patient from 21.64 to 16.57. However, the MMEs prescribed did not significantly decrease after the law was implemented. 18 Interestingly, the Rhode Island law limited initial opioid prescriptions to 30 MMEs per day, 19 whereas Florida law HB21 limits prescriptions to a 3-day supply. 13 Although the Rhode Island law was successful in decreasing the number of pills prescribed, it did not achieve its stated goal of a significant decrease in MMEs after hand surgery.
Interestingly, we found that patients who received preoperative opioid prescriptions were 6.5 times more likely to require additional opioid prescriptions postoperatively, suggesting that careful preoperative patient evaluation and selection is important when considering which patients may be good surgical candidates.
Using E-FORCSE data, we found that just 82% of written opioid prescriptions were received by patients, indicating that some patients may not require opioid prescriptions. This is consistent with the findings of a prospective study by Moutzouros et al, 20 which concluded that 45% of patients started on a nonopioid pain protocol after orthopedic sports procedures did not require prescription opioids. Furthermore, Li et al 21 found multimodal pain control involving preemptive analgesia, peripheral nerve blockage, patient-controlled analgesia, and local infiltration analgesia to be superior to opioids alone after total knee arthroplasty. There have been prospective, randomized, double-blinded trials demonstrating that a narcotic-free pain control regimen can successfully treat patients undergoing soft tissue hand procedure surgery.22,23 Based on this, orthopedic hand surgeons may be able to further decrease postoperative opioid requirements by working with other specialists to provide multimodal pain regimens. Prior studies have shown quality improvement programs and standardized order sets to be effective in reducing MME requirements after hand surgery.24,25 Based on these findings, it may be true that evidence-based order sets may be used to supplement legislation to further decrease opioid use after hand surgery.
Despite the success of HB21 in decreasing opioid prescriptions in other fields of medicine and within some fields of orthopedics, it did not significantly reduce the MMEs prescribed per patient after hand surgery in our study. Although the reduction in MMEs was not statistically significant, we did see a reduction in MMEs prescribed that approached statistical significance when controlling for age (P = .54). These findings may be clinically relevant even though they were not statistically significant. Therefore, the law may have been successful in its political intent of decreasing the number of pills prescribed per patient. Although the law does appear to help in its stated goal and may have had a small impact, it did not lead to dramatic differences in opioid prescribing patterns.
Ultimately, although Florida law HB21 may have resulted in fewer pills prescribed per patient, it did not significantly affect MMEs prescribed, suggesting that legislation alone may not change prescriber behavior or patient demand regarding postoperative opioid prescriptions after outpatient hand and upper extremity surgery. Despite this, the decrease in MMEs seen in the present study may be clinically relevant even though it was not found to be statistically significant. Further multi-institutional studies with larger patient cohorts are required to truly determine the effects of HB21 on opioid prescribing patterns after outpatient hand and upper extremity surgery.
There are several limitations to this study, including its retrospective nature. Our study only includes a single provider and therefore our results may not be representative of all hand surgeons. In addition, our results cannot be generalized to other subspecialties or other states with different laws. Our patients were not consecutive across the entire study, as we chose to use a cohort from 2020 to use E-FORCSE data, which is only available for the most recent 2-year period at any given time. Therefore, our results may have been confounded by variables that may have influenced prescribing behavior, such as changes in physician behavior, surgical technique, or general attitudes toward pain management. Future multicenter studies with larger cohorts are needed to assess the effects of HB21 on opioid prescribing patterns in Florida after outpatient hand surgery.
Supplemental Material
sj-docx-1-han-10.1177_15589447231217763 – Supplemental material for The Impact of Florida Law HB21 on Opioid Prescribing Patterns After Outpatient Hand Surgery
Supplemental material, sj-docx-1-han-10.1177_15589447231217763 for The Impact of Florida Law HB21 on Opioid Prescribing Patterns After Outpatient Hand Surgery by Joseph S. Geller, Moses I. Markowitz, Juan J. Lizardi, Sinan K. Jabori and Seth D. Dodds in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
Institutional Review Board approval was obtained for this study.
Statement of Human and Animal Rights
This study was approved by the University of Miami’s Human Subject Research Office (approval on June 17, 2021).
Statement of Informed Consent
This study involves the retrospective review of medical records. There will be no prospective contact with potential study participants prior to acquisition of the requested data. As a result, the study team was granted waiver of consent in accordance with 45 CFR § 46.116(f)(3) and a HIPAA Waiver of Authorization in accordance with 45 CFR § 164.512(i).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.