
Abstract
Background:
The aim of this study was to validate the use of temperature sensors to accurately measure thermoplastic volar forearm splint wear in a healthy cohort of volunteers using 5- and 15-minute temperature measurement intervals.
Methods:
A prospective diagnostic study was performed to evaluate the diagnostic accuracy of temperature sensors in monitoring splint wear in 8 healthy volunteers between December 2022 and June 2023. Temperature sensors were molded into thermoplastic volar forearm splints. Volunteers who were familiar with the study aims were asked to keep an exact log of the time spent wearing the splint (“actual wear time”). Sensors recorded temperatures every 5 or 15 minutes, and separate algorithms were developed to determine the sensor-detected wear time compared with the actual wear time as the gold standard. The algorithms were then externally validated with the total population.
Results:
The 5-minute and 15-minute algorithms demonstrated excellent sensitivity (99.1% vs 96.6%), specificity (99.9% vs 99.9%), positive (99.4% vs 99.5%) and negative (99.9% vs 99.3%) predictive value, and diagnostic accuracy (99.8% vs 99.3%), respectively. The 5-minute algorithm recorded 99.5% of the total splint hours, whereas the 15-minute algorithm recorded 96.1%. There was no significant difference between the actual time per wear session (5.4 ± 2.7 hours) and the time estimated by the 5-minute algorithm (5.4 ± 2.6 hours; P = .40), but there was a significant difference for the 15-minute algorithm (5.2 ± 2.6 hours; P < .001).
Conclusion:
Temperature sensors can be used to accurately monitor thermoplastic volar forearm splint wear.
Level of Evidence:
Diagnostic II.
Introduction
Splints are commonly prescribed to patients for a variety of hand conditions as definitive conservative treatment or as an adjunct for postoperative protection. Studies have assessed the efficacy of splinting for the treatment of trigger finger,1,2 de Quervain’s tenosynovitis,3,4 carpal tunnel syndrome,5,6 and the postoperative immobilization of distal radius fractures,7 -9 among others. Studies in the hand surgery literature, however, have relied on patient-reported splint adherence rather than quantitative methods with superior accuracy.
Other areas of orthopedic surgery have demonstrated that patient-reported brace adherence is unreliable and poorly correlated with actual brace wear as measured with temperature sensors. In patients with adolescent idiopathic scoliosis, Morton et al 10 showed children and parents reported 75% adherence with bracing recommendations, whereas the actual adherence was only 47%. Sangiorgio et al 11 similarly showed parents estimated 77% adherence with idiopathic clubfoot brace wear, whereas the actual brace adherence was 62%. This difference was magnified in the oldest children, where parents overreported brace wear by 38%. In adults undergoing shoulder surgery, Grubhofer et al 12 showed patients overestimated sling use by 21%, and Weir et al 13 showed patient-reported sling wear was poorly correlated with actual sling wear (r = 0.32) with a sensitivity of 83%, specificity of 29%, positive predictive value of 50%, negative predictive value of 67%, and accuracy of 54%.
Temperature sensors have been validated to monitor scoliosis brace, 10 clubfoot brace, 11 and shoulder sling wear,12,14 but no such validation studies have been performed to monitor splint wear in hand surgery patients. These prior studies have configured the temperature sensors to record brace temperatures every 15 minutes. Given foot, torso, and shoulder braces are relatively difficult to don and doff, such monitoring intervals are likely sufficient. The splints used for hand conditions are easier to remove without assistance, potentially rendering the 15-minute temperature measurement intervals insufficient in this population. Therefore, the aim of this study was to validate the use of temperature sensors to accurately measure volar forearm thermoplastic orthosis wear in a healthy cohort of volunteers using 5- and 15-minute temperature measurement intervals. We hypothesized that temperature-based monitoring would have high diagnostic accuracy and the 5-minute temperature measurement intervals would be significantly more accurate than the 15-minute intervals.
Materials and Methods
Study Protocol
After obtaining institutional review board approval, a prospective diagnostic study was performed in 8 healthy volunteers from December 2022 to June 2023. There were 3 female and 5 male volunteers ranging from 31 to 47 years of age, with a body mass index (BMI) ranging from 23.6 to 29.3 kg/m2, and all were right-hand dominant except for one left-handed volunteer. The Onset series of temperature sensors (HOBO MX2201; Onset Computer Corporation, Bourne, Massachusetts) were molded into thermoplastic volar forearm orthoses fitted to each volunteer. All participants wore the splint on the nondominant forearm.
The thermoplastic volar forearm orthosis was fabricated by certified hand therapists by encasing the temperature sensor along the forearm belly. We felt this provided the best contact between the sensor and the skin. The wrist orthosis was placed in the orthosis pan with water heated to 60℃. Once heated to the correct temperature the orthosis was molded around the sensor. The wrist orthosis with the sensor was placed back into the pan for a short period of time and then molded to the arm. The result was a well-fit orthosis with a stable and secure sensor (Figure 1).
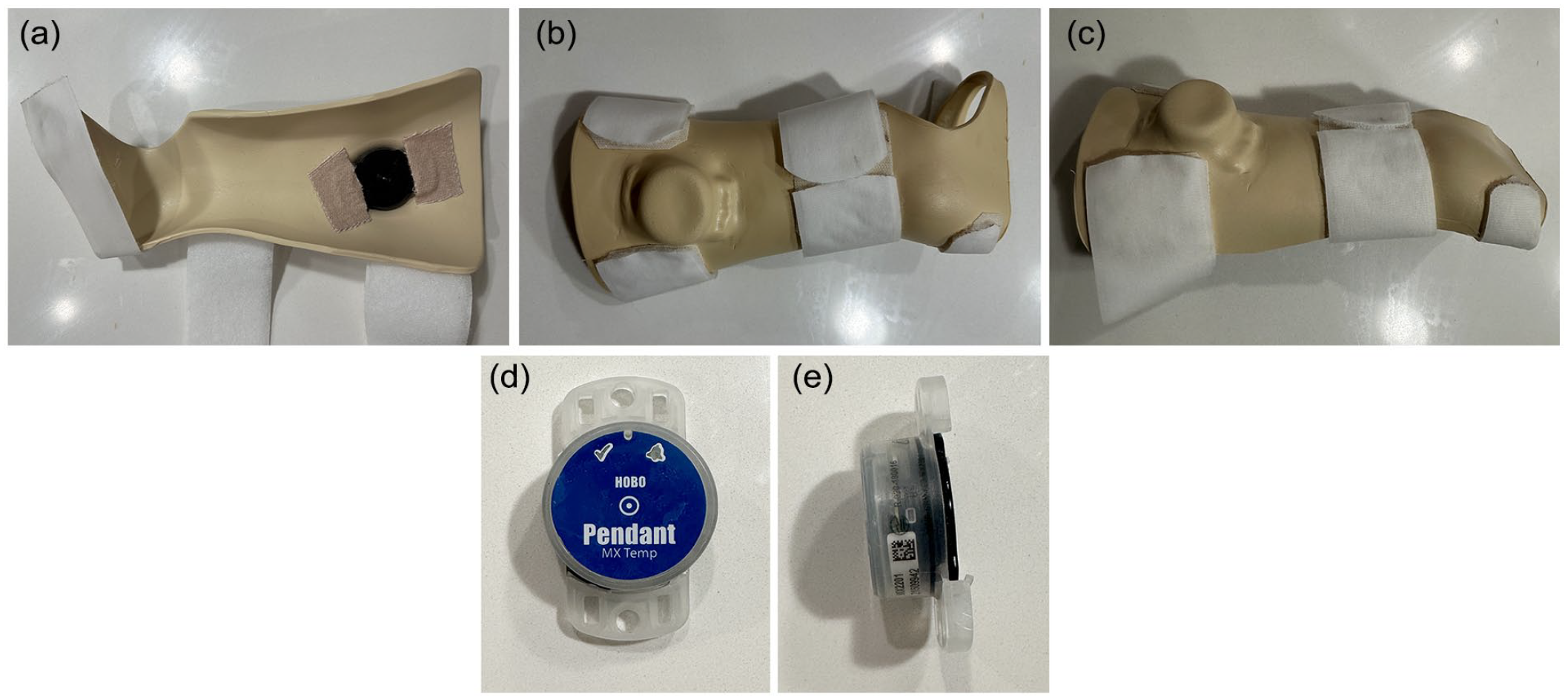
Dorsal (a), volar (b), and oblique (c) views of the volar forearm thermoplastic splint with temperature sensor embedded. Front (d) and side (e) views of the temperature sensor.
The volunteers were asked to keep an exact log of the time spent wearing the volar forearm orthosis (“actual wear time”) to act as the gold standard to validate the temperature sensors in detecting splint wear. The volunteers were informed of the aims of the study and that the most important aspect of their splint wear was the accuracy of their log rather than the amount of time spent wearing the splint. They were not instructed on how much to wear the splint to prevent bias and inflation of the splint wear logs. Volunteers were free to remove the splint throughout the day to perform daily tasks. When the splint was not in use, the volunteers were asked to store it at room temperature. This provided multiple splint “wear sessions” and their associated temperature curve variations for each volunteer, which could then be analyzed to determine the temperature sensor–detected splint wear time. Healthy volunteers were enrolled given prior literature has shown a poor correlation between patient-reported and actual brace wear for shoulder pathology, adolescent idiopathic scoliosis, and idiopathic clubfoot.10 -13,15 In addition, enrolling participants with a pathological condition requiring a splint for treatment would necessitate splint wear recommendations that could bias patient logs.
Temperature Sensors
The HOBO MX2201 (Onset Computer Corporation, Bourne, Massachusetts) temperature sensors have ±0.5℃ accuracy from −20℃ to 70℃, have dimensions of 3.35 × 5.64 × 1.8 cm, weigh 12.75 g, and are waterproof up to 30.5 m. The sensors can be configured to record temperature readings at custom intervals. For the purposes of this study, the temperature sensors were configured to record temperature readings every 5 or 15 minutes depending on the algorithm. They have a battery life of 1 to 2 years and a storage capacity of 96 000 datapoints. The temperature sensors use Bluetooth Low Energy (Bluetooth Special Interest Group, Kirkland, Washington) technology to wirelessly transfer temperature data directly to a smartphone with the HOBOconnect Monitoring Application (Onset Computer Corporation, Bourne, Massachusetts). The sensors are password protected, which limits the potential for tampering of data. 16
Algorithm Development
Two algorithms were developed to determine the sensor-detected splint wear: one based on temperature recordings every 5 minutes and one with recordings every 15 minutes. The algorithms were adapted from the study by Sood et al. 14 The 15-minute algorithm was first developed from a sample of 100.1 splint wear hours of the total population. Although it demonstrated comparable diagnostic characteristics to those previously reported, 14 we sought to improve the accuracy by increasing temperature recordings to every 5 minutes. The 5-minute algorithm was then developed from a similar sample of 100.0 hours of the total population. All 8 volunteers were included in the 15-minute algorithm, whereas 5 volunteers were included in the 5-minute algorithm. Three volunteers were excluded from the 5-minute algorithm, as the decision to pursue the 5-minute algorithm was not made until after the initial 15-minute algorithm was created. The algorithms were developed by comparing the temperature-detected splint wear hours to the gold standard temperature logs that were recorded by the volunteers. External validation was conducted by applying each algorithm to the total population to compare the actual versus temperature-detected splint wear hours. The algorithms were created using Microsoft Excel (Microsoft Corporation, Redmond, Washington).
Fifteen-Minute Algorithm
For a timepoint to be considered the start of a splint wear session, 3 criteria must be met. First, the temperature must rise to a threshold of greater than or equal to 25.6℃. Second, the temperature must increase by either (option A) greater than or equal to 1.11℃ at two consecutive timepoints before crossing the 25.6℃ threshold or (option B) the temperature must have two consecutive increases of greater than or equal to 1.67℃ and cross the greater than or equal to 25.6℃ threshold within 30 minutes. The “splint on” time for option A is the time immediately preceding the greater than or equal to 1.11℃ increase. The “splint on” time for option B is the point immediately succeeding the first greater than or equal to 1.67℃ increase. Third, the temperature must remain greater than or equal to 25.6℃ for at least 30 minutes to be considered a splint wear session.
For a timepoint to be considered the end of a splint wear session (ie, “splint off”), 3 criteria must be met. First, the timepoint must be part of an established splint wear session. Second, the timepoint must be the first of two consecutive timepoints where the temperature decreases by greater than or equal to 1.67℃. Third, the temperature must decrease to less than 25.6℃ within 30 minutes of the greater than or equal to 1.67℃ temperature decrease.
Five-Minute Algorithm
For a timepoint to be considered the start of a splint wear session, 3 criteria must be met. First, the temperature must rise to a threshold of greater than or equal to 25.6℃. Second, the temperature must increase by either (option A) greater than or equal to 0.56°C at two consecutive timepoints before crossing the 25.6℃ threshold or (option B) the temperature must have two consecutive increases of greater than or equal to 1.11℃ and cross the greater than or equal to 25.6℃ threshold within 10 minutes. The “splint on” time for option A is the time immediately preceding the greater than or equal to 0.56℃ increase. The “splint on” time for option B is the point immediately succeeding the first greater than or equal to 1.11℃ increase. Third, the temperature must remain greater than or equal to 25.6℃ for at least 10 minutes to be considered a splint wear session.
For a timepoint to be considered the end of a splint wear session (ie, “splint off”), 3 criteria must be met. First, the timepoint must be part of an established splint wear session. Second, the timepoint must be the first of two consecutive timepoints where the temperature decreases by greater than or equal to 1.11℃. Third, the temperature must decrease to less than 25.6℃ within 10 minutes of the greater than or equal to 1.11℃ temperature decrease.
Statistical Analysis
The diagnostic characteristics of the 5- and 15-minute algorithms were calculated, including the sensitivity, specificity, positive predictive value, negative predictive value, and the diagnostic accuracy. A receiver operating characteristic (ROC) curve was plotted and the area under the curve (AUC) was calculated to determine the discriminative power of the two algorithms to estimate splint wear. A perfect test has an AUC of 1.0. 17 Youden’s index was calculated to quantify the overall discriminative power of the temperature sensor algorithms. A perfect test has a Youden’s index of 1.0. 18
After the development of the 5- and 15-minute algorithms, external validity was assessed by comparing the actual and sensor-detected splint wear time for the total population. The statistician was blinded to the actual splint wear results when applying the algorithm to the temperature data to reduce the risk of bias. Descriptive statistics were used to compare actual and sensor-detected splint wear time and paired samples t tests compared the mean hours per splint wear session. Finally, the 5-minute algorithm was directly compared with the 15-minute algorithm by converting the 5-minute temperature recordings to 15-minute temperature recordings.
The sample size of 8 patients was based on prior orthopedic validation studies of brace wear which used 3 or 4 volunteers to validate the temperature sensor algorithms.10,14 The 15-minute temperature recording data yield 4 datapoints per hour, whereas the 5-minute temperature recording data yield 12 datapoints per hour. Therefore, there were 51 386 temperature datapoints for the 15-minute temperature data and 105 212 temperature datapoints for the 5-minute temperature data. Given that the minimum sample size for diagnostic studies generally ranges from 34 to 4860 tests, 19 the sample size was felt to be sufficient for analysis. A post hoc power analysis for the difference between two dependent means revealed 99.4% power was achieved for the total cohort. All statistical analyses were performed using SPSS (Version 29; IBM Corporation, Armonk, New York). Differences with P ≤ .05 were considered statistically significant.
Results
The temperature sensors recorded data for 12 847 hours for the 8 healthy volunteers. The splints were worn for 1223.7 hours (9.53%) of the total study period. Table 1 shows the diagnostic characteristics of the 5- and 15-minute interval temperature sensor algorithms. The 5-minute interval algorithm captured 99.7% of the actual splint wear, whereas the 15-minute interval algorithm captured 97.1% of the actual splint wear. Both algorithms demonstrated excellent sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy. Figures 2 and 3 show the ROC curves of the two algorithms. The algorithms demonstrated the temperature sensors were nearly perfect at detecting actual splint wear, but the AUC for the 5-minute algorithm demonstrated better sensitivity than the 15-minute algorithm.
Diagnostic Characteristics of the Temperature Sensor Algorithms.
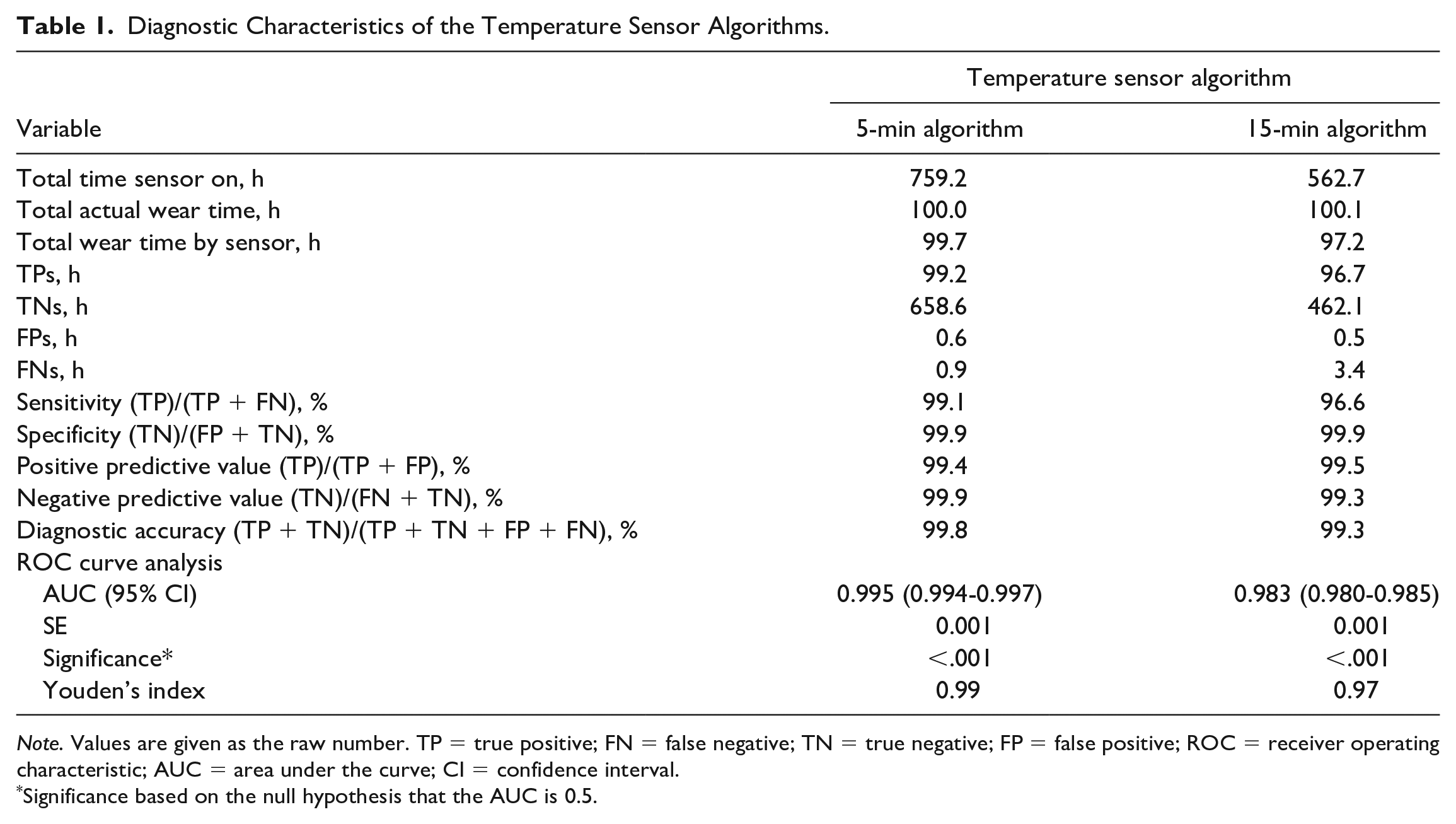
Note. Values are given as the raw number. TP = true positive; FN = false negative; TN = true negative; FP = false positive; ROC = receiver operating characteristic; AUC = area under the curve; CI = confidence interval.
Significance based on the null hypothesis that the AUC is 0.5.
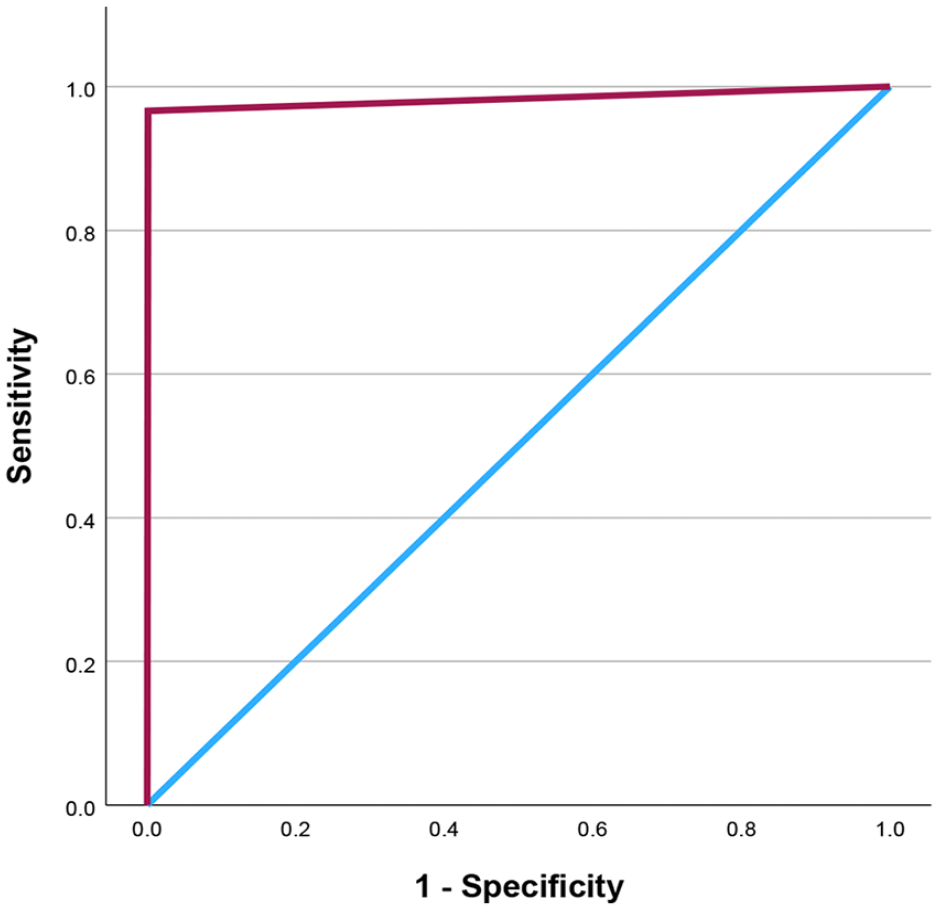
Receiver operating characteristic curve for the 15-minute algorithm. The area under the curve is 0.983.
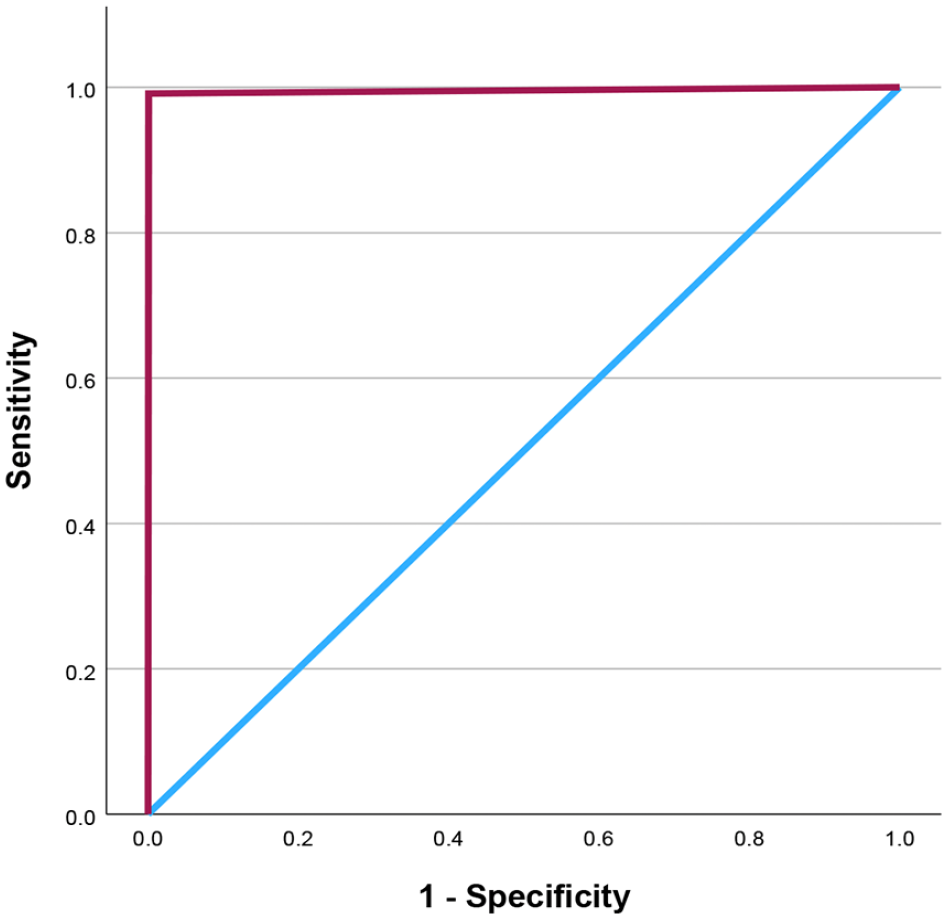
Receiver operating characteristic curve for the 5-minute algorithm. The area under the curve is 0.995.
Table 2 shows the actual and sensor-detected splint wear using the 15-minute interval algorithm. Of the 202 splint wear sessions, the temperature sensor did not detect 2 wear sessions. The missed sessions had a mean actual wear time of 0.83 hours. Of the 1223.7 hours of actual splint wear time, the temperature sensor did not detect 33.5 hours (2.7%). Among participants, the difference in sensor-detected and actual splint wear time ranged from 1.0% to 7.3% of the actual wear time. There was a significant difference between the actual and sensor-detected time per splint wear session (6.9 ± 1.0 vs 6.8 ± 0.9 hours, respectively; P < .001).
Splint Hours Using the 15-Minute Temperature Sensor Algorithm.
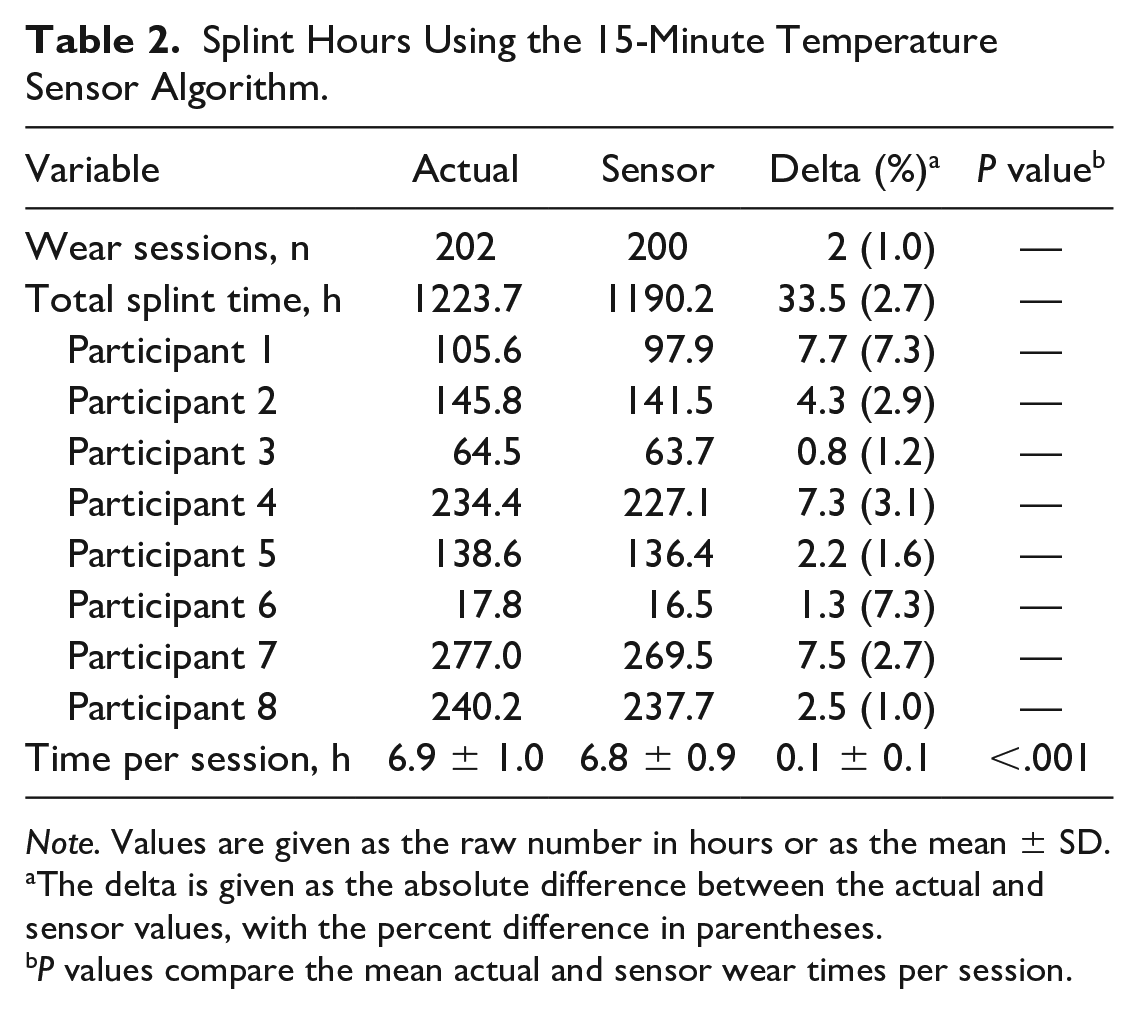
Note. Values are given as the raw number in hours or as the mean ± SD.
The delta is given as the absolute difference between the actual and sensor values, with the percent difference in parentheses.
P values compare the mean actual and sensor wear times per session.
In a matched-pairs analysis, Table 3 compares the actual and sensor-detected splint wear using both the 5- and 15-minute interval algorithms. The 5-minute algorithm detected 81 of 81 (100%) splint wear sessions, whereas the 15-minute algorithm failed to detect 1 (1.2%) splint wear session of 1.03 hours. Of the 438.2 hours of actual splint wear, the 5-minute algorithm detected 436.2 hours (99.5%), and the 15-minute algorithm detected 421.2 hours (96.1%). Among participants, the difference between sensor-detected and actual splint wear time ranged from 0.0% to 2.8% of the actual wear time for the 5-minute algorithm, and 1.2% to 7.3% for the 15-minute algorithm. There was no significant difference between the actual (5.4 ± 2.7 hours) and sensor-detected time per splint wear session for the 5-minute algorithm (5.4 ± 2.6 hours; P = .40), but the 15-minute algorithm was significantly different (5.2 ± 2.6 hours; P < .001).
Splint Hours Comparing the 5- and 15-Minute Temperature Sensor Algorithms.
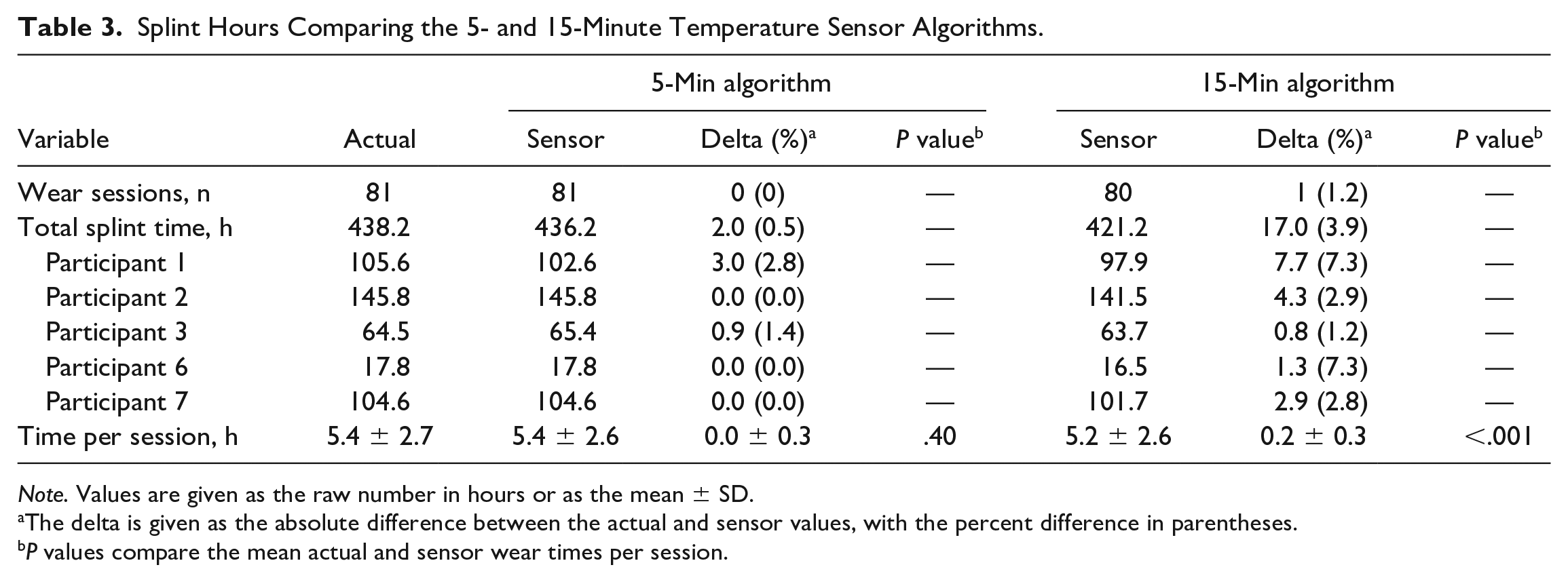
Note. Values are given as the raw number in hours or as the mean ± SD.
The delta is given as the absolute difference between the actual and sensor values, with the percent difference in parentheses.
P values compare the mean actual and sensor wear times per session.
Discussion
In a prospective cohort of healthy volunteers, this study sought to validate the use of temperature sensors to accurately monitor volar forearm thermoplastic splint wear using two algorithms. Similar to results in other areas of orthopedics,10,12,14 we showed temperature sensors demonstrate excellent diagnostic characteristics. The 5-minute algorithm minimized false-negative measurements, resulting in improved sensitivity compared with the 15-minute algorithm. With an AUC of 0.995 for the 5-minute algorithm and 0.983 for the 15-minute algorithm, both are nearly diagnostically perfect in the detection of volar forearm splint wear. This was confirmed in an external validation arm of the study where the algorithms were applied to a healthy group of volunteers. The 15-minute algorithm captured 97.3% of the actual splint wear in the total cohort. A paired comparison of the 5- and 15-minute algorithms revealed the 5-minute algorithm captured 99.5% of the actual splint wear, whereas the 15-minute algorithm captured 96.1% of the actual splint wear. These data can be used by hand surgeons and therapists to develop novel study designs to assess the efficacy of splint wear more accurately in the nonoperative and postoperative management of hand conditions.
Adherence in the hand surgery literature is almost exclusively patient-reported, which is prone to bias and poorly correlates with actual adherence.10 -13,15 In a 2023 Cochrane review of splinting for carpal tunnel syndrome, 15 of the 29 included randomized controlled trials reported splint adherence, all of which were based on retrospective questionnaires or self-reported adherence. 6 O’Brien performed a systematic review to assess therapeutic splint wear for acute upper extremity injuries. 20 Of the 6 included studies, adherence measures included failure to attend hand therapy sessions, self-reported splint wear, removal of the splint prior to the physician’s decision to discontinue treatment, and the number of self-reported splint removal instances. In one of the included studies, Sandford et al administered a self-reported questionnaire of splint adherence to 80 patients who underwent flexor or extensor tendon repairs 4 weeks prior, finding 67% reported nonadherence and 33% reported complete adherence. 21 There were 3 ruptures in the study, one of which was in a self-reported adherent patient and two in self-reported nonadherent patients. Dobbe et al performed the only study to our knowledge that uses a quantitative method of evaluating adherence in zone II flexor tendon injury patients. 22 The authors developed a device attached to a modified Kleinert splint to accurately track when patients performed exercises. 23 In a small sample of 15 patients with zone II flexor tendon injuries, the authors showed no strong correlations between the number of exercise counts per hour and the total active or passive motion at final follow-up. The device used in that study is relatively large and only records the frequency of exercises rather than quantifying the amount of splint wear time.
Multiple studies have assessed the role of splints following volar plating of distal radius fractures. Poiset et al performed a prospective cohort study of patients undergoing volar plating of distal radius fractures. 8 All patients were transitioned to a thermoplastic splint within 2 weeks postoperatively, regardless of receiving a soft dressing or plaster splint intraoperatively. Although the authors reported improved motion and patient-reported outcomes in the soft dressing group, the differences did not achieve the minimum clinically important difference. In addition, all patients received a thermoplastic splint at 2 weeks postoperatively and adherence was not reported for this presumably longer period of immobilization. Lozano-Calderón et al performed a randomized controlled trial comparing early and late motion following distal radius fracture volar plating. 9 The authors showed no significant differences between initiating motion at 2 versus 6 weeks postoperatively, but the authors did not report adherence to the thermoplastic volar splint wear postoperatively. Other trials of splinting after distal radius fracture fixation also fail to report adherence to the splint protocol. 24 The use of temperature sensors to accurately monitor splint wear following distal radius fracture fixation would provide valuable information to surgeons and therapists to understand how much time patients spend in their splints postoperatively and whether this is linked to outcomes.
The use of temperature sensors to accurately monitor brace wear has led to significant findings in other orthopedic fields. In patients with adolescent idiopathic scoliosis, Katz et al showed that brace wear of more than 12 hours per day was significantly associated with the prevention of curve progression. 15 In bracing for idiopathic clubfoot patients, Sangiorgio et al also showed increased brace wear is associated with a lower risk of relapse of deformity. 11 In patients undergoing rotator cuff repair, Grubhofer et al 25 showed that patients with less than 60% sling compliance had a 13-fold increased risk of rotator cuff repair failure at 1 year postoperatively. Similarly, Weir et al 13 showed increased sling wear was associated with female sex and a lower BMI following shoulder surgery. Patients with increased sling wear had better early pain scores and fewer image-based failures at 6 weeks and 1 year postoperatively. Finally, Livesey et al 26 showed patients were more likely to wear a shoulder sling postoperatively if they had a better understanding of the sling’s purpose (ie, to protect the shoulder repair) and had assistance at home. Given the multiple studies that have used temperature sensors to better understand the influence of postoperative bracing, applying this technology to patients with hand conditions is a logical next step that will pave the way for impactful studies in the future.
This study had multiple limitations. First, the study assessed splint wear in healthy volunteers rather than patients with pathological hand conditions. Splint wear sessions occurred at the convenience of each volunteer rather than as a prescribed amount of time per day. Volunteers understood their self-reported logs represented the gold standard to create the temperature sensor algorithms, and the most important aspect of the study was the accuracy in reporting the splint wear sessions. Second, the study included relatively few volunteers. Prior validation studies have similarly used 3 to 4 volunteers for scoliosis, clubfoot, and shoulder brace wear.10 -13 In the validation of a device to monitor flexor tendon exercises, Dobbe et al enrolled 5 healthy volunteers. 23 Despite the small number of participants, the temperature data included 202 wear sessions and 156 598 datapoints for analysis. Third, the temperature sensor algorithms have inherent limitations based on design. The 15-minute algorithm is best suited to detect wear sessions of at least 75 minutes in duration, whereas the 5-minute algorithm can detect wear sessions of 30 minutes. The 15-minute algorithm failed to record 2 wear sessions with a mean 0.83 hours of wear time, indicating shorter splint wear intervals are at risk of not being recorded. The 5-minute algorithm did not fail to record any splint wear session. Fourth, the sensors used in this study are too large to use in a hand-based splint. Other authors have used smaller sensors that could be used in hand-based splints, but these were more costly and therefore not used in the present study.12,27 The size of the sensors was not bothersome to the volunteers and did not cause any skin irritation. Although beyond the scope of the present study, the Hawthorne effect is a potential concern for the use of these temperature sensors in future studies.
Conclusion
The use of splints in patients with hand conditions is extensive and is central to the daily practice of surgeons and therapists. Despite their common prescription for a variety of conditions, no studies have been able to accurately quantify how much patients wear the splint and whether it is associated with outcomes. In this study, we showed temperature sensors have excellent diagnostic accuracy in detecting volar forearm thermoplastic splint wear in healthy volunteers. The 5-minute algorithm optimizes the sensitivity of the sensors and is recommended given the ability to detect shorter splint wear sessions that may occur if patients don and doff the splint more frequently. This study paves the way for future research using temperature sensors to accurately monitor splint wear in patients undergoing treatment for hand conditions.
Footnotes
Acknowledgements
The authors would like to thank Timothy Zerwic, Brittany Samson, and Tom Kane for their assistance and contributions to this project. The authors would also like to thank Anshum Sood for his prior work to inspire this study.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors declared research grant funding from the Hand Rehabilitation Foundation. M.N.G. declared additional grant funding for research support from Orthofix and consulting fees from Arthrex and Tigon. A.L.O. declared additional research support from Auxilium and Skeletal Dynamics; royalties from Elsevier and Skeletal Dynamics; consulting fees from AM Surgical, Arthrex, and Auxilium; paid speaking for Accumed, Arthrex, and Auxilium; and is on the editorial board of Orthopedics Today and Wrist.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was performed with the financial support of the Hand Rehabilitation Foundation, a 501(c)(3) nonprofit corporation.