
Abstract
Background:
The purpose of this study was to identify preoperative factors associated with worse postoperative Patient-Reported Outcomes Measurement Information System (PROMIS) pain interference (PI) scores 2 years after hand and wrist surgery. We hypothesized that older age, more comorbidities, increased substance use, and lower socioeconomic status would correlate with worse 2-year PROMIS PI scores.
Methods:
This study was a retrospective review of prospectively acquired data on 253 patients. Surveys were administered within 1 week of surgery and 2 years postoperatively. Bivariate and multivariable analyses were conducted to identify significant predictors of worse 2-year PROMIS PI scores and change in PROMIS PI scores.
Results:
Older age, higher body mass index, more comorbidities, lower preoperative expectations, more prior surgeries, unemployment, smoking, higher American Society of Anesthesiologists (ASA) score, and multiple other socio-demographic factors were correlated with worse 2-year PROMIS PI scores (P ≤ .018). Similar factors were also correlated with less improvement in 2-year PROMIS PI scores (P ≤ .048). Worse scores on all preoperative patient-reported outcome measures correlated with worse 2-year PROMIS PI scores (P ≤ .007). Multivariable analysis identified smoking history, less frequent alcohol consumption, worse preoperative PROMIS social satisfaction and Numeric Pain Scale whole body scores, and higher ASA scores as independent predictors of worse 2-year PROMIS PI. The same factors in addition to better baseline PROMIS PI were predictive of less improvement in 2-year PROMIS PI.
Conclusion:
Numerous preoperative factors were predictive of worse postoperative 2-year PROMIS PI and less improvement in 2-year PROMIS PI for patients undergoing hand and wrist surgery.
Introduction
As the number of hand and wrist surgeries continues to increase, especially in the elderly population, understanding which factors influence postoperative pain is crucial to optimizing treatment plans.1,2 Proper pain control is critical to help restore function and maintain patient satisfaction postoperatively. And historically, pain management has consisted of opiate medications, with orthopedic surgeons among the highest prescribers of opioids in the United States. However, more recently, alternative pain therapies with a comparable level of efficacy have been adopted to attempt to avoid the adverse effects of opioids.3 -5 Among hand surgery patients, those with greater postoperative opioid use reported higher Visual Analog Scale pain scores and lower satisfaction with pain management and surgery. 6 In addition, among opioid-naïve patients undergoing hand surgery, 13% continued to fill opioid prescriptions between 90 and 180 days after hand surgery, suggesting that pain control with alternative analgesic therapies is critical to prevent opioid use patterns preceding long-term dependence. 7
Successful pain management has been correlated with greater patient-reported outcomes after hand and wrist surgery. Adequate patient-reported analgesia has been shown to be associated with greater postoperative patient satisfaction 8 Likewise, higher postoperative physical function (PF) has been shown to be independently predictive of lower postoperative pain interference (PI) scores in patients recovering from hand surgery, suggesting that successful pain management may improve surgical outcomes.9,10 It is important to note that postoperative pain can be influenced by multiple factors that are not directly related to the procedure itself, such as mental health distress, worse general health, and socioeconomic status.11,12
Given the multidimensional nature of postoperative pain, it is imperative to use a pain scale that reflects this complexity. The Patient-Reported Outcomes Measurement Information System (PROMIS) PI item bank assesses to what extent pain hinders the patient’s social, cognitive, emotional, and physical activities.13,14 The National Institutes of Health introduced PROMIS to help standardize patient-reported outcome assessments, but there are also many other existing measures of pain, such as the Numeric Pain Scale (NPS) and the Brief Pain Inventory. 14 Unlike NPS, which is limited to a 0 to 10 scale and is rarely used for observation periods beyond 12 weeks, PROMIS PI accounts for various components of pain that correlate to overall improvement and has been validated for use in observation periods years after surgery. 15 Despite the prevalence of numerous pain measurement tools, more research is needed to better understand the factors that influence pain in hand and wrist surgery patients.
The goal of this study is to determine what modifiable and nonmodifiable preoperative patient characteristics are associated with postoperative PI among hand and wrist surgery patients. We hypothesized that older age, more comorbidities, increased substance use, and lower socioeconomic status would correlate with worse 2-year PROMIS PI scores.
Materials and Methods
This study was a retrospective review of prospectively acquired data between June 2015 and July 2018 of patients undergoing elective hand and wrist surgery by 4 surgeons. Eligible patients were consented at a single academic urban institution and enrolled in an institutional review board–approved orthopedic registry. 16 Data collected were both self-reported (demographic information, social history, surgical history) and obtained from medical records (medications, smoking status, Charlson Comorbidity Index [CCI], 17 American Society of Anesthesiologists [ASA] score, and Current Procedural Terminology [(CPT] codes). The CPT codes for each patient were confirmed from the operative notes.
Questionnaires for patient-reported outcome measures were administered electronically and collected at baseline and again 2 years postoperatively. Patients were administered with the baseline survey 1 week prior to their date of surgery and were able to complete the baseline survey up until 1 week following their surgery (in reference to their status prior to surgery). Survey data were collected and managed by REDCap. 18 Participants were administered with PROMIS Computer Adaptive Testing, 19 which consisted of the following 6 domains: PI, PF, social satisfaction (SS), fatigue, anxiety, and depression. Patient-Reported Outcomes Measurement Information System scores range from 0 to 100, with 50 ± 10 being the average score for the population. A higher PROMIS score indicates more of the measured concept. For instance, PROMIS PI measures the extent to which pain hinders the patient’s social, cognitive, emotional, and physical activities. Therefore, a higher PI score indicates a higher degree of hindrance in these activities and thus is a “worse” PI. Consequently, a negative change in PROMIS PI (calculated by subtracting the 2-year PI score by the baseline score) indicates outcome improvement. Pain was further evaluated on a standard numeric scale using the NPS 15 for the operative hand or wrist and whole body. Preoperative patient expectations were assessed with the Musculoskeletal Outcomes Data Evaluation and Management System questionnaire. 20 Physical activity level was evaluated using the Tegner Activity Scale (TAS) 21 and Marx Activity Rating Scale (MARS) for the upper extremity. 22 Hand function was assessed using the Brief Michigan Hand Questionnaire (BMHQ). 23
Deidentified data were extracted from REDCap. Each continuous variable was reported as a mean and SD. A goodness of fit test was run to assess for normality and a minority of variables were found to have a normal distribution, justifying the use of nonparametric tests. The Spearman’s rank correlation coefficient (ρ) was used to evaluate correlations between continuous variables and PROMIS PI. Each categorical variable was reported as a frequency and percentage. The Wilcoxon rank-sum test was used to compare means between 2 groups, and the Kruskal-Wallis test was used to compare means between 3 or more groups. Post hoc analysis was conducted when necessary, using the Bonferroni correction. Significant continuous and categorical variables from bivariate analysis were incorporated into a stepwise backward linear regression model to determine the independent preoperative predictors of 2-year PROMIS PI and change in PROMIS PI. All tests were 2-sided with a significance level of P less than .05. All analyses were conducted using JMP Pro (Version 13; JMP, SAS Institute Inc, Cary, North Carolina).
Results
A total of 361 patients completed baseline preoperative surveys, and 253 of these patients completed 2-year follow-up surveys (70.1% completion rate). The mean age was 50.4 ± 16.2 years. The mean preoperative PROMIS PI score was 59.1 ± 7.3. The mean 2-year PROMIS PI score improved to 50.7 ± 10.0 (P <.001). The mean change in PROMIS PI score was −8.4 ± 10.6.
The 5 most common CPT codes for this cohort are listed in Table 1. There was a statistically significant difference among CPT codes in 2-year PROMIS PI scores (P = .001). Post hoc analysis clarified that the CPT codes 64721 (carpal tunnel release) and 26055 (trigger finger release) were associated with the worst 2-year PROMIS PI scores. Likewise, there was a statistically significant difference among CPT codes in change in PROMIS PI scores (P = .002). Post hoc analysis clarified that 25607 (open treatment of distal radial extra-articular fracture with internal fixation) was associated with the greatest PROMIS PI improvement.
Top 5 All CPT Codes.
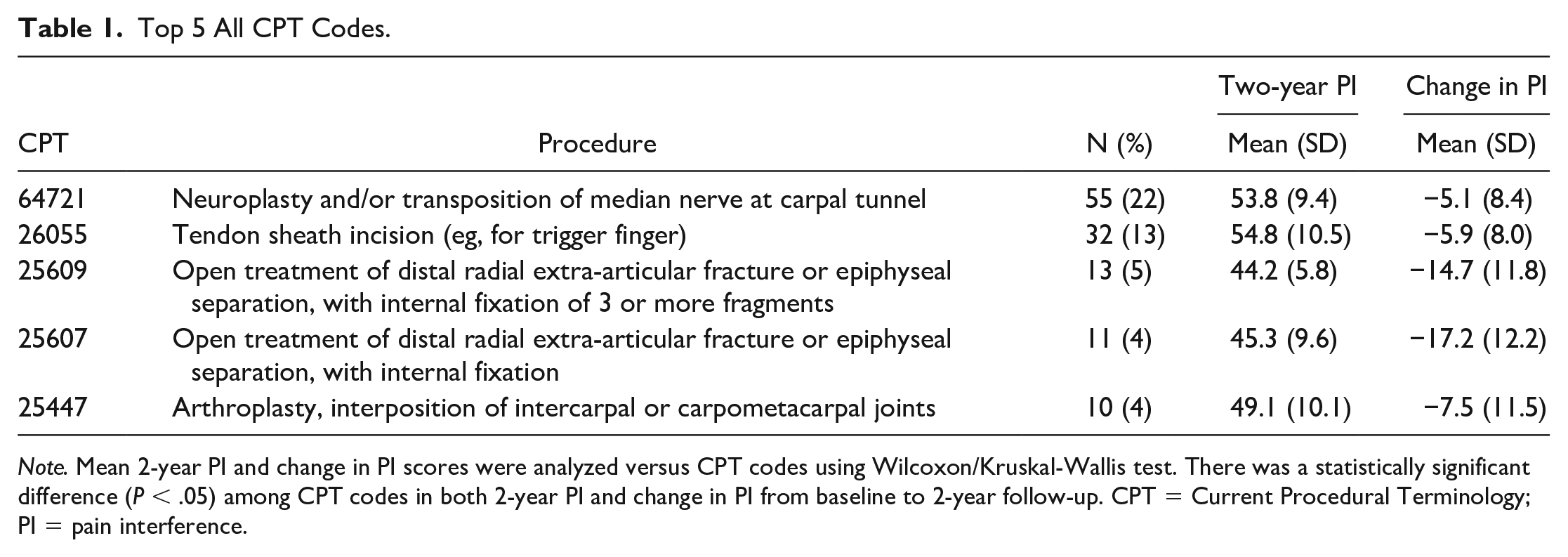
Note. Mean 2-year PI and change in PI scores were analyzed versus CPT codes using Wilcoxon/Kruskal-Wallis test. There was a statistically significant difference (P < .05) among CPT codes in both 2-year PI and change in PI from baseline to 2-year follow-up. CPT = Current Procedural Terminology; PI = pain interference.
Preoperative continuous variables were correlated with 2-year and change in PROMIS PI scores (Table 2). The following factors were found to be significantly correlated with worse 2-year PROMIS PI scores: older age, higher body mass index, higher CCI, lower preoperative expectations, and more previous orthopedic and general surgeries. These same factors were significantly correlated with less improvement in PROMIS PI scores.
PROMIS Pain Interference by Continuous Variables.
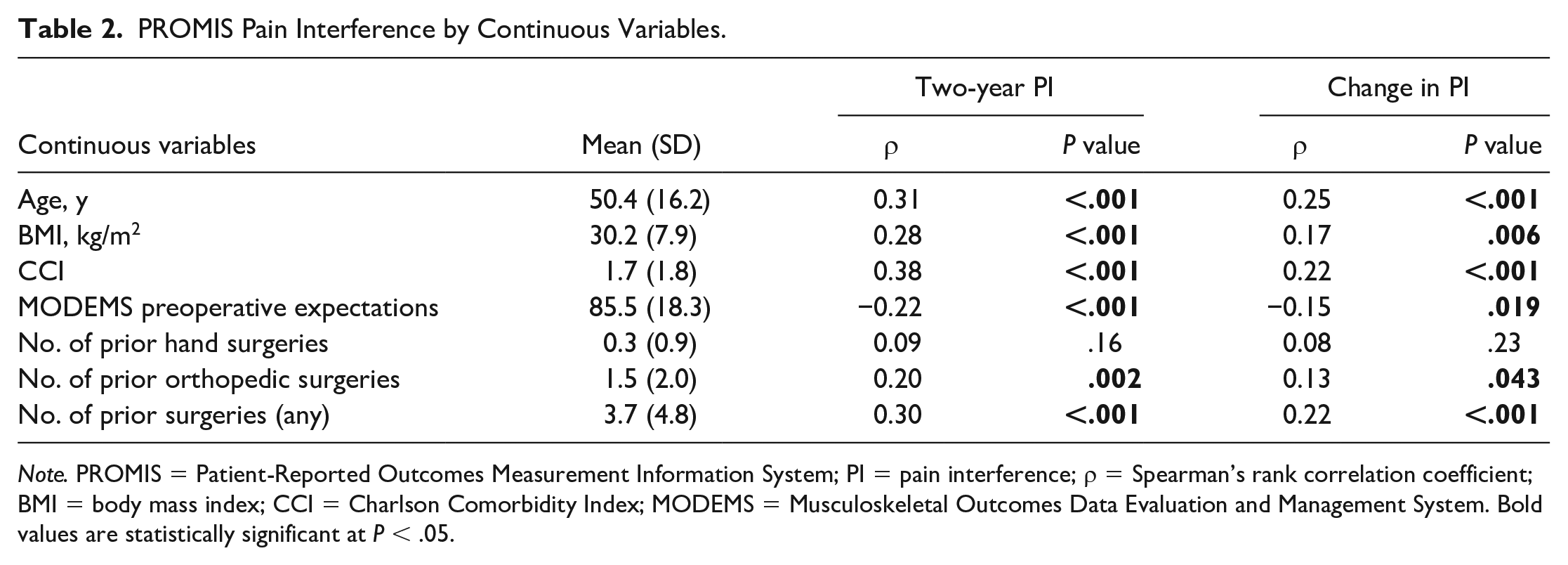
Note. PROMIS = Patient-Reported Outcomes Measurement Information System; PI = pain interference; ρ = Spearman’s rank correlation coefficient; BMI = body mass index; CCI = Charlson Comorbidity Index; MODEMS = Musculoskeletal Outcomes Data Evaluation and Management System. Bold values are statistically significant at P < .05.
Preoperative categorical variables correlated with 2-year and change in PROMIS PI scores are shown in Table 3. The following demographic/social factors were found to be significantly correlated with worse 2-year PROMIS PI scores: female sex, black race, education less than college degree, unemployment, lower income (<$70 000), presence of a legal claim, and government-sponsored insurance (P ≤ .018). The following clinical factors were also found to be significantly correlated with worse 2-year PROMIS PI scores: absence of injury leading to surgery, smoking, less frequent alcohol consumption, history of depression or anxiety, and a higher ASA score (P ≤ .011). The following factors were associated with less improvement in PROMIS PI from baseline to 2-year follow-up after surgery: black race, unemployment, presence of a legal claim, government-sponsored insurance, a workers’ compensation claim, absence of injury leading to surgery, smoking, less frequent alcohol consumption, and a higher ASA score (P ≤ .048).
PROMIS Pain Interference by Categorical Variables.
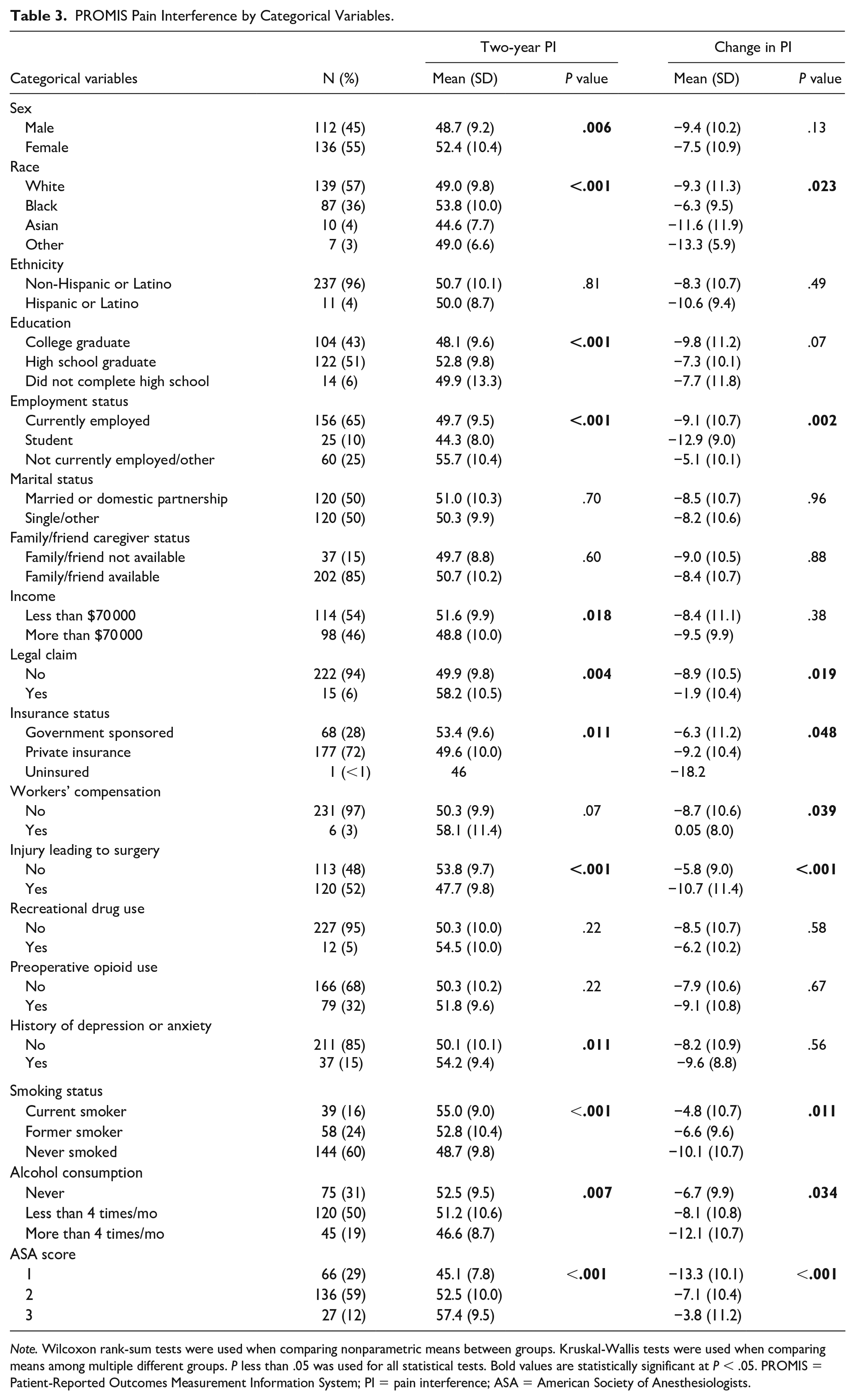
Note. Wilcoxon rank-sum tests were used when comparing nonparametric means between groups. Kruskal-Wallis tests were used when comparing means among multiple different groups. P less than .05 was used for all statistical tests. Bold values are statistically significant at P < .05. PROMIS = Patient-Reported Outcomes Measurement Information System; PI = pain interference; ASA = American Society of Anesthesiologists.
Preoperative patient-reported outcome measures correlated with 2-year and change from baseline PROMIS PI scores are presented in Table 4. Worse overall 2-year PROMIS PI scores were significantly correlated with worse scores on all preoperative measures (P ≤ .007). Less improvement from baseline at 2 years in PROMIS PI was significantly correlated with better preoperative PROMIS PI, PROMIS SS, and BMHQ scores and worse preoperative MARS and NPS whole body scores (P ≤ .048).
Preoperative Patient-Reported Outcomes Correlated to 2-Year and Change in PROMIS Pain Interference.
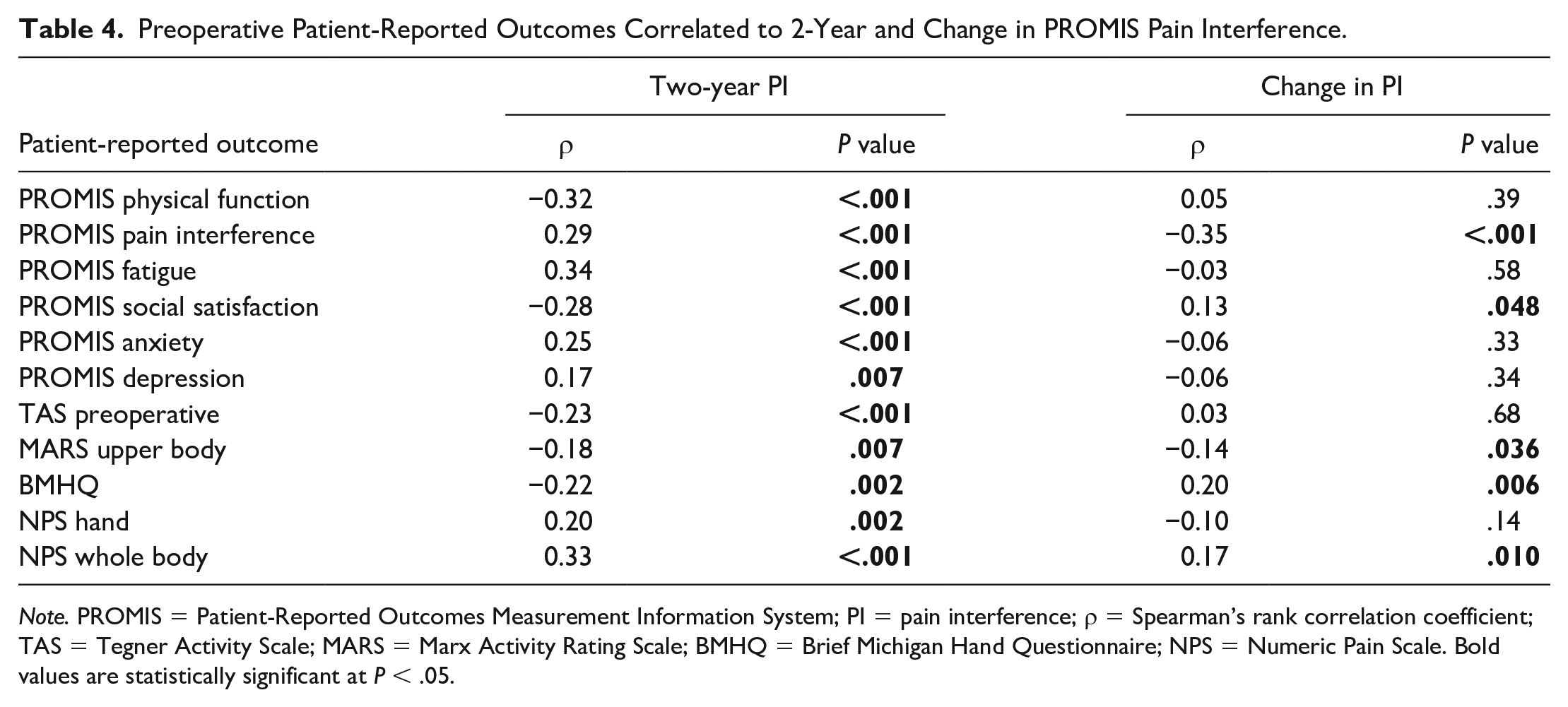
Note. PROMIS = Patient-Reported Outcomes Measurement Information System; PI = pain interference; ρ = Spearman’s rank correlation coefficient; TAS = Tegner Activity Scale; MARS = Marx Activity Rating Scale; BMHQ = Brief Michigan Hand Questionnaire; NPS = Numeric Pain Scale. Bold values are statistically significant at P < .05.
The multivariable analysis confirmed smoking history (P = .026), less frequent alcohol consumption (P = .002), worse preoperative PROMIS SS (P < .001) and NPS whole body scores (P < .001), and higher ASA scores (P < .001) as independent predictors of worse overall 2-year PROMIS PI scores (Table 5). This model accounted for 30% of the variance in 2-year PROMIS PI scores. In addition, multivariable analysis confirmed current smoking (P = .026), less frequent alcohol consumption (P = .003), worse preoperative PROMIS SS scores (P = .010), worse preoperative NPS whole body scores (P < .001), better preoperative PROMIS PI scores (P < .001), and higher ASA scores (P < .001) as independent predictors of less improvement from baseline in 2-year PROMIS PI scores in Table 6. This model accounted for 41% of the variance in change in PROMIS PI scores from baseline to 2 years.
Multivariable Linear Regression Model of Independent Predictors of 2-Year PROMIS Pain Interference.
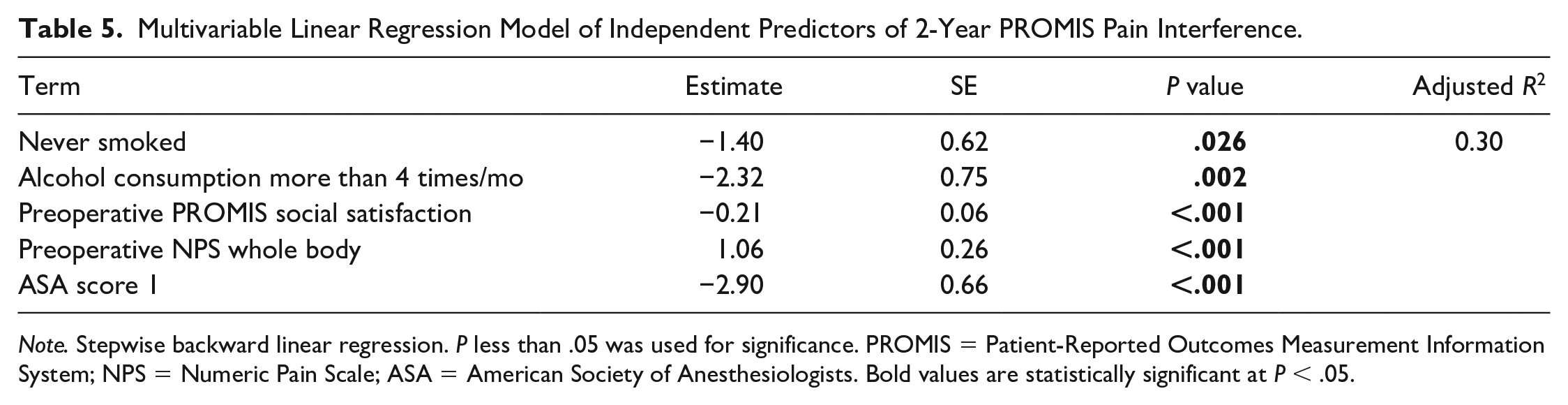
Note. Stepwise backward linear regression. P less than .05 was used for significance. PROMIS = Patient-Reported Outcomes Measurement Information System; NPS = Numeric Pain Scale; ASA = American Society of Anesthesiologists. Bold values are statistically significant at P < .05.
Multivariable Linear Regression Model of Independent Predictors of Change in PROMIS Pain Interference.
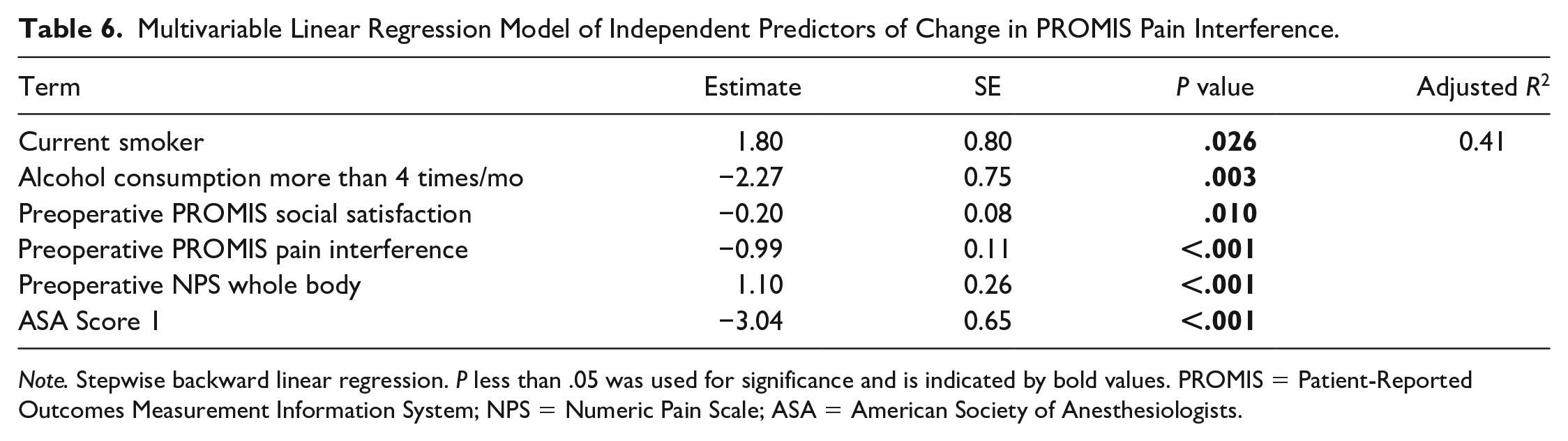
Note. Stepwise backward linear regression. P less than .05 was used for significance and is indicated by bold values. PROMIS = Patient-Reported Outcomes Measurement Information System; NPS = Numeric Pain Scale; ASA = American Society of Anesthesiologists.
When also including CPT codes as part of the multivariate analyses, smoking history (P = .0008) and preoperative NPS whole body (P < .0001) both remained as predictors of 2-year PROMIS PI scores, in addition to CPT codes 25609, 25607, and 25447 (Table 7). Similarly, smoking (P = .004), higher preoperative NPS whole body scores (P < .0001), and better preoperative PROMIS PI scores (P < .0001) remained predictors of less improvement from baseline in PROMIS PI at 2 years postoperatively, in addition to CPT codes 25609 and 25607 (both open reduction and internal fixation of distal radius fractures; P = .0006; Table 7).
Multivariable Linear Regression Model of Independent Predictors of 2-Year and Change in PROMIS Pain Interference (With CPT Codes).
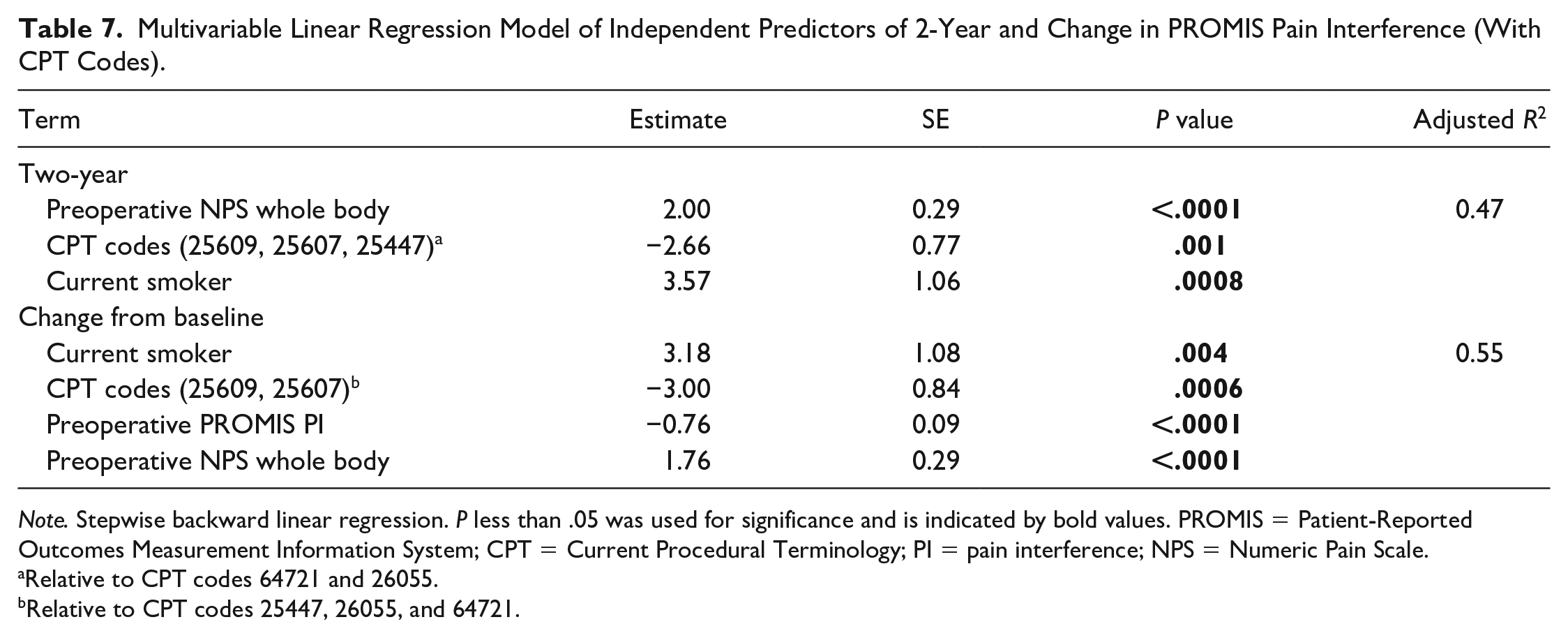
Note. Stepwise backward linear regression. P less than .05 was used for significance and is indicated by bold values. PROMIS = Patient-Reported Outcomes Measurement Information System; CPT = Current Procedural Terminology; PI = pain interference; NPS = Numeric Pain Scale.
Relative to CPT codes 64721 and 26055.
Relative to CPT codes 25447, 26055, and 64721.
Discussion
Adequate pain management is a vital aspect of patients’ recovery from hand and wrist surgery. Preoperative PROMIS PI scores have been shown to be predictive of postoperative PROMIS PI scores following hand surgery, 24 but the factors that underlie this relationship are poorly understood. A better understanding of both the modifiable and nonmodifiable preoperative factors that correlate with postoperative pain can help providers to optimize expectations and recovery outcomes following hand and wrist surgery. Here we demonstrated that numerous clinical, socio-demographic, and patient-reported outcome measures such as older age, higher CCI, smoking history, lower socioeconomic metrics, lower preoperative SS, and higher preoperative pain were all associated with worse 2-year PROMIS PI, thus supporting our hypothesis.
It is important to note that the 2-year scores and improvement in PROMIS PI for distal radial fractures were significantly better compared with carpal tunnel release and trigger finger release. Generally, internal fixation leads to immediate and sustained relief as well as a high rate of restoration of PF. 25 The other 2 procedures, although highly successful, can have variable recovery timelines based on individual factors such as occupation and preoperative functional status.26,27 This may explain why patients who underwent distal radius fracture fixation had better 2-year PI scores and more improvement in PI scores compared with the other procedure types. However, despite this difference, all 5 of the most common procedures demonstrated a decrease in PROMIS PI after 2 years, which underscores the success of hand and wrist operations in improving pain. 28
Our findings for various demographic and clinical factors associated with 2-year PROMIS PI for hand and wrist surgery patients were consistent with studies in other patient populations. Hernández et al 29 demonstrated a strong association between worse postoperative pain and female sex, low socioeconomic status, worse preoperative pain, more comorbidities, poorer baseline functional status, and greater preoperative anxiety and depression in knee or hip arthroplasty patients. Similarly, Ip et al 30 found worse preoperative pain, anxiety, and older age to be associated with worse postoperative pain in a mixed subspecialty surgical patient population. In addition, lower scores in baseline function (PROMIS PF, TAS, BMHQ, and MARS) were associated with worse 2-year PROMIS PI scores. This finding further strengthens the link between preoperative functional status and postoperative PI.10,29
Anxiety and depression have also been shown to be commonly associated with worse postoperative pain in the literature.29 -34 In our study, we found that a clinical history of depression and anxiety as well as worse preoperative PROMIS anxiety and depression scores were all significantly correlated with worse 2-year PROMIS PI. Crijns et al 10 have previously reported that better PROMIS depression scores are independently associated with higher postoperative PROMIS PF scores 1 month after hand surgery. The results of our study expand on this idea in 2 ways. First, psychiatric comorbidities are associated not only with worse postoperative PROMIS PF, but also with worse PROMIS PI. Second, our follow-up period of 2 years is substantially longer than the previous study’s 1-month follow-up, which suggests that the debilitating effects of psychiatric comorbidities on postoperative outcomes in hand and wrist surgery patients persist long after surgery and may benefit from perioperative intervention.
Preoperative opioid use was not shown to be a predictor of worse postoperative pain, despite some evidence of this relationship in various patient populations.4,5 This could be attributed to an effective transition from preoperative opioid use to over-the-counter analgesics for pain management in a significant number of patients in this study. 35 Nevertheless, further investigation is needed on opioid use as a predictor of pain specifically in hand and wrist surgery patients. Another somewhat unexpected finding was that absence of an injury leading to surgery was associated with worse 2-year PROMIS PI and less improvement in PROMIS PI. This may be because non-injury-related conditions requiring surgery tend to be long term and degenerative in nature, whereas an acute injury that requires surgery is more likely to result in a return to preinjury pain levels postoperatively. However, further research is needed on this topic.
Never having smoked was determined to an independent predictor of better 2-year PROMIS PI, consistent with the literature. 32 Interestingly, smoking preoperatively was predictive of less improvement in 2-year PROMIS PI, which highlights the importance of quitting smoking prior to a hand or wrist operation. This trend persists even when accounting for the CPT code for the procedure in which the patients underwent. This emphasizes the utility of preoperative counseling by providers on smoking cessation and could potentially incentivize patients to quit. Alcohol consumption more than 4 times a month was a predictor of better 2-year PROMIS PI and greater improvement in PROMIS PI. Alcohol consumption has been well established as an effective short-term analgesic, but its long-term analgesic effects warrant further study. 36 Furthermore, withdrawal from long-term alcohol use has been shown to increase pain sensitivity, which might motivate patients to continue drinking or increase consumption to reverse this effect, perhaps leading to better 2-year PROMIS PI scores. 37
Worse preoperative PROMIS SS was a predictor of both a worse 2-year and improvement in PROMIS PI. This reciprocal association is well established: Uncontrolled pain has been shown to have undesirable physiologic and psychological outcomes, such as reduced postoperative patient satisfaction. 38 Our study contributes to the literature by demonstrating that preoperative SS may predict both the severity and degree of improvement of postoperative PI. A lower ASA score, which is an indicator of overall physical health, was also a predictor of better 2-year PROMIS PI scores. Patients with better preoperative health status have been shown to have better recovery outcomes and more effective pain management. 39 This is an expected finding given that we hypothesized those with more comorbidities to have worse 2-year PROMIS PI. This was further reinforced by the association between a greater CCI (more comorbidities) and worse 2-year PROMIS PI.
Finally, the literature has demonstrated an association between worse preoperative pain and worse postoperative pain.24,29 In our model, we see a similar association with preoperative NPS whole body and 2-year PROMIS PI. Multivariable analysis demonstrated that a worse preoperative NPS whole body was an independent predictor of a worse 2-year PROMIS PI score even when accounting for the specific type of procedures patients underwent. However, worse preoperative NPS whole body scores and better preoperative PROMIS PI scores were both independent predictors of less improvement in PROMIS 2-year PI. This could be attributed to the difference in scales: NPS whole body simply asks patient to rate their whole body pain on a scale from 0 to 10, whereas PROMIS PI considers the extent to which pain hinders the patient’s social, cognitive, emotional, and physical activities.14,15 Nadarajah et al 40 concluded that the strong association noted between PROMIS PI and psychosocial and behavior factors compared with NPS makes it a more fitting choice for surgeons who are interested in measuring a patient’s improvement in functioning and decrease in the hindrance of pain following shoulder surgery. In addition, those that have been able to maintain a high level of function in all these activities prior to their surgery will most likely not see great improvement in PROMIS PI following surgery. Bernstein et al 24 found that patients that have a worse preoperative PROMIS PI have more potential for improvement in PI compared with those with less preoperative PROMIS PI, in line with these findings. Ultimately, our findings further suggest that PROMIS PI may be superior to NPS in accurately measuring how patient pain relates to function.
Nevertheless, there are limitations to this study. Despite the overall high follow-up rate, 29.9% of patients were lost to follow-up, potentially introducing a response bias. Furthermore, due to the retrospective study design, we can assume correlations between variables, but cannot infer causality. Also, although we measured and controlled for many variables, unknown patient factors may have affected our analyses. The data for this study were collected from patients at a single urban medical center, which may affect the generalizability of the results to the general population. Despite these limitations, we believe that we have presented the largest cohort of patients undergoing hand and wrist surgery in which 2-year PROMIS PI was investigated.
Conclusion
Numerous preoperative factors were predictive of worse postoperative 2-year PROMIS PI and less improvement in 2-year PROMIS PI for patients undergoing hand and wrist surgery. This information can be used by surgeons to identify and counsel patients with risk factors for worse postoperative PI as well as manage postoperative expectations.
Footnotes
Acknowledgements
J. Kathleen Tracy, PhD; Ali Aneizi, MD; Andrew G. Dubina, MD; Julio J. Jauregui, MD; Vidushan Nadarajah, MD; Patrick M.J. Sajak MD; Tina Zhang, MD; Joshua M. Abzug, MD; Ngozi M. Akabudike, MD; W. Andrew Eglseder, MD; Mohit N. Gilotra, MD; S. Ashfaq Hasan, MD; Ebrahim Paryavi, MD; Cameran I. Burt; Shaun H. Medina; Keyan Shasti; Dominic J. Ventimiglia; Alexander J. Wahl; and Michael P. Smuda for their assistance with data collection.
Ethical Approval
This study was approved by the Institutional Review Board (IRB) Committee at the University of Maryland, Baltimore (HP-00062261).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RAP—Globus Medical; royalty or licenses, consulting fee, paid presenter or speaker, stock or stock options. CGL—Synthes; consulting fee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from The James Lawrence Kernan Hospital Endowment Fund, Incorporated (BL1941007WS).