
Abstract
Background:
The scaphoid is the most commonly fractured carpal bone in children. True scaphoid fractures have proven to be difficult to diagnose, as they may not be apparent on initial imaging. Children with clinical suspicion of a scaphoid fracture may be treated with continued immobilization, even in the absence of radiographic evidence of a fracture. The purpose of this study is to identify predictors of true scaphoid fractures in children to help guide management.
Methods:
This study is a retrospective cohort study of children presenting to a tertiary pediatric hospital with hand or wrist injuries. Patients were grouped based on the presence of a true scaphoid fractures (confirmed on imaging) or those with clinical suspicion of a scaphoid fracture alone (no radiographic evidence of fracture). Demographic and clinical characteristics were compared with univariate and multivariate statistics to identify fracture predictors.
Results:
One hundred and thirty patients were included in the study: 57 in the true scaphoid fracture group and 73 in the clinical scaphoid fracture group. Patients with a true scaphoid fracture were older than those with a clinical scaphoid fracture (median age [interquartile range], 14.2 [13.0-15.4] vs 12.9 [11.9-14.4], P = .01). Men were more likely to sustain a true scaphoid fracture (65.0% vs 35.0%, P = .01). Older age and male sex were shown to be independent predictors of true scaphoid fractures (odds ratio [95% confidence interval], 1.25 [1.03-1.50] and 2.93 [1.39-6.17], respectively).
Conclusions:
In the pediatric population, older age and male children may be at increased risk of true scaphoid fractures. This may help guide decisions surrounding further imaging and treatment.
Introduction
As initial radiographs may miss 12% to 37% of scaphoid fractures, it has been recommended that patients are immobilized, and radiographs are repeated 7 to 14 days following injury.1,2 We previously demonstrated that even following repeat radiographs, 5% of scaphoid fractures may remain occult. 3 Missed fractures of the scaphoid may lead to nonunion, avascular necrosis, and long-term morbidity. 4 The management of patients with persistent symptoms worrisome for a scaphoid fracture but negative radiographs remains controversial.
Traditionally, these patients were treated with continued immobilization until symptoms resolve or a fracture is identified on subsequent serial radiographs. Although this ensures that no fracture is missed, a significant majority of patients may be overtreated with unnecessary immobilization, follow-up visits, and radiographs. 3 Alternatively, advanced imaging such as magnetic resonance imaging (MRI) and computed tomographic (CT) scans may enable earlier confirmation of the presence or absence of a fracture with high sensitivity and specificity. Cost-effectiveness of early advanced imaging, however, has not been demonstrated in children.
Due to costs, availability, and the lower prevalence of scaphoid fracture in children, it may not be practical to perform advanced imaging for all children presenting with a suspected scaphoid fracture. Identifying a subset of patients that would benefit from advanced imaging would be advantageous. The purpose of this study, consequently, was to identify predictors of true scaphoid fractures in children.
Materials and Methods
Study Design and Procedures
A retrospective cohort study of children with suspected and confirmed scaphoid fractures was conducted. Electronic medical records for all patients assessed in the Orthopedic and Plastic Surgery clinic at a single tertiary pediatric center were reviewed. Patients with a diagnosis of scaphoid fracture or hand or wrist pain or sprain between August 2015 and August 2017 were identified using the International Classification of Diseases, 10th Revision codes (Supplemental Material). Nonspecific hand and wrist pain and sprain codes were included to keep inclusion criteria broad, as there is no specific diagnostic code for a “suspected” or “clinical” scaphoid fracture. Patients were excluded if they presented subacutely (>6 weeks following injury), if they were more than 18 years of age at the time of presentation, or if they had another type of hand or wrist injury in the absence of a scaphoid fracture (eg, radius fracture, ulna fracture, triangular fibrocartilage complex, thumb injury, other carpal fracture, finger or thumb injury).
The medical records and imaging of identified patients were reviewed. Information was extracted by reviewing all records in the hospital’s electronic medical record, including the emergency department, clinic, surgical, laboratory, and radiologic reports. Demographic data, injury specifics, investigations, treatment, fracture characteristics (where appropriate), and outcomes were recorded.
Patients were classified as a true scaphoid fracture if they had a scaphoid fracture confirmed on any imaging modality (eg, radiograph, CT, MRI) at any time point during their care. If there was discordance between surgeon and radiologist interpretations of radiographs, a patient was considered to have a true fracture if both the radiologist and surgeon identified a fracture on imaging, or if one reported a fracture and the other reported a suspected fracture. If both the radiologist and surgeon reported the radiograph as suspicious for a fracture, it was not considered a true scaphoid fracture. If either the radiologist or surgeon reported a true fracture and the other reported no fracture, it was recorded as a conflict. Patients were diagnosed with a clinical scaphoid fracture if their imaging at all time points was negative for scaphoid fracture postinjury, but clinical suspicion of a scaphoid fracture remained.
Statistical Analysis
Descriptive statistics were performed. Mann-Whitney U test was used to descriptively compare between continuous variables and Fisher’s test for categorical variables. To assess the association of age, sex, and side of injury with the diagnosis of true scaphoid fracture, a univariate and multivariable logistic regression was used. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Two-sided P value less than .05 was considered statistically significant. All statistical analyses were carried out using R statistical language (Version 4.0.5; Reference: R Core Team [2021]. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/).
Results
One hundred and thirty pediatric patients were identified. Fifty-seven patients had a true scaphoid fracture confirmed by imaging, whereas 73 were diagnosed as a clinical scaphoid with no evidence of fracture on imaging. The majority of the 57 true fractures were confirmed on initial radiograph, except for 19 patients (33%). Five of the 19 patients had confirmed scaphoid fractures on subsequent radiograph (7, 11, 14, 21, 25 days postinjury, respectively), and the remaining 14 patients were diagnosed on advanced imaging.
True scaphoid fractures were located either at the distal pole (47%) or at the waist (47%) of the scaphoid. The remaining 6% were at the proximal pole of the scaphoid. Sixteen percent (9/57) of true fractures had displacement reported on imaging. Eighty-two percent (47/57) had open radial physes. Ninety-three percent (53/57) of these patients were treated with immobilization. The remaining 2 patients underwent surgical reduction and internal fixation (3.0%). There were no cases of nonunion or avascular necrosis.
Patients with a true scaphoid fracture were older than those with no fracture (median age [interquartile range], 14.2 (13.0-15.4) vs 12.9 (11.9-14.4), P = .01; Table 1). Men were more likely to sustain a fracture compared with women (64% vs 35%, P = .01). Side of injury was distributed evenly in the true scaphoid fracture group (47.4% right-side injury in fractures vs 33.3% in clinical fracture, P = .15), though there was a trend toward the left wrist in the clinical scaphoid fracture group. The prevailing mechanism of injury for clinical scaphoid fracture was sports (64%), whereas for true scaphoid fracture it was falling from standing height (35.2%) followed by sports (30.8%). Mechanism of injury was not recorded in 19% of patients. Hand dominance was not routinely recorded. Clinical examination findings were also not systematically documented to a level of granularity to be useful.
Demographic Descriptive Stratified by Fracture Status.
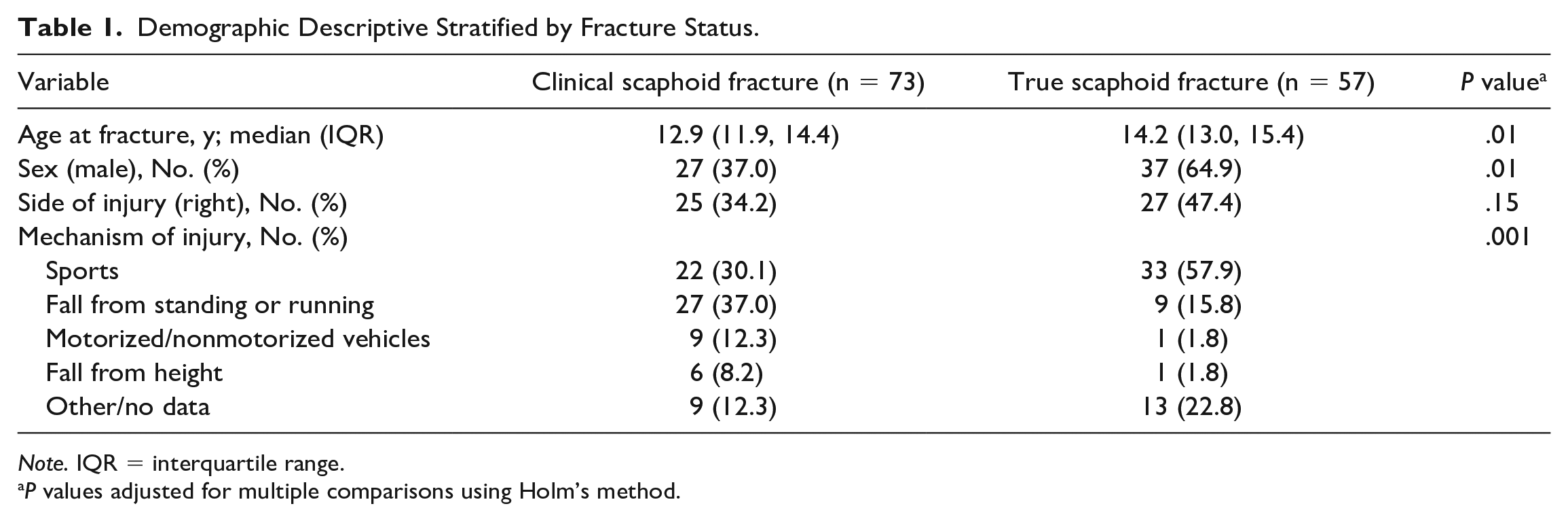
Note. IQR = interquartile range.
P values adjusted for multiple comparisons using Holm’s method.
Univariate and multivariable logistic regression modeling showed that every year increase of age is associated with an increased odds of true scaphoid fracture by 25% (adjusted OR: 1.25, 95% CI, 1.03-1.50, P = .02; Figure 1). Men had nearly triple the odds of true scaphoid fractures compared with women (adjusted OR: 2.93, 95% CI, 1.39-6.17, P = .005). Side of injury did not show any association with having a true scaphoid fracture (Table 2).
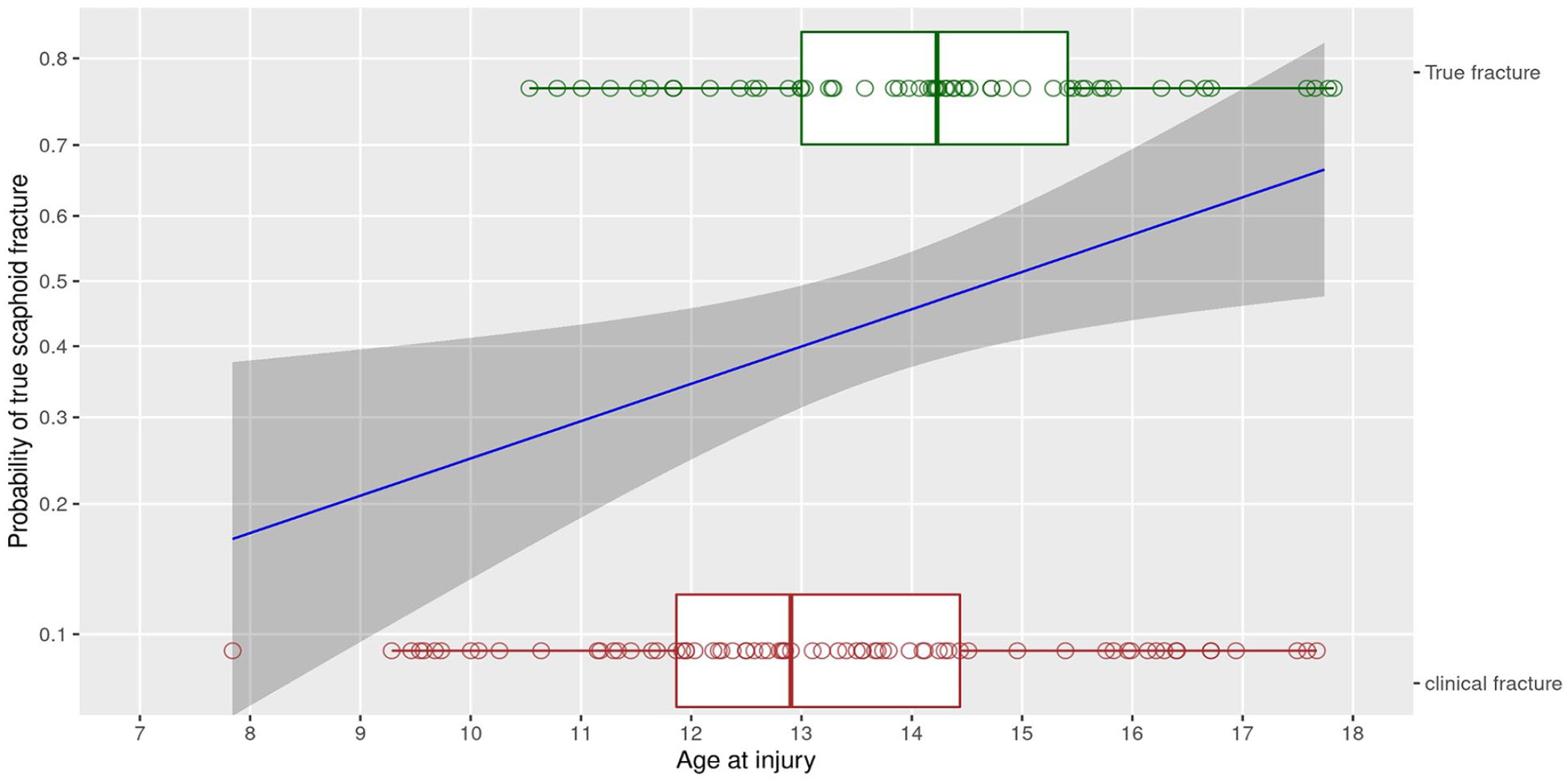
Probabilities of a true scaphoid fracture with age at injury.
Results of Multivariable Logistic Regression.
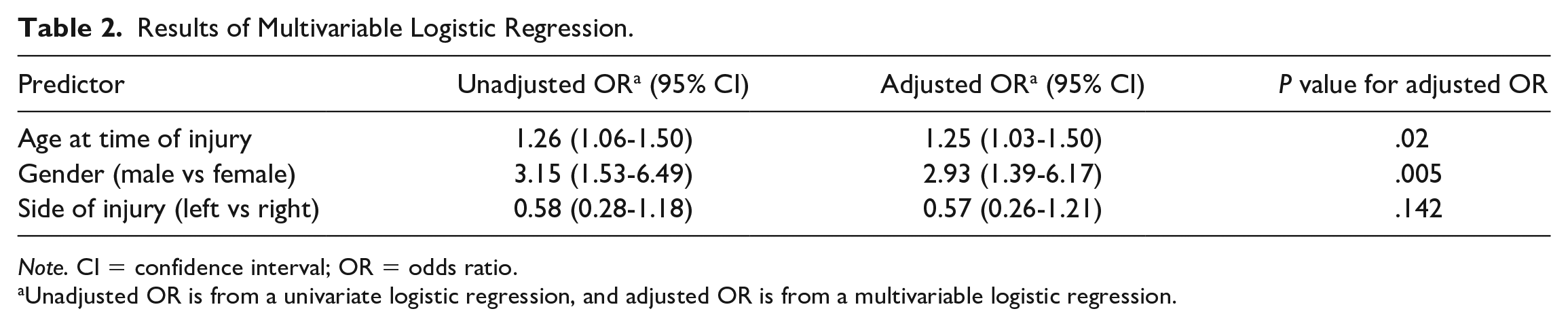
Note. CI = confidence interval; OR = odds ratio.
Unadjusted OR is from a univariate logistic regression, and adjusted OR is from a multivariable logistic regression.
Discussion
There is a paucity of evidence surrounding the management of children with suspected scaphoid fractures when radiographs are normal. Empiric immobilization may lead to overtreatment for most children. 3 Routine use of advanced imaging may not be cost-effective. Understanding the risk factors for fracture may guide management and enable judicious use of health care resources. We identified risk factors for scaphoid fracture in children presenting to a tertiary pediatric orthopedics and plastic surgery clinic.
For every year older, risk of true scaphoid fracture increased by 25%. Similarly, by being a man, risk of true scaphoid fracture diagnosis was almost 3 times higher than that of women at the same age. Our results confirm that side of injury is not adding any predictive value to the model to predict diagnosis of true fracture.
Thus, a higher index of suspicion of true scaphoid fracture in older men (and conversely, a lower index of suspicion in younger women) may be indicated. Understanding the likelihood of true scaphoid fractures may enable evidence-based decisions regarding the use of advanced imaging and management. Evidence in children is limited. Evenski et al identified volar scaphoid tenderness, radial deviation pain, and pain with active wrist range of motion as predictors of scaphoid fracture. 5 In adults, male sex has been identified as a predictor of true scaphoid fracture by Duckworth et al, but male sex and older age have never been identified as predictors of fracture in children. 6 Our results, however, seem plausible as it is hypothesized that older men are more likely to engage in high-impact activities. Other studies in adults have identified a number of other possible demographic and clinical examination predictors of fracture. Rhemrev et al identified extension less than 50%, supination strength less than or equal to 10% the contralateral side, and previous fracture to be independent predictors of true scaphoid fractures in adults. 7 A clinical decision rule was developed in adults using sex, swelling of the anatomic snuffbox, tenderness in the anatomic snuffbox, painful ulnar deviation, and painful axial thumb compression to predict scaphoid fractures, with a sensitivity of 97% but a specificity of 20%. 8 These physical examination findings unfortunately were not systemically documented in our medical records.
Scaphoid fracture location and prognosis in our population seem to be in agreement with previous literature, tending to occur at the distal pole and healing well. 9 Gholson et al showed that increasing body mass index produces a fracture pattern similar to the adult population, with waist fractures the most common followed by distal pole fractures and proximal pole fractures. 4 Our study demonstrates a similar distribution of distal pole and waist fractures. Porter and colleagues’ retrospective chart review of 144 wrists in children aged 4 to 11 years suggests that clinical suspicion for scaphoid fractures does not need to be x-rayed or immobilized. 10 In our study, 14% (8/56) of scaphoid fractures occurred in patients aged 11 years or younger, suggesting that although less common, scaphoid fractures do occur in this age group.
As a single-center retrospective cohort study, identification of other potential predictors was limited by the retrospective nature of this study. History, detailed clinical examination, and outcomes were not consistently recorded in the medical records. The diagnosis of a true scaphoid fracture may also be a limitation as few patients were referred for advanced imaging (CT, MRI). Young children with incompletely ossified carpal bones may also have fractures not visible on plain radiograph. As such, we may be underestimating the true incidence of scaphoid fracture. There is also considerable variability in the assessment of radiographs for scaphoid fractures. We attempted to mitigate this risk by using radiographic interpretations from both the surgeon and the radiologist. The clinical significance of a scaphoid fracture that is only visible on CT or MRI, however, remains to be determined.
This study identifies older age and male sex as predictors of true scaphoid fractures in children with suspected scaphoid injuries. As it may be unreasonable to MRI all children with a suspected scaphoid injury, knowledge of the risk of scaphoid fracture in children at high and low risk may guide management. For example, children in higher risk groups may benefit from further investigations and prompt treatment, whereas children in lower risk groups may require less advanced imaging and less caution. Alternatively, it may be advantageous to perform advanced imaging for low-risk children to rule out a fracture and obviate the need for immobilization whereas high-risk children are simply immobilized. Further studies are required before developing such a rule in or rule out strategy for advanced imaging.
Supplemental Material
sj-docx-1-han-10.1177_15589447241231311 – Supplemental material for Predictors of True Scaphoid Fractures in Children
Supplemental material, sj-docx-1-han-10.1177_15589447241231311 for Predictors of True Scaphoid Fractures in Children by Daniel Milad, Aneesh Karir, Kevin Smit, Sasha Carsen and Kevin Cheung in HAND
Footnotes
Supplemental material is available in the online version of the article.
Author Contributions
DM: data collection, analysis, manuscript writing; AK: data collection, analysis, manuscript reviewing; KS: study design, manuscript reviewing; SC: study design, manuscript reviewing; KC: study design, data analysis, manuscript writing.
Ethical Approval
This study was approved by the Children’s Hospital of Eastern Ontario Research Ethics Board (approval no. 17/128X).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
This study is retrospective in nature and did not require informed consent as per the Research Ethics Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.