
Abstract
Background:
Percutaneous pinning has been the predominant technique for fixation of proximal phalanx fractures, but stiffness is a reported complication. The introduction of intramedullary (IM) nail fixation of proximal phalanx fractures provides a stronger biomechanical fixation for amenable fracture patterns with the added benefit of not tethering the soft tissue. The goal of this study was to compare the surgical outcomes of IM nail and percutaneous pin fixation in isolated proximal phalanx fractures.
Methods:
A retrospective review was performed at our institution between the years 2018 and 2022 for patients treated for proximal phalanx fractures. Patients that underwent fixation with IM nails or percutaneous fixation for isolated extraarticular proximal phalanx fractures were included. Patients were excluded if they had concomitant hand fractures, tendon injury, or intraarticular extension.
Results:
A total of 50 patients were included in this study. Twenty-eight patients received percutaneous pin fixation, and 22 patients underwent IM nail or screw fixation. There was no significant difference in injury patterns or demographics between these two groups. Patients that underwent IM nail fixation had a significantly quicker return to active motion, shorter duration of orthosis treatment, and fewer occupational therapy visits. In addition, patients in the IM fixation group had significantly improved range of motion (ROM) at 6 weeks postoperatively.
Conclusions:
This study demonstrates that patients receiving percutaneous pin or IM nail fixation have equivocal union and complication rates. The IM nail fixation group was able to have quicker return to mobilization, fewer required occupational therapy visits, and improved early ROM.
Introduction
Phalangeal fractures are some of the most common injuries encountered by hand surgeons. 1 Stable, nondisplaced fractures can be managed nonoperatively; however, patients presenting with unstable fracture patterns or concern for malrotation on examination are indicated for reduction and fixation. 2 Kirschner wires (K-wires) have traditionally been used for fixation of proximal phalangeal fractures. 3 Periarticular placement of K-wires provides reliable results with percutaneous treatment to amenable fracture patterns. Kirschner-wire fixation provides the benefit of preservation of periosteum and blood supply to phalangeal fractures. However, percutaneous placement does tether soft tissue structures and requires prolonged immobilization which can lead to joint stiffness and delayed return to function. 4
Intramedullary (IM) fixation is a keystone principle in load sharing osteosynthesis fracture management. 5 Biomechanical studies have demonstrated that IM fixation of metacarpal fractures results in a stronger construct compared with crossing K-wires.6 -8 Although fixation with plates and screws provides an equivalent construct strength, placement of IM fixation does not have the same associated complications in proximal phalanx fractures including extensor lag, hardware failure, infection, and need for additional surgery for hardware removal or tenolysis.9,10 Metacarpal fractures have been previously treated with noncompressive nail and headless compression screw fixation. 11 A nail provides noncompressive fixation with equal thread pitch to prevent any undesired deforming forces. A headless compression screw has variable pitch to apply compressive forces between fracture segments. The use of IM fixation in metacarpal fractures is well established.12,13 The role of IM fixation in proximal phalanx fractures is not as well delineated.
A cadaveric study confirmed the feasibility of IM fixation and preferential intraarticular placement for proximal phalanx fractures. 14 Previous studies have demonstrated that IM fixation can successfully be used in the treatment of proximal phalangeal fractures.15 -17 The goal of this study was to compare postoperative outcomes between K-wire and IM fixation in extraarticular proximal phalanx fractures. The authors hypothesized that patients receiving IM fixation would have an earlier improved range of motion (ROM) compared with K-wire treatment.
Methods
The protocol for this study received approval from our institutional review board. A retrospective review was performed at our institution between January 2018 and May 2022. All patients for which Current Procedural Terminology codes 26725, 26727, and 26735 were billed for treatment of proximal and middle phalanx fractures during this time period were identified. Inclusion criteria for patients included: closed, isolated, extraarticular proximal phalanx fracture, treatment with IM nail/screw or percutaneous K-wire fixation, and age greater than 18 years old. Patients were excluded if they had middle phalanx fractures, concomitant hand fractures, tendon injury, intraarticular extension, fracture comminution, or follow-up less than 30 days. Patient comorbidities and demographics were obtained including smoking status, history of diabetes, age, sex, hand dominance, mechanism of injury, and fracture pattern.
Surgical site infection was defined as any patient requiring treatment with postoperative antibiotics following the perioperative period. Bony union was defined as union, malunion, or nonunion based on evaluation of postoperative radiographs by the operative surgeon at postoperative clinic appointment. Immobilization duration was defined as the period in which the patient was placed in orthosis and instructed to not perform any ROM. Duration until orthosis clearance was defined as the time in which a patient was prescribed any orthosis in the postoperative period. This includes treatment of orthosis for immobilization protection, but also custom splints to aid in finger positioning and ROM prescribed by the occupational hand therapists.
All patients underwent evaluation and treatment by a hand occupational therapist (OT) postoperatively. Number of visits was recorded and determined by the recommendations of the treating therapist. All patients were evaluated 6 weeks postoperatively for active range of motion (AROM) at the surgical finger metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints. Range of motion measurements were taken by hand OT using finger goniometer. In addition, patients completed the patient-reported outcomes measurement information system upper extremity (PROMIS UE) and pain inference (PROMIS PI) computer adaptive tests at the 6-week postoperative visit. The results of these patient-reported outcomes (PROs) were converted to T score and range from 10 to 90. Patient-reported outcomes measurement information system upper extremity higher scores are indicative of increased function specifically related to the upper extremity. Patient-reported outcomes measurement information system pain inference higher scores are related to increased interference in function secondary to pain.
Surgical Technique
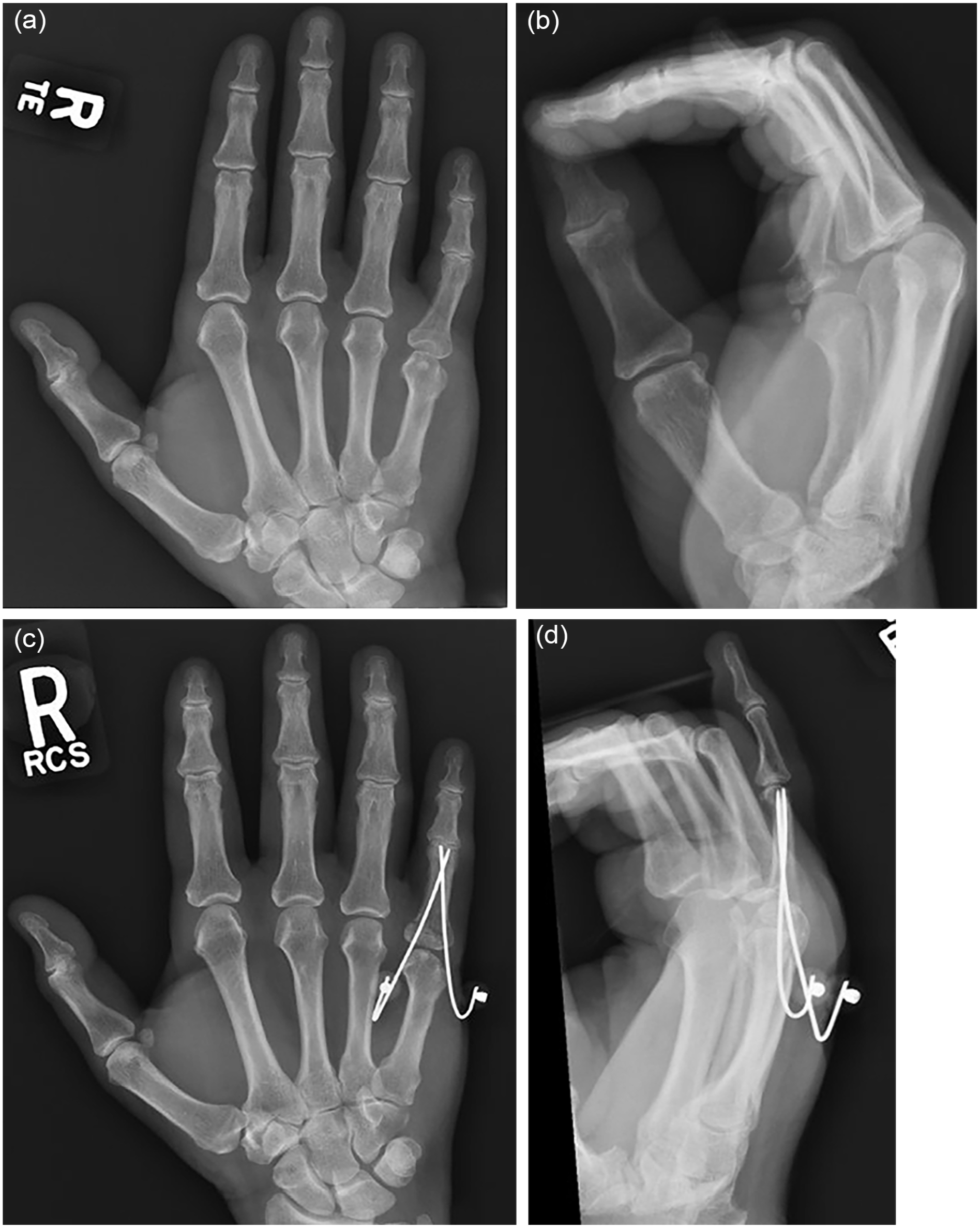
All surgeries were performed by fellowship-trained hand surgeons. All surgeries were performed at a surgery center under general anesthesia or regional block with monitored anesthesia care sedation. Closed reduction was performed for all fractures using traction, manipulation via hand pressure, and/or penetrating reduction forceps. All IM fixations were performed using the intraarticular antegrade approach. A guidewire was placed from the base of the proximal phalanx across the fracture into the IM canal of the bone. A small 5-mm skin incision was made at the entry site of the guidewire to allow for drill placement. The guidewire was then over drilled with power drill and appropriate screw or nail length was radiographically measured. Placement of the IM nail or headless compression screw was determined by the operative surgeon depending on the fracture pattern and the desire for compression or noncompressive fixation. All screws and nails ranged between 2.0 and 2.5 mm in diameter and varied in length. Screws and nails were used from a variety of companies including Acumed ExsoMed INnate NailTM (Hillsboro, Oregon), Field Orthopaedics NX NailTM (Basel, Switzerland), and Arthrex QuickFix Cannulated ScrewTM (Naples, Florida). A second IM nail/screw was placed at the discretion of the operative surgeon (Figure 1).

A 27-year-old woman presented with transverse extraarticular base fracture of the small finger proximal phalanx after a fall (a and b). She was treated with closed reduction and intraarticular antegrade placement of a 2.0-mm intramedullary nail with 30 mm in length (c and d).
Kirschner-wire fixation was performed using a periarticular approach with 0.045-inch K-wires placed antegrade from the radial and ulnar articular edge. No patients received transarticular fixation. In addition, all patients were treated with two crossing K-wires (Figure 2). At the completion of each case, the patient was placed into splint orthosis or soft dressing based on the discretion of the operative surgeon.
A 61-year-old woman presented with transverse extraarticular base fracture of the small finger proximal phalanx after a fall (a and b). She was treated with closed reduction and percutaneous fixation with two crossing 0.045-inch Kirschner wires (c and d).
Statistical analysis was performed on the data using an independent t tests for continuous variables, Fisher’s exact test for categorical variables with less than five categories, and chi-squared analysis for all other categorical analysis with P value less than .05 considered statistically significant. A post hoc power calculation was performed based on the independent mean values of joint ROM and standard deviation, number of sample participants per group, and alpha value of 0.05. Post hoc power analysis demonstrated sufficient power for findings.
Results
A total of 50 patients met inclusion criteria for this study. Twenty-two patients were treated with IM fixation and 28 patients were treated with percutaneous pins. Patient demographics, comorbidities, and injury characteristics are depicted in Table 1. There was no statistically significant difference between the two cohorts for demographics or injury characteristics. Forty-three patients (86%) sustained blunt trauma injuries. The most commonly injured digit was the small finger with 36 (72%). Most patients were treated for oblique or transverse shaft fractures (70%). Fifteen patients (30%) were treated for oblique shaft or base fractures.
Demographics of Patients.
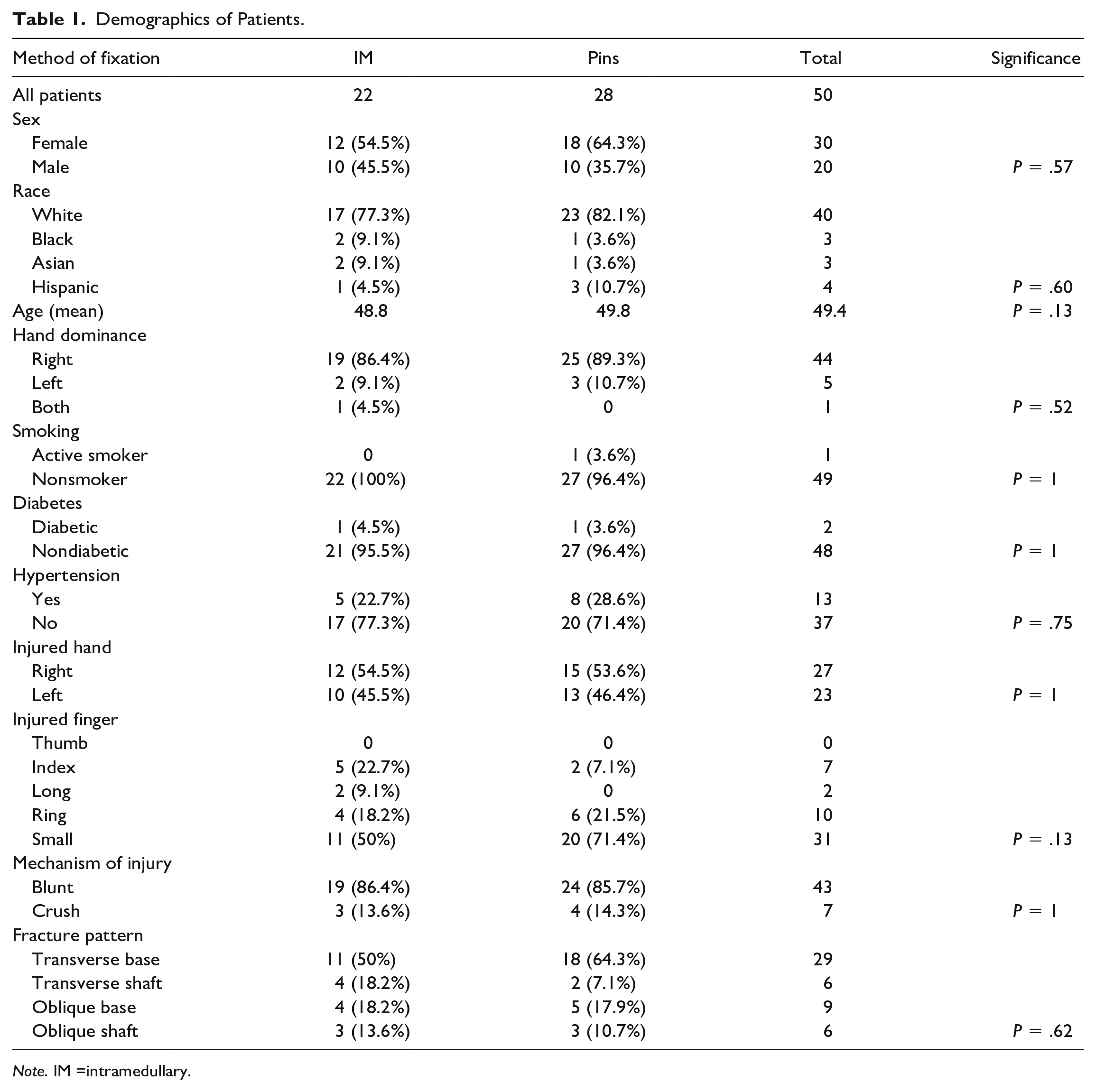
Note. IM =intramedullary.
The average follow-up for all patients was 129 days (Table 2). There was no statistically significant difference in operative time between the IM and K-wire cohorts (40.1 vs 31.3 minutes, P = .19). Two patients in the K-wire cohort presented with postoperative surgical site infections treated with oral antibiotics compared with zero patients in the IM group. One patient in the IM cohort resulted in a loss of reduction in the early postoperative period (Figure 3). This patient returned to the operating room (OR) for IM nail removal and conversion to K-wire fixation. A single patient within the K-wire cohort required return to the OR for buried K-wire removal and flexor tenolysis due to prolonged stiffness.
Surgical Outcomes.
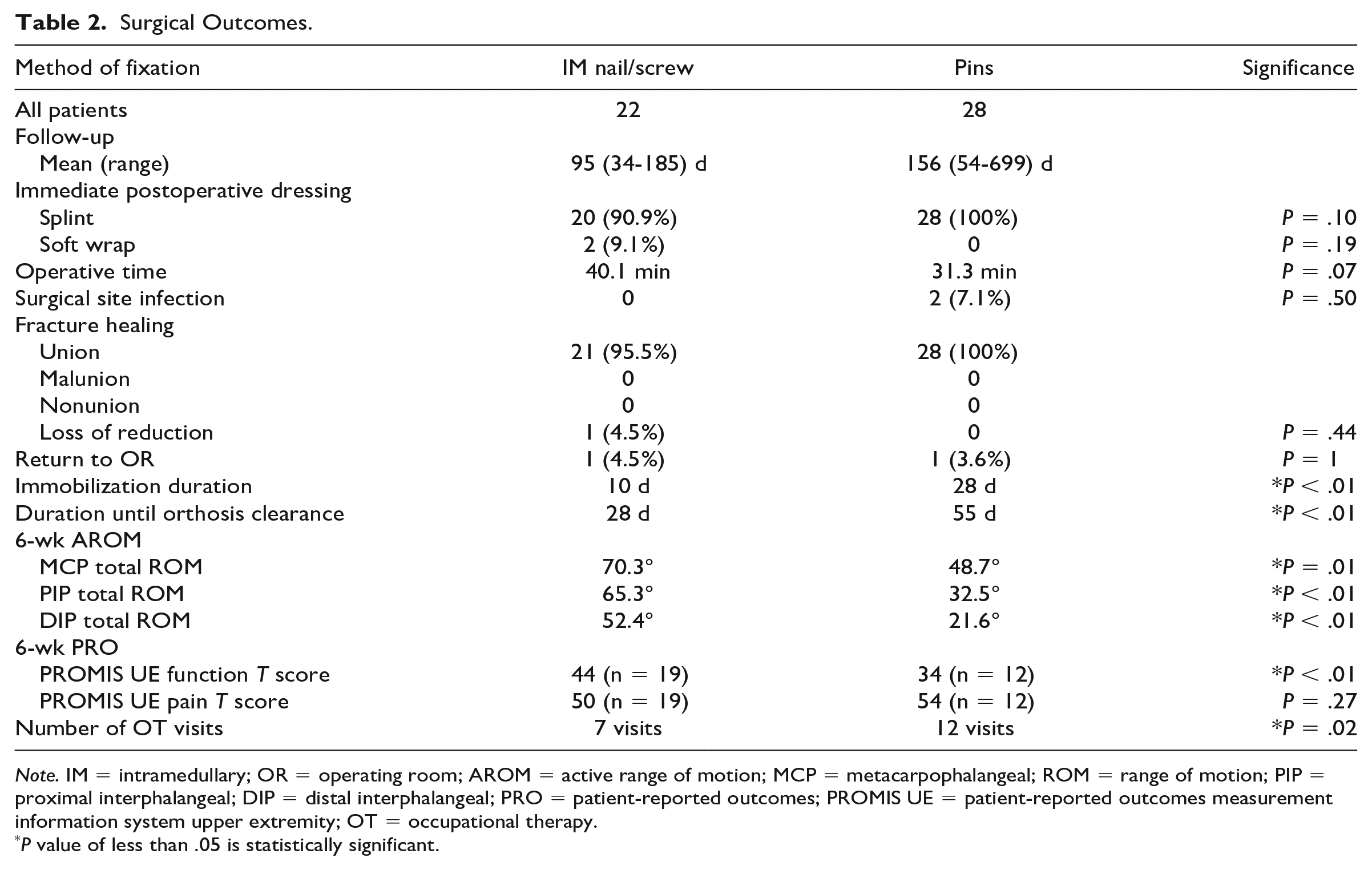
Note. IM = intramedullary; OR = operating room; AROM = active range of motion; MCP = metacarpophalangeal; ROM = range of motion; PIP = proximal interphalangeal; DIP = distal interphalangeal; PRO = patient-reported outcomes; PROMIS UE = patient-reported outcomes measurement information system upper extremity; OT = occupational therapy.
P value of less than .05 is statistically significant.
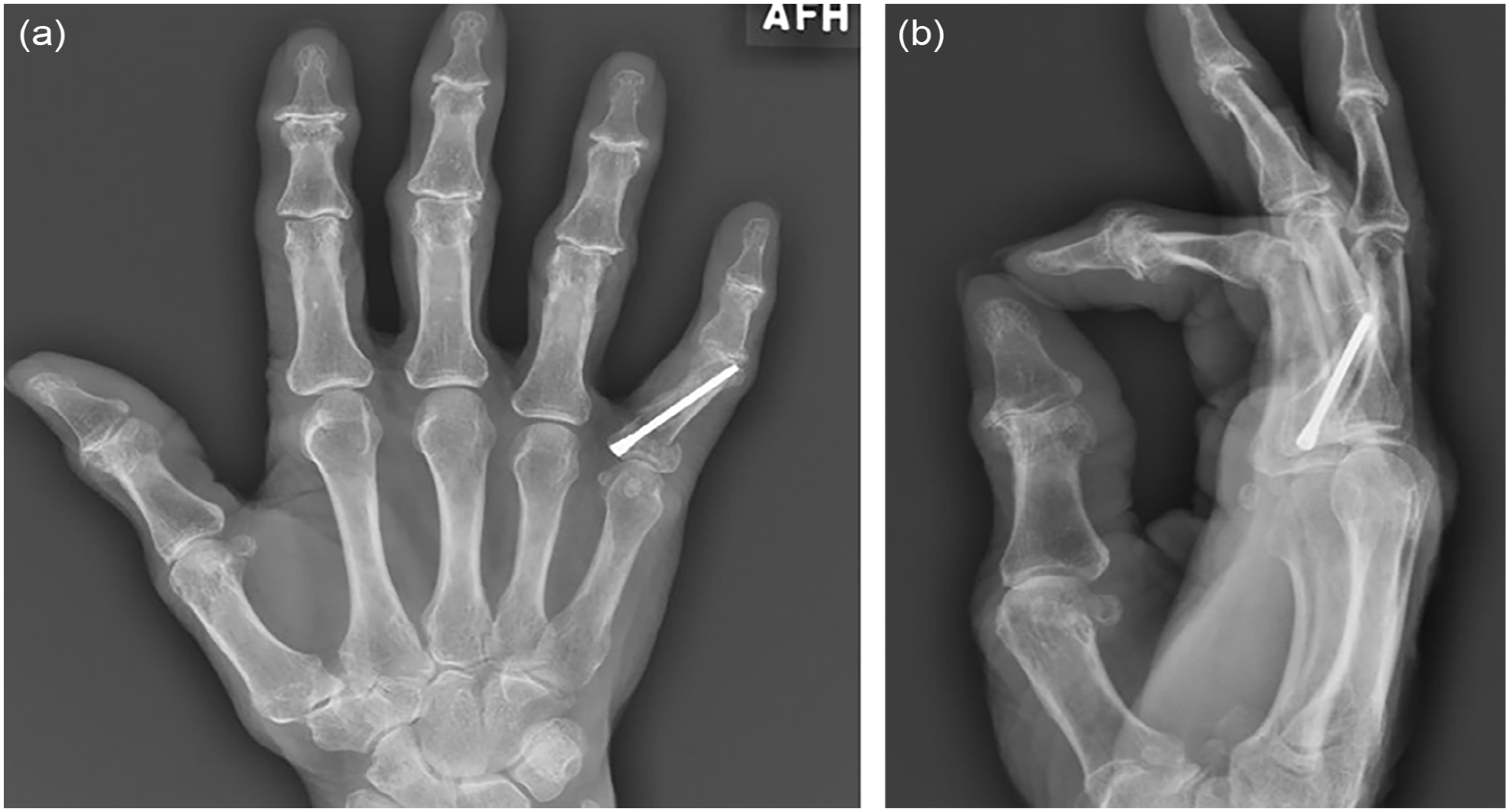
A 71-year-old woman underwent single intramedullary nail (2.0 mm) fixation of the right ring finger. At postoperative day 15, she was noted to have loss of alignment (a and b) and returned to the operating room for nail removal and percutaneous pin fixation.
Patients that received IM nail/screw fixation had a significantly lower mean duration of immobilization compared with K-wire fixation (10 vs 28 days, P < .01). In addition, the IM patients also were cleared from any orthosis earlier compared with the K-wire cohort (28 vs 55 days, P < .01). The IM treatment group had significantly improved total AROM at the MCP, PIP, and DIP joint compared with the K-wire treatment at 6 weeks postoperatively. The IM screw/nail patients on average required fewer hand OT visits compared with K-wire patients (7 vs 12 visits, P = .02).
A total of 21 patients completed the PROMIS UE and PROMIS PI evaluations at the 6-week postoperative visit. The IM cohort had a significantly higher PROMIS UE score on average compared with the K-wire cohort (44 vs 34, P = .02). There was no statistically significant difference between the average scores of the PROMIS PI between the two treatment groups.
Of the 22 patients in the IM cohort, 19 were treated with noncompressive nails (Table 3). Seven patients were treated with two IM nails and 15 patients were fixated with a single IM nail. On average, the length of initial nail was 32 mm. If a second nail was used, it had an average length of 22 mm. The average length of nail was dependent on the injured finger with the longest nail average of 40 mm in the long finger proximal phalanx and 26 mm average nail length for the small finger.
IM Fixation Details.
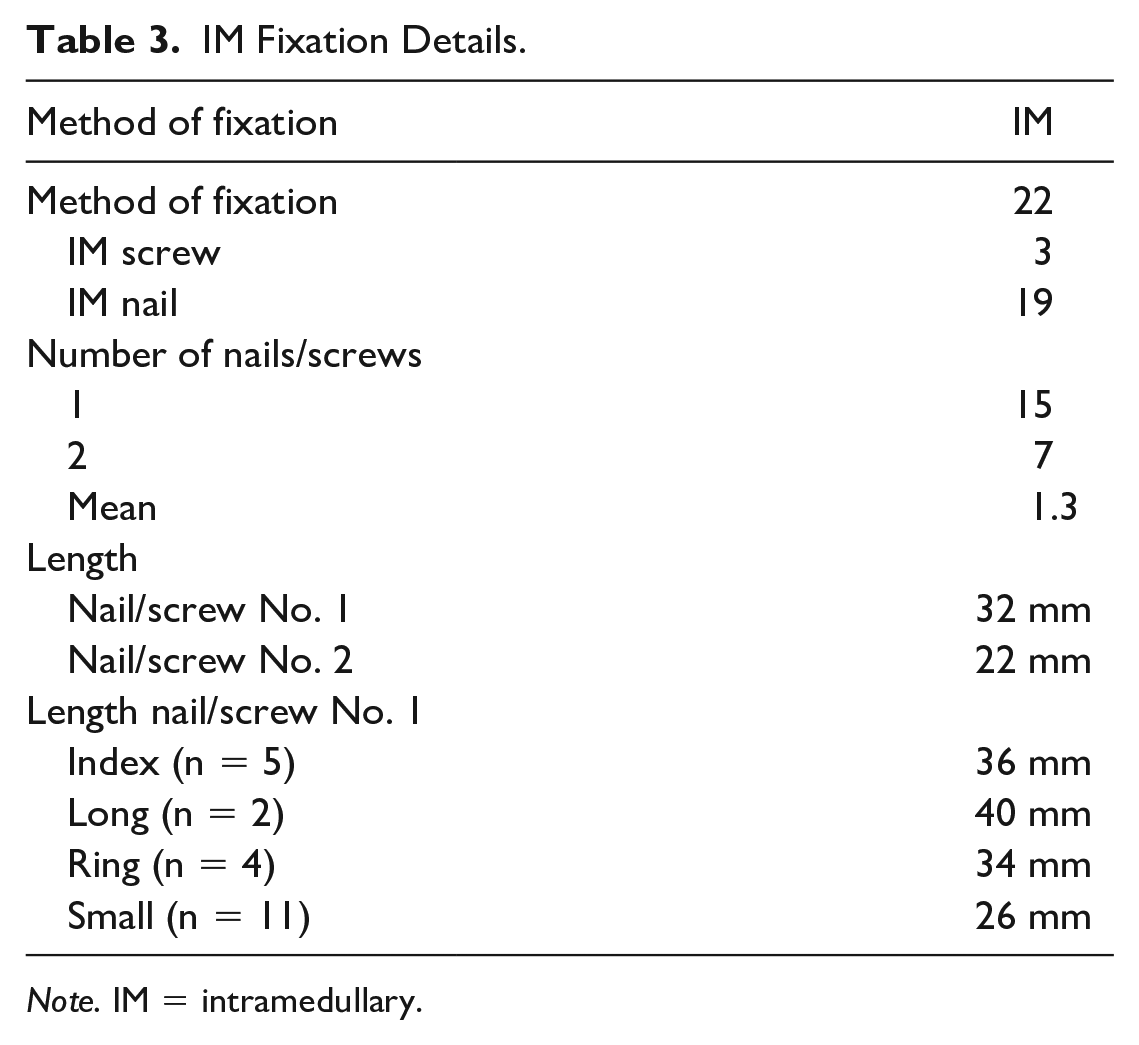
Note. IM = intramedullary.
Discussion
The results of this study demonstrate that IM fixation of proximal phalanx fractures results in improved and earlier ROM compared with K-wire fixation in comparable fracture patterns in the early postoperative period. Fracture characteristics may limit or guide surgical fixation options. Patients with significant comminution or intraarticular involvement were excluded. This was reflected in our patient cohort with majority of included patients presenting with shaft fractures. Intraarticular fractures, especially involving the PIP joint, can be challenging to manage. 18 These intraarticular injuries can often be associated with structural joint injuries that limit postoperative recovery. Percutaneous pins, plates, and interfragmentary screws remain as necessary treatment options for comminuted, intraarticular, or significantly displaced proximal phalanx fracture patterns that cannot be successfully treated with IM nails. 19 This study was designed to select patients with isolated proximal phalanx extraarticular fractures amenable to IM fixation. The results are limited to patients presenting with extraarticular oblique and transverse proximal phalanx fractures.
Patients treated with IM nails/screws had a significantly improved ROM at the MCP, PIP, and DIP joints at 6 weeks postoperatively. This improved ROM can be attributed to multiple factors. Intramedullary fixation has been demonstrated to have superior biomechanical fixation without the need for immediate postoperative immobilization.20,21 Two of the patients in this study were treated without immediate orthosis and the IM group had significantly shorter duration of immobilization compared with the K-wire fixation cohort. Early mobilization has been demonstrated to significantly affect early ROM recovery. 22 The more recent patients treated at our institution with IM nails for proximal phalanx fractures are being selected for immediate mobilization. This evolving trend would further shift the difference observed between these two patient groups for early ROM. Certain K-wire fixation methods have been associated with tethering of collateral ligaments, joint capsule, and the extensor mechanism which limits early postoperative ROM. 23
The longer recovery in the K-wire fixation group was also associated with longer duration of overall need for orthosis. This result reflects the K-wire patients requiring more frequent use of orthosis for finger positioning or ROM corrections. Orthosis protocol duration in postoperative pin fixation is not standardized among hand surgeons. The need for prolonged splinting may be a result of our institution’s preference and the prolonged orthosis for ROM corrections may be a result of this prolonged immobilization. Longer recovery was also evident by the higher average number of OT visits in the K-wire cohort. Increased utilization of OT hand therapy is directly related to overall health care burden of hand fractures. 24 Although initial costs of K-wires are lower than that of IM screws or nails, a study by Brewer et al found that IM screw treatment of metacarpals had a lower overall cost burden compared with K-wires. 25 More studies are necessary to evaluate the cost analysis of percutaneous pins or IM nails in the proximal phalanx injury population.
There was no significant difference in postoperative bony union or infection rates between the K-wire and IM fixation groups. A single patient in the K-wire group required return to the OR for buried pin removal and an additional trip for flexor tenolysis. Both buried pins and stiffness requiring tenolysis are known complications of K-wire fixation. 26 Well-reduced proximal phalanx fractures have high rates of reported bony union. 4 One patient in the IM nail group presented with loss of alignment in the early postoperative period. This nail was removed and the patient was converted to K-wire fixation with immobilization. This patient was treated with a single 2.0-mm IM nail at the initial operation. A nail with larger diameter (2.5 mm) or second nail placement may have provided improved stability across the fracture site. Optimizing nail diameter and placement reduces the risk of early loss of alignment.
Studies evaluating proximal phalanx IM screw and nail fixation have described using screw diameter ranging from 2.0 to 3.0 mm. 27 A previous anatomic study demonstrated the proximal phalanx isthmus diameter ranged from 2.0 to 3.3 mm on average and was dependent on the specific finger. 28 Evaluation of each patient’s anatomy is critical for successful IM fixation. The advantage of selecting a single tightly fitting diameter nail compared with placement of two smaller diameter nails remains unknown. Selecting a nail with an oversized diameter may result in a propagating fracture when over drilling. A study by Gaspar et al demonstrated that dual headless screw fixation for proximal phalanx fractures may provide additional biomechanical strength compared with single screw fixation. 17 In our study, single nail/screw fixation was performed in 15 patients, compared with two nail/screw fixation in 7 patients. As expected, nail or screw length was dependent on the injured finger. The selection of headless compression screws for 3 patients in this study was all performed based on surgeon judgment and need for compression to aid in proximal phalanx reduction. The results of this study can be applied for proximal phalanx treatment with both headless compression screw and nail fixation.
The patients in the IM cohort had a significantly higher PROMIS UE score at 6 weeks compared with the pins group. Only 21 of the 50 patients in this study had completed the PRO at 6 weeks after surgery. This small sample size is a limitation of these findings. Kazmer et al reported a minimal clinically important difference for the PROMIS UE in the nonshoulder general upper extremity population to be 2.1. 29 The difference of 10 points at 6 weeks is both statistically and clinically significant.
This study does have limitations. A retrospective study has inherent selection bias between patients for each cohort. The selection of fixation method was not randomized and therefore it may skew which patients receive pins or IM screws. This bias was minimized by comparing injury patterns and demographics that were not statistically different between the two treatment groups. The treatment selection difference most likely reflects the changing practice of hand surgeons at our institution with more recent patients being treated with IM nails or screws. The small sample size of the two groups also limits the power and analysis of the study. Including patients with only isolated proximal phalanx fractures and without any tendon or soft tissue injury reduced the patient group size. This limits confounding factors, but also decreases generalizability of the results. Ensuring adequate follow-up in the trauma population for accurate postoperative assessment also limited the study numbers but was necessary to yield meaningful conclusions. The findings of this study only reflect a very short follow-up period of results for ROM. The surgeons’ preference for longer immobilization of pin-treated patients also decreases earlier ROM. The authors would expect the ROM difference would decrease between the two cohorts with longer follow-up.
Conclusion
This is the first study to perform cohort comparison of IM and K-wire fixation in proximal phalanx fractures. Extraarticular proximal phalanx fractures treated with IM nails have significantly improved early ROM compared with treatment with K-wire fixation with equivalent clinical outcomes. Further studies need to be performed to identify the ideal method of IM fixation for specific fracture patterns.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.S.R. has received royalties from Acumed and Zimmer and serves as a consultant for Acumed and Depuy Synthes. M.J.R. has received royalties from Acumed and Field Orthopaedics and serves as a consultant to Acumed, DJO Global, restor3d, and Zimmer Biomet. All other authors have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.