
Abstract
Background:
Distal radius fractures (DRFs) are common upper extremity fractures and often require surgical fixation when they are intraarticular. Preoperative computed tomography (CT) has emerged as a surgical planning tool to evaluate intraarticular DRFs. Although CT affords additional details, patients receive higher radiation doses than standard radiographs. We aim to develop a low-dose CT (LDCT) protocol, relative to the institutional standard-dose CT wrist for intraarticular DRFs although providing adequate detail for surgical decision-making.
Methods:
A single-institution prospective study was conducted on patients with intraarticular DRFs who underwent closed reduction and below-elbow splinting who otherwise would undergo wrist CT. Observations were defined as total measurements taken, with each view undergoing 44 measurements. Patients underwent 2 scans with a standard dose and a 10× dose reduction. Articular step and gap measurements were recorded in the sagittal and coronal images.
Results:
A total of 11 patients were enrolled (7 women and 4 men). The mean age was 55 years (SD = 20.1). There were a total of 4 reviewers: 1 attending surgeon, 2 resident physicians, and 1 student. When comparing LDCT and conventional-dose CT (CDCT), there were no significant differences in step and gap measurements across all reviewers.
Conclusion:
This study demonstrated that LDCT provides comparable imaging quality for surgical planning as a CDCT without significant diagnostic decay in the setting of DRFs. This comes with the added benefit of a 10-fold reduction in radiation exposure. These results suggest that LDCT is an opportunity to reduce effective radiation in patients although providing beneficial preoperative imaging.
Introduction
Fractures of the distal radius are the most common fracture of the upper extremity, accounting for up to 15% of all fractures in adults. 1 Particularly problematic among these fractures are those involving the intraarticular surface, as failure to adequately restore articular congruity has been associated with the development of premature radiocarpal, ulnocarpal, and distal radioulnar joint arthritis. 2 Residual articular displacement of greater than 2 mm at the time of union has been associated with symptomatic posttraumatic arthritis in up to 91% of patients, independent of the amount of displacement observed preoperatively. 2
To aid and improve surgical planning, preoperative computed tomography (CT) wrist has emerged as a useful diagnostic tool for intraarticular distal radius fractures (DRFs). 3 Although radiographs remain the gold standard for initial imaging modality for patients with suspected wrist trauma, multiple authors have investigated the use of CT in more accurately classifying fracture patterns and developing treatment plans based on their more detailed representations of articular incongruity.4-6 Radiographs may also underestimate, or miss entirely, areas of articular displacement that may benefit from operative intervention. Arora et al 4 found in their prospective series of 120 intraarticular DRFs that the use of CT images along with plain radiographs changed the proposed treatment plan in 23% of cases, including a significant reduction in the number of cases thought to be amenable to nonoperative treatment.
Although CT examinations afford additional detail regarding injury patterns in periarticular fractures, they require subjecting patients to higher doses of radiation. 7 The risks of such exposures have been historically documented, most notably for the possibility of increased risk of cancer among those subjected to recurrent CT imaging.8,9 Several groups have described imaging protocols aimed at reducing the effective dose (ED) of radiation. Konda et al 10 reported their experience of using an ultra–low-dose CT (LDCT) protocol to diagnose fractures of the upper and lower extremities and found no significant difference in their diagnostic capabilities. Using this ultra-LDCT protocol, they were able to reduce the estimated ED in their study group by nearly 14-fold. A similar dose reduction CT protocol has been used to accurately detect the presence of intraarticular air in a cadaveric model of a traumatic arthrotomy at a threshold of 0.1 cc of air. 11 In addition, Lorenzana et al 12 demonstrated that LDCT images were sufficient for reliable preoperative planning in shoulder arthroplasty. These results further demonstrate the ability of a dose reduction CT to yield high-quality images, although reducing the ED conferred to patients.
To our knowledge, there are currently no studies in the literature comparing the use of LDCT to conventional-dose CT (CDCT) in DRFs. Therefore, we aim to evaluate the diagnostic capacity of LDCT and CDCT in DRFs for the assessment of articular step and gap displacement. Our goal in doing so is to develop a LDCT wrist protocol for patients with intraarticular DRFs that provides adequate detail for surgical planning at a decreased radiation dose compared with CDCT.
Materials and Methods
After approval by our institutional review board radiation subcommittee, we prospectively enrolled patients aged greater than or equal to 18 years with intraarticular DRFs who underwent closed reduction and application of a below-elbow plaster splint that would otherwise undergo a CT scan of the wrist as a part of routine care of the wrist injury. Patients were enrolled by the study team after being identified on presentation to the emergency department or in the hand surgery clinic. Patients were only recruited if their injury occurred less than 2 weeks before the time of enrollment. Exclusion criteria included patient ages less than 18 years, inability to speak English for completion of the consent process, pathologic fracture, prisoners, open fractures, and pregnant women. Women of childbearing age who were interested in participating in the study completed a urine pregnancy test before being able to provide their consent to participate in the study.
After completing appropriate informed consent for study participation, patients who elected to enroll underwent two CT scans in the same encounter on 1 of 6 different CT scanner models (GE HD750, GE Light Speed, 3 Siemens Flash, and Siemens Force). First, the CDCT protocol images were obtained using our current standard-of-care CT dose index (CTDI). Computed tomography dose index is a standardized measure of the radiation output of a particular CT scanner. The ability to quantify this value allows for a standardized means of comparing the radiation output of different CT scanner models. The current clinical dose protocols for extremity CT scans at our institution are on the order of 7 to 10 mGy CTDI, thus we sought to use a CTDI of 8 mGy. After the CDCT images were obtained, the patient remained in the same position on the CT scanner gantry, and the LDCT images were obtained. The CTDI for the LDCT protocol was obtained using a target dose reduction of approximately 10×—target CTDI of 0.8 mGy. This 10× CTDI dose reduction is similar to the CT dose reduction protocol used by Konda et al 10 in their cohort of intraarticular extremity fractures. The CTDI of both the CDCT and LDCT protocols for each patient was recorded. Images were obtained in the axial, sagittal, and coronal planes in both the CDCT and LDCT protocols (Figure 1). After the CDCT and LDCT were obtained, the study team reviewed the resultant images for each patient. Both the sagittal and coronal images representing the greatest step and gap displacement from the CDCT and LDCT of each patient were identified and marked for review. A total of 4 reviewers then reviewed the images and measured the step and gap displacement of each fracture using the longitudinal axis methods as described by Cole et al 13 (Figure 2). These measurements were chosen as a persistent articular gap and a step-off greater than 1 mm after DRF may lead to posttraumatic arthritis of the radiocarpal joint. 14
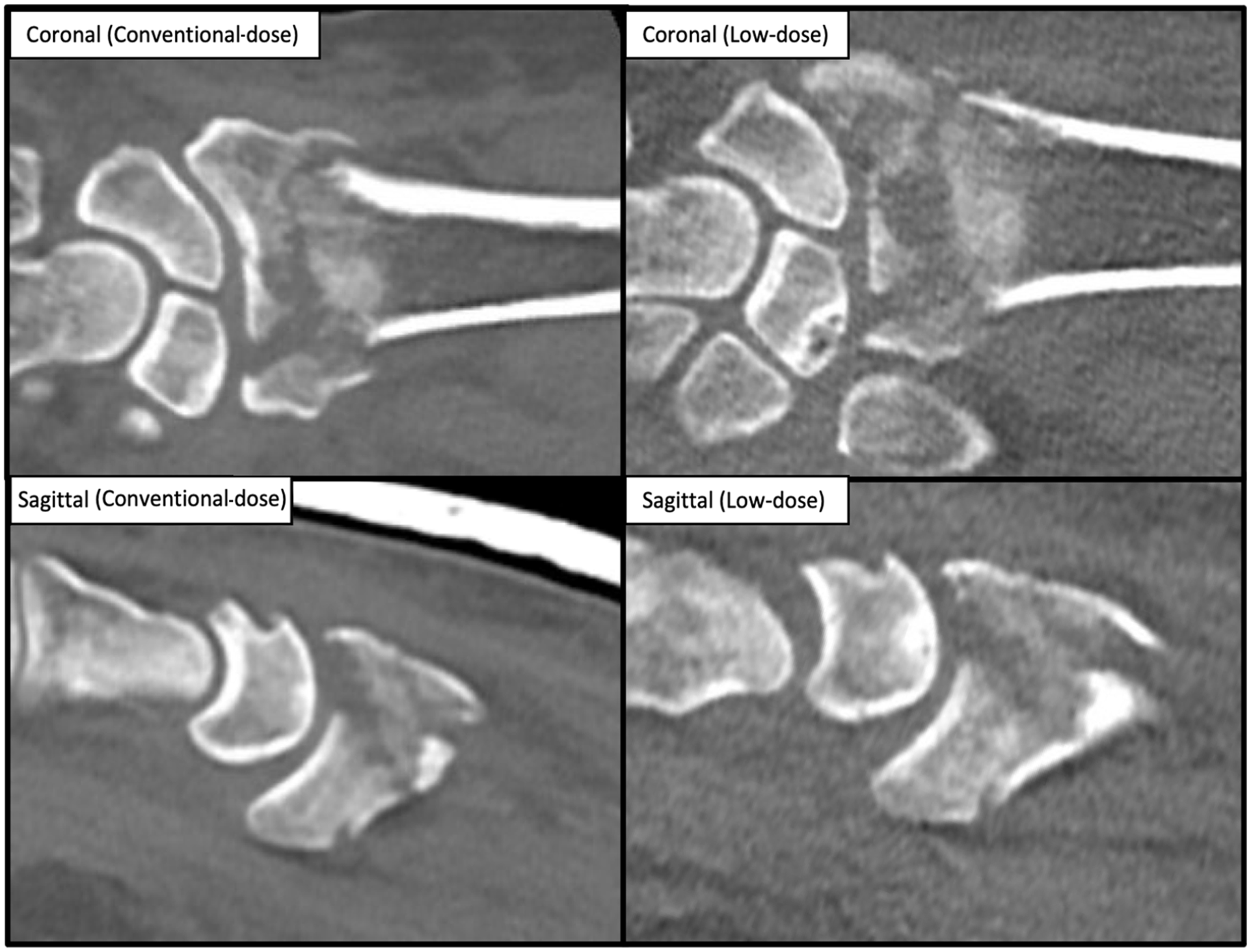
Conventional-dose and low-dose computed tomography (CT) images. Comparison of CT images of identical distal radius fractures at CT dose index of 8 and 0.8 mGy in the coronal and sagittal views, respectively.
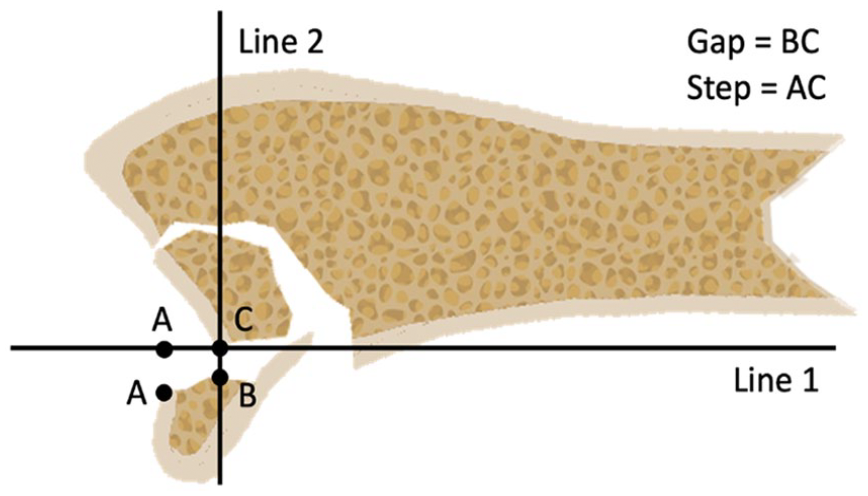
Longitudinal axis method.
Each patient’s demographic information was obtained from the electronic medical record. The final treatment plan—operative or nonoperative treatment—for each patient was recorded. The protocol report from each patient’s CT encounter was reviewed to obtain the CTDI and dose-length product for both the CDCT and LDCT sequences.
An a priori power analysis was performed via the program G*Power, using the predetermined parameters P = 80% and an effect size of 0.45. 15 This corresponded to a necessary sample size of 41 observations, for 40 degrees of freedom. Observations were defined as individual measurements taken by reviewers. The resulting data set was evaluated using a Student paired t-test. For all comparisons across different training levels, the number of raters at each training level was kept consistent for statistical analysis (raters = 1). As such, a representative resident was chosen via a random number generator for each comparison. Interrater reliability was assessed using the intraclass correlation coefficient (ICC) in a single-rater, two-way random effects model with absolute agreement. An ICC of less than 0.50 indicated poor reliability, between 0.50 and 0.75 indicated moderate reliability, between 0.75 and 0.90 indicated good reliability, and greater than 0.90 indicated excellent reliability. Statistical calculations were performed in the software environment R (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 11 patients were enrolled in the study, which included 7 women and 4 men. The mean age of the study population was 55 years (SD = 20.1).
There was a total of 4 reviewers: one hand fellowship–trained attending surgeon, one orthopedic surgery resident physician (PGY4), one plastic surgery resident physician (PGY4), and one medical student (MS4). When comparing LDCT and CDCT, there were no significant differences in measurements across all 4 reviewers (Figure 3). This included the step (P = .096) and gap (P = .766) measurements in the sagittal view as well as the step (P = .824) and gap (P = .128) measurements in the coronal view (Table 1).
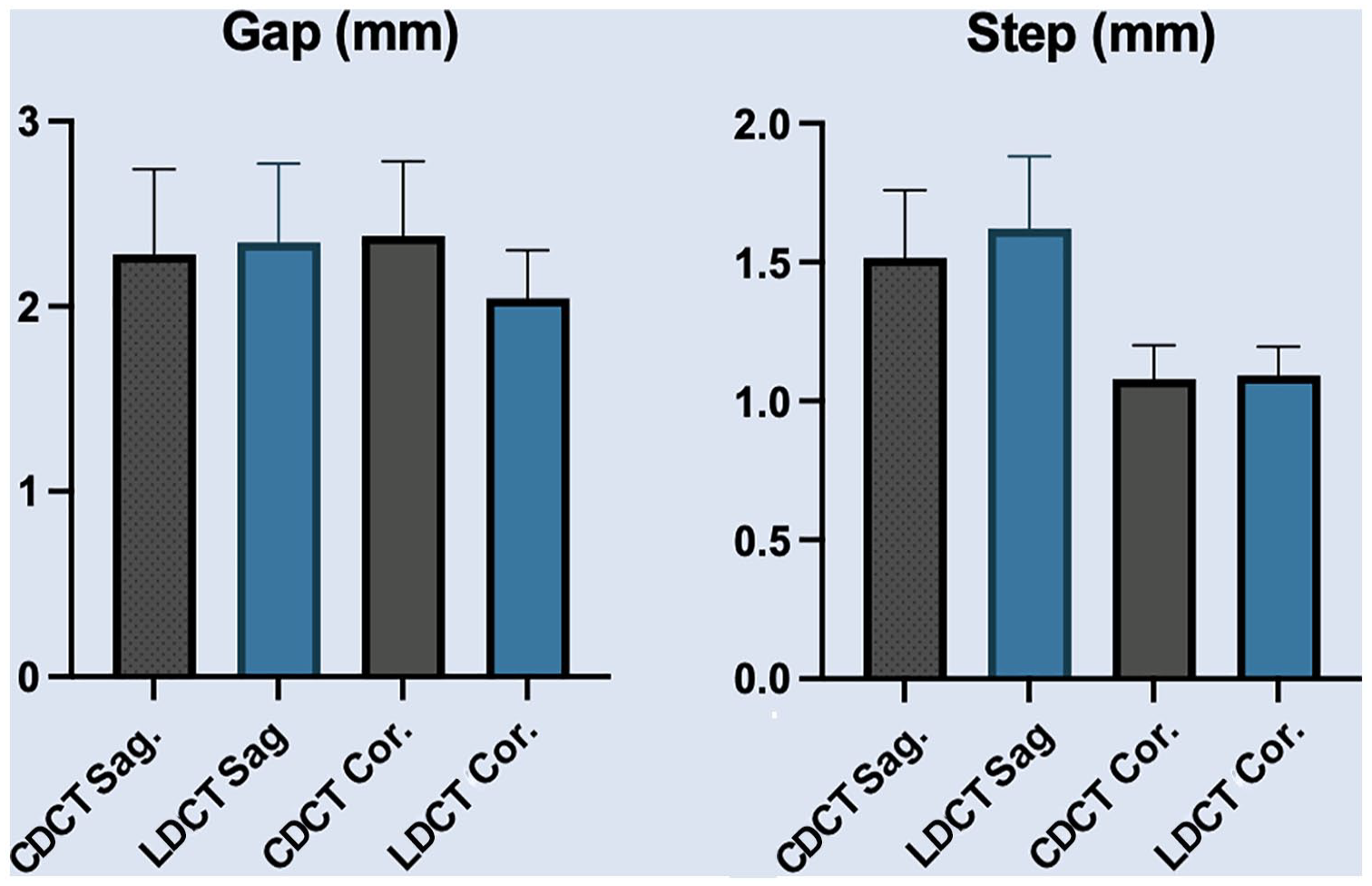
Conventional-dose and low-dose measurements. A comparison of aggregate CDCT and LDCT measurements showing no significant difference in both the sagittal (step: P = .096, gap: P = .766) and coronal (step: P = .824), gap: P = .128) views.
Step and Gap Measurements per Patient Averaged Across Each Reviewer as well as Total Mean per Measurement.
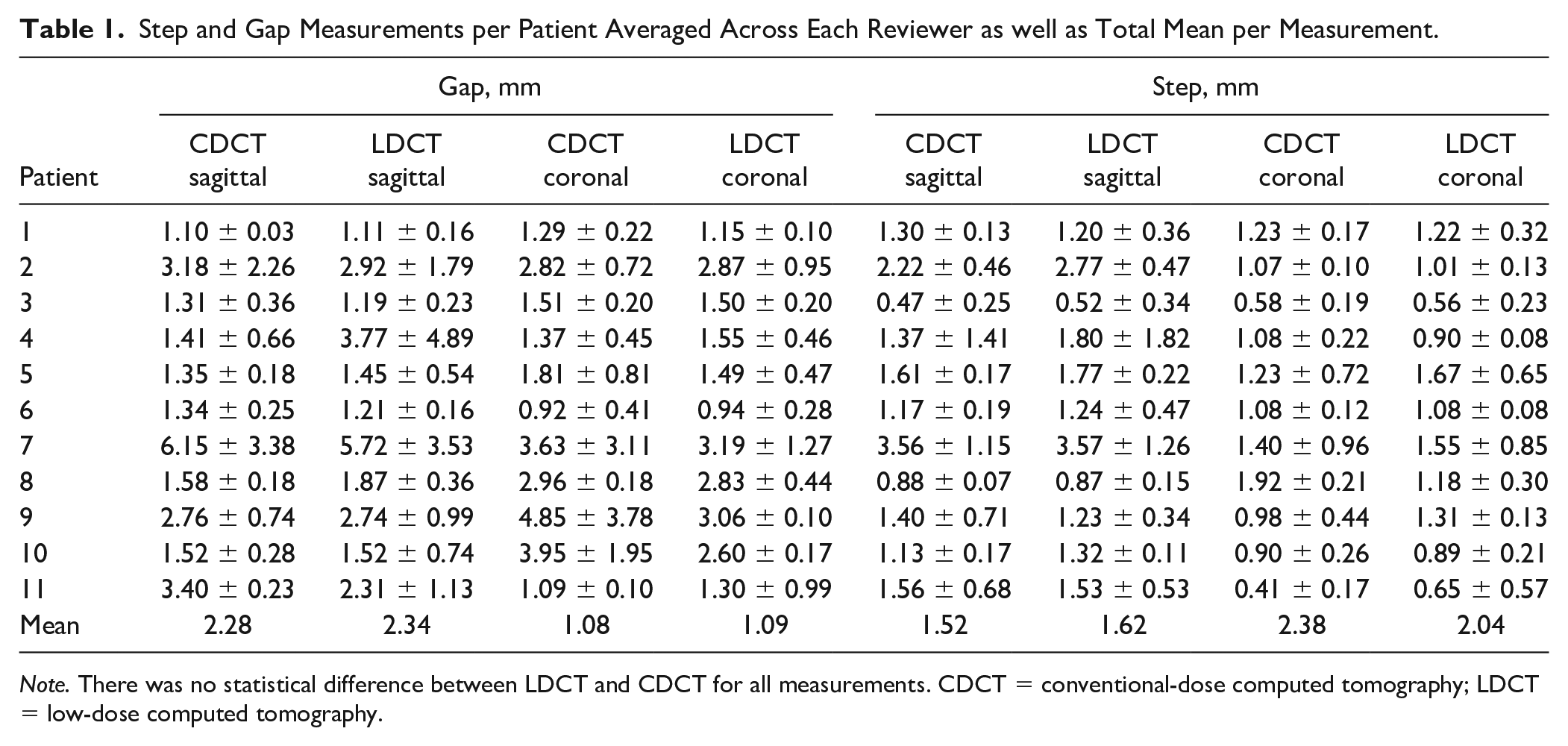
Note. There was no statistical difference between LDCT and CDCT for all measurements. CDCT = conventional-dose computed tomography; LDCT = low-dose computed tomography.
The ICC was calculated for the interrater reliability of the fracture measurements. We examined separate reliabilities looking at all reviewers in addition to comparing reviewers of different training levels. Overall, the pair of measurements taken in the sagittal view at a CDCT had the highest ICC values at 0.561 for the step measurement and 0.553 for the gap. These were considered moderately reliable. The lowest pair of measurements, of ICC values, was the coronal step (0.394) and gap (0.326) measurements at a CDCT. At LDCTs, we found an ICC value of 0.526 for the step and 0.248 for the gap measurement in the sagittal view. For the low-dose coronal view, we found an ICC value of 0.312 for the step and 0.628 for the gap measurement.
We found varying levels of reliability when comparing measurements taken by reviewers with different levels of training. We opted to only examine reliabilities for the coronal gap measurements at the LDCT, as these had the highest overall reliability (ICC = 0.628). We found the highest level of reliability was between the student and resident measurements at 0.831. There was moderate reliability (ICC = 0.56) between the attending and resident, and the lowest reliability (ICC = 0.435) was seen when comparing the student and attending.
Discussion
The use of CT has increased over the past several decades because of its proven utility in multiple medical and dental applications.16,17 As the relative frequency of CT use has increased, a growing interest in reducing the radiation dose imparted to patients has emerged. This is evidenced by the American College of Radiology’s Appropriateness Criteria, which was started during the 1990s to better guide the appropriate use of imaging technologies. Reduction in radiation exposure to patients can be achieved via strict indications for the use of ionizing radiation, as well as modulation of the delivered radiation dose such that the lowest achievable dose of radiation which provides images of sufficient diagnostic quality is used (the As Low As Reasonably Achievable method).18-20 The relationship between ionizing radiation and future cancer risk remains controversial, and a source of considerable debate in the literature.21-23 However, most treating physicians would agree that if opportunities exist to reduce effective radiation dose to patients under their care, this would be desirable provided that their ability to provide high-quality care is not impeded.
The validity of an LDCT scanning protocol has already been shown in the setting of other traumatic fractures. Hamard et al 24 demonstrated that an ultra–low-dose protocol was able to better detect spine and pelvis fractures when compared with radiography of the same effective radiation dose. In addition, Rozema et al 25 showed the efficacy of a low-dose, multidetector CT in unilateral zygomaticomaxillary fractures. Our study adds to these efforts by reducing radiation exposure in patients undergoing CT imaging for DRFs. Our described protocol demonstrated that LDCT and CDCT have a similar diagnostic capacity in DRFs for assessment of articular step and gap displacement. Furthermore, our findings were consistent in both the sagittal and coronal views.
Although plain radiographs remain the gold standard for initial imaging of DRFs, they may not always demonstrate the desired detail of periarticular fractures and are limited to two dimensions. Overall, CT has become a useful tool to assess articular involvement, which is critical in preoperative evaluation and planning. However, preoperative wrist CT examinations are ordered at the discretion of the treating surgeon and may be underused due to cost and/or radiation dose concerns. This practice pattern was before the advent of LDCT, and we hope that our data lower surgeons’ thresholds for ordering additional preoperative imaging in cases where it would potentially benefit the patient.
Our study included 4 different reviewers at various training levels, ranging from student to attending. We found that LDCT is an adequate diagnostic tool for specific preoperative measurements in the setting of DRFs, as evidenced by the lack of statistically significant differences between step and gap measurements between LDCT and CDCT in multiple views. Regarding the moderate to poor interrater reliability, these findings are consistent with the current literature as Gibbs et al 26 also reported low interobserver agreement in the LDCT assessment of acetabular fracture displacement. However, low reliability challenges the overall efficacy of LDCT in DRFs. Misinterpretation can lead to false negatives such as failing to recognize a fracture. One possible explanation may be our reviewers’ wide range of training and experience. Future studies that investigate the optimization of LDCT in DRFs should be performed with reviewers of similar training levels to further validate this technique.
Cone beam CT (CBCT) is another imaging modality that is of interest for its generally lower radiation dose. Commonly used in dentistry and maxillofacial imaging, CBCT provides submillimeter resolution and radiation exposure 10 times less than CDCT. 27 In addition, CBCT has been shown to provide high-fidelity assessment in the distal radius and scaphoid fracture morphology. 28 Currently, there is no evidence to our knowledge that compares the efficacy of CBCT versus LDCT in DRFs. Based on our findings, however, we believe that LDCT represents a viable low-radiation imaging modality for clinicians who do not have access to CBCT at their institution.
There are several limitations to this study. The current analysis is based on a small sample size from a single institution. Another limitation is that representative slices of each fracture were preselected for review by attending surgeons. It is possible if reviewers were given access to all images that they would have selected other images, affecting fracture measurements. In addition, we only looked at the fracture gap and step in the radiocarpal joint. We did not look at fracture size, which also may be important in surgical decision-making and we did not look at the sigmoid notch of the distal radial ulnar joint. Finally, our interrater reliabilities were likely impacted by the heterogeneous training levels of our reviewers. We strongly suggest that any future studies place a strong emphasis on acquiring reviewers of the same training level, preferably that of a fellowship-trained attending, to eliminate any potential bias from differences in experience.
Conclusion
In conclusion, we demonstrated that our LDCT wrist protocol provides comparable imaging quality as CDCT without substantial diagnostic decay for preoperative planning in the setting of DRFs. This comes with the added benefit of a 10-fold reduction in radiation dosage to patients. Our results suggest that LDCT is an opportunity to reduce the effective radiation dose for patients although also providing clinicians with beneficial preoperative imaging for intraarticular DRFs. Further studies that optimize the use of LDCT in patients in intraarticular DRFs should emphasize its reliability among reviewers of similar training levels.
Footnotes
Acknowledgements
Daniel Lorenzana, MD.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.S.K. is a paid consultant for Acumed LLC, a paid consult with stock options for Restore3d, and a paid consultant for Smith and Nephew. All other authors declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.