
Abstract
Background:
Disparities in social determinants of health (SDH) have been shown to play an increasingly important role in the equitable delivery of health care. Distal radius fractures (DRFs) are among the most common upper-extremity injuries encountered. This study aims to examine the influence of economic, educational, social, environmental, and healthcare disparities on management of these injuries.
Methods:
PearlDiver Mariner insurance claims database was analyzed for treatment patterns of DRF in patients aged 18 to 65 years based on the presence or absence of social determinants of health disparities (SDHDs). Outcome variables included the primary mode of management of DRF, including operative versus non-operative, as well as concomitant procedures. Multivariate logistic regression was used to compare fracture management modality in patients with and without SDHDs.
Results:
Of 161 704 patients identified with DRF, 38.3% had at least 1 reported SDHD. The majority of SDHDs were economic. Patients identified with 1 or more SDHDs had a higher medical comorbidity index. Patients with environmental SDHD were more likely to receive non-operative management. Within any SDHD and economic subgroups, odds of operative management were higher. No relationship was identified between SDHD and concomitant procedures.
Conclusions:
The presence of environmental disparities in SDH may predispose patients disproportionately to non-operative management. The presence of SDHDs may influence medical decision-making in favor of open reduction and internal fixation in patients with DRF treated operatively. In treating at-risk populations, providers should be aware of the potential for implicit bias associated with SDHDs and prioritize shared decision-making between patients and physicians.
Introduction
Distal radius fractures (DRFs) are one of the most common fractures seen in adults with an incidence of 16.2 per 10 000 person-years in the United States and an annual estimated cost burden approaching $247 million in the age-over-65 cohort alone.1,2 Selection of a treatment modality for DRF is multifactorial, including both patient-specific factors (age, comorbidities, bone health, occupation, avocations, and so on) and fracture-specific factors (fracture morphology, stability, and so on). Over the last decade, rates of non-operative management for DRF have declined from 86% to 77.5%, with a concomitant rise of operative fixation, most commonly in the form of open reduction and internal fixation (ORIF).3,4
Social determinants of health (SDH) are the physical and environmental conditions, the community and social contexts, the socio-economic factors, and health care systems that can influence health outcomes and costs. Social determinants of health vary significantly from individual to individual and can lead to a range of disparities that ultimately lead to inequitable health outcomes. 5 Disparities in social determinants of health (SDHDs) are classified into educational, economic, environmental, healthcare, and social categories. Developmental delays, low literacy rates, and inadequate education all contribute to educational disparities. Economic disparities are characterized by hardships involving unstable employment, housing, and finances. Environmental disparities include exposure to unsafe toxins, disasters, and safety concerns such as abuse and assault. Healthcare disparities include inadequate access to healthcare services or health insurance coverage. Social disparities encompass cultural, racial/ethnic, and legal challenges.
Disparities in social determinants of health were found to be prognostic of poorer outcomes following operative intervention, including increased rates of postoperative complications, re-admission, reoperation, and longer length of postoperative stay following both elective and trauma-associated orthopedic procedures.6 -8 Despite evidence that SDHDs may contribute to adverse events, increased healthcare costs, and poor patient-reported outcomes associated with medical and orthopedic conditions, little is known about how these educational, economic, social, environmental, and healthcare disparities may influence the medical decision-making for treatment of DRF.
The present study was designed to investigate the relationship between the presence of disparities in social determinants of health and the mode of management, operative and non-operative, for the treatment of adult patients of the age range 18 to 65 years with a diagnosis of DRF. Secondary endpoints of the study were the relationship of patient-specific factors and comorbidity index with SDHD. The existence of a relationship between SDHD and treatment decisions for DRF could indicate the presence of implicit bias among care providers that may warrant further investigation.
Methods
Data Source
This study was conducted utilizing PearlDiver (PearlDiver Inc, Colorado Springs, Colorado; www.pearldiverinc.com) patient records database, which contains de-identified, anonymous, and Health Information Portability and Accountability Act–compliant Mariner private payer, Medicare, and Medicaid patient records from 2010 to 2018. The database contains approximately 20 million patients and utilizes International Classification of Diseases, 9th Revision (ICD-9) and 10th Revision (ICD-10) and procedures or Current Procedural Terminology (CPT codes) to create retrospective cohorts. The records available for analysis by the database are de-identified, anonymous, and compliant with the privacy rules of the Health Information Portability and Accountability Act and were therefore exempted from review by the institutional review board at our institution.
Study Population
The database was queried for DRFs in patients of ages 18 to 65 years from 2010 to 2018 who received either operative or non-operative treatment as defined by ICD-9, ICD-10, and CPT codes seen in Supplemental Table 1. Filters for first instance of fracture and insurance coverage through 1 year following fracture claim were applied to control for complications from prior fractures and patient loss to follow-up, respectively. Within the DRF population, patient groups were created based on the presence or absence of SDHD. International Classification of Diseases 9th and 10th Revision diagnostic code specifications were developed utilizing definitions from the Agency for Healthcare Quality and Research through the Department of Health and Human Services (https://www.ahrq.gov/sdoh/index.html) and as described by Kamalapathy et al 7 and Khalid et al. 9 Distal radius fracture cohorts were identified without any SDHD or with the presence of any SDHD category (any SDHD group) as well as category-specific groups representing economic, educational, social, environmental, and healthcare disparities. Subsequent queries were used to gather demographic information, including gender and age, as well as comorbidity data for each group (see Table 1).
Demographics and Patient Factors Associated With Distal Radius Fractures.
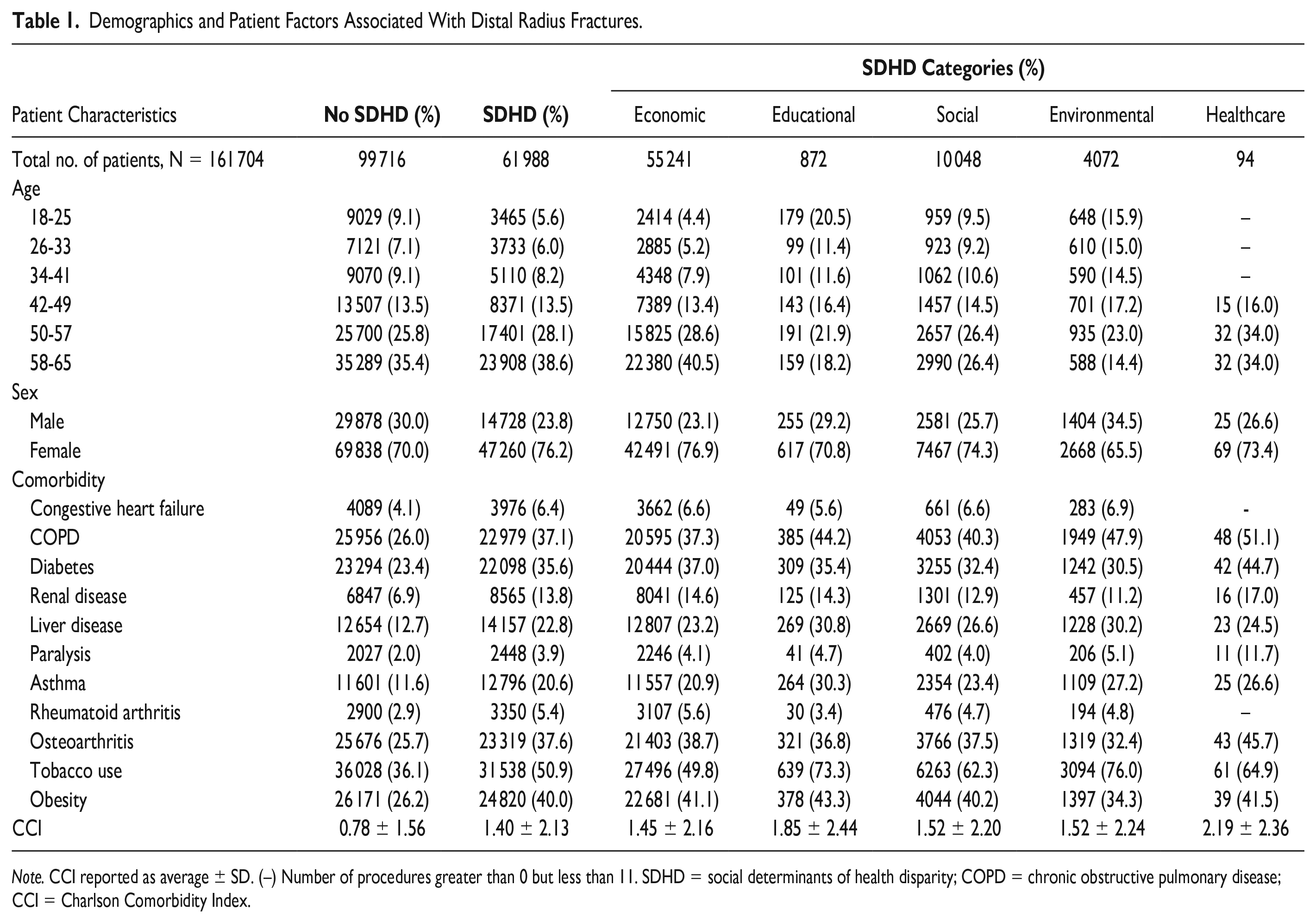
Note. CCI reported as average ± SD. (–) Number of procedures greater than 0 but less than 11. SDHD = social determinants of health disparity; COPD = chronic obstructive pulmonary disease; CCI = Charlson Comorbidity Index.
Outcomes
The primary outcome variables of the study were the primary DRF management as non-operative versus operative. Secondary variables included the use of any concomitant procedures, including carpal tunnel release, wrist arthroscopy, distal radioulnar joint (DRUJ) reconstruction, wrist capsulorrhaphy, and bone graft placement, performed on the same day as operative management. Operative management was stratified into ORIF, external fixation (EF), and closed reduction percutaneous pinning (CRPP). Non-operative management was classified by procedural codes including closed reduction. International Classification of Diseases 9th and 10th Revision procedural codes and CPT codes for fracture management are presented in Supplemental Table 1. Procedural queries were filtered to exclude any operative or non-operative management that occurred more than 60 days following fracture diagnosis. Patients who received both operative and non-operative treatment within 60 days of fracture diagnosis were considered operative management outcomes. Results were presented as totals, percentage of group population, and odds ratios (ORs).
Statistical Analysis
Utilizing RStudios statistics software (R Foundation for Statistical Computing, Vienna, Austria) embedded in the PearlDiver program, multivariate logistic regression was used to produce ORs comparing fracture management in SDHD groups to management in those without SDHD, adjusting for age, gender, and each comorbidity (see Table 1). Confidence intervals (CIs) were presented as 95% Wald CIs based on asymptotic normality. Data cells with greater than 0 and less than 11 occurrences were not displayed in accordance with OptumLabs policy. Values of P < .05 were considered statistically significant.
Results
Descriptive Characteristics
The database query captured 161 704 patients who received either operative or non-operative treatment for DRFs. Of the patients, 61 988 (38.3%) had at least 1 SDHD, and 99 716 (61.7%) had no disparities. The most common disparity seen within the SDHD population was economic disparity (n = 55 241, 89.1%), followed by social (n = 10 048, 16.2%), environmental (n = 4072, 6.6%), educational (n = 872, 1.4%), and healthcare (n = 94, 0.2%) disparities.
The average CCI score was greater in the any SDHD group (CCI 1.40; SD 2.13) and all SDHD subgroups than in the non-disparity group (CCI 0.78; SD 1.56). Specifically, patients with healthcare disparities presented with the worst average CCI (CCI 2.19; SD 2.36). Patients in all SDHD groups had higher percentages of each comorbidity assessed in this study than in those without SDHD. The top comorbidities were tobacco use (50.9% vs 36.1%), obesity (40.0% vs 26.2%), chronic obstructive pulmonary disease (COPD) (37.1% vs 26.0%), and osteoarthritis (37.6% vs 25.7%).
Operative Management
Among patients with a DRF who underwent non-operative or operative management, patient totals (Table 2) and associated ORs (Table 3) for primary management are shown. Patients in the any SDHD group (OR 1.03; 95% CI 1.01-1.06) and economic disparity group (OR 1.04; CI 1.02-1.07) were more likely to be treated with operative management than their non-SDHD counterparts. However, patients with environmental disparities were more likely to receive non-operative management (OR 1.14; CI 1.07-1.22). Looking further into specific procedures within operative management—ORIF, EF, and CRPP—a higher rate of management with ORIF was seen in the any SDHD group (OR 1.05; CI 1.03-1.07) and economic disparity group (OR 1.06; CI 1.04-1.08) than in patients without SDHD, and a lower rate was seen in the environmental disparity group (OR 0.91; CI 0.85-0.97). Management with EF was more prevalent in the any SDHD group (OR 1.13; CI 1.06-1.20) and economic subgroup (OR 1.16; CI 1.08-1.23) than in the no disparity group. Closed reduction percutaneous pinning was less commonly utilized in patients with any SDHD (OR 0.90; CI 0.85-0.95), economic disparity (OR 0.91; CI 0.86-0.96), and social disparity (OR 0.83; CI 0.75-0.93) groups.
Management Totals for Distal Radius Fractures.
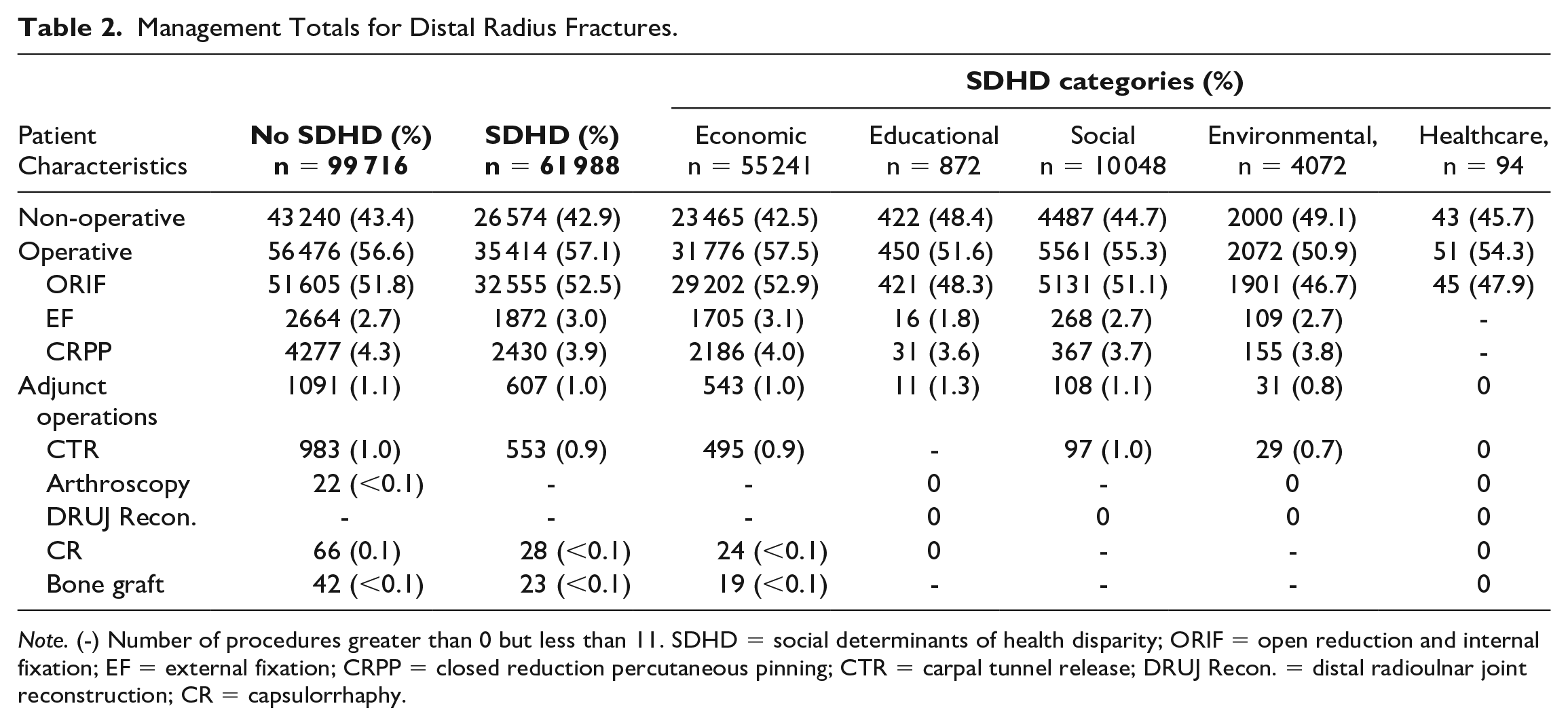
Note. (-) Number of procedures greater than 0 but less than 11. SDHD = social determinants of health disparity; ORIF = open reduction and internal fixation; EF = external fixation; CRPP = closed reduction percutaneous pinning; CTR = carpal tunnel release; DRUJ Recon. = distal radioulnar joint reconstruction; CR = capsulorrhaphy.
Management Odds Ratios for Distal Radius Fractures.
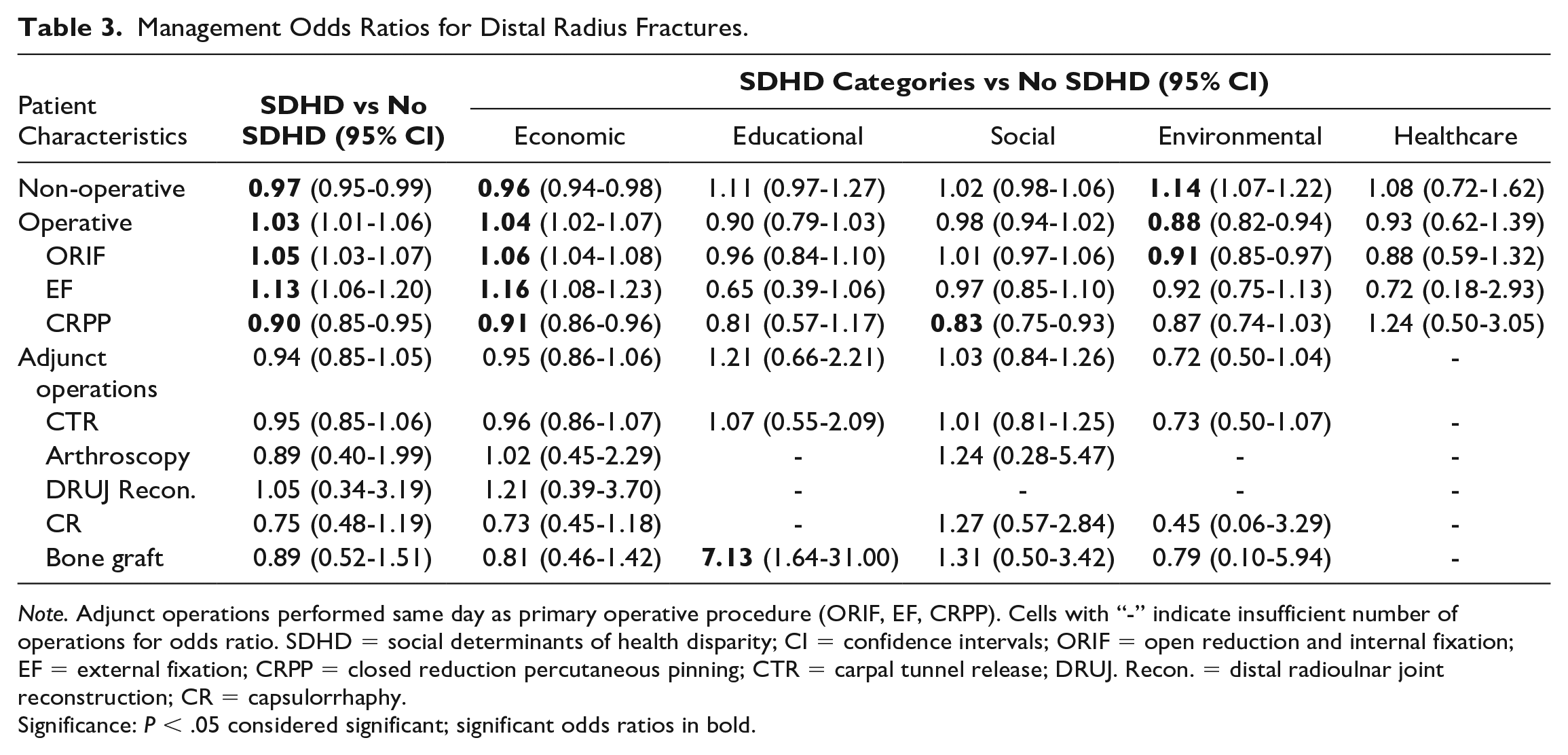
Note. Adjunct operations performed same day as primary operative procedure (ORIF, EF, CRPP). Cells with “-” indicate insufficient number of operations for odds ratio. SDHD = social determinants of health disparity; CI = confidence intervals; ORIF = open reduction and internal fixation; EF = external fixation; CRPP = closed reduction percutaneous pinning; CTR = carpal tunnel release; DRUJ. Recon. = distal radioulnar joint reconstruction; CR = capsulorrhaphy.
Significance: P < .05 considered significant; significant odds ratios in bold.
Concomitant Procedures
With respect to concomitant procedures (Tables 2 and 3), bone graft placement was more commonly reported in patients with educational disparities (OR 7.13; CI 1.64-31.00); however, no differences were noted comparing the presence or absence of any SDHD and concomitant procedures overall.
Discussion
We investigated the relationship between the presence of disparities in social determinants, including factors associated with educational, economic, environmental, healthcare, and social challenges to care, and the mode of management of fractures of the distal radius in adults of the age range 18 to 65 years. Disparities in social determinants of health are common in patients with DRF, accounting for more than one third of patients. The majority of SDHDs are economic, which include employment, income, and poverty-associated barriers to care. Distal radius fracture patients identified with any SDHD had an increased medical complexity reflected by increased medical comorbidities rates.
In similar studies investigating the effect of SDHD on postoperative outcomes, economic disparities are consistently the most common with rates as high as 94% of the observed SDHD.7,9 -12 The frequency of economic disparities with relatively low rates of reported educational, environmental, social, and healthcare components of SDHD highlights the potential for under-reporting of other SDHD categories. Economic disparities, such as poverty status and unemployment, are easier to track and often included in patients’ medical records or available through agencies or the Census Bureau. However, the other categories of SDHD rely on direct patient survey or reporting by physicians, nurses, or social workers for data collection. 13 Potential issues that may contribute to underestimation of the disparity burden on patients include the time requirement for administration and completion of these surveys, patients’ comfort level reporting disparities, lack of standardized data collection within the healthcare setting, and outdated diagnostic codes lacking specificity for SDHD.13 -15 Specifically in our study, surveying a health insurance database does not capture the uninsured population leading to further underrepresentation of disparities.
Our results showed a higher comorbidity burden for all SDHD groups with DRF. Previous studies have also associated SDHD with lower overall health status, higher rates of musculoskeletal disorders, and increased frequency of type 2 diabetes along with greater likelihood of drug and alcohol abuse and increased psychological distress.16 -19 Even without consideration of treatment differences that might occur within this population with SDHD, comorbidities alone highlight the increased healthcare risk these patients face.
The presence of SDHD was associated with differences in the utilization of operative management of DRF. When investigating rates of DRF treatment, our study found an increased likelihood of patients with environmental disparities receiving non-operative management. In contrast to management trends for patients with environmental disparities, patients in the any-SDHD group and those within the economic disparity subgroup were more likely to receive operative management than patients without SDHD. Decisions around conservative versus surgical fixation of DRF are certainly multifactorial, including radiographic fracture morphology, degree of displacement, associated bone quality along with patient-specific factors such as age, desire for functionality, and length of recovery. 20 Causation cannot be determined regarding the reasons behind the higher rate of non-operative management in patients with environmental disparities or operative management in the economic subgroup, but this was not the primary goal of our study. In addition, the environmental group did represent the smallest reported SDHD of all disparity subgroups. However, a more important factor to highlight is that several studies on the association between SDHD and surgical outcomes have noted increased postoperative complications and increased length of stay in patients with SDHD compared to patients without disparities.9,12,21 In addition, Kamalapathy et al 7 found in their study on SDH in orthopedic fracture care that environmental disparities, specifically, were associated with increased odds of re-admission within 90 days following ankle surgery. In a review on socio-economic determinants in bone health, Miszkiewicz and Cooke 22 found that individuals with lower socio-economic status seem to incur fractures at an earlier age in addition to having decreased quantity and quality of bone with age. Likewise, Singh et al 23 demonstrated increased rates of fragility fractures among individuals with poorer living conditions. This suggests a potential inherent susceptibility to more severe fractures in patients with SDHD. While exact reporting of SDHD remains imperfect and a conclusive statement regarding mode of management cannot be drawn, an emphasis on patient and provider recognition of SDHDs will be an invaluable part of healthcare, including optimization of modifiable risk factors and the treatment of DRF.
Research shows that the choice between surgical options is mainly based on a surgeon’s preference for one method over another. 24 Differences to consider among the surgical options include cost, recovery, and complication profile. One prior study investigating the cost of operative management of DRFs demonstrated that, when factoring in unpaid caregiving and loss of productivity, ORIF was the least costly option for operative management, as patients who underwent ORIF returned to work an average of 10 days earlier than patients who underwent CRPP. On the other hand, EF was the costliest. 25 While some evidence supports the use of CRPP, other literature indicates higher rates of postoperative infection than ORIF.26,27 Other studies indicate there is no difference in long-term functional outcome and complications between CRPP and ORIF.28 -31 Our results indicated that odds of CRPP were significantly lower in the any SDHD group as well as in both the economic and social disparity subgroups. In randomized controlled trials comparing CRPP to ORIF, the overwhelming consensus is that ORIF is the management type of choice if patients require a quick return to function.30,32,33 While CRPP is less invasive and provides comparable results, the longer recovery time and additional postoperative needs such as clinic, or even operating room, visits for pin removal may not be feasible for patients battling SDHD.
Secondary outcomes for this study included analysis of concomitant procedures performed on the same day as operative management of the DRF. Common additional surgeries include carpal tunnel release, wrist arthroscopy, DRUJ reconstruction, capsulorrhaphy, and bone graft placement. These procedures serve as prophylactic intervention to reduce postoperative complications associated with DRF, including carpal tunnel syndrome, malunion, and radioulnar joint instability.34 -37 No treatment disparities were found among patients without SDHD compared to the combined SDHD group. However, a significantly higher occurrence of bone graft placement was observed in patients within the educational disparities’ subgroup. As there were a low number of total procedures among the groups, additional studies on the rates of concomitant procedures are needed to conclusively show if patients with disparities receive different operative management.
Overall, assessing differences in the management of DRF patients with and without SDHD is an important, yet complex and multifactorial, issue. Extrapolating causation was not the goal of this study and, therefore, leaves room for future research. Patients often have multiple co-existing SDHDs, making it difficult to decipher which specific SDHD is associated with the outcome of interest. In addition, the degree to which patients are affected by SDHD can be observed along a spectrum, making the evolving nature of SDHD an additional challenge in determining disparities in management.
Limitations in this study are inherent to large database studies and one using an insurance database. The severity of SDHD within this population is unable to be assessed and likely underrepresented. The lack of systematic data collection for SDHD in addition to the lack of diagnostic codes specifically tailored for SDHD also leads to an underestimation of the rate of disparities. In addition, this study was done using compliant Mariner private payer, Medicare, and Medicaid patient records, which fail to include uninsured patients with SDHD who have been treated for DRF. The use of both ICD-9 and ICD-10 codes is another limitation of this study. However, as the period analyzed was from 2010 to 2018, the use of only ICD-10 codes, which were not implemented until 2015, would severely limit the patient population captured within this database study. A targeted area of future research will be to use ICD-10 codes to stratify fracture morphology and severity and compare the differences and roles each plays in DRF management within the SDHD population.
Conclusion
By investigating the impact of SDHD on DRF management and having current, relevant information available to physicians, additional considerations may be given to patients that present with SDHD to ensure equitable management of DRF. Economic disparities are the most often reported factors, but future effort is needed to accurately identify and record additional socio-economic, cultural, and environmental factors that influence patient care. Disparities in social determinants of health are associated with a higher incidence of comorbidities adding complexity to treatment planning. Evidence-based medicine has yet to identify superiority among DRF treatment modalities, but as emerging technologies evolve treatment of DRFs, future studies should aim to identify whether SDHD continue to play a role in medical decision-making. 38 Whether the impact of these disparities on treatment is implicit or not, awareness of potential biases, comorbidities, and patient barriers to healthcare is important for all physicians to appreciate in order to provide the highest quality care.
Supplemental Material
sj-docx-1-han-10.1177_15589447241233369 – Supplemental material for The Impact of Social Determinants of Health on the Treatment of Distal Radius Fracture
Supplemental material, sj-docx-1-han-10.1177_15589447241233369 for The Impact of Social Determinants of Health on the Treatment of Distal Radius Fracture by Graham Grogan, Kristen L. Stephens, Jesse Chou, Jasmina Abdalla, Ryan Wagner, Kacy J. Peek, Aaron M. Freilich and Brent R. DeGeorge in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
The current study was performed with the PearlDiver database using de-identified and publicly accessible insurance records and therefore did not require institutional board review or informed consent at our institution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.