
Abstract
The purpose of this systematic review is to describe the pathoanatomy, presentation, diagnostic workup, treatment modalities, and outcomes of posterior interosseous nerve (PIN) palsy in patients with rheumatoid arthritis (RA). All reported cases of PIN palsy in patients with RA were reviewed to yield 72 cases of PIN palsy in 70 patients. The male-to-female ratio was 1:2.7. Pain involving the elbow was very common (20/33 cases reporting this information), and paralysis or weakness of digit extension was noted in 27/33 cases and 6/33 cases, respectively. Only 1 of the 54 cases undergoing surgical intervention reported persistent weakness, and this 1 patient had undergone a 3-month trial of conservative management. In conclusion, Appropriate pharmacologic management in conjunction with magnetic resonance imaging (MRI) and ultrasound monitoring may be used for conservative management, but surgical decompression should still be utilized for patients with a compressive disease pathology who fail to improve with 6 weeks of conservative treatment, or for those with advanced disease on initial presentation.
Keywords
Introduction
Posterior interosseous nerve (PIN) palsy is a rare complication of rheumatoid arthritis (RA), a chronic inflammatory disease involving predominately synovial joints. Although RA is estimated to be present in 5 per 1000 people, PIN compression is an exceedingly rare complication of the disease, with only 72 cases reported to date. 1 Moreover, optimization of RA disease management is ongoing. Excitedly, recent therapeutic advancements have been estimated to prevent progression of irreversible joint damage in up to 90% of patients with RA. 1
Owing to these pharmacologic advances, a recent decrease in RA morbidity may explain the relative scarcity of RA-associated PIN palsies reported in the literature over the past decade. Despite the publication of multiple systematic reviews and the year-over-year increase in scientific publications, only 3 additional cases have been reported since 2012.2,3
Nevertheless, PIN palsy is a known complication of RA that clinicians should be aware of, particularly in resource-limited environments that may lack access to modern anti-rheumatologic regimens. Prompt treatment of this condition is necessary to prevent long-term disability. The purpose of this review is to provide a concise synopsis of the pathophysiology, presentation, natural history, diagnostic workup, and potential treatments for PIN palsy in rheumatoid patients.
Materials and Methods
Data Sources and Searches
The literature search used EMBASE and MEDLINE and included all studies up through September 2023. Various combinations of the key words “rheumatoid,” “interosseous nerve,” “posterior interosseus,” “deep branch of the radial nerve,” “radial nerve,” “radial neuropathy,” and “supinator syndrome” were used. Database searches were supplemented by a review of reference lists from recent and relevant systematic reviews.
Inclusion/Exclusion Criteria
The inclusion criteria for the studies were as follows: (1) involving a PIN palsy in a patient with known rheumatoid arthritis; (2) did not attribute the PIN palsy to anything other than the patient’s rheumatoid arthritis; and (3) if the full article could not be accessed, had an abstract or equivalent text of sufficient quality to confirm the originality of the case.
The exclusion criterion for reported cases was as follows: if 2 or more studies included the same patient case, the case was only counted once and taken from the original paper.
One author performed an electronic search using EMBASE and MEDLINE. All abstracts with relevant titles were browsed, excluding abstracts with clearly irrelevant titles. If an abstract was found to provisionally meet inclusion/exclusion criteria, the article was accessed and evaluated. If the article was found to still meet the inclusion/exclusion criteria, the study was included. The author additionally reviewed all references from the relevant articles. Texts in French, Czech, German, or Spanish were translated into English using Google translator, a software that has been demonstrated to be a viable tool for this purpose. 4 Articles were identified, screened, and selected for inclusion in the study based on a modification of the PRISMA flow diagram for systematic reviews. 5
Data Collection and Statistical Analysis
Demographic information (age, sex), duration of rheumatologic disease, maintenance therapy regimens at time of presentation, disease classification (seropositive/negative and erosive disease status), PIN palsy treatment duration, treatment modalities (conservative and surgical), treatment response (complete resolution, lingering symptoms with no pursuit of further treatment, or escalation of care), and time to full recovery were obtained. Averages and ranges were reported for quantitative variables.
Due to variable reporting methods used by authors, the following measures were taken: (1) for the 2 cases of bilateral PIN palsy, each patient was counted twice (once for each palsy) in the analysis2,6; and (2) the pretreatment symptom duration unit was days, which was converted from weeks/months reported in some studies.
Results
In total, 123 articles were identified from the electronic search. There were 72 articles that were excluded due to irrelevant titles. Of the 52 remaining studies, 10 were excluded due to irrelevant abstracts, and 13 were excluded as they were reviews or tangentially related topics which did not include any original case of PIN palsy. One article was unable to be accessed but was still assessed for eligibility by screening the abstract. Twenty-eight articles ultimately met inclusion criteria, one of which only the abstract could be accessed. 7 Figure 1 depicts the PRISMA flow diagram for the literature review. A total of 72 cases were found in 70 patients between the years 1965 and 2022. Two of 72 cases had only enough information to support their originality, with no information besides a mentioning of their existence. 8 A Supplementary Table S1 provides a summary of the results.
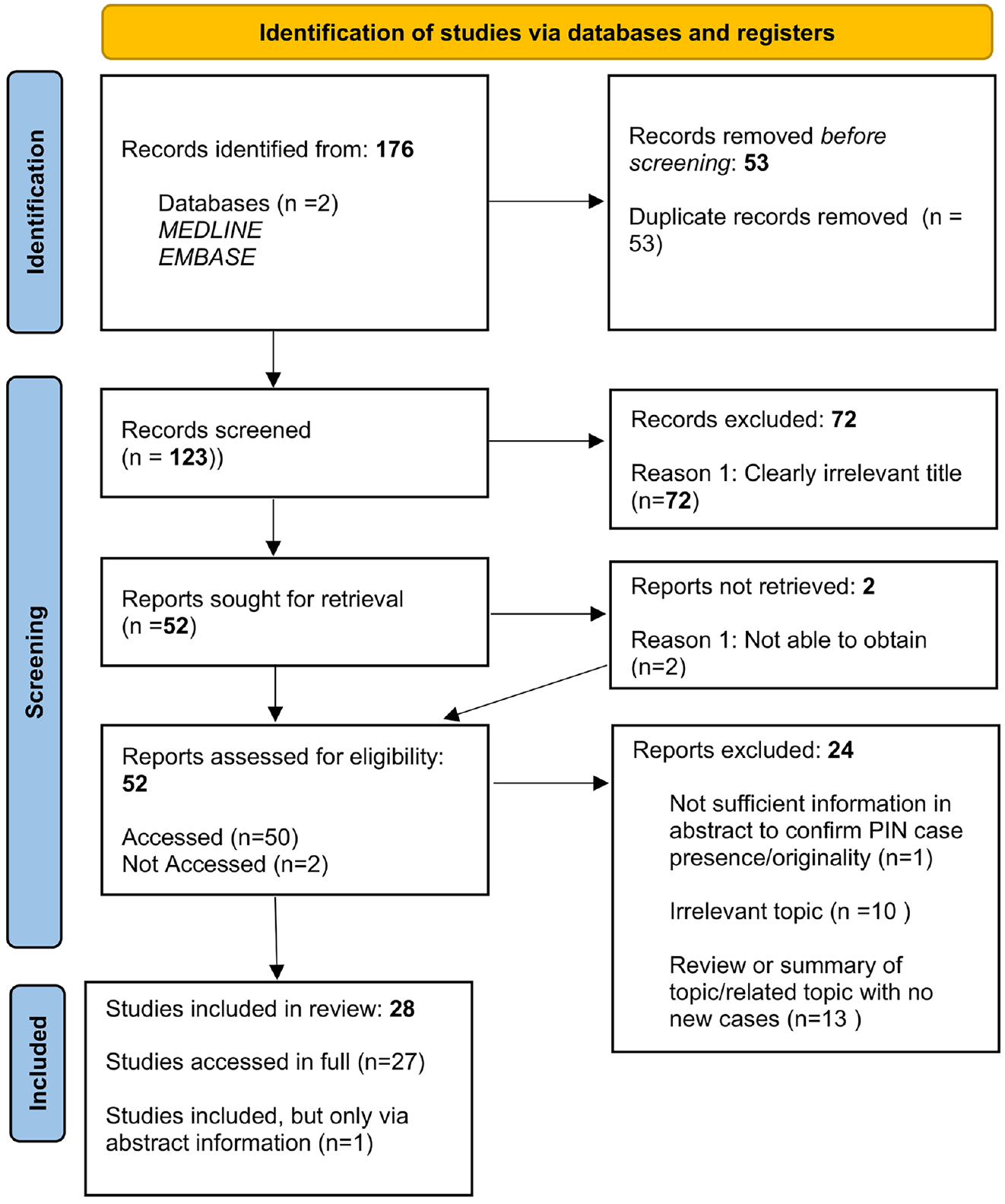
Using the PRISMA flow diagram, 28 articles were ultimately included in the review, with 27/28 being accessed in full.
Demographics
We found a male-to-female ratio of 1:2.7, an average age of 56 years at presentation (range 30-74, n = 33), and average duration of RA prior to presentation of 9.5 years (range 2-20, n = 24).
Presentation
Pain involving the elbow was very common (20/33 cases included this information), and physical examination revealed either paralysis or weakness of digit extension in all cases (27/33 cases and 6/33 cases, respectively). At the time of diagnosis, 4/20 patients were on maintenance therapy with no disease-modifying antirheumatic drugs (DMARDs), 14/20 were on a medication regiment involving at least 1 conventional DMARD, and 2/20 patients were on a regimen involving at least 1 advanced therapy agent. Of these 2, 1 was on adalimumab monotherapy and the other was on combination therapy with etanercept and methotrexate.2,9 Ten of 12 patients had seropositive disease and 13/21 had erosive disease as noted by the authors’ interpretation of elbow imaging or intra-operative pathology. EMG findings were consistent with PIN palsy in 19/22 patients. Two of the 3 negative EMG studies were likely obtained too early in the disease course to demonstrate electrophysiologic changes.10,11 The remaining 1 negative EMG study indicated reinnervation and was used in conjunction with nerve conduction studies (NCS) and other adjuncts to diagnose a vasculitic neuropathy. 12
Treatment
Pretreatment: The average pretreatment duration was 21 days (range 7-304, n = 21). First treatment: Excluding the 2 cases without any reported treatment and 2 cases of advanced disease requiring tendon transfer, 20/68 cases underwent an initial trial of conservative treatment to include any combination of watchful waiting, splinting, medication management, or steroid injection. 48/ 68 cases underwent surgical PIN decompression as the first treatment. Second treatment: Out of the 20 cases that had undergone a conservative treatment trial—excluding 1 case of vasculitis and 1 case of drug toxicity—8/18 eventually had surgical decompression. None of the 48 cases for which surgical decompression was used as the initial treatment reported repeat decompression surgery. Other: 5 of 68 cases had undergone prior dorsal wrist exploration, of which 3 demonstrated intact extensor tendons.13 -15 Two of the 70 cases eventually underwent tendon transfer for advanced disease.13,16
Discussion
Anatomy
The PIN is a continuation of the radial nerve and provides motor innervation to the extensor muscles of the forearm and sensory innervation to the wrist capsule. Along with the superficial branch of the radial nerve, it constitutes the bifurcation of the radial nerve that occurs just proximal to the radiocapitellar joint.17,18 Moving distally, the PIN winds around the radial aspect of the proximal radius and through the supinator muscle, to eventually enter the posterior compartment of the forearm. 17
The radial tunnel, through which the PIN courses on its way to the posterior forearm, is a musculo-aponeurotic furrow extending from the lateral epicondyle of the humerus to the distal edge of the supinator muscle. 18 The roof is formed proximally by aponeurotic expansions from the lateral condyle and the insertion of the extensor carpi radialis brevis and most distally by the superficial head of the supinator. Its floor is formed proximally by the radial head and elbow capsule and distally by the deep head of the supinator.16,18 The entrance to the radial tunnel is a J-shaped fibrous band formed by the proximal edge of the superficial head of the supinator known as the Arcade of Frohse and is the most common location of compression. The fibrous bands originate at the tip of the lateral epicondyle, descend over the elbow capsule and radial head, and insert on the medial aspect of the lateral epicondyle immediately lateral to the articular surface of the capitellum.16,19 Figure 2 demonstrates the course of the radial nerve about the elbow.
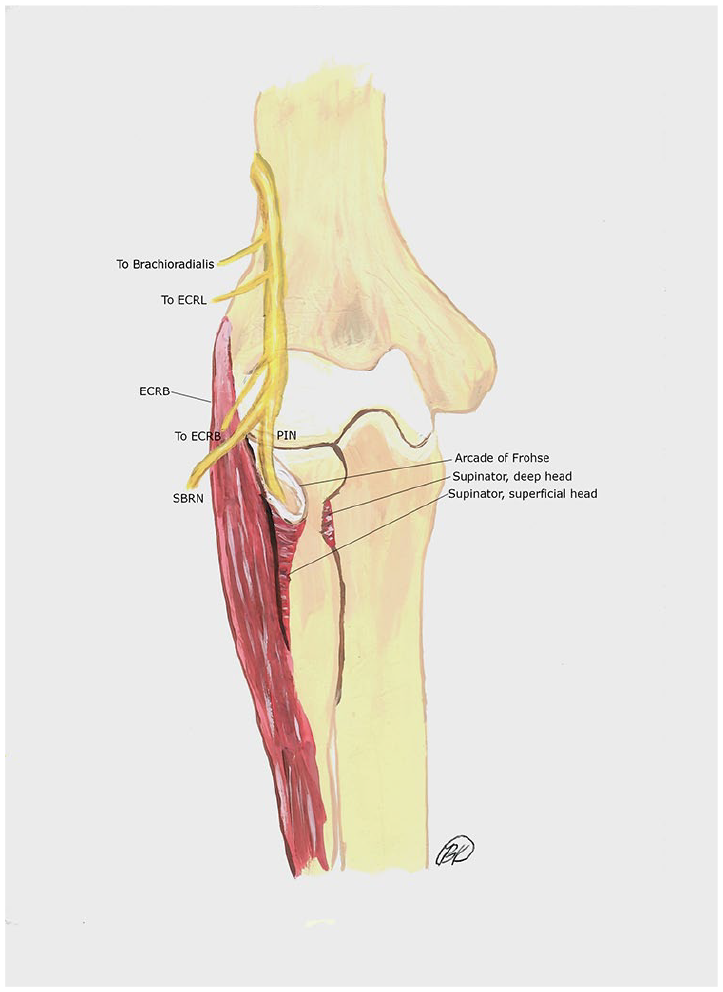
Course of the radial nerve about the elbow.
Pathoanatomy
Muramatsu et al 20 proposed a modification of Chamberlain and Bruckner’s description of RA-associated peripheral neuropathy specific to patients with neuropathies of the forearm and hand: (1) rheumatoid neuropathy directly caused by vascular damage to the peripheral nerve; (2) compression neuropathy secondary to rheumatoid synovitis or swollen joints; and (3) cervical neuropathy caused by cervical spine disorders such as atlantoaxial dislocation.
Isolated PIN palsy in patients with RA may occur due to mechanical compression on the nerve from surrounding structures, vasculitic ischemia, or direct autoimmune neuropathy. Table 1 summarizes the 3 etiologies of PIN palsy in patients with RA, as adapted from Muramatsu’s classification. Since cervical neuropathy will not cause an isolated PIN syndrome, we suggest modifying the classification by replacing cervical neuropathy with autoimmune mononeuropathy, as shown in Table 1.
Classification of Etiologies for Isolated PIN Palsy.
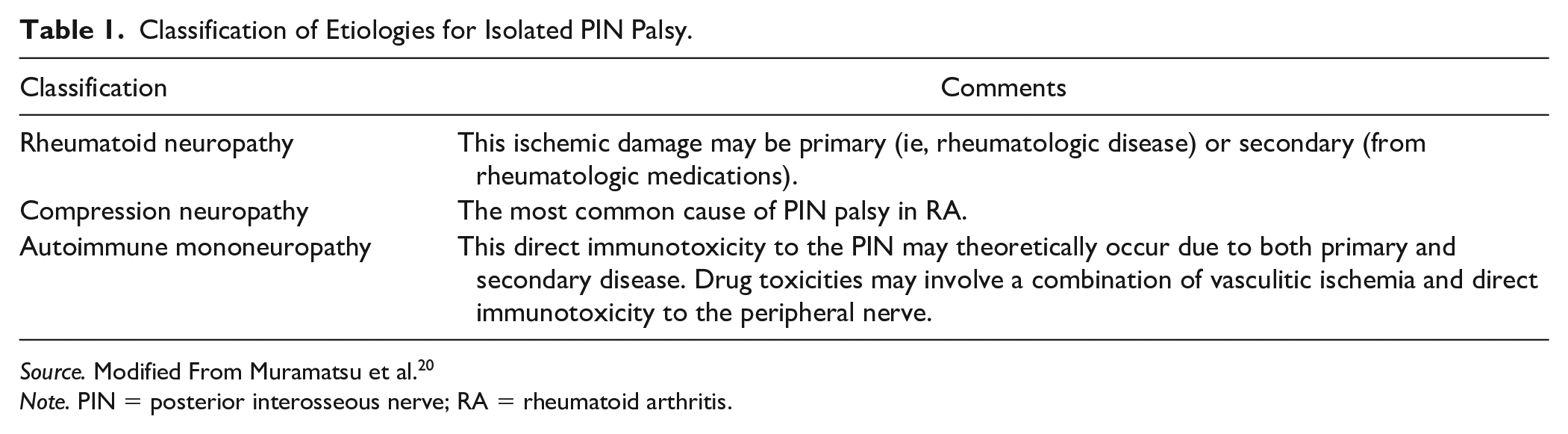
Source. Modified From Muramatsu et al. 20
Note. PIN = posterior interosseous nerve; RA = rheumatoid arthritis.
Nonmechanical Etiologies: Vasculitis and Autoimmune Mononeuropathy
Vasculitis-induced PIN palsy may be caused by both RA itself as well as toxicity to drugs prescribed for RA such as leflunomide, gold, methotrexate, and infliximab.2,9 Anti-TNF alpha treatments have been associated with the development of motor neuropathies and conduction blocks to include PIN palsy, which is thought to be caused by both direct immunotoxicity to the nerve as well as ischemic damage. 21
Mechanical Compression
Anatomic locations of radial tunnel narrowing/inflammation specifically from RA include the elbow capsule (hyperplastic synovium, cysts), local musculature (nonspecific inflammation of the superomedial edge of extensor carpi radialis brevis, deep head of supinator), radius (rheumatoid-associated dislocation), and soft tissue tumors (neuroma).16,18 Despite the various structures within the radial tunnel that may cause narrowing/inflammation, the most common point of PIN entrapment is the Arcade of Frohse. 18 Moreover, Spinner 19 postulated that a tendinous/fibrous Arcade variant as opposed to one that is membranous may be a risk factor for the development of PIN palsy. This variant was found to be present in 87% of cadaveric dissections. 18
History and Physical Examination
Posterior interosseous nerve entrapment should be considered in any patient with long-standing, poorly-controlled RA who presents with weakness of the forearm extensors. Muramatsu and Pallis raised the important points that: (1) physicians tend to focus on joints in RA to the neglect of neurologic impairments; and (2) that the physical examination for patients with RA may be difficult due to chronic joint deformities, limited range of motion, disuse atrophy and even fear of pain.20,22 Nevertheless, a focused physical examination is essential in narrowing the diagnosis and guiding further imaging and treatment modalities.
Muramatsu described the diagnostic constellation of findings for PIN palsy in patients with RA as: (1) severe swelling of the elbow joint; (2) intact sensorium in the hand; (3) intact tenodesis effect; (4) absence of severe deformity at the wrist and metacarpophalangeal (MCP) joint; and (5) EMG demonstrating intact wrist extensors with denervation potential of the finger extensors. 20
At initial presentation, pain involving the elbow is very common. Synovitis of the elbow is also common and may be appreciated by palpating for the sulcus between the radial head and the capitellum. 23 Characteristically, physical examination will reveal paralysis or weakness of digit extension. There should also be intact, but possibly weakened, wrist extension with radial deviation due to the innervation of the extensor carpi radialis longus (ECRL) and brevis (ECRB) by the radial nerve proximal to the Arcade. 23 There should be no associated sensory symptoms in the distribution of the superficial branch of the radial nerve, which would point to a more proximal cause such as radial neuropathy, plexopathy, or cervical radiculopathy. 10
The most characteristic electrophysiologic signature is involvement of the extensors with sparing of ECRL, ECRB, brachioradialis, and radial nerve sensorium. However, it should be noted that changes on EMG are not typically observed in the initial weeks after injury.14,24 The appropriate time to obtain EMG studies may be challenging in RA, as it is not a discreet injury, but rather a progressive worsening of the condition over time.14,24 A vasculitic, rather than mechanical, cause should be suspected in patients who present with an acute onset of extensor weakness and associated neuropathic pain. 12 A vasculitic cause may be distinguished from mechanical compression by combined EMG and NCS, which demonstrate the presence of axonal regeneration in the case of vasculitic neuropathy. 12 Drug toxicity should be suspected for symptom appearance within 6 months of treatment initiation—most notably TNF alpha agents—and symptom cessation within 9 months of therapy discontinuation. 21
Extensor paralysis/weakness of the digits may be caused by several other common complications of RA, including extensor tendon rupture or tenosynovitis, MCP joint dislocation, and extensor tendon subluxation. One should also keep in mind that multiple pathologies may coexist with a PIN palsy, as exemplified in 1 case report of a patient with simultaneous MCP dislocation and PIN palsy. 13
It is important to differentiate extensor tendon rupture from PIN palsy, as failure to do so can lead to unnecessary dorsal wrist exploration. Palpation of the extensor tendons, ultrasound, and the presence of intact tenodesis effect are useful for diagnosis. Furthermore, tendon rupture typically has a more acute presentation, whereas PIN entrapment has an insidious onset. Patients with tendon rupture may also have a history of dorsal wrist tenosynovitis, steroid injection, and caput ulnae syndrome. 25 Extensor tendon rupture commonly involves the thumb or ulnar digits, in contrast to PIN palsy, which most often involves all 5 digits simultaneously.21,25
Extensor tendon subluxation is often subacute and exhibits preserved extensor strength when the digit is passively extended. 25 A snap may be felt on physical examination as the extensor tendon subluxates during active motion. An MCP dislocation is best detected on plain films.25,26
Diagnostic Studies
Plain radiographs of the hand, wrist, elbow, and cervical spine are important in establishing the severity and character of rheumatoid disease. Likewise, NCS/EMG is essential in establishing the diagnosis of PIN palsy and in determining the severity of neuropathy for purposes of treatment guidance. 27
In identifying the source of mechanical PIN compression, arthrography has been helpful in the past for visualizing outpouchings and cysts of the elbow synovium but has largely been surpassed by magnetic resonance imaging (MRI) (the last arthrography study was performed in 2004).6,15,28,29 Ogawa et all proposed MRI as the most useful diagnostic modality, as it was the only modality able to detect supinator inflammation and associated soft tissue swelling. 30 Moreover, MRI may be used to identify more upstream pathologies that mimic PIN palsy. In 1 case, it was used to identify a chronic, pure motor axonal plexopathy that was initially misdiagnosed as PIN palsy and resolved with intravenous immunoglobulin. 31 Finally, ultrasound has shown some promise in identifying obvious compressive lesions such as synovial bulging or cysts.3,32 However, more nuanced findings such as increased nerve diameter and hypervascularity on color Doppler may not be as practical for providers who lack extensive ultrasound experience and access to a high-frequency linear array transducer. 33
Treatment
In the past, conservative treatment with medication management and steroid injection has been deemed largely ineffective.6,27 Moreover, there is the fear that a delay in surgical decompression may decrease the chances for recovery following surgical release, as Mulholland demonstrated for PIN palsies. 34
Recent opinion has shifted toward a trial of conservative therapy for PIN entrapment in RA.2,32,35 Vasculitic or drug toxicity etiologies should be managed with medication rather than surgery.9,35 The argument for a trial of conservative treatment for mechanical entrapment has become more attractive by virtue of rheumatoid pharmacologic advancements such as disease-modifying antirheumatic drugs and advanced therapies. In addition, the accessibility to MRI and ultrasound allows for frequent and precise treatment response monitoring, thereby avoiding the question of an optimal trial period.2,23,32,36,37 In patients presenting with a short duration of symptoms, a trial of conservative treatment through a combination of rheumatologic medication management, splinting/passive exercise, cyst drainage, and/or steroid injection with periodic imaging and examination may be used.
Surgery should be considered for patients who fail a conservative trial or for those with advanced disease or prolonged symptoms. Kerschbaumer et al 23 proposed a trial period of no more than 6 weeks by the end of which extensor paralysis should be completely resolved. Changes on EMG are indicative of more advanced neuropathies that have been ongoing for weeks to months. 14 In addition, extreme presentations such as extensor muscle atrophy should prompt PIN decompression to prevent complete paralysis. For patients who fail to improve with PIN decompression or for those with long-standing palsy, tendon transfers may be useful.13,16
The operation itself typically involves exploration and decompression of the PIN with synovectomy, cystectomy, and the excision of any space-occupying lesions. The anterolateral approach is recommended for cases where anterior bulging of the elbow synovium or cubital cysts are present, while a posterolateral approach confers easier access for radial head excision when appropriate.6,29
Although treatment of this disease is complicated and should be tailored to each patient’s unique disease characteristics and clinical presentation/trajectory, Figure 3 depicts a workup and treatment algorithm that may serve as a starting point for creating a personalized treatment plan for these complex patients.
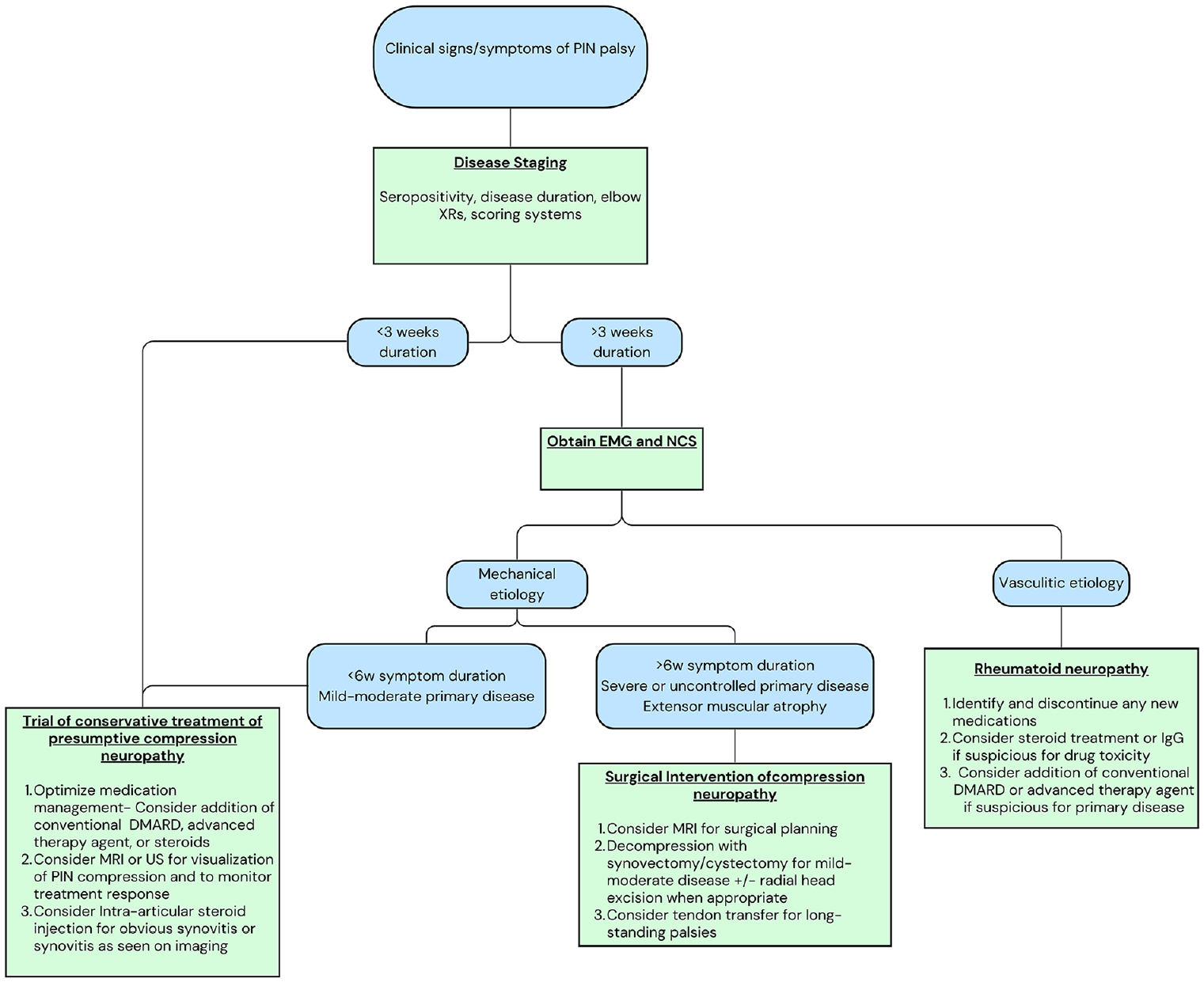
Diagnostic and treatment algorithm for PIN palsy in patients with RA. It should be noted that management of these patients is complex and should involve close dialogue between patient and provider, as well consideration of each patient’s unique disease characteristics.
Limitations
There were several limitations to our study. First, the cases were limited to case series and case reports. Second, the degree of detail with which the cases were described varied in both quantity and content. Specifically, one study in which 2 cases were reported provided no details besides the existence of the cases, and 2 studies reported 31 cases but only reported treatment outcomes (Privat, Popelka, Pallis).8,22,38 Finally, we included cases from the years 1965-2014, a period during which great strides were made in the fields of rheumatologic therapies and diagnostic imaging. Despite these shortcomings, the present study is the most thorough systematic review of PIN palsy secondary to RA and the only one to include cases from the non-English literature. Despite heterogeneities in the selected cases, we hope this review elucidates the history and trajectory of the treatment of PIN palsy in patients with RA, which may help guide management of this complex disease.
Supplemental Material
sj-docx-1-han-10.1177_15589447241260766 – Supplemental material for Posterior Interosseous Nerve Palsy in Rheumatoid Arthritis: A Systematic Review
Supplemental material, sj-docx-1-han-10.1177_15589447241260766 for Posterior Interosseous Nerve Palsy in Rheumatoid Arthritis: A Systematic Review by Brooke Kowalski, Nicholas J. Zarkadis, Mitchell Harris, John Scanaliato and John Dunn in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was irb-exempt”, since it was purely a review of the literature.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This article does not contain any studies with human or animal subjects.
Statement of Federal Employment
Some authors are employees of the U.S. Federal Government and the United States Army. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of Madigan Army Medical Center, Blanchfield Army Medical Center, William Beaumont Army Medical Center, the Department of Defense, or United States government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.