
Abstract
Background:
Despite increasingly wider use, there remains controversy among anesthesiologists regarding preferred formulations and the role of steroid adjuvants in regional anesthesia. There is also uncertainty in the role of dexamethasone when administered directly versus peripherally. We hypothesize that directly mixing dexamethasone into the regional nerve block rather than peripherally administered intravenous dexamethasone will demonstrate a difference in efficacy concerning duration and rebound pain, decreased postoperative pain scores, or opioid consumption within the short-term postoperative period.
Methods:
A prospective, randomized controlled blinded study was conducted for patients undergoing open reduction and internal fixation with a volar plate technique for distal radius fractures. Patients were randomized for their preoperative anesthesia. One group had ultrasound-guided supraclavicular block with ropivacaine with a direct mix of dexamethasone 4 mg (Direct group), while the other group had ultrasound-guided supraclavicular block with ropivacaine and peripheral intravenous dexamethasone 4 mg (Indirect group). Data was collected pre, intra, and postoperatively.
Results:
Fifty patients consented and participated in the study, with 27 participants in the direct group and 23 participants in the indirect group. Compared to intravenous administration, directly administered dexamethasone demonstrated a significant difference in the average time for the block to fade, onset of motor and sensory recovery, and block resolution.
Conclusion:
Our findings prove that directly mixing dexamethasone compared to peripherally administered intravenous dexamethasone will demonstrate a difference in efficacy with regards to duration and rebound pain, but do not prove that there will be a difference in decreased postoperative pain scores or opioid consumption within the 24-hour postoperative period.
Level of Evidence:
Prognosis Level I
Keywords
Introduction
The use of intravenous dexamethasone and a ropivacaine nerve block appears to have occurred in conjunction; yet its efficacy in prolonging nerve block duration when given intravenously versus peripherally is not commonly expressed in the anesthesia community. A supraclavicular block (SCB) with long-acting local anesthetic (e.g. ropivacaine) is commonly used for distal radius fracture surgery; however, at present, this method has been associated with rebound pain and increased opiate consumption during the initial postoperative period.1,2 Dexamethasone has been reported to prolong sensory and motor blockade when administered with a local anesthetic perineurally. 3 This is thought to be mediated by attenuating the release of inflammatory mediators, reducing ectopic neuronal discharge, and inhibiting potassium channel-mediated discharge of nociceptive C-fibers. 4
The efficacy of perineural dexamethasone added to ropivacaine at doses ranging from 1 to 10 mg is well documented. 2 Administering dexamethasone mixed with the local anesthetic has been reported to improve nerve block efficacy and duration, allow for improved postoperative pain scores, and reduce opioid use in the early postoperative period.1-7 However, the best administrative modality to reduce rebound pain and opiate consumption remains unclear, as the efficacy of both intravenous and perineural administration of dexamethasone is still not commonly accepted in the anesthesia community.
The purpose of this study is to test the hypothesis that adjuvant dexamethasone directly mixed into the local anesthetic will exhibit superior efficacy on nerve block duration and rebound pain compared to that of peripherally administered intravenous dexamethasone, yielding decreased postoperative pain scores and longer nerve block duration, and opioid consumption within the 24-hour postoperative period. Second, this study investigates the patient’s opioid consumption in the 24-hour postoperative period, comparing the opioid intake between the group of patients receiving intravenous dexamethasone with those receiving direct dexamethasone in their nerve block.
Materials and Methods
After institutional review board approval, a prospective randomized controlled blinded study was conducted for patients undergoing open reduction and internal fixation of an isolated, closed distal radius fracture with no concurrent injuries. Inclusion criteria were patients over the age of 18 undergoing open reduction and internal fixation of a distal radius fracture less than 3 weeks from injury with a volar plate technique. Patients could take nonsteroidal anti-inflammatory drugs (NSAIDs) for pain control up to 5 days before surgery and bridge with Tylenol subsequently thereafter. All patients were American Society of Anesthesiologists (ASA) class 1 to 3 and cleared for surgery in a stand-alone ambulatory surgery center. Finally, no chronic pain patients were included and no patients using long-term opioids were included. Exclusion criteria consisted of individuals with open fractures; concurrent nerve injuries; a history of drug, opioid, or alcohol abuse; an inflammatory disorder (rheumatoid arthritis, osteoarthritis, etc.); infection, dementia, psychiatric or neurological disorder, relevant drug or local anesthetic allergy; and relevant long-term upper extremity pain disorder (complex regional pain syndrome, fibromyalgia, neuralgia, etc.). Patients who were pregnant or had polytrauma (concurrent scaphoid fracture, ulna fracture, etc.) were also excluded from this study.
After obtaining informed consent, patients were randomized to 1 of 2 treatment groups regarding their preoperative anesthesia through an online randomization generator:
1.
2.
Postoperative oxycodone was electronically prescribed and dispensed to the patient on the date of surgery (DOS), and no sooner. No narcotics were dispensed by surgeons before surgery.
Data were collected at the following time points: preoperatively, immediately postoperatively in the post-anesthesia care unit (PACU), and 24 hours after surgery. Preoperatively, age, gender, hand dominance, involved side, ASA status, time of block administration, and dexamethasone modality were recorded. For the placement of the nerve block, patients received 2 mg midazolam and 100 mcg of fentanyl. All patients received total intravenous anesthesia with propofol intraoperatively.
Postoperatively, the patient’s Visual Analog Scale (VAS) pain score (scaled 1-10) and occurrence of nausea/vomiting were recorded. Incomplete or suboptimal block or pain control was noted both intraoperatively and postoperatively if occurred.
In the PACU, patients were given a pain block diary to fill out postoperative Day 1 through postoperative Day 11 and bring it back to the surgeon during their first postoperative follow-up appointment. The date and time were recorded accordingly.
In addition, patients were instructed to record the time and quantity (number) of prescribed pain pills taken per day, time, type, and amount (in milligrams) of nonprescribed pain pills taken per day, worst pain rating per the VAS (1-10) per day, and average pain rating per the VAS (1-10) per day. The date and time were recorded per patient for the following questions: when the patient first noticed their block wearing off, when the block entirely worn off, when the patient was first able to move their fingers, when the patient first felt sensation/feeling returning to their fingers, and when the patient first noticed any sign of pain.
As per the standard of care at the surgical center, a surgical center nurse called the patient for follow-up 24 hours postsurgery, collecting the following information: the rating of their current pain on a scale from 1 (none) to 10 (worst), pain medication prescribed and how many pills given, how many prescribed pain pills taken thus far, how many other pain medicines taken since surgery that were not prescribed (ibuprofen, acetaminophen, naproxen, etc), and any experience of nausea/vomiting since surgery. Furthermore, the surgical center nurse asked for the recorded date and time of the questions that were on the pain diary 24 hours postsurgery.
Statistical power was evaluated for this study. Based on prior sample size determinations, we concluded that with an average analgesia duration of approximately 22 hours, and an assumed clinically significant difference of 3 hours, 20 patients per treatment group (40 total) would be needed to provide 80% power to conclude the absence of effect at a .05 significance level between treatment groups. To allow for 20% attrition, 25 subjects per group (50 total) was the target for enrollment, which was achieved. Statistical analysis included descriptive statistics in the form of averages and standard deviation. P values < .05 were deemed statistically significant between treatment groups.
Results
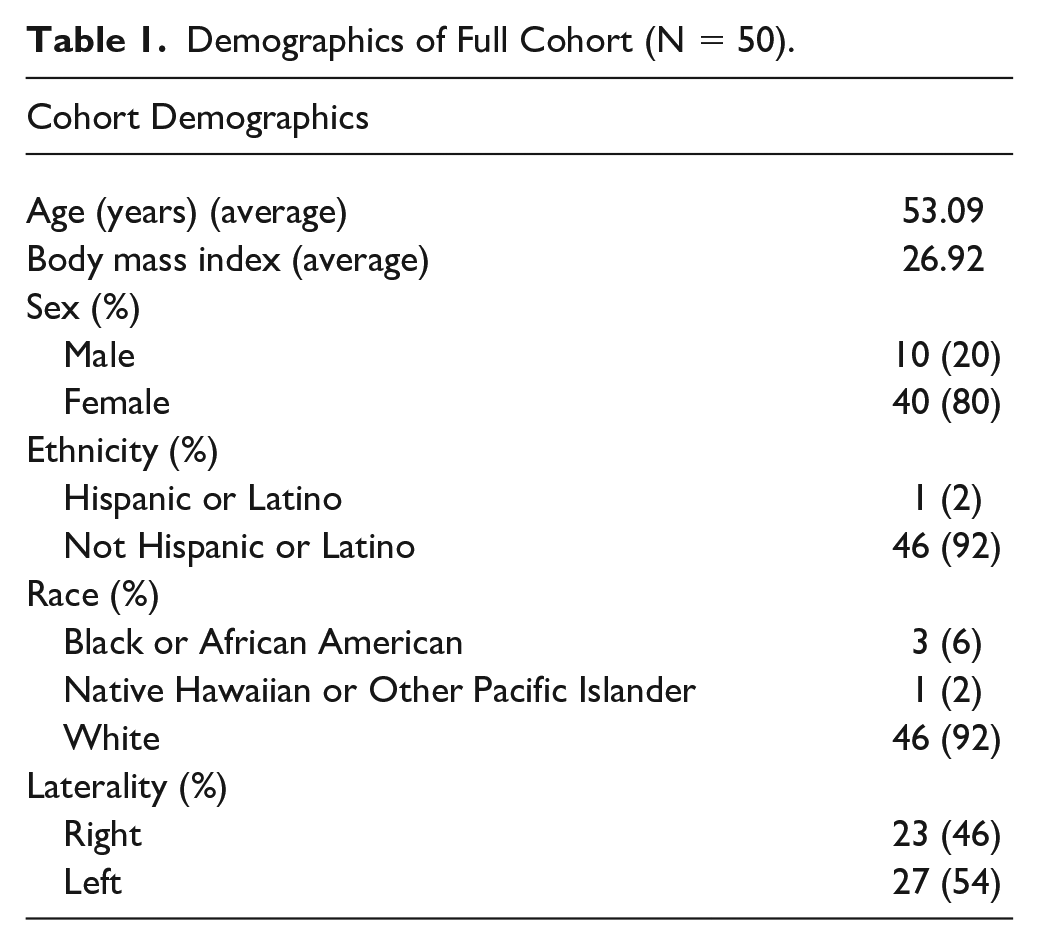
Fifty patients consented and participated in the study, with 27 participants in the direct group and 23 participants in the indirect group. Most of the patients were female, White, not Hispanic or Latino, and had a laterality of the left hand. The average age was 53 ± 16.42 years. The average body mass index was 26.92 ± 5.17. All participants had an ASA level of 2, and the time of the administered block spanned from 8:30 AM to 3:30 PM (Table 1). One patient was excluded for needing a second block in the PACU while another participant terminated their participation prior to returning their pain diary.
Demographics of Full Cohort (N = 50).
Across all participants, the average number of prescribed pain pills taken was 7 ± 6 pills and their average VAS pain post-24-hours was a 3. All participants took over-the-counter pain pills, specifically either NSAIDs (N = 27) and/or Tylenol (N = 15), in addition to the prescribed pain pills. The average time the nerve block wore off was slightly under 16 (15.96 ± 3.77) hours, while the average time patients reported the block was completely gone was slightly above 21 (21.19 ± 4.50) hours. Finger movement and finger sensation averages were similar across patients (17.18 ± 3.42 and 17.43 ± 4.42, respectively). Patients reported the first sign of pain to be at an average of 19.32 hours after the nerve block was administered (Table 2).
Results of Full Cohort (N = 50).
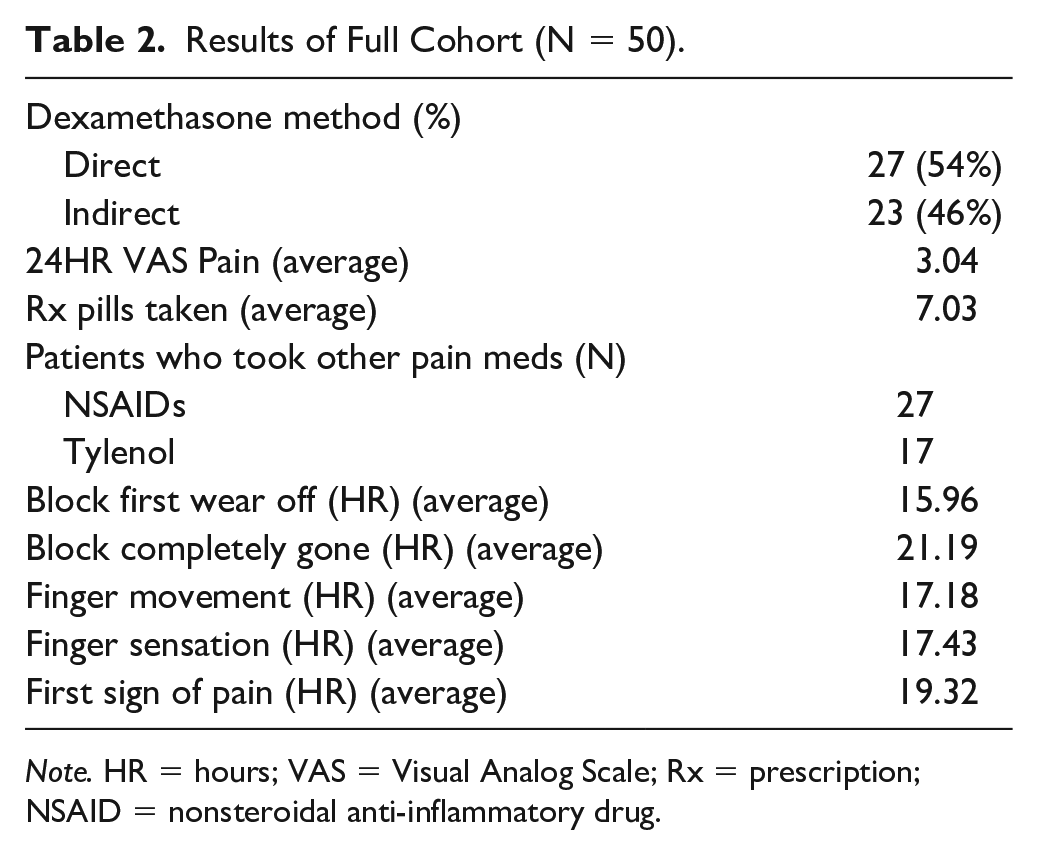
Note. HR = hours; VAS = Visual Analog Scale; Rx = prescription; NSAID = nonsteroidal anti-inflammatory drug.
Between-group analysis is shown in Table 3. Compared to peripheral intravenous administration, directly administered dexamethasone demonstrated a significant difference in the average time for the block to fade (P < .001), onset of motor and sensory recovery (P = .029 and P = .039, respectively), and complete block resolution (P = .001). There was also a significant difference in first sign of pain between groups with the direct group feeling pain after a longer amount of time compared to the indirect group (P < .01). There was no significant difference in prescribed pain pills taken (P = .1136) and postoperative pain felt after 24 hours (P = .376).
Comparison Between Dexamethasone Groups (N = 50).
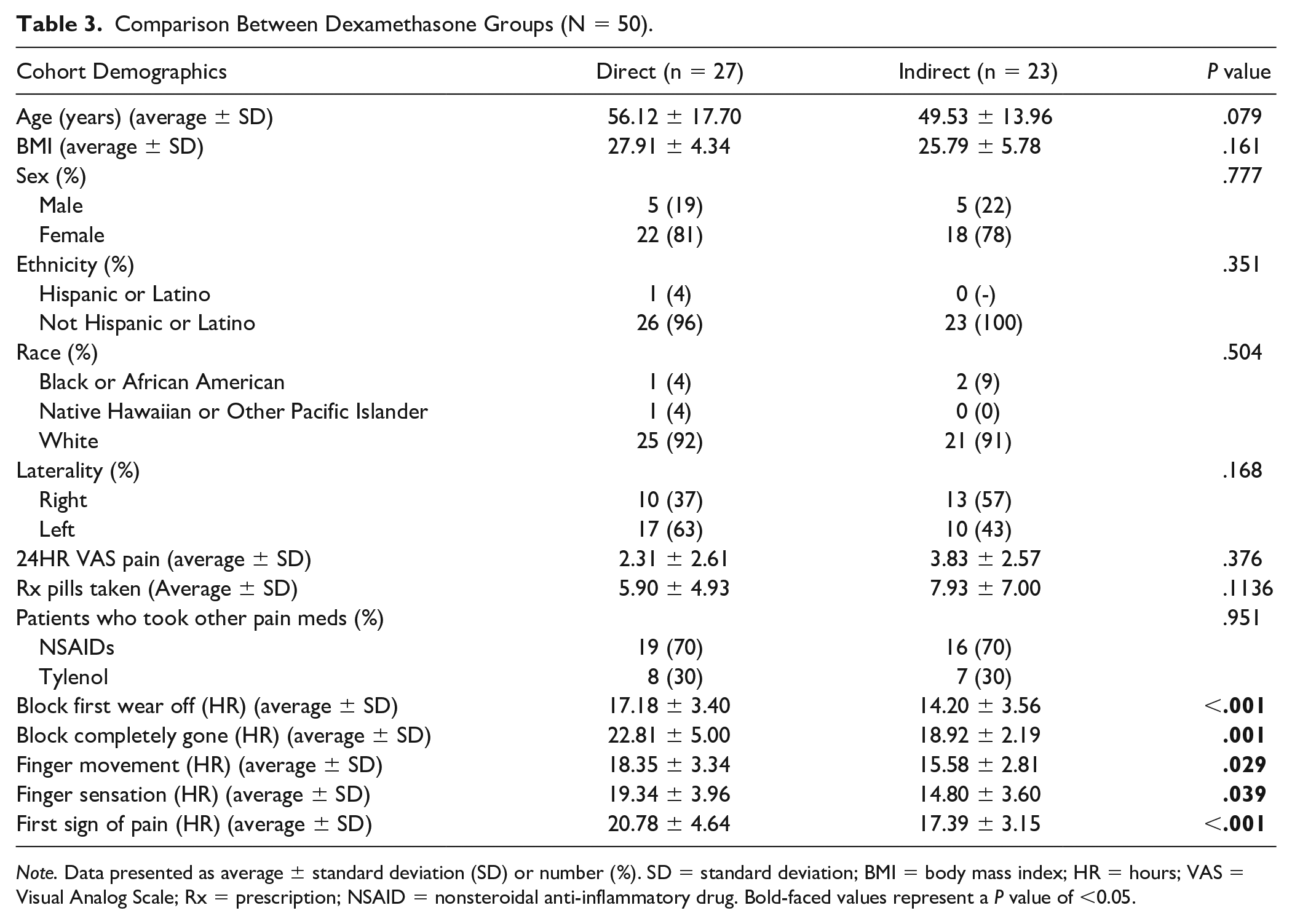
Note. Data presented as average ± standard deviation (SD) or number (%). SD = standard deviation; BMI = body mass index; HR = hours; VAS = Visual Analog Scale; Rx = prescription; NSAID = nonsteroidal anti-inflammatory drug. Bold-faced values represent a P value of <0.05.
Discussion
Prior studies have suggested that perineural dexamethasone mixed with a ropivacaine-based nerve blockade may improve overall block duration and efficacy.1,2,8-12 However, the superiority of such an administrative modality on the reduction of rebound pain and opiate consumption remains unknown, as this direct-mixed method has not been previously compared to the intravenous delivery of dexamethasone in a prospective manner.
A study by Gouda et al established that steroid-adjuvant therapy demonstrated a significant increase in time until the block began to wear off. All steroid study groups also demonstrated a significant increase in the duration of the block before its effects were completely gone when compared with the control group. 2 Our study expanded upon this finding by giving all patients in both groups ropivacaine with dexamethasone to prolong postoperative analgesia, and we did find a significant difference between groups for prolonged analgesia effects.
In addition, Maagaard et al included 16 participants in a randomized study where they compared perineural dexamethasone to systemic dexamethasone and placebo in terms of the duration of sensory nerve block. Maagaard et al 13 found that perineural dexamethasone resulted in greater duration when compared with placebo, but systemic dexamethasone had a similar duration to the placebo. However, they did not directly compare systemic to perineural dexamethasone. Our study did not have a placebo group but instead was focused on comparing peripheral and directly administered dexamethasone. Furthermore, Maagaard et al had an average of 11.8 hours for the perineural block duration and 11.3 hours for the systemic block duration. Both the peripheral and direct groups in our study had an average block duration of just over 21 hours, almost twice the lengths of Maagaard et al, along with having more than 3 times the number of participants. The discrepancy between this study and ours is most likely due to Maagaard et al’s study being focused on the ulnar nerve, while our study included the entire brachial plexus at the level of the supraclavicular artery; thus we were able to use much more volume and, therefore, much more local anesthetic.
Furthermore, several meta-analyses have been produced comparing perineural and intravenous dexamethasone use. Pehora et al evaluated the efficacy of perineural dexamethasone and intravenous dexamethasone. In their review of 9 studies, they found that perineural dexamethasone had a significantly longer duration of sensory block compared to intravenous (MD 3.14 hours, 95% confidence interval [CI]: 1.68-4.59; participants 720; studies 9). Postoperative pain between the 2 treatment groups was not significant, along with no difference in the post-24-hour opioid consumption (MD: −3.87 mg, 95% CI: −9.93 to 2.19; participants 242; studies 4). 14 Similarly, a study by Tan et al 15 found that perineural has a greater duration of analgesia compared to intravenous dexamethasone ([MD]: 2.72 h, 95% CI [1.42, 4.01], P < .001). Our single large institutional study adds to the existing literature that there is a significant difference in the duration of analgesia between perineural and intravenous dexamethasone. Our study furthermore explored the differences between block wearing off, finger movement and sensation, and the first sign of pain, all of which were significantly different.
Limitations of the study include the variability of when the block was administered between patients, thus causing variable times on when the block wore off. In a future study, administering the block, whether peripherally or directly, at the same time of day for every patient may eliminate confounding variables. In addition, if the block was started when patients were asleep, we believe this would contribute to false assumptions about the block duration. Furthermore, data were taken from one institute through the patients of 3 practicing orthopedic surgeons. To increase generalizability, including patients from more physicians and more than one institution can be incorporated into the study methodology in future studies.
Despite limitations, our findings accept the hypothesis that directly mixing dexamethasone into the regional nerve block compared to peripherally administered intravenous dexamethasone will demonstrate a difference in efficacy concerning duration and rebound pain. However, we reject the hypothesis that there will be a difference in decreased postoperative pain scores or opioid consumption within the 24-hour postoperative period.
Conclusion
Our findings accept the hypothesis that directly mixing dexamethasone into the regional nerve block compared to peripherally administered intravenous dexamethasone will demonstrate a difference in efficacy concerning duration and rebound pain. However, we reject the hypothesis that there will be a difference in decreased postoperative pain scores or opioid consumption within the 24-hour postoperative period. For clinicians who do not feel comfortable mixing preservative-containing dexamethasone formulations with their local anesthetic for perineural administration, the option to deliver dexamethasone intravenously remains viable, with added confidence that there is no clinical drop-off in block efficacy or duration. Future studies may consider investigating the effect that the dose of dexamethasone given intravenously plays in prolonging the efficacy and duration of the block as well as the timing of intravenous administration of dexamethasone to the placement of the nerve block.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.