
Abstract
The diagnosis and optimal management of radial tunnel syndrome (RTS) is controversial with little consensus among the many possible pathophysiological mechanisms and surgical approaches. Thus, we performed a systematic review in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines on studies reporting outcomes of surgical treatment for RTS. PubMed/MEDLINE, Embase, Web of Science, and Cochrane databases were queried. Patient demographics, surgical approach, intraoperative findings, postoperative patient-reported outcomes, and complications were recorded and synthesized. We included 11 studies comprising 401 upper extremities (381 patients). Of the included forearms, 54% (n = 155) were approached dorsally, and 46% (n = 130) were approached volarly. Studies that utilized a dorsal approach between the extensor carpi radialis brevis and extensor digitorum communis had the most favorable Roles and Maudsley scores and patient satisfaction when compared with volar approaches. However, volar approaches identified a greater number of constrictions at the arcade of Frohse (19% vs 7%) when compared with dorsal approaches. Wide variability of surgical approaches used for treatment of RTS is present in the literature. Compared with volar approaches, dorsal approaches are associated with favorable reported outcomes. However, in RTS secondary to vascular constriction, volar approaches may be better suited for release.
Keywords
Introduction
Radial tunnel syndrome (RTS) is a compressive neuropathy involving the posterior interosseous nerve (PIN) within or surrounding the radial tunnel of the forearm. 1 While many patients are initially treated conservatively, surgical intervention may be indicated for refractory cases. 2 Multiple surgical approaches have been described to release the compressed PIN; however, there is limited agreement in the literature regarding the efficacy of these surgical techniques and is often decided by surgeon preference.3 -5 Furthermore, there is vast variability in the physician- and patient-reported outcome measures utilized across studies, making evidence-based decisions on best surgical approach difficult.
Potential sites of compression of the PIN have been described to include the arcade of Frohse (the proximal fibrous bands of the superficial layer of the supinator muscle), the leash of Henry (vascular branches from the radial recurrent artery), fibrous bands at the radiocapitellar joint, and tendinous bands at the superomedial margin of the extensor carpi radialis brevis (ECRB), as well as others. 6 Unfortunately, imaging, electromyography (EMG) and nerve conduction studies (NCS), as well as physical examination findings have shown limited utility in reliably and accurately discerning the site of compression and guiding surgical approaches, resulting in variable outcomes. 6
This systematic review aimed to evaluate the efficacy of operative intervention for RTS based on surgical approach. The findings of this review will provide information that will aid surgeons in identifying which surgical approaches are supported by the literature for surgical management of RTS.
Materials and Methods
This systematic review was performed in accordance with the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Eligibility Criteria
We included original studies written in English and published from inception to November 2022, evaluating surgical outcomes for treatment of RTS. Studies were excluded for being duplicate, non-English text, abstract only, review, meta-analysis, reports with fewer than 5 patients, commentary, editorial, purely radiographic, surgical technique, and surgical approaches that did not stratify results. (Figure 1).
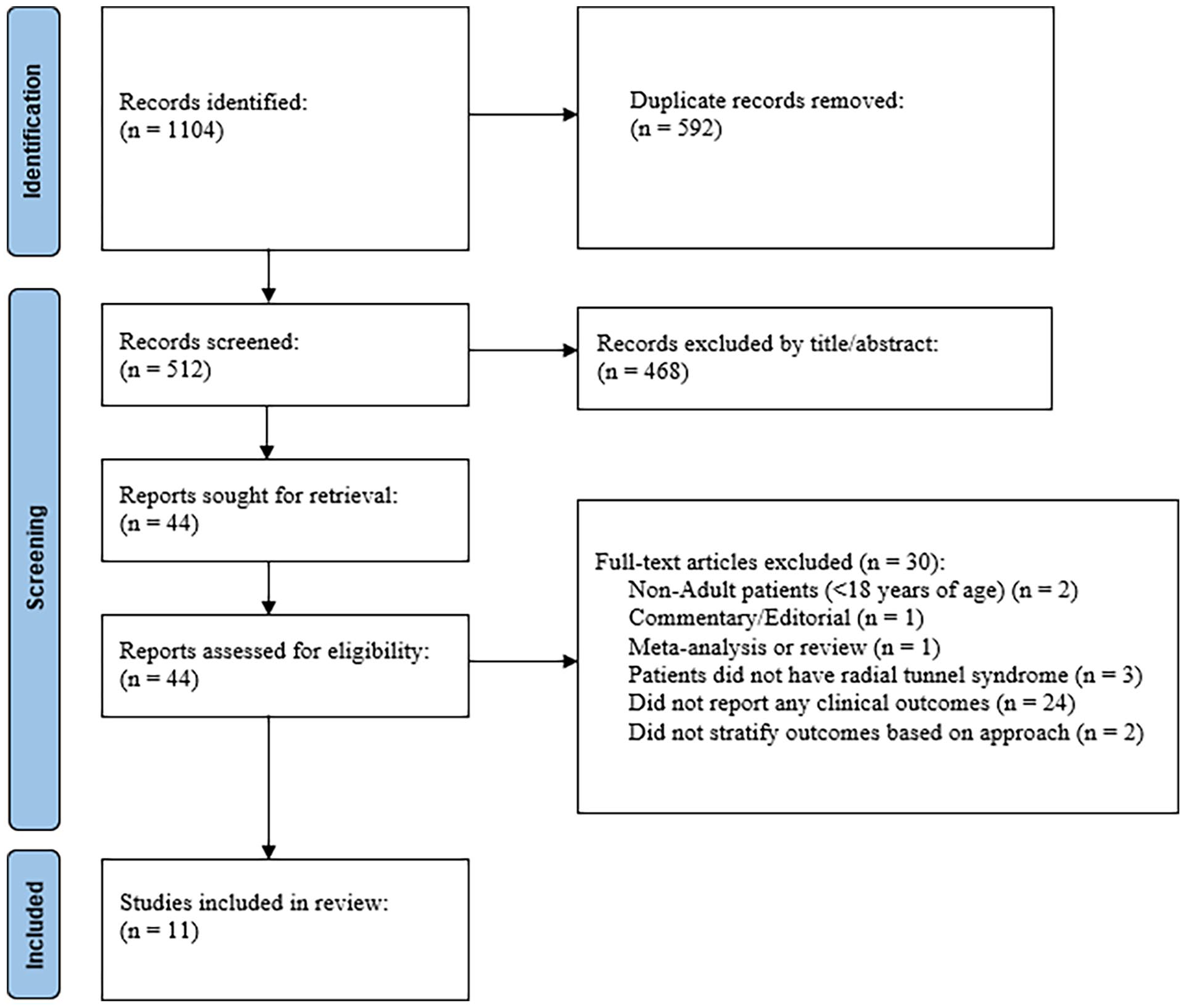
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of the study selection criteria.
Search Strategy
We queried the PubMed/MEDLINE, Embase, Web of Science, and Cochrane databases using the following search terms: “radial tunnel,” “radial nerve compression,” “supinator syndrome,” “posterior interosseous nerve,” and posterior interosseous nerve compression” (see Appendix A for database-specific search strategies). Articles were first screened by title and abstract for exclusion criteria by K.M.H. If inclusion eligibility was questionable, the authors included the study. Subsequent full text screening was conducted by 2 authors (B.R. and K.M.H.). A panel of senior upper-extremity surgeons provided expert opinion.
Data
Data extraction was completed using a standardized data-collection form by 2 authors (B.R. and L.C.M.). Data collected included level of evidence, country of study, and study type, number of patients and extremities, minimum and mean length of follow-up, average age, sex, intraoperative findings, intraoperative compressive sites, patient-reported outcomes (PROs), range of motion, strength measures, and complications. Study characteristics were summarized descriptively. Weighted means were calculated for study demographics.
Surgical approaches were grouped as dorsal or volar and further stratified by the muscle interval. Dorsal approaches included those between the ECRB and extensor digitorum communis (EDC) (Thompson approach), between brachioradialis (BR) and extensor carpi radialis longus (ECRL), and transmuscular BR split. Volar approaches included between BR and biceps or brachialis, and between BR and flexor carpi radialis (FCR) (Henry approach).
Risk of Bias Assessment
The Methodological Index for Non-Randomized Studies (MINORS) criteria was utilized to assess bias by a single investigator (D.P.). 7 See supplementary table for individual studies and MINORS scores.
Evidence Synthesis
Study characteristics were summarized descriptively. Weighted means, based on the number of upper extremities in each study, were calculated for study demographics and characteristics of interest. Since a lack of homogeneous outcomes prohibited meta-analysis, we performed a descriptive synthesis of outcomes reported by each study based on surgical approach to identify which approaches were associated with favorable outcomes.
Results
Search Results
Our search strategy returned 1104 publications, of which 11 unique articles were found to meet inclusion criteria (Figure 1).
Study and Patient Characteristics
The level of evidence was IV for all included studies, with 2 being prospective cohort studies and 9 being retrospective cohort series. The articles were mostly published in the Journal of Hand Surgery including both American and British volumes (27%, n = 3) and Journal of Plastic, Reconstructive and Esthetic Surgery (18%, n = 2). The 11 articles totaled 275 patients with 285 upper extremities affected by RTS. The weighted mean age was 43 years [range: 37-52 years], follow-up was 42 months [range: 12-97 months], and 58% were female.
Surgical Characteristics
Of the included surgeries, 5 different approaches were reported, with the most common being the interval between the BR and FCR (34%, n = 98) followed by the interval between the BR and biceps or brachialis (20%, n = 57). The number of articles that reported site of compression was 8 (3 dorsally [105 forearms] vs 5 volarly [133 forearms]). The most common site of compression was the Arcade of Frohse (39%, n = 110) followed by the fibrous band proximal to the Arcade (15%, n = 42) and the Leash of Henry (11%, n = 32). Mean duration of symptoms prior to surgical intervention was reported in 9 studies with the mean duration being 21 months.
In total, 46% (n = 130) of forearms, in 5 studies, were approached dorsally while 54% (n = 155) of forearms, in 6 studies, were approached volarly. Age at surgery, duration to follow-up, female sex distribution, and duration of symptoms prior to surgery were similar between groups (Table 1). Of the dorsal approaches, the interval between the BR and ECRL and between the ECRB and EDC were the most utilized (41%, n = 53, both), followed by a transmuscular BR-splitting approach (18%, n = 24). Of the volar approaches, the volar Henry approach was the most utilized (63%, n = 98) followed by between the BR and biceps or brachialis (37%, n = 57).
Demographics.

Note. Values reported as weighted mean [range] unless otherwise specified.
Site of Compression
Dorsal approaches more often identified a constriction at the fibrous bands proximal to the arcade of Frohse (100% [n = 42] vs 0%, [n = 0]) and at the distal border of the supinator (100% [n = 9] vs 0% [n = 0]) when compared with volar approaches; whereas volar approaches identified a greater number of constrictions at the arcade of Frohse (74% [n = 81] vs 26% [n = 29]), leash of Henry (88% [n = 28] vs 12% [n = 4]), and ECRB belly (55% [n = 18] vs 45% [n = 15]), when compared with dorsal approaches (Table 2).
Identified Location of Constriction.

Note. AOF = arcade of Frohse; LOS = leash of Henry; ECRB = extensor carpi radialis brevis; BR = brachioradialis; ECRL = extensor carpi radialis longus; EDC = extensor digitorum communis; FCR = flexor carpi radialis.
Approaches with multiple sites of compression noted within at least one forearm.
Outcomes of Dorsal Approaches
Two studies utilized the interval between the BR and ECRL and both reported poor outcomes (Table 3). Atroshi et al 8 included 37 forearms that underwent transection of all compressing structures overlying the PIN as well as the fibrous edge of supinator muscle with concomitant free fat transplant. The authors reported low postoperative satisfaction (39%) and low rates of return to preoperative employment (43%). Patterson et al 9 included 15 forearms that underwent surgical release of the tendinous leading edge of the ECRB and the leading edge of the supinator muscle and reported a poor postoperative Disabilities of the Arm, Shoulder, and Hand (DASH) score of 33.5, which is substantially poorer than previously reported patient acceptable symptom state (PASS) thresholds (15.9–20.5). 10
Findings by Study for Dorsal Approaches.

Note. BR = brachioradialis; ECRL = extensor carpi radialis longus; N/A = not applicable; FCR = flexor carpi radialis; ECRB = extensor carpi radialis brevis; DASH = Disabilities of the Arm, Shoulder, and Hand score; SD = standard deviation; VAS = visual analog scale; EDC = extensor digitorum communis; MEPS = Mayo Elbow Performance Score.
At least 1 patient with bilateral forearms included.
Two studies utilized the interval between the ECRB and EDC and reported satisfactory outcomes. Ertem et al 11 released the tendinous edge of the ECRB until the leash of Henry in 10 forearms and reported mean postoperative Mayo Forearm Performance Score (MEPS) of 87.5, mean DASH score of 6.8, 80% excellent or good Roles and Maudsley score, and 90% of patients reporting postoperative satisfaction. Simon Perez et al 12 dissected the supinator muscle in 43 forearms and found 86% of patients to have excellent or good postoperative Roles and Maudsley score.
One study utilized a transmuscular BR- splitting technique and was associated with modest success. Jebson and Engber 13 released the fibrous edge of the supinator in 24 forearms and found 67% of patients to have excellent or good postoperative Roles and Maudsley score and 67% of patients to have a good Ritts score with 79% satisfied postoperatively.
Outcomes of Volar Approaches
Two studies utilized the interval between the BR and biceps or brachialis muscles and reported poor results (Table 4). Lawrence et al 14 released sites of compression proximal to the arcade of Frohse in 30 patients and found only 41% of patients were able to return to activities of daily living. Complications were reported in 24% of patients, most of which were nerve-related. Lee et al 15 released all possible sites of compression including fascial bands, constricting vessels, and the medial edge of the ECRB in 27 patients and found 67% of patients with a good Ritts score. A postoperative superficial branch of the radial nerve palsy was noted in 11% (n = 3) of patients.
Findings by Study for Volar Approaches.

Note. BR = brachioradialis; N/A = not applicable; VAS = visual analog scale; ECRB = extensor carpi radialis brevis; FCR = flexor carpi radialis.
At least one patient with bilateral forearms included.
Four studies utilized the interval between the BR and the FCR, and with most reporting poor outcomes. De Smet et al 16 transected the fibrous edge of the supinator in 22 forearms and found low overall postoperative satisfaction (36%). Sotereanos et al 18 performed a radial tunnel release (not further specified) in 28 forearms and found low overall postoperative satisfaction (57%) and low percentage being able to return to preoperative employment (21%). Verhaar and Spaans 19 transected the fibrous edge of the supinator and veins running over the radial nerve and concomitantly placed a free fat transplant over their nerve in 10 patients and reported only one patient had a good Roles and Maudsley score, with the 9 remaining patients rating their outcome as fair or poor. Conversely, Roles and Maudsley 17 reported satisfactory outcomes in 36 patients that had transection of the superficial part of the supinator muscle with 97% having excellent or good Roles and Maudsley score.
Discussion
Optimal diagnostic and treatment modalities remain poorly defined in RTS. Heterogeneity across literature describing location of compression, surgical approach, means of reporting outcomes, and lack of controlled comparisons has made it difficult to provide evidence-based recommendations. In this review, we aimed to synthesize patient outcomes based on surgical approaches to help guide operative management and future investigation of RTS. We identified that dorsal approaches more commonly identified constrictions at the proximal and distal portions of the arcade of Frohse (AOF), while volar approaches more commonly identified vascular constrictions. We found that studies reporting outcomes of a dorsal approach between the ECRB and EDC reported the best clinical outcomes.
There is currently no consensus regarding the optimal surgical approach for treatment of RTS, as evidenced by a relatively similar distribution of dorsal (46%) and volar (54%) approaches in this review. Compared with volar approaches, dorsal approaches, particularly between the ECRB and EDC and transmuscular BR-splitting approach, had superior outcomes including superior postoperative PROs and functional outcomes. When comparing the 2, the ECRB and EDC interval (Thompson approach) demonstrated > 80% of patients reporting “excellent” or “good” postoperative Roles and Maudsley score in 2 studies11,12 when compared with 67% of patients in one study. 13 This may be explained by the fact that the interval between the ECRB and EDC gives direct visualization of the supinator muscle and the PIN as it runs through the radial tunnel, allowing the surgeon to identify potential sites of compression proximal and distal to the radial tunnel with the option to transect the superficial portion of the supinator muscle. 20 While the BR and ECRL interval and transmuscular BR-splitting interval still allow for visualization of the proximal portion of the supinator, both of these approaches are more lateral to the ECRB and EDC approach, allowing for potential misses of constrictions of the PIN as it transverses medially in the dorsum of the forearm.
Moradi et al 3 has noted that if there is clinical suspicion for localization of compression, such as associated sensory symptoms, this can suggest a more proximal source of RTS and would favor release of the leash of Henry. 3 We identified that a majority of studies that released the leash of Henry were through a volar approach (88%). These findings are consistent with a cadaveric study performed by Urch et al 4 who reported that volar approaches afforded significantly better visualization of the leash of Henry when compared with dorsal approaches. The interval between BR and FCR, also known as the Henry approach, was the most documented volar approach in our study (63%). This is likely due to the broad utility for this approach resulting in increased surgeon familiarity and ease of extension both proximally and distally to the elbow. 21 However, when compared with the other reported volar interval (between the BR and biceps or brachialis), this approach was associated with poorer postoperative satisfaction.
There is a well-established correlation between the presence of RTS and other compressive neuropathies which should be considered when choosing a surgical approach.3,9,12,13,15,18 The rate of concomitant lateral epicondylitis has been reported to range from 18-43% and requires careful evaluation prior to the decision to pursue surgery for treatment of RTS.9,12,13,15,18 One study utilizing the transmuscular BR-splitting approach reported 4 cases of concurrent lateral epicondylitis missed at time of surgery and at least one required return to the operating room. 13 If planning for a simultaneous release, the dorsal approach via the Thompson or BR and ECRL interval are favored due to the ability to be extended proximally. 3
Few complications, aside from failure to completely resolve symptoms, were noted in this review. While the number of overall reported complications were comparable between the groups (dorsal, 44% vs volar, 56%), studies utilizing a volar approach reported more severe and permanent deficits, with superficial branch of the radial nerve (SBRN) injury being the most common. Sotereanos et al 18 using a volar approach reported postoperative SBRN neuropraxia in 31% of patients (11/35), with most improving within 24 months; the authors attributed this high rate of SBRN neuropraxia to the use of greater retraction during the Henry approach. In the cadaveric study performed by Urch et al, 4 the SBRN was visualized in all volar and anterolateral approaches, but was only visualized in 40% of posterior approaches, placing it at a higher risk of injury compared with volar approach due to its anatomic course. Of note, in this review, only 1 case of neuropraxia of the SBRN was observed in the dorsal group, while 3 were identified in the volar group. The most common complication reported among the dorsal approach group was transient weakness (n = 22), with only 3 cases of noted paresis of the extensors. All cases of paresis were noted in the study performed by Simon Perez et al 12 who noted that 2 recovered in less than 3 months, and the remaining individual obtained a partial recovery.
Heterogeneity of reported outcomes precluded meta-analysis of clinical outcomes in volar versus dorsal approaches. In order to facilitate future cross-study comparison, the authors of this study propose that future research report, at least, Roles and Maudsley and DASH (or QuickDASH) scores. The Roles and Maudsley 17 score is a subjective assessment of patient pain during function and is rated as follows: excellent—no pain (1 point), full movement, full activity; good—occasional discomfort (2 points), full movement and full activity; fair—some discomfort after prolonged activity (3 points); poor—pain limiting activity (4 points). Successful interventions are defined as those that score “excellent” or “good” when comparing postoperative to baseline values. The score has been used across various orthopedic pathologies and has been widely utilized to validate novel scoring systems.22 -24 The DASH questionnaire is the most commonly used questionnaire for assessing activities of daily living after arm injuries, and is considered a valid and reliable non-supervised test.25 -27 Furthermore, the QuickDASH may be utilized when necessary to reduce questionnaire fatigue by patients as this score has been validated to show similar precision as the full-length DASH score. 28 Other outcomes reported in this systematic review such as the Ritts score, an outcome measure that rates patients’ satisfaction of their results as “good,” “fair,” or “poor,” may be utilized to supplement the minimum recommended outcome scores as aforementioned.
This study is the first systematic review article, to our knowledge, to examine and compare the variety of surgical approaches available for the management of RTS. However, the results of this review should be viewed with consideration for the limitations of this study. One such limitation is that the authors of this systematic review assumed that the included patients had an accurate diagnosis of RTS at time of surgery. However, it was purposefully chosen to not have confirmatory imaging, EMG, or NCS as an inclusion criteria as RTS remains a clinical diagnosis without diagnostic criteria and confirmatory testing is controversial. 3 Other limitations inherent to systematic reviews are pertinent to this study and include potential for selection bias, attrition bias, selective outcome reporting attributed to single surgeon case series, and heterogeneity. Analysis of outcomes was limited by the heterogeneity in PROs reported. Despite the pooling effect of systematic reviews, there was a smaller than ideal pool of qualified data; however, it should also be noted the overall incidence of RTS is relatively low (.003%–.03%). 3 Finally, despite using the guidelines proposed by PRISMA and searching multiple databases, there is the risk of missing articles that would significantly affect data due to the overall low number of patient’s included in this study.
Conclusion
Series reporting the outcomes of surgical treatment for RTS using a dorsal approach through the ECRB and EDC interval noted the best outcomes relative to series utilizing other surgical approaches. While dorsal approaches more commonly reported constrictions at the proximal and distal portions of the arcade of Frohse, vascular constrictions were more commonly reported with volar approaches. Heterogeneity in reported outcomes among included studies limited cross-study comparisons; we suggest that future studies, at a minimum, report Roles and Maudsley and DASH scores to help facilitate future comparison.
Supplemental Material
sj-docx-1-han-10.1177_15589447251315761 – Supplemental material for Clinical Outcomes of Operative Management for Radial Tunnel Syndrome According to Surgical Approach: A Systematic Review
Supplemental material, sj-docx-1-han-10.1177_15589447251315761 for Clinical Outcomes of Operative Management for Radial Tunnel Syndrome According to Surgical Approach: A Systematic Review by Brittany Raymond, Robert J. Cueto, Laura C. Mazudie Ndjonko, Kevin A. Hao, C. David Pfaehler, Timothy R. Buchanan, Tammy Phillips, Thomas W. Wright, Joseph J. King and Keegan M. Hones in HAND
Footnotes
Appendix
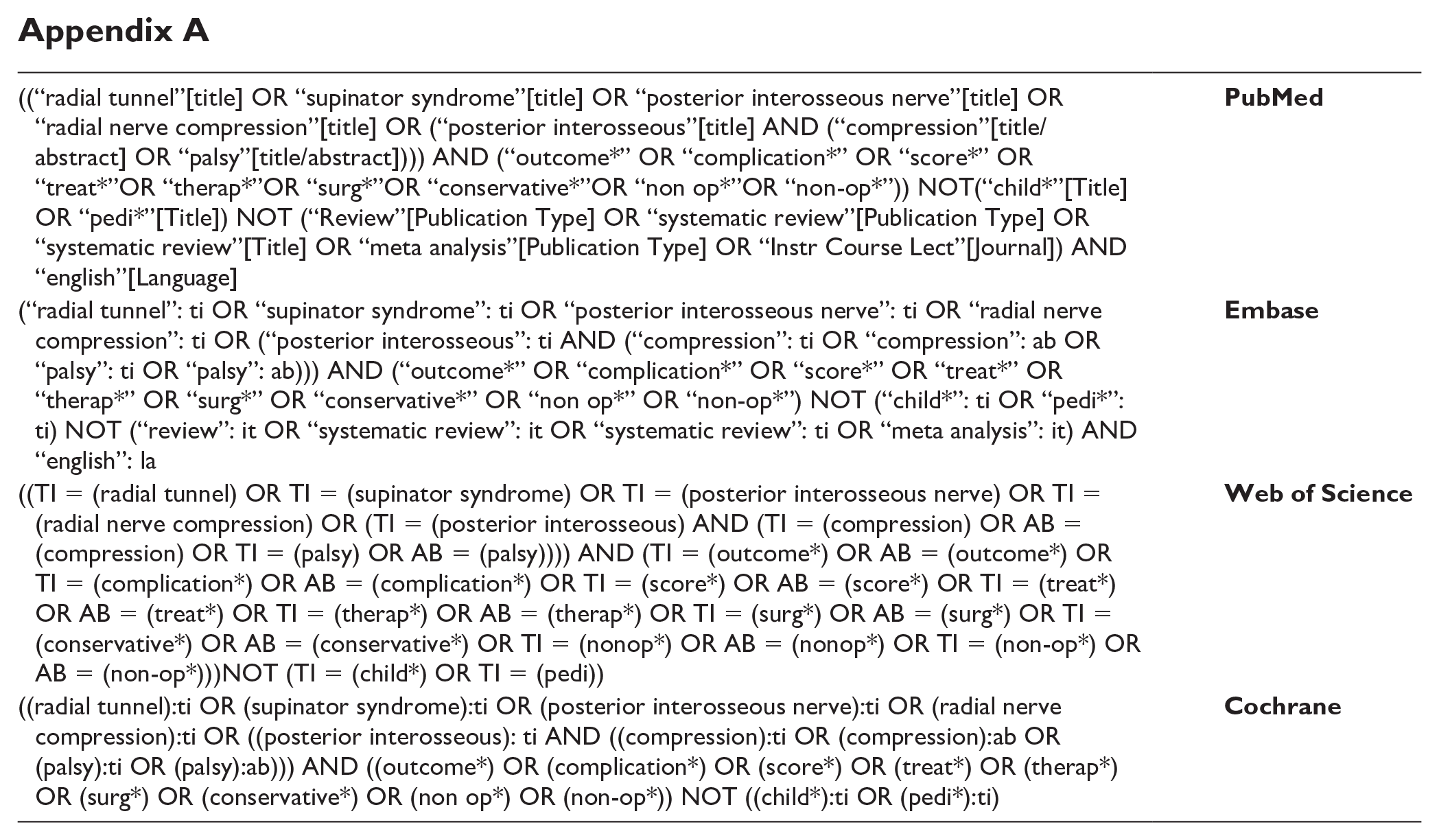
| ((“radial tunnel”[title] OR “supinator syndrome”[title] OR “posterior interosseous nerve”[title] OR “radial nerve compression”[title] OR (“posterior interosseous”[title] AND (“compression”[title/abstract] OR “palsy”[title/abstract]))) AND (“outcome*” OR “complication*” OR “score*” OR “treat*”OR “therap*”OR “surg*”OR “conservative*”OR “non op*”OR “non-op*”)) NOT(“child*”[Title] OR “pedi*”[Title]) NOT (“Review”[Publication Type] OR “systematic review”[Publication Type] OR “systematic review”[Title] OR “meta analysis”[Publication Type] OR “Instr Course Lect”[Journal]) AND “english”[Language] |
|
| (“radial tunnel”: ti OR “supinator syndrome”: ti OR “posterior interosseous nerve”: ti OR “radial nerve compression”: ti OR (“posterior interosseous”: ti AND (“compression”: ti OR “compression”: ab OR “palsy”: ti OR “palsy”: ab))) AND (“outcome*” OR “complication*” OR “score*” OR “treat*” OR “therap*” OR “surg*” OR “conservative*” OR “non op*” OR “non-op*”) NOT (“child*”: ti OR “pedi*”: ti) NOT (“review”: it OR “systematic review”: it OR “systematic review”: ti OR “meta analysis”: it) AND “english”: la |
|
| ((TI = (radial tunnel) OR TI = (supinator syndrome) OR TI = (posterior interosseous nerve) OR TI = (radial nerve compression) OR (TI = (posterior interosseous) AND (TI = (compression) OR AB = (compression) OR TI = (palsy) OR AB = (palsy)))) AND (TI = (outcome*) OR AB = (outcome*) OR TI = (complication*) OR AB = (complication*) OR TI = (score*) OR AB = (score*) OR TI = (treat*) OR AB = (treat*) OR TI = (therap*) OR AB = (therap*) OR TI = (surg*) OR AB = (surg*) OR TI = (conservative*) OR AB = (conservative*) OR TI = (nonop*) OR AB = (nonop*) OR TI = (non-op*) OR AB = (non-op*)))NOT (TI = (child*) OR TI = (pedi)) |
|
| ((radial tunnel):ti OR (supinator syndrome):ti OR (posterior interosseous nerve):ti OR (radial nerve compression):ti OR ((posterior interosseous): ti AND ((compression):ti OR (compression):ab OR (palsy):ti OR (palsy):ab))) AND ((outcome*) OR (complication*) OR (score*) OR (treat*) OR (therap*) OR (surg*) OR (conservative*) OR (non op*) OR (non-op*)) NOT ((child*):ti OR (pedi*):ti) |
|
Ethical Approval
This article contains only information from prior publications which had individually been de-identified. As such, ethical approval was not required to conduct this study.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed Consent was obtained when necessary.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr K.A.H. is a paid statistical consultant for LinkBio Corp. Dr J.J.K. is a consultant for Exactech, Inc. and LinkBio Corp. Dr T.W.W. is a consultant for Abyrx and receives royalties from Exactech, Inc. Dr W.R.A. is a consultant for Exactech, Inc. The other authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.