
Abstract
Osteoarthritis of the carpometacarpal (CMC) joint of the thumb is commonly treated with intraarticular corticosteroid injections in clinic. In this case report, we present 2 patients who experienced immediate pain, pallor, and discoloration of their fingers distal to the site of attempted injection of the CMC joint of the thumb. It is believed that this occurred due to inadvertent injection of the dorsal branch of the radial artery as it branches to join both the superficial and deep palmar arches. This caused vasospasm and vasoocclusion leading to subsequent ischemia. To relieve symptomatic pain and prevent ischemic necrosis, both patients underwent sympathectomies of the radial and ulnar arteries and of the common palmar digital arteries. Both patients experienced relief of their pain and reperfusion of their hand and digits.
Introduction
Osteoarthritis (OA) is a prevalent condition affecting both large and small joints, commonly including the carpometacarpal (CMC) joints. In the treatment of OA of the CMC joint of the thumb, intraarticular corticosteroids are commonly administered in primary care or surgical specialist clinics. This case report highlights 2 patients who experienced immediate pain, pallor, and discoloration of their fingers distal to the attempted corticosteroid injection site (in both cases, methylprednisolone acetate) for CMC joint OA. It is believed that this occurred due to inadvertent injection into the dorsal branch of the radial artery, which branches to join both the superficial and deep palmar arches. To our knowledge, there have been no previous reports of this adverse event from attempted thumb CMC corticosteroid injection.
Case Report
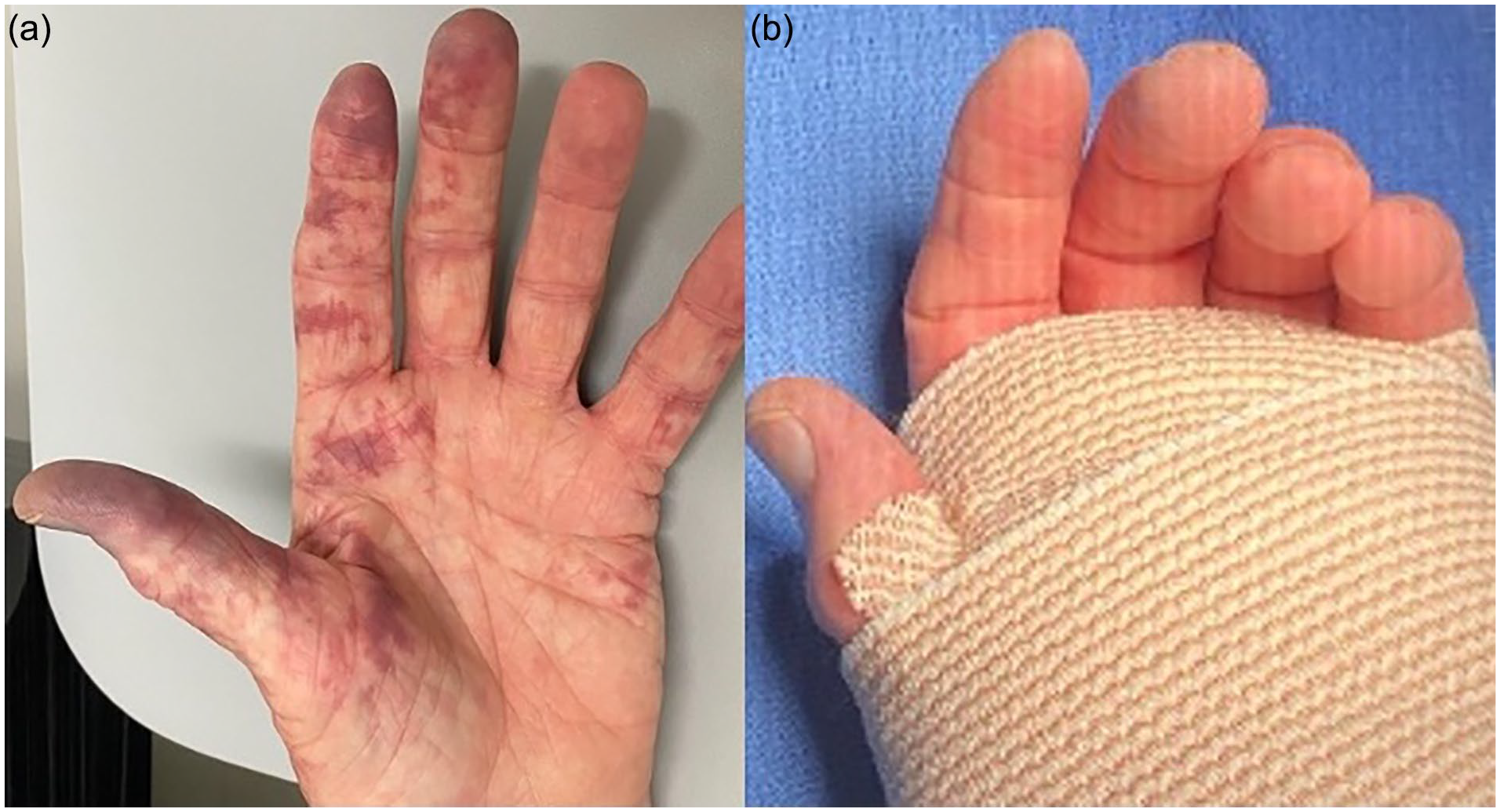
Patient 1, a 60-year-old man, initially sought treatment at an outside orthopedic office for a steroid injection in his right thumb CMC joint. Following the injection, he experienced numbness in the fingers of his right hand. Over the subsequent hours, he noticed discoloration in these fingers, particularly at their distal tips. On returning to the original clinic, he was prescribed apixaban but found no relief from his symptoms after 1 week. Three weeks postinjection, he presented to our hand clinic with pronounced signs of ischemia. His fingers appeared mottled and violaceous (Figure 1a), exhibited swelling, felt cold to the touch, and were highly tender to palpation. On examination, capillary refill time was noted to be 4 to 5 seconds in all digits proximal to the interphalangeal (IP) and distal interphalangeal (DIP) flexion crease. Distal to this crease, it was difficult to appreciate any amount of capillary refill due to the significant amount of mottling and discoloration. Allen’s test confirmed occlusion of the radial artery. An indurated segment of the radial artery was palpable within the anatomic snuff box. Despite this, he retained full range of motion in his wrist and all fingers. He reported escalating pain in the affected fingers, accompanied by a decrease in sensation.

Patient 1: (a) right hand 3 weeks postinjection, (b) immediately postoperatively.
During his initial visit, the plan was to initiate treatment with a dihydropyridine calcium channel blocker (dCCB; amlodipine) and observe his symptoms for 1 week. However, after 1 week, there was minimal improvement in his symptoms. Following an extensive discussion with the patient, he elected to undergo sympathectomy of the digital arteries of his right hand and his right radial artery. He elected to not undergo angiography prior to surgery as it was discussed it would yield little change in clinical decision-making given the extent of his symptoms and physical examination findings. Commentary and details of the surgical technique used for periarterial sympathectomy can be found in the discussion section of this article. Immediately after the operation, there was a remarkable improvement in the color of his fingers (Figure 1b).
At his 2-week postoperative follow-up, the patient exhibited complete resolution of his symptoms. He reported being free from pain and was observed to have intact sensation and brisk capillary refill throughout all fingers. In addition, the tip of the index finger, which appeared mottled immediately postoperatively, healed without issue.
Patient 2, a 67-year-old man, initially sought treatment at an external orthopedic office for a steroid injection in his left thumb CMC joint. His presentation was more acute compared with patient 1, as he reported that blood “shot out” as soon as the needle was removed, accompanied by immediate burning pain in his fingers. He observed his hand becoming “very splotchy,” and over the next 2 hours, the pain intensified, prompting him to seek care at the local emergency department (ED). At the ED, he was diagnosed with a steroid embolism in the radial artery and was administered nitropaste and given a prescription for amlodipine. However, he opted not to fill this prescription.
Two weeks postinjection, he presented to our hand clinic with symptoms of numb yet painful fingers with mottled, violaceous discoloration (Figure 2a). He experienced severe symptoms in his thumb, index, and long finger, with milder manifestations in his ring and small finger. On examination, he exhibited diminished sensation in the tips of his thumb, index, and long finger, with a palpable radial pulse proximal to the wrist but not distal. At the level of the wrist, an indurated segment of the radial artery was palpable within the anatomic snuff box. In the thumb, index, and long fingers, no capillary refill was able to be appreciated distal to the IP and DIP joints respectively. Proximal to this crease, capillary refill was very sluggish (4-5 seconds). Allen’s test confirmed occlusion of the radial artery. Despite this, he retained full range of motion of his wrist and all fingers. His radial digits were cold to the touch.
Patient 2: (a) left hand 2 weeks postinjection, (b) immediately postoperatively from sympathectomy of digital arteries.
After extensive discussion with the patient, he elected to undergo sympathectomy of the common and proper digital arteries in his left hand. Following the procedure, there was immediate improvement in the color of his fingers (Figure 2b). His index and long finger returned to healthy, baseline appearance, with brisk capillary refill observed. However, his thumb still exhibited significant mottling, albeit with slightly improved capillary refill.
Seventy-two hours postoperatively, the patient reported improvement in his index and long finger, but he continued to experience significant pain and ischemic changes in his thumb. The thumb displayed violaceous mottling and felt cold to the touch, indicating persistent vascular compromise in that digit despite the intervention.
He had an arteriogram of his left upper extremity revealing a patent superficial arch but an abruptly ending dorsal branch of the radial artery (Figure 3). Subsequently, the patient underwent a sympathectomy of the radial and ulnar arteries at the level of the wrist, which led to considerable improvement in the coloration of his fingers, with only a small amount of residual mottling observed in his left thumb (Figure 4a and 4b). Immediately following the procedure, a pulse oximeter was placed on both thumbs, revealing a reading of 96% for the healthy right thumb and 91% for the postoperative, impaired left thumb. Bilateral pulse waveforms were appreciated.
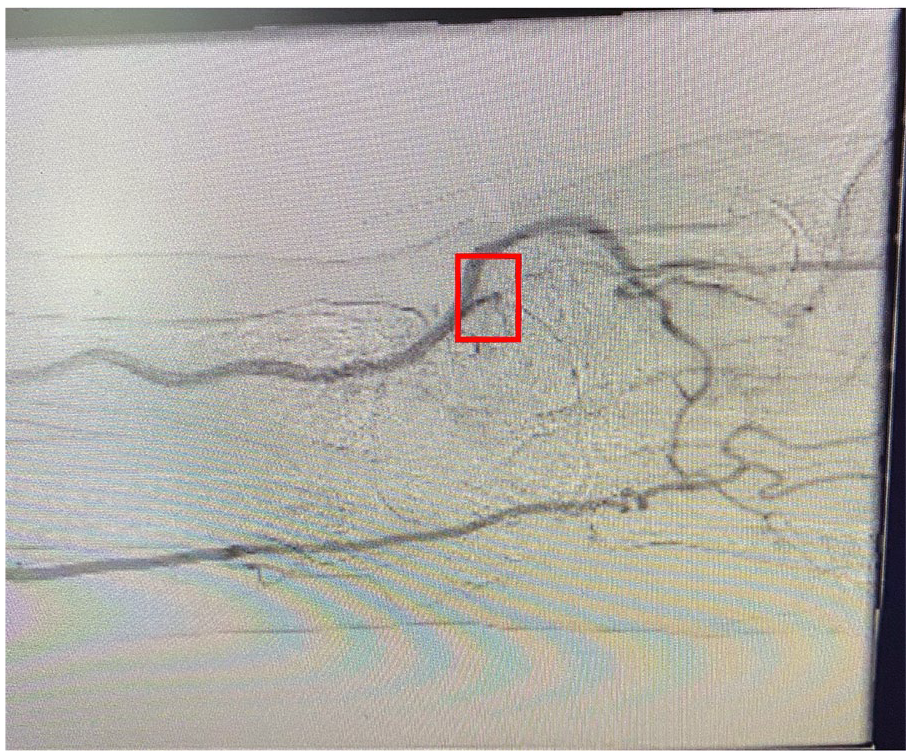
Patient 2: arteriogram of the left upper extremity showing abrupt ending of dorsal branch of radial artery (red box).
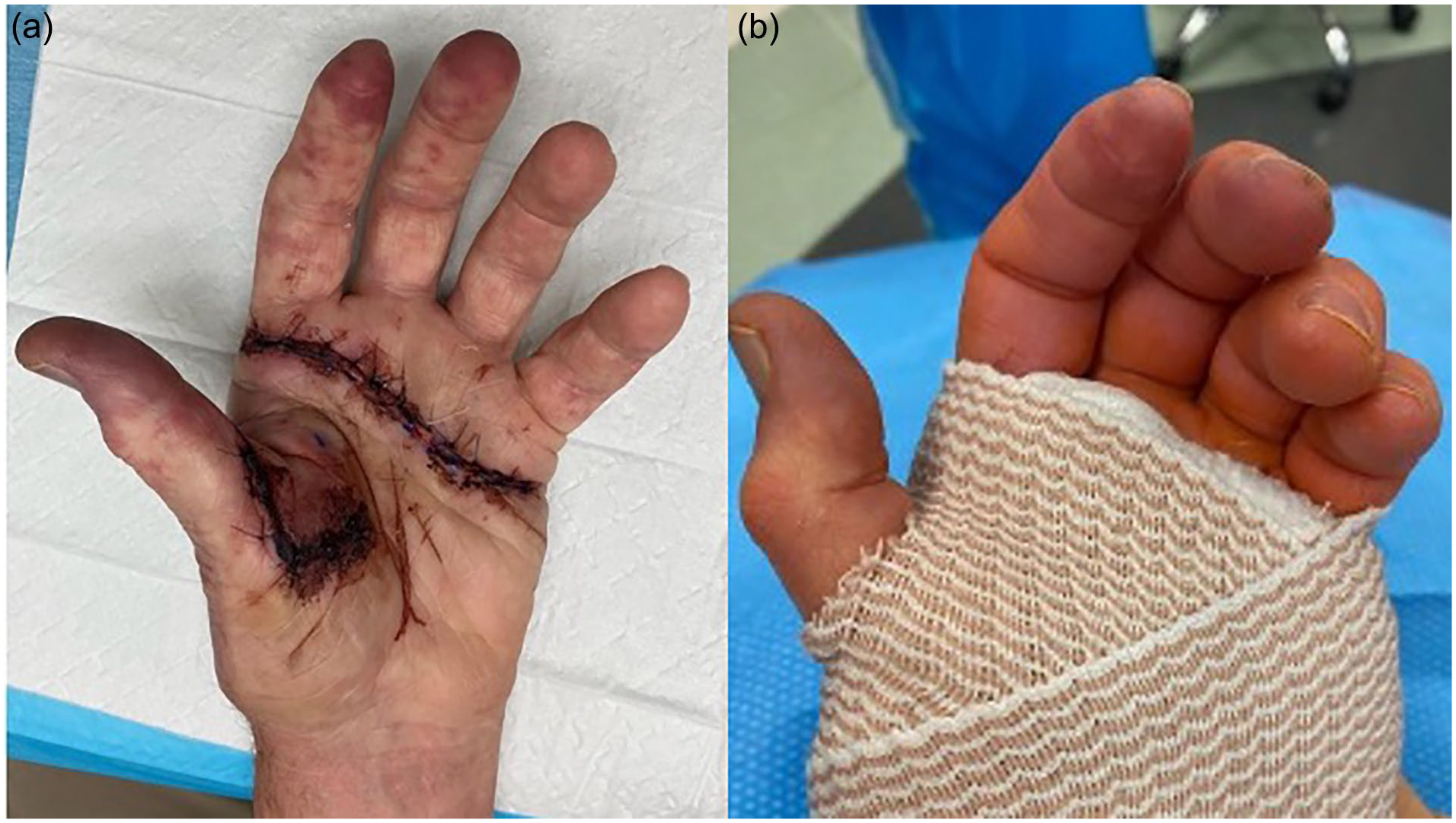
Patient 2: left hand (a) 72 hours postsympathectomy of digital arteries, (b) immediately postsympathectomy of radial and ulnar arteries at the level of the left wrist.
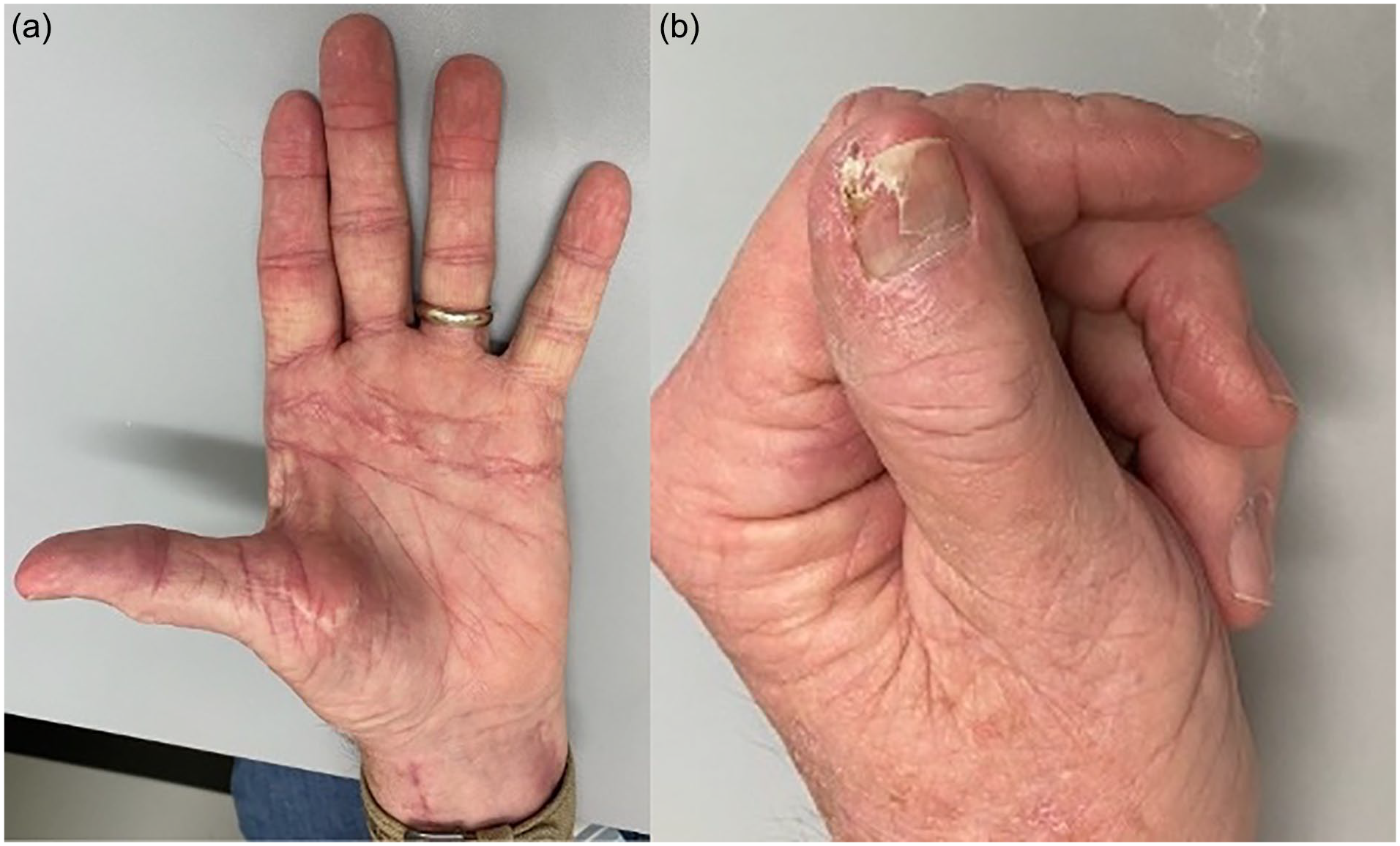
Three weeks after radial and ulnar artery sympathectomies, the patient reported significant improvement in pain and color in all his fingers except his thumb. Although he still experienced mild, intermittent discomfort at the tips of his fingers, his symptoms gradually improved. However, the most distal aspect of his left thumb exhibited a necrotic appearance (Figure 5a and 5b).

Patient 2: (a) thumb and (b) palmar view 21 days postsympathectomy of radial and ulnar arteries at the level of the left wrist.
At his 2-month postoperative follow-up, the patient had achieved complete resolution of his symptoms (Figure 6a). In addition, the necrotic tip of his left thumb had naturally sluffed, exposing healthy dermis beneath (Figure 6b).
Patient 2: (a) palmar view and (b) thumb 8 weeks postsympathectomy of radial and ulnar arteries at the level of the left wrist.
Discussion
The dorsal branch of the radial artery travels just proximal to the CMC joint of the thumb, crossing dorsally over the scaphotrapeziotrapezoid joint (Figure 7a and 7b). Figure 7a shows the radial artery crossing dorsally just proximal to the needle placed in the CMC joint of the thumb. Therefore, it is likely that while attempting to inject the CMC joint, the needle was placed too proximal and the steroid was injected into the dorsal branch of the radial artery, resulting in vasospasm and vasoocclusion with subsequent ischemia.
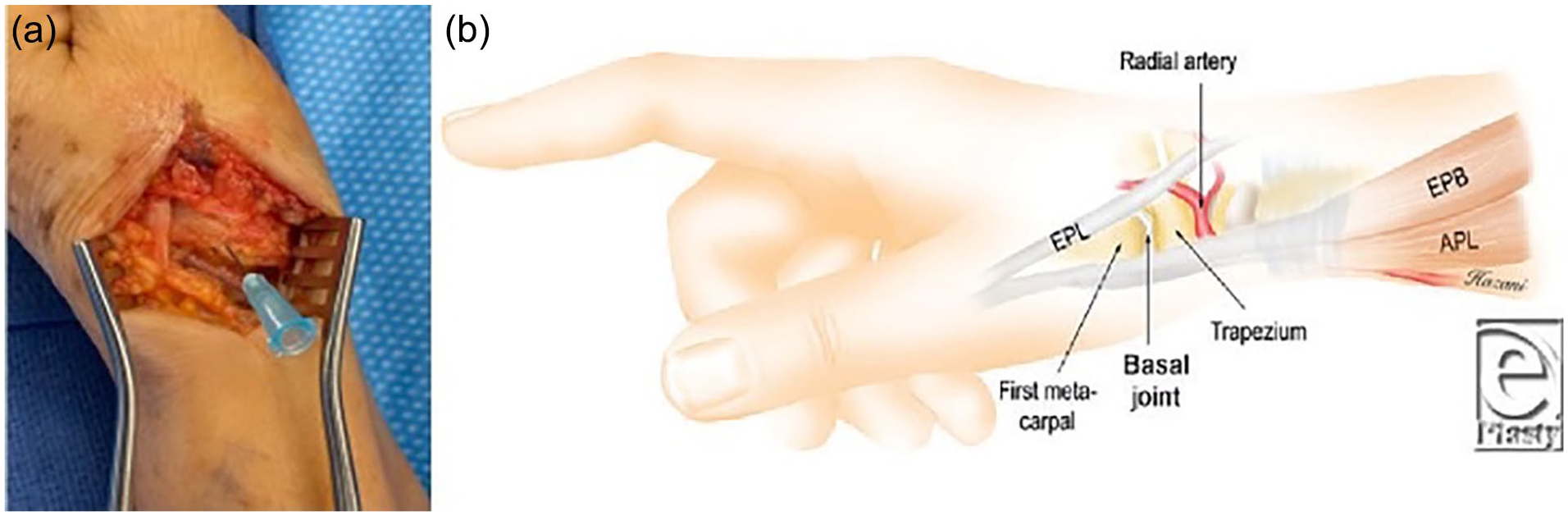
Surgical anatomy: (a) with needle in the carpometacarpal (CMC) joint of the thumb, (b) diagram of the dorsal branch of the radial artery in relation to the CMC joint. 1
Both patients presented with clinical signs including palpable radial artery induration, mottling and discoloration, reduced or absent capillary refill, and a positive Allen’s test indicating radial insufficiency. They also reported symptoms of decreased sensation and severe ischemic pain. Based on this clinical presentation, we strongly suspected the presence of a radial artery thrombus. Given the abundance of clinical findings, we considered additional diagnostic workup (such as Doppler ultrasound, hypercoagulability labs, or pulse oximetry) unnecessary at the time, given their results were unlikely to change our clinical impression. As ulnar flow typically compensates when radial flow is obstructed, we suspected additional arterial occlusion distal to the primary injection site. We hypothesized that microemboli, vasospasm, and/or endothelial damage distal to the radial artery were significantly contributing to the observed symptoms. As a result, a simple thrombectomy, which would only address the apparent radial thrombus and not the more distal sequelae, was considered insufficient. Although it was impossible to be certain of all the factors contributing to their presentation, the immediate symptom relief and significantly improved blood flow following sympathectomy support our hypothesis that vasospasm played a significant role in the pathology.
Perivascular botulinum toxin injections were considered due to their use (and proposed mechanism of action, which involves blocking norepinephrine release to create a chemical sympathectomy) in patients with digital ischemia and refractory Raynaud disease/phenomenon.2-6 Although observational studies have shown some efficacy for botulinum toxin injections, particularly in subjective measures like pain and symptom severity (though rarely reaching statistical significance), 2 a randomized controlled trial yielded worse objective results and no statistically significant difference in most subjective outcomes when comparing botulinum toxin to placebo. 4 This may be explained by the “well-known and significant placebo effect [that] exists among patients with less severe Raynaud’s.” 6 In addition, unlike our cases, several reports of botulinum toxin’s potential benefits have used arteriograms to rule out thrombus prior to treatment.5,6 In the setting of acute traumatic hand injury, one case series did report some protective benefit of botulinum toxin in polytrauma patients with contraindications to anticoagulation, though the comparison was made against aspirin and warm water baths as the alternative treatments. 3 Ultimately, the absence of high-quality evidence in this clinical scenario, combined with the well-documented short duration of perceived benefit (approximately 6 months on average), guided our decision to pursue a more definitive treatment approach.
Hyperbaric oxygen therapy, commonly used for threatened flaps/grafts, burns, long-term wounds, and compartment syndrome, as well as continuous nerve catheterization, which induces transient vasodilation, were both considered as treatment options. However, given the timing and duration of the injuries at presentation, along with the diffuse ischemic signs and symptoms suggesting the involvement of microemboli, vasospasm, or endothelial damage, we concluded that these interventions would likely be insufficient. The situation we were presented with warranted definitive, long-term treatment that would allow the resolution of endothelial damage and microemboli over the span of several months.
Given Poiseuille’s Law, vasospasm can significantly reduce the radius of the affected arteries, thus drastically reducing the blood flow. By removing sympathetic innervation to an artery and thus increasing its radius, distal blood flow can be drastically increased. 7 However, pathways of sympathetic innervation of the upper extremity arterial system are inconsistent and often rely on many small sympathetic branches originating from larger nerves instead of traveling as distinct bundles of the branchial plexus. These small sympathetic branches then run within the adventitia of the artery, between the adventitia and the tunica media. Thus, the more distal the sympathectomy, the more likely it is to produce the desired result with lasting effects. 8 Digital artery sympathectomy has previously been used for the treatment of diminished arterial flow to the hand secondary to scleroderma, severe Raynaud phenomenon, hypothenar hammer syndrome, and laceration or embolization of the digital arteries. Sympathectomy is performed by circumferentially removing adventitia of the artery along a segment 1 to 4 cm (generally approximately 2 cm) long with the assistance of Loupe magnification or operative microscope.7-9
For the digital arteries, this is done by removing the adventitia from the common digital arteries and including the proximal part of both proper digital arteries of the affected digits, as branches into the proper digital arteries from the dorsal arch contain additional sympathetic fibers. For the index and little fingers, this would include the radial proper digital and the ulnar proper digital arteries, respectively. This is accomplished through a transverse incision centered at the distal palmar crease.7-9 For the thumb, digital sympathectomy is performed by removing a 2 cm length of adventitia on both the radial and ulnar digital arteries at the level of the metacarpophalangeal joint. For the radial artery, this is done by an incision made in the anatomical snuff box for access to the dorsal branch of the radial artery followed by circumferential stripping of the adventitia. 7
The precise mechanism underlying the phenomenon of vasospasm and vasoocclusion due to steroid injection remains unclear. However, a parallel can be drawn to the well-documented adverse events associated with epidural steroid injections. Among the risks of these injections is inadvertent intraarterial steroid administration, which can trigger stroke-like episodes affecting the brain or spinal cord, potentially leading to paraplegia. 10 Although the acute effects of steroids on vasculature are not extensively studied, evidence suggests that steroids can impact both the intimal lining and innervation of blood vessels.11-13 Studies indicate that steroids can exert significant effects on vasoregulation within minutes of injection, with potential longer term impacts on vascular smooth muscle cells.11-13 Furthermore, common additives in steroid preparations have been implicated in vascular and endothelial injury. 10
Although steroids have the potential to damage blood vessels, the primary theory regarding end-organ damage and ischemia revolves around the mechanical obstruction of the blood vessel lumen. Various theories exist regarding the mechanism behind this occlusion. Several studies have indicated that the particulate nature of certain steroids can lead to aggregation and microembolization following intravascular injection, ultimately resulting in vascular occlusion.10,14-16 Specifically, Depo-Medrol and Kenalog have been found to form large aggregates (>100 μm) in vitro, which have the potential to easily occlude vessels. 16 This theory finds further support in the findings of Okubadejo et al, who demonstrated that animals injected with methylprednisolone into their vertebral arteries exhibited neurologic deficits, whereas those injected with nonparticulate steroids showed no such effects. The authors even suggested that the use of nonparticulate steroids might mitigate such complications.
Laemmel et al, in their investigation to further elucidate the mechanism of aggregation and embolization, discovered that several particulate steroids, including prednisolone, methylprednisolone, and triamcinolone, triggered the formation of red blood cell (RBC) emboli in a mouse model. This process was associated with the transformation of RBCs into spiculated forms, and it was the unexpected agglutination of RBCs immediately after injection that was responsible for plugging arterioles. These findings further supported the notion that particulate steroids were culpable, as no change in perfusion was observed with the administration of cortivazol or dexamethasone. The precise mechanisms by which steroids induce alterations in RBC shape, as well as the roles of drug concentration, osmolarity, and viscosity, remain unknown. 17
However, Dawley et al presented some conflicting data, demonstrating (via a rat model) significant injury resulting from the intraarterial injection of the nonparticulate carrier of Depo-Medrol, in addition to particulate steroids. This suggests that the mechanism of injury may be more complex than previously thought, extending beyond the embolism of particulate matter. They proposed that injury may arise not only from particulate obstruction but also from the toxicity of the carrier or steroid itself. 14
However, despite the research that has been done regarding the effects of injected steroids, there is a paucity of literature about accidental intraarterial injection into the radial artery or treatment of this potential adverse event. Few case reports exist reporting acute ischemia following presumed injection of corticosteroids into the radial artery, and only in the setting of treating tenosynovitis. In one case from 1990, management involved thrombectomy combined with tissue plasminogen activator, thymoxamine, and heparin. 18 Unlike the cases in this study, however, that historical case benefited from immediate diagnosis and treatment, all occurring within 20 hours of the injury. In addition, we believed the underlying mechanism in our cases was multifactorial, making a simple thrombectomy insufficient. Another study reported a suspected intraarterial injection of the princeps pollicis artery following a steroid injection for trigger finger, resulting in soft tissue necrosis at the distal aspects of the second and third digits due to presumed retrograde flow. 19 This patient was treated conservatively with nonsteroidal anti-inflammatory drugs and pain control alone. 19 However, at the time of presentation, there was appreciable pulsatile Doppler flow on the volar pads of the affected fingers, which “influenced our decision not to perform a surgical intervention, such as a digital sympathectomy.” 19
Dihydropyridine calcium channel blockers and phosphodiesterase inhibitors have been employed in the treatment of ischemia of the hand in Raynaud phenomenon. 20 Nevertheless, in the case of patient 1, minimal to no improvement was observed despite the administration of a dCCB.
Anatomical landmarks are crucially important for proper steroid injection. As seen in Supplemental Figure 1a, easily identifiable landmarks of the thumb can be used to ensure proper needle insertion. Supplemental Figure 1b shows proper technique when injecting the CMC joint of the thumb, inserting the needle while applying distal traction to the thumb.
Although steroid injections of the CMC joint of the thumb are common and generally considered low-risk procedures, they can lead to serious consequences, such as inadvertent injection into the dorsal branch of the radial artery. This underscores the critical importance of adhering to proper technique and promptly recognizing and addressing complications as they arise. Accurately identifying anatomical landmarks and aspirating before injection may help prevent inadvertent injection into the artery.
The authors believe that if a patient presents with acute-onset signs and symptoms of ischemia distal to the site of a recent steroid injection of the CMC joint of the thumb, expedited treatment is warranted, and definitive treatment should be considered early. This could consist of performing a sympathectomy of the proper digital arteries of all affected fingers, as well as the radial artery, and, if the ulnar-supplied digits are affected, the ulnar artery as well. This approach has been shown to be effective in managing the condition and preventing further complications, making sympathectomy a viable treatment option in these cases.
Supplemental Material
sj-jpeg-1-han-10.1177_15589447251322915 – Supplemental material for The Use of Digital Hand Sympathectomies for the Treatment of Ischemia and Pain Following Inadvertent Corticosteroid Injection of the Radial Artery: Two Case Reports
Supplemental material, sj-jpeg-1-han-10.1177_15589447251322915 for The Use of Digital Hand Sympathectomies for the Treatment of Ischemia and Pain Following Inadvertent Corticosteroid Injection of the Radial Artery: Two Case Reports by Luke Anderson, Victoria Masear, Ashley Bentley and Grady Maddox in HAND
Footnotes
Authors’ Note
This abstract was also presented at the 2023 Alabama Orthopaedic Society Annual Hand Meeting.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Written informed consent was obtained from both patients whose cases and pictures are reported in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.