
Abstract
Proximal phalangeal fractures occur at a higher frequency than other phalanges, but the optimal management of these injuries remains subject to debate. The use of intramedullary screw (IMS) fixation has gained popularity over the last decade and aims to minimize extensor apparatus violation whilst providing adequate construct stability to allow early motion and rehabilitation. This systematic review aims to provide an updated analysis of patient- and clinician-reported outcome measures following fracture fixation using IMS in the proximal phalanx. A literature search was conducted using PubMed, Ovid Medline, Embase, and the Cochrane Controlled Register of Trials, yielding 16 studies with 204 fractures for inclusion. A mean total active motion of 237°, Quick Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) score of 3.58, and DASH score of 2.65 was revealed by pooled analysis of the included studies. A total complication rate of 6.4% was reported, including screw prominence, fracture displacement, infection, and flexion contracture. This updated systematic review finds good functional outcomes and a low complication rate following the use of IMS fixation for proximal phalangeal fractures.
Keywords
Introduction
Fractures in the hand are among the most common skeletal injuries and are being fixed with increasing frequency. 1 Proximal phalanx fractures occur at a higher frequency than other phalanges—despite their prevalence, the optimal management of these injuries remains subject to debate. 1
When requiring fixation, operative modalities must balance the need for rigid fixation to allow early motion and rehabilitation against the extensive soft-tissue dissection often required to achieve this stability. Kirschner wire (K-wire) insertion minimizes soft-tissue dissection, but a lack of stability often necessitates a period of immobilization prior to rehabilitation. 2 Furthermore, the wires may tether the extensor apparatus or lead to pin site infection. 2 Plate fixation has traditionally been performed through a dorsal tendon splitting approach and confers rigid stability—however, the greater invasiveness results in formation of adhesions which (in combination with the plate’s intimate contact with the extensor apparatus) results in decreased postoperative range of motion. 2 Alternate plate positions which do not violate the extensor apparatus have been proposed to preserve range of motion and function. 3
The use of intramedullary screw (IMS) fixation has gained popularity over the last decade and aims to minimize extensor apparatus violation whilst providing adequate construct stability to allow early motion and rehabilitation. 1 Intramedullary screw fixation has been associated with reduced operative time and substantial savings to both the individual patient and the health system when compared to alternative stabilization modalities.4,5 Promising early- to medium-term patient- and clinician-reported outcome measures have also been reported following IMS fixation of metacarpal, proximal phalangeal, and middle phalangeal fractures, with alternative insertion methods broadening the range of fractures in which this technique can be used.6-9
Although early reviews of outcomes following IMS fixation in the proximal phalanx were encouraging, there has been a proliferation of results since with no comprehensive evaluation. 9 Thus, the aim of this review was to provide an updated analysis of patient- and clinician-reported outcome measures following fracture fixation using IMS in the proximal phalanx.
Methods
This study was registered with PROSPERO. An electronic literature search was performed in June 2024 in accordance with PRISMA guidelines, using the databases PubMed, Ovid Medline, Embase, and the Cochrane Controlled Register of Trials (CENTRAL). 10 Various combinations of the search terms “proximal,” “phalanx,” “fracture,” “screw,” “intramedullary,” “minimally invasive,” and “compression” were used. After exclusion of duplicates, abstracts were screened for relevance before undergoing full-text appraisal by 2 independent reviewers (DCP and HF). The reviewers also evaluated the references of these papers to identify any additional studies for inclusion.
Studies were eligible for inclusion if they were published in the English language; reported primary data following the use of one or more IMSs for the fixation of proximal phalangeal fractures; and reported on at least one postoperative measure of function. Studies were excluded if they did not use IMS fixation; if the pathology treated was not a primary fracture; or if the study did not report an appropriate outcome measure. Any disagreements on inclusion were resolved via consensus or discussion with the senior author. In studies where only part of the cohort met the inclusion criteria, data were extracted for that subgroup only. In studies where data were not presented in an extractable manner, the corresponding authors were contacted to access the original data. Studies reporting cadaveric findings were not included in the review.
Studies were then graded by level of evidence as per the Journal of Bone and Joint Surgery (JBJS) criteria. 11 Data extracted included demographic and injury information; surgical approach; prostheses type; outcome measures including total active motion (TAM); and complications. Total active motion is defined by the American Society for Surgery of the Hand as the sum of active motion of the metacarpophalangeal and interphalangeal joints of a digit and can be compared to an uninjured contralateral digit or a norm of 260°. 12 Major complications included infection, nonunion, malunion, arthrosis, and symptomatic hardware requiring removal. Minor complications included stiffness, delayed union, clicking, and asymptomatic hardware removal. All data were displayed in tables, with simple statistical analysis performed where appropriate.
Studies were appraised using Cochrane’s Risk of Bias in Non-randomized Studies (ROBINS-1). 13 The risk of bias across 7 domains was rated as low to critical by 2 authors (DCP and HF). Where there was discrepancy, the risk of bias was discussed with the senior author. These are presented in Figure 2, using the Robvis tool. 14
Results
The electronic search yielded 428 studies for screening. Following the removal of duplicates and irrelevant studies through title and abstract screening, 24 studies remained for full review (Figure 1). Sixteen studies were deemed eligible for inclusion, with 10 reporting on proximal phalanges alone (Table 1), and an additional 6 reporting mixed data for proximal and middle phalanges, where isolated data were not available (Table 2). All articles were published after 2015 and were consistent with Level 4 evidence as per the JBJS criteria. 11
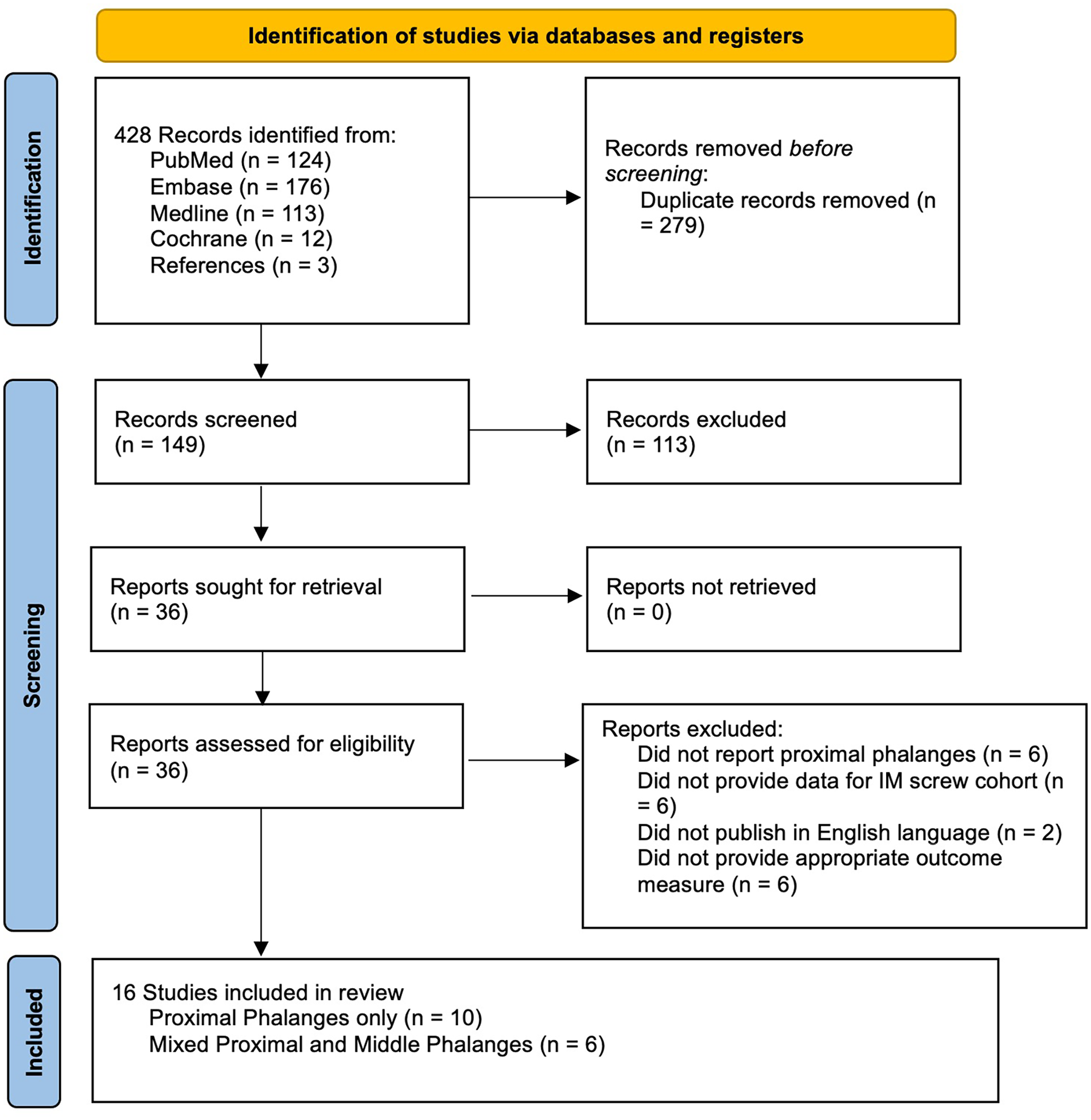
PRISMA search flow diagram. 10
Patient Demographics and Surgical Technique for Cohort of Proximal Phalanges Only.

Note. IM = intrameduallry; CCS = cannulated compression screws; DTJ = double threaded screw Japan; HCS = headless compression screws.
Pooled demographics for the cohort of metacarpal and phalangeal fractures.
Complications and Outcomes Proximal Phalanges Only.

Note. TAM = total active motion; AROM = active range of motion; DASH = Disabilities of the Arm, Shoulder, and Hand; VAS = visual analog scale; MCPJ = metacarpophalangeal joint; PIPJ = proximal interphalangeal joint; DIPJ = distal interphalangeal joint; PROMIS UE = Patient-Reported Outcomes Measurement Information System Upper Extremity; MC = metacarpal.
When considering the proximal phalanx cohort alone, a total of 204 fractures were reported with a mean patient age of 39 years (16-67). Most of the 204 fractures were treated using an antegrade intra-articular approach (82), followed by antegrade transarticular (68) and retrograde intra-articular (54). Compression screws from a variety of manufacturers were used, as demonstrated in Table 1. A mean TAM of 237° was revealed by pooled analysis of the 8 studies that reported this metric.
Pooled analysis of Quick Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) demonstrated a mean of 3.58 (3 studies),6,22,23 and assessment of DASH scores finding a mean of 2.65 (3 studies).15,16,18 Thirteen complications were noted, yielding a total complication rate of 6.4%. These complications included 7 hardware removals for screw prominence, 3 revisions for displacement, 2 infections, and 1 flexion contracture.
Grip strength was reported in 7 of the included studies. Four studies reported this metric as a percentage of the contralateral side, finding a pooled average of 92.57%.16,18,21,24 The remaining 3 measured grip strength via a Jamar dynamometer, noting a pooled average of 26.72 kg.22,25,26
When assessing the mixed cohort of proximal and middle phalangeal fractures, an additional 231 fractures were considered, resulting in a total cohort of 435 phalangeal fractures. A similar distribution of retrograde and antegrade surgical approaches is demonstrated in Tables 3 and 4 for this mixed cohort, with pooled analysis revealing a mean TAM of 234°. The complication profile was also similar, with a further infection requiring screw removal following union; 3 patients undergoing hardware extraction for prominence; and 3 revisions due to loss of fracture reduction.
Patient Demographics and Surgical Technique for Mixed Cohort of Proximal and Middle Phalanges.

Note. CCS = cannulated compression screws; HCS = headless compression screws.
Complications and Outcomes for Mixed Cohort of Proximal and Middle Phalanges.

Note. TAM = total active motion; DASH = Disabilities of the Arm, Shoulder, and Hand.
Discussion
This systematic review provides an updated analysis of the use of intramedullary screw fixation in proximal phalangeal fractures, finding excellent patient- and clinician-reported outcomes with a low complication rate. Intramedullary screw fixation is a safe and effective method of stabilization in proximal phalangeal fractures.
These findings are consistent with the literature on the use of intramedullary screws in a broader range of hand fractures. Beck reviewed 169 metacarpal neck and shaft fractures, reporting 100% radiographic union, a mean TAM of 251° and grip strength of 96% compared to the contralateral side. 30 Hug assessed 958 hand fractures (metacarpal, proximal phalangeal and middle phalangeal) and reported a similar mean TAM of 243°; a grip strength of 97.5% of the contralateral limb; DASH score of 3.7; and a major complication rate of less than 1%. 31 Additional benefits of IMS fixation include a shorter mean operating time of 26.4 minutes; quicker return to work (mean time off work of 7.3 weeks); and cost savings to both the individual and the health system, when compared to plate fixation.5,31
Minimally invasive techniques are particularly pertinent in phalangeal fractures, where an intimate relationship between the bone and surrounding soft tissues entails that tendon disruption, periosteal stripping, and prominent hardware result in the formation of adhesions. These adhesions lead to postoperative stiffness, which impairs function and delays return to normal activities. 3 The postoperative TAM noted in our review (pooled mean of 237°) compares favorably with that demonstrated for plating (which ranges from 183° to 248°).32,33 When performing plating for proximal phalangeal fractures, minimization of extensor apparatus disruption is beneficial, with Sivakumar et al 3 noting an improvement in TAM of 8.5° in a meta-analysis comparing tendon splitting to sparing approaches. The use of IMS also obviates the risk of flexor tendon irritation following dorsal plating, due to the presence of volar midline longitudinal grooves in both the proximal and middle phalanx which can obscure excessive screw penetration. 34
Intramedullary screw fixation also affords the compression and construct stability required for early rehabilitation, in contrast to the utilization of K-wires; in addition, K-wire stabilization may result in tethering of the apparatus and pin site infections. 2 Horton et al 2 reported a high complication rate in his series of 17 proximal phalangeal fractures treated with K-wires, noting 2 superficial infections, 1 deep infection, and 3 patients requiring extensor tenolysis for stiffness. The 0.98% infection rate noted in our review of IMS fixation compares favorably with that noted in the literature following the use of K-wires, which ranges from 7% in a series of 1213 patients undergoing fixation of hand and wrist fractures to more than 15% where the wires were left proud.35,36
These promising clinical outcomes are supported by in vitro studies. Ibanez et al 37 reported greater rigidity and load to failure with the use of IMS as compared to lateral plating in polyurethane models, whilst Miles et al 38 demonstrated equivalent interfragmentary displacement over 2000 flexion and extension cycles following stabilization with IMS or plate fixation in cadaveric short oblique proximal phalangeal fractures. Sivakumar et al 39 found that both IMS and lateral plate fixation afford enough stability in transverse mid-shaft proximal phalangeal fractures to withstand the likely forces associated with early active motion in a cadaveric model (although dorsal plating was significantly stiffer).
Cadaveric studies have also been used to alleviate concerns regarding the degree of articular surface disrupted following IMS insertion. Borbas et al 40 employed digital imaging to calculate involvement of 4.5% and 8.5% of the proximal phalanx base when using 2.2 and 3.0 mm screws, respectively, with no difference being found between intra- and transarticular insertion. del Piñal et al 17 used computed tomography to estimate violation of between 18% and 25% of the proximal phalangeal head when 2.5 and 3.0 mm screws were inserted in a retrograde fashion (albeit most of the relatively nonarticulating intercondylar sulcus). Although these lesions are unlikely to significantly redistribute reaction forces and result in arthritis in the nonload-bearing joints of the upper limb, we recommend retrograde K-wire insertion with antegrade IMS instrumentation wherever possible to diminish the relative proportion of articular cartilage disrupted, as well as the avoidance of corresponding “kissing” lesions via transarticular insertion. 9
Choice of stabilization modality of proximal phalangeal fractures is dictated by numerous factors, including surgical specialty, volume of phalangeal fractures treated, practice location, and surgeon experience. A survey of hand surgeons in Australia noted that orthopedic surgeons and less-experienced clinicians were more likely to advocate for IMS fixation, which may demonstrate greater familiarity with intramedullary constructs and newer techniques. 1 Nonetheless, the results of this review and the relevant literature suggest that IMS fixation should be considered over other modalities whenever possible.
This systematic review has several limitations. The studies included were predominantly case series, with few comparative studies amenable to meta-analysis. These case series inherently confer risk of bias due to their observational nature, lack of a control group and unblinded measurement of outcomes. As a result, Figure 2 highlights a “serious” risk of bias assessment across all included studies. Variation in reporting precluded pooled analysis of several outcome measures (such as grip strength), and 6 studies reported mixed outcomes of proximal and middle phalangeal fractures that were unable to be separated. Data heterogeneity limited further stratification and analysis based on variables such as fracture characteristics, which may be useful in confirming the indications and relative contraindications for this fixation technique.
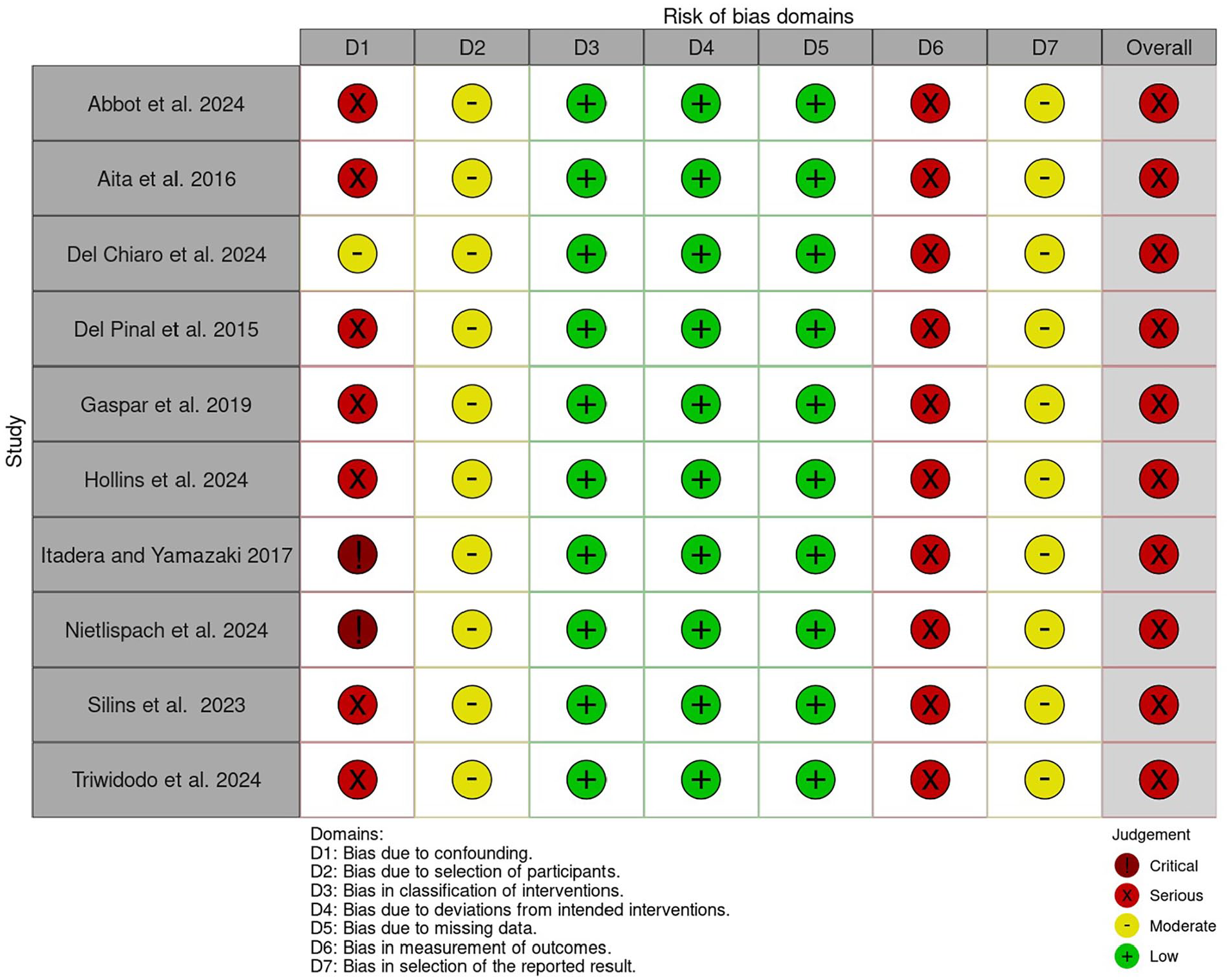
Risk of bias graph for this study. 14
However, this updated systematic review finds good functional outcomes and a low complication rate following the use of IMS fixation for proximal phalangeal fractures. These results contribute to the growing body of evidence supporting the use of IMSs as a safe and effective technique with several important advantages over alternate methods of fixation.
Footnotes
Ethical Approval
This study was approved by our Institutional Review Board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Given this is a review of previously published data, ethical approval was not required.
Statement of Informed Consent
This is a review article using only pooled, previously published data, and informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.