
Abstract
Background:
We investigated associations of cannabis and tobacco use with complications after open reduction and internal fixation (ORIF) of wrist fractures.
Methods:
We retrospectively analyzed PearlDiver data from 337 538 patients who underwent ORIF for wrist fractures from 2010 to 2022. We identified 5587 patients with a history of cannabis use disorder (“cannabis group”); 12 806 patients with a history of tobacco use and no history of cannabis use disorder (“tobacco group”), and 310 108 patients with no history of cannabis use disorder or tobacco use (“control group”). We excluded patients with a history of using other illicit drugs. Propensity matching was used to control for age, sex, and comorbidity burden. Demographic characteristics, comorbidity profiles, and medical and surgical complications were compared using chi-squared tests. Complications were assessed within 90 days after surgery. Postoperative outcomes were also stratified by fracture location. Alpha = .05.
Results:
Compared with the control group, the cannabis group had a significantly higher incidence of all medical complications and of fracture malunion, nerve injury, and tendon, muscle, or fascia injury. Compared with the tobacco group, the cannabis group had significantly lower incidence of sepsis, pneumonia, deep venous thrombosis, urinary tract infection, nerve injury, and wound dehiscence.
Conclusions:
Compared with nonusers of cannabis and tobacco, cannabis users had a higher incidence of several medical and surgical complications after ORIF for wrist fractures. These findings will help physicians better anticipate complications in patients who use cannabis or tobacco.
Introduction
The recent legalization of cannabis in many US states has catalyzed an uptick in its consumption for medicinal and recreational use.1,2 In the past decade, there was an approximate 20% increase in recreational cannabis use. 3 Furthermore, from 2020 to 2022, there was a 23% increase in the population prevalence of licensing for medical cannabis use. 4 This increase is largely attributed to the medical benefits of cannabis, including for management of pain and symptoms of psychological disorders. 5 Therefore, it is important to understand the association of its use with complications after surgical procedures.
Research has assessed the association between cannabis use and complications after total joint arthroplasty. In a meta-analysis of studies of total joint arthroplasty, cannabis use was associated with higher odds of deep vein thrombosis (DVT), unplanned revision surgery, and pneumonia. 6 These results are similar to those after total shoulder arthroplasty, where the incidence of deep and superficial infections is higher in cannabis users. 7 Little is known about how cannabis use affects medical and surgical outcomes of upper-extremity fracture care. However, the effects of cannabis on general bone healing have been widely discussed in the literature. In 2022, Heath et al 8 published a comprehensive study on the orthopedic effects of cannabis, reporting that cannabis users have higher risk of delayed bone healing, lower bone mineral density, and a higher incidence of fractures compared with nonusers. Given the effects cannabis has, we hope to further determine how its use may affect patients with upper extremity fractures.
In this study, we investigated the associations between cannabis use and complications after open reduction and internal fixation (ORIF) of wrist fractures, stratified by location in the distal radius, scaphoid, and ulnar shaft. Outcomes of interest were the 90-day incidence of medical complications and 6-month incidence of surgical complications after ORIF. By identifying risks associated with cannabis use in this context, we hope to inform clinical practices and guidelines to improve patient outcomes after upper extremity surgery.
Methods
Data Source
This study was a retrospective review of the PearlDiver national insurance claims database (https://pearldiverinc.com). PearlDiver contains health data for more than 157 million patients in the United States from January 2010 through April 2022. We chose the PearlDiver database because its large data set enabled a robust analysis of postoperative outcomes in a diverse, nationwide patient sample. Each included patient is assigned a unique identifier, which facilitates longitudinal tracking of health information. This feature also enables deidentification of the data; therefore, this study was deemed exempt from institutional review board approval (IRB00387181).
Patient Selection
Using Current Procedural Technology (CPT) codes and International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes (Supplemental Table 1), we identified 442 879 patients who had undergone ORIF in 1 of the 3 locations in the wrist: the distal radius, scaphoid, or ulnar shaft. We excluded 97 875 patients with incomplete records, 7466 with a history of illicit drug use other than cannabis, and 9037 with a history of malignancy, leaving 328 501 patients for analysis. Of this group, 292 618 (89%) had distal radius fractures, 21 851 (6.7%) had scaphoid fractures, and 14 032 (4.3%) had ulnar shaft fractures (Figure 1). The primary analysis focuses on distal radius fractures because of their predominance in the data set. Scaphoid and ulnar shaft fractures are presented to provide additional insights.
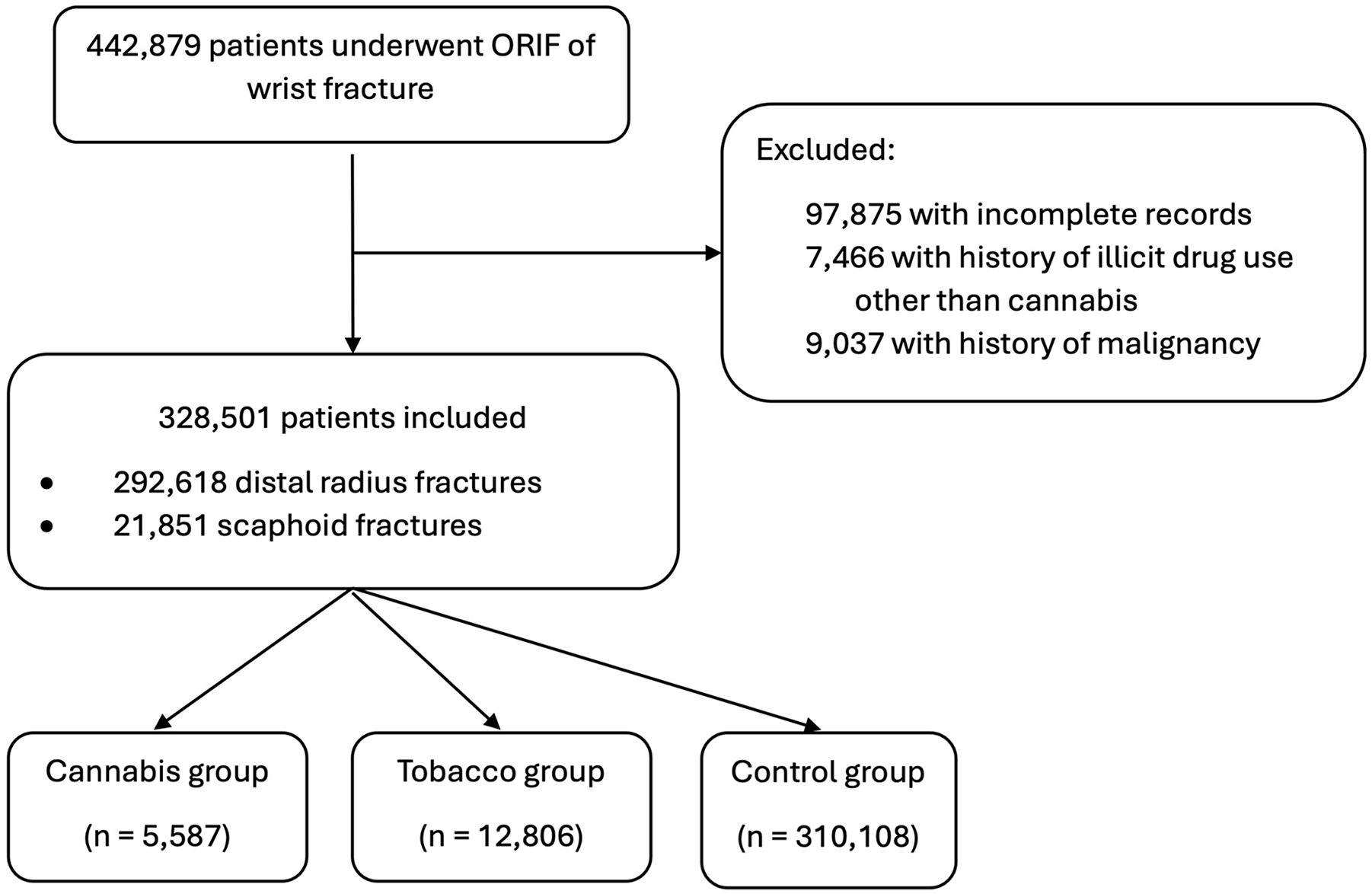
Patient selection flowchart.
Patients were stratified into three groups. The “cannabis group” consisted of 5587 patients (1.7%) with a history of cannabis use disorder, cannabis dependence, nondependent cannabis abuse, or unspecified forms of cannabis abuse and excluded patients with tobacco use. The “tobacco group” consisted of 12 806 patients (3.9%) with ICD-9 or ICD-10 code-defined diagnoses of tobacco use or tobacco use disorders and excluded patients with a history of cannabis use. The “control group” consisted of 310 108 patients (94%) with no recorded history of cannabis or tobacco use. Lastly, we analyzed complications by fracture type to identify any differences that may be related to cannabis use and specific fracture types.
Patient Characteristics
Patient characteristics queried in this study were age, biological sex, and Charlson Comorbidity Index (CCI) values. Charlson Comorbidity Index is a numerical representation of a patient’s likelihood of death according to the patient’s comorbid conditions and is a validated reflection of comorbidity burden. 9
The cannabis group was younger (mean ± standard deviation, 33 ± 15 years) than both the tobacco group (46 ± 19 years) and control group (46 ± 19 years) (both, P < .001). The mean CCI value in the cannabis group (1.3 ± 1.8) was lower than that of the tobacco group (2.0 ± 2.4) and higher than that of the control group (0.97 ± 1.7) (both, P < .001). The sex distribution also differed among the groups, with the proportions of men being 66% in the cannabis group, 44% in the tobacco group, and 36% in the control group (all, P < .001). The groups were also compared in terms of specific comorbidities at baseline, the results of which are shown in Table 1.
Demographic Characteristics and Comorbidities of Patients Who Underwent Open Reduction and Internal Fixation of Wrist Fractures, PearlDiver Database, 2010-2022.
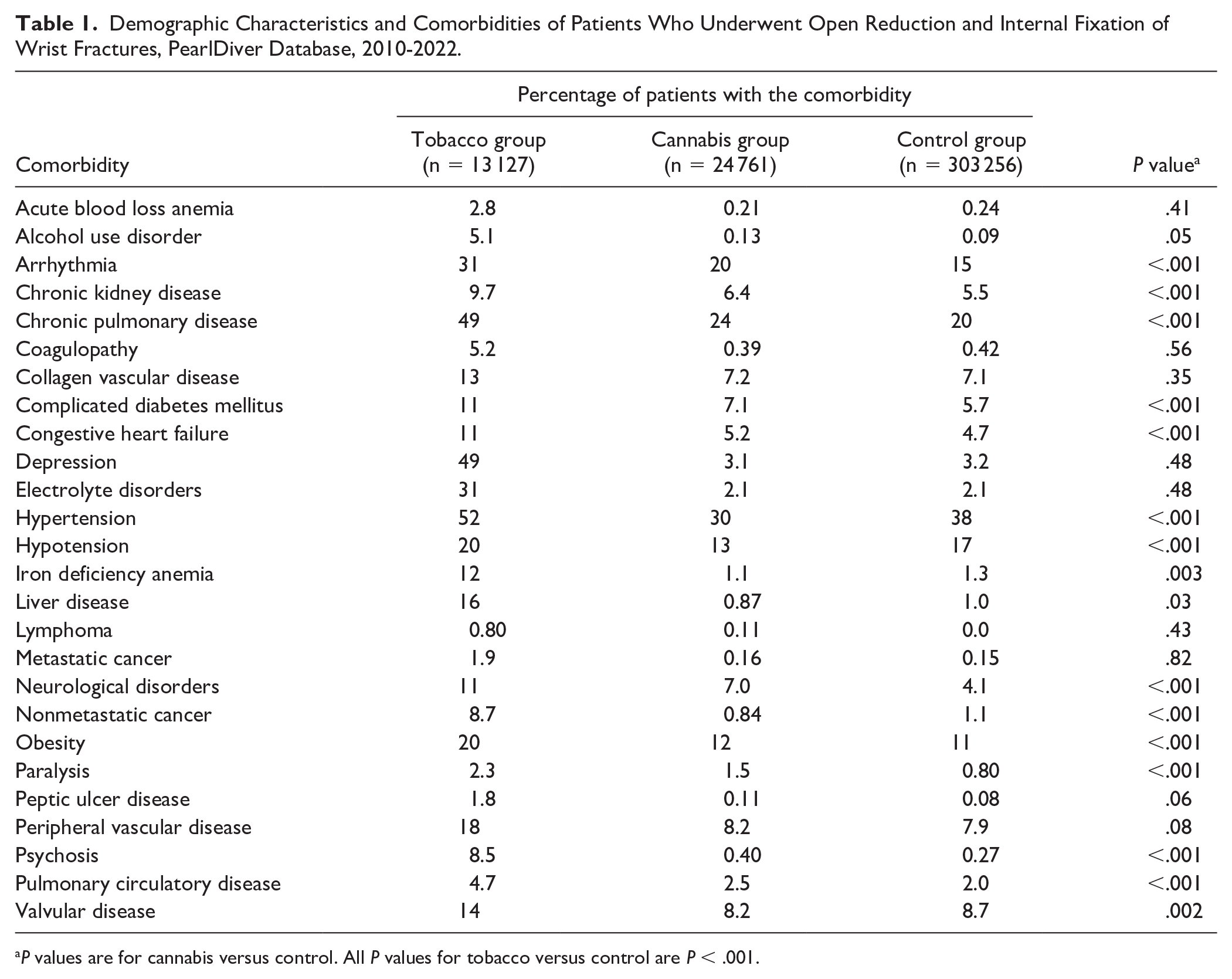
P values are for cannabis versus control. All P values for tobacco versus control are P < .001.
Outcome Measures
Our primary outcome measures were the 6-month incidence of surgical complications after ORIF, including fracture malunion, nerve injury, and tendon or muscle injury. Medical complications are presented to provide context regarding the overall health risks associated with cannabis and tobacco use. Surgical complications comprised malunion; nerve injury; nonunion; repair or revision; tendon, muscle, or fascia injury; vessel injury; and wound dehiscence. Medical complications were categorized as severe (acute kidney injury [AKI], cardiac arrest, myocardial infarction, pulmonary embolism, sepsis, and stroke), moderate (deep vein thrombosis [DVT], pneumonia, and superficial surgical site infection [SSI]), or mild (hypoglycemia and urinary tract infection [UTI]).
Statistical Analysis
We used R software (R Foundation for Statistical Reporting, Vienna, Austria) provided through the PearlDiver system to perform statistical analysis. To minimize confounding factors, we used propensity score matching in a 1:4 ratio of the cannabis group to both the tobacco and control groups to control for age, biological sex, and CCI value. Propensity score matching was used to minimize confounding from differences in age, sex, and comorbidity burden. While cannabis users exhibited higher rates of comorbidities, this analysis highlights their association with both medical and surgical complications.
Differences in baseline characteristics and comorbidities were assessed using Student t tests and chi-squared tests for continuous and categorical variables, respectively. Chi-squared tests were also used to assess differences in the incidence of medical and surgical complications after ORIF. P values < .05 were considered significant.
Results
Surgical and Medical Complications
Cannabis versus control group
Compared with the control group, the cannabis group had a higher incidence of malunion (P = .009), nerve injury (P < .001), and tendon, muscle, or fascia injury (P = .04) and a higher incidence of all medical complications (Table 2). We found no difference between the cannabis and control groups in the incidence of nonunion, repair or revision, vessel injury, or wound dehiscence.
Surgical Complications Within 6 Months and Medical Complications Within 90 Days After Open Reduction and Internal Fixation of Wrist Fractures, PearlDiver Database, 2010-2022.
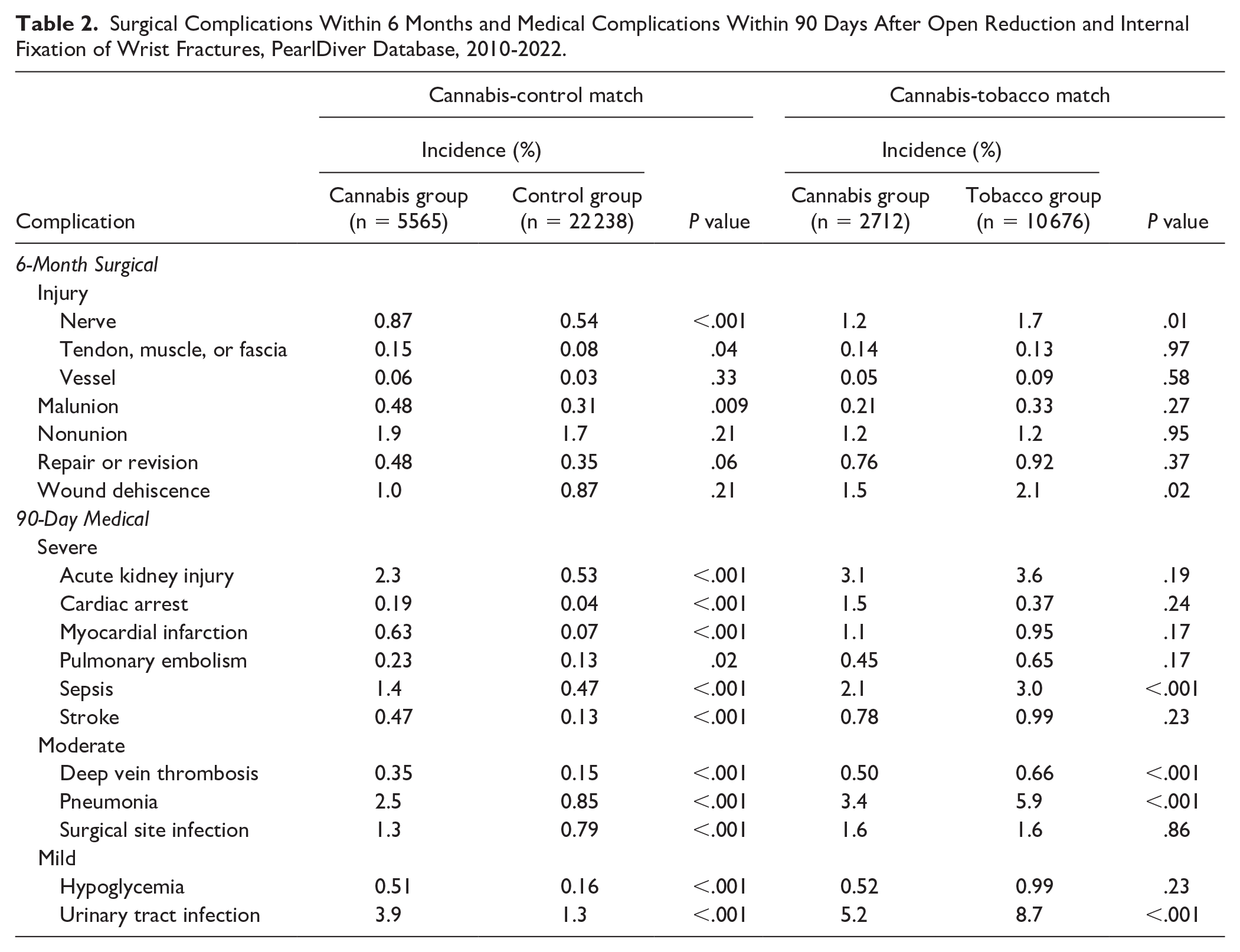
Cannabis versus tobacco group
Compared with the tobacco group, the cannabis group had a lower incidence of nerve injury (P = .015) and wound dehiscence (P = .02) but no difference in the incidence of malunion; nonunion; repair or revision; tendon, muscle, or fascia injury; or vessel injury. Compared with the tobacco group, the cannabis group had a lower incidence of DVT, pneumonia, sepsis, and UTI (all, P < .001). We found no differences in the incidence of AKI, cardiac arrest, hypoglycemia, myocardial infarction, pulmonary embolism, stroke, or SSI between the cannabis and tobacco groups.
Outcomes by Fracture Type
Distal radius
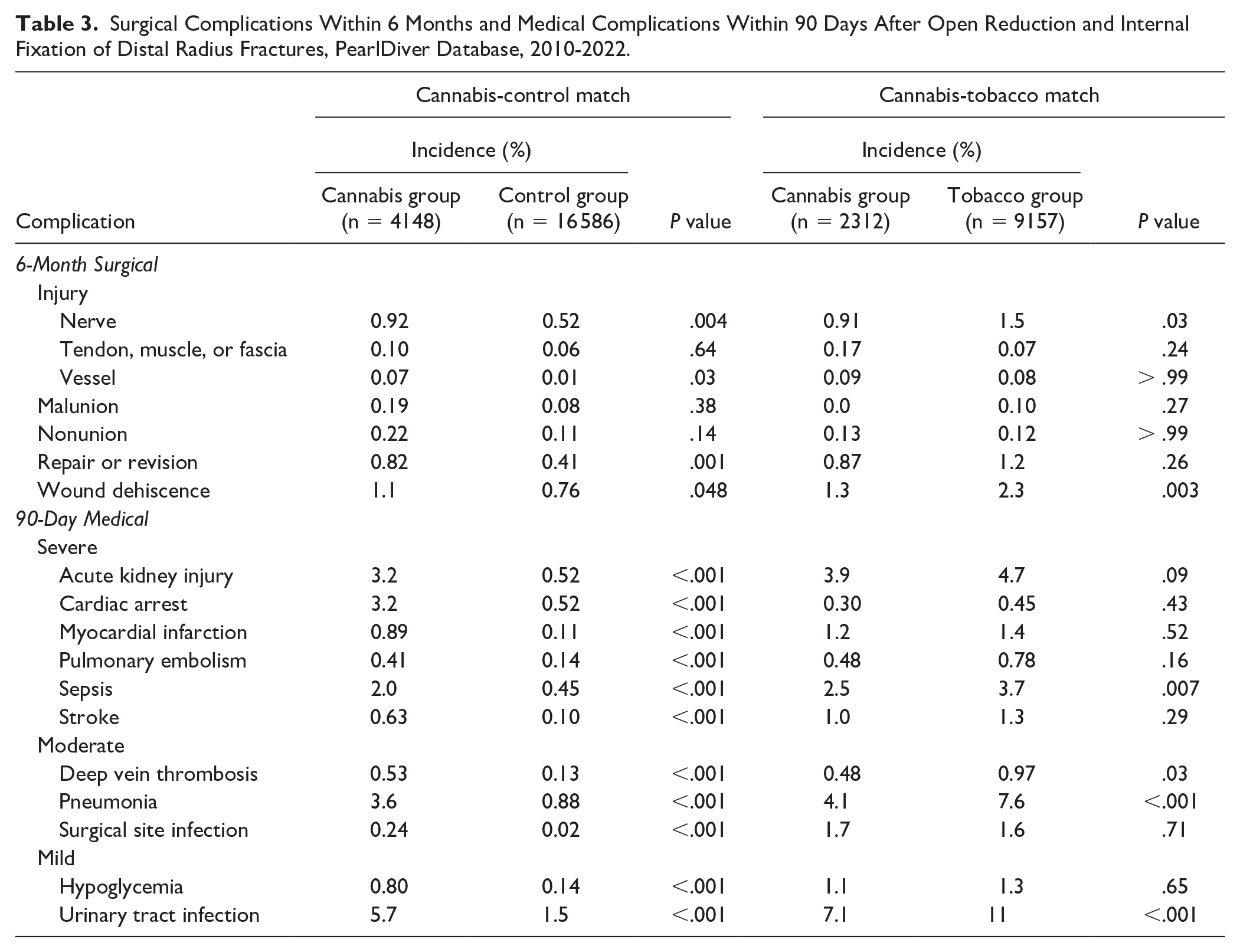
Compared with the control group, the cannabis group had higher incidence of nerve injury (P = .004), repair or revision (P = .001), vessel injury (P = .03), and wound dehiscence (P = .048). Compared with the tobacco group, the cannabis group had lower 6-month incidence of nerve injury (P = .03) and wound dehiscence (P = .003).
For patients who underwent ORIF of the distal radius, those in the cannabis group had higher incidence of every medical complication compared with the control group (all, P < .001; Table 3). Compared with the tobacco group, those in the cannabis group had lower incidence of DVT (P = .03), pneumonia (P < .001), sepsis (P = .008), and UTI (P < .001).
Surgical Complications Within 6 Months and Medical Complications Within 90 Days After Open Reduction and Internal Fixation of Distal Radius Fractures, PearlDiver Database, 2010-2022.
Scaphoid
The cannabis group had a higher incidence of SSI (P = .03) than the tobacco group. Compared with the control group, the cannabis group had higher incidence of wound dehiscence (P < .001) and nonunion (P = .006). Compared with the tobacco group, the cannabis group had higher incidence of nonunion (P = .03). In patients who underwent ORIF for scaphoid fracture, those in the cannabis group had higher incidence of AKI (P < .001), hypoglycemia (P = .006), myocardial infarction (P = .006), pneumonia (P < .001), sepsis (P = .006), stroke (P = .03), SSI (P < .001), and UTI (P = .001) compared with the control group (Supplemental Table 2).
Ulnar shaft
Compared with the tobacco group, the cannabis group had no differences in incidence of any medical or surgical complication. In patients who underwent ORIF for ulnar shaft fracture, those in the cannabis group had higher incidence of AKI (P = .001), hypoglycemia (P = .01), pneumonia (P = .001), sepsis (P = .004), stroke (P = .01), SSI (P = .001), and UTI (P < .001) compared with the control group (Supplemental Table 3).
Discussion
The legalization of cannabis in many US states has led to a sharp increase in use during the past decade. It is important that we understand how this use may lead to differences in complications after surgery. We found that, compared with patients with no documented cannabis or tobacco use, those with documented cannabis use had higher incidence of numerous medical and surgical complications after ORIF for hand or wrist fracture. Interestingly, we found no difference in the 6-month incidence of surgical complications between cannabis and tobacco users. Moreover, after ORIF for scaphoid fracture, the cannabis group had higher incidence of surgical site infection and nonunion than the tobacco group did. These results can help surgeons tailor postoperative care according to the cannabis- and tobacco-associated risks their patients face and to be mindful of the higher risks of surgical and medical complication.
Oster et al 10 conducted a similar study using the PearlDiver database on infection risk after total knee arthroplasty. Within their tobacco, cannabis, and co-user groups, there was a higher risk of myocardial infarction, respiratory failure, and surgical site infection compared with controls. The increase among all groups demonstrates the importance of delineating differences in surgical outcomes between patients with cannabis versus tobacco use. Ultimately, these findings are similar to the results of our study, suggesting that cannabis use may increase surgical wound–related complications.
One notable finding of our study is that cannabis users had higher incidence of surgical complications compared with the nonusers. In 2022, Heath et al 8 published a comprehensive analysis of the orthopedic effects of cannabis. They found that cannabis users were at greater risk for delayed bone healing, lower bone mineral density, and fractures compared with nonusers. 8 Other studies have found associations between cannabis use and longer time to wound healing as a result of SSI, joint infections, and wound infections.7,11 A cohort study published in 2023 compared postoperative outcomes in cannabis and tobacco users. Similar to our findings, they reported that cannabis users experienced higher risk of infection and malunion after operative treatment of distal radius fractures. 12
In our study, patients with cannabis use generally had a higher incidence of complications than nonusers did. Our findings agree with those of previous studies of surgical fracture fixation. A retrospective study published in 2023 compared perioperative outcomes between cannabis users and nonusers after elective surgical procedures. 13 The authors found higher incidence of complications and death among cannabis users compared with nonusers. 13 Specifically, they found higher odds of AKI, stroke, respiratory complications, infections, and surgical complications after propensity score matching. 13 It is noteworthy that despite using a different database, their findings were similar to those of our study. Another retrospective cohort study published in 2023 found higher incidence of postoperative pneumonia, cerebrovascular disease, pulmonary embolism, respiratory failure, and surgical site infection in patients who used cannabis compared with nonusers. 14
Despite the higher incidence of various medical complications among cannabis users in our study, our analysis shows intriguing distinctions between cannabis users and a matched group of tobacco users. Cannabis users had lower incidence of pneumonia, DVT, UTI, and sepsis within the same period compared with tobacco users. While these findings underscore the heightened risks associated with cannabis use relative to controls, the overall lower risk for these specific outcomes compared with those of tobacco users suggests a nuanced risk profile. In a study conducted in Tucson, Arizona, chronic cough was observed less frequently in individuals who smoked only marijuana compared with those who smoked tobacco. However, when both substances were smoked together, the effects on cough and sputum production appeared to be additive. 15
It is important to consider these differences when evaluating the risks associated with each substance. In the Vancouver-based Burden of Obstructive Lung Diseases study of adults older than 40, marijuana use alone was not associated with higher odds of chronic respiratory symptoms, but combined use of marijuana and tobacco was associated with of higher odds (OR 2.6, 95% CI, 1.6-3.6) compared with tobacco alone. 16 This comparison helps to place cannabis-related risks in context, showing that while cannabis use is a risk factor, its effects on certain postoperative complications may not be as severe as those of tobacco use. Additionally, during the 6-month postoperative period, cannabis users had lower incidence of nerve injury and wound dehiscence compared with tobacco users. These differences suggest a complex interplay between substance use and surgical outcomes that have been shown in previous literature. In a retrospective study published in 2023, both cannabis and tobacco users were at higher risk for hypoxia, venous thromboembolism, pulmonary complications, and cardiac complications after spine surgery compared with non–substance users. 17 Notably, even when analyzing those who used only tobacco, the risk of complications remained higher than for cannabis users, which is in accordance with our results.
Prior research has identified that cannabis users have increased comorbidity burdens, which could in part explain the higher rate of medical complications. It is important to determine which factors are responsible for the higher rate of complications among cannabis users and whether they are related to cannabis use itself or to other medical conditions. Future studies should explore additional variables that may influence complications after ORIF, such as socioeconomic status, geographic location, and access to health care services. In addition, qualitative data (eg, patient-reported outcomes, health care provider perspectives) could offer greater insight into the experiences and perceptions of patients undergoing ORIF who use cannabis or tobacco. These findings highlight the need for preoperative counseling for patients who use cannabis or tobacco, emphasizing potential risks and the importance of personalized perioperative care. They also underscore the importance of tailored perioperative planning and risk stratification. There is no indication for withholding surgical intervention based on substance use alone. Such analysis could provide a more holistic understanding of the factors influencing postoperative complications. This study provides novel insights into the differential impact of cannabis and tobacco use on surgical outcomes, contributing to the broader understanding of substance use in orthopedics.
This study has several limitations. First, the retrospective design prevents the determination of causality and may introduce biases and confounding factors that could influence the observed associations. Second, the PearlDiver database relies on the manual input of providers and is subject to inaccuracies that may skew the data in either direction. However, the large sample size, encompassing many national insurance claims, supports the generalizability of our findings. Third, we lacked information on the method, frequency, and type of cannabis use, preventing us from analyzing how these factors may be associated with postoperative complications. Despite our effort to separate groups, underreporting of cannabis or tobacco use may have led to misclassification. This limitation highlights the need for future studies with detailed clinical and substance use data. Information on nonsteroidal anti-inflammatory drug (NSAID) use, including duration, was not available in the data set. Prior research suggests that extended NSAID use may impair bone healing and influence postoperative outcomes, 18 highlighting the need for future research to incorporate detailed medication histories.
Conclusion
This study sheds light on the 6-month surgical complications after ORIF for wrist fracture experienced by patients who use cannabis. These findings underscore the importance of considering cannabis use as a potential risk factor during perioperative care planning and emphasize the need for tailored approaches to improve outcomes and enhance patient counseling in wrist fracture management. It is also important that providers be vigilant during postoperative care because of the greater incidence of surgical complications within 6 months and medical complications within 90 days. Future research can help identify the underlying mechanisms and develop strategies to mitigate the adverse effects of cannabis use on postoperative recovery. By addressing these questions, we can improve care for the growing number of orthopedic patients who use cannabis.
Supplemental Material
sj-docx-1-han-10.1177_15589447251336399 – Supplemental material for The Highs and Lows of Fracture Fixation: Complications After Wrist Fracture Fixation for Users of Cannabis, Tobacco, or Neither Substance
Supplemental material, sj-docx-1-han-10.1177_15589447251336399 for The Highs and Lows of Fracture Fixation: Complications After Wrist Fracture Fixation for Users of Cannabis, Tobacco, or Neither Substance by Arman Kishan, Victoria E. Bergstein, Blake Prieskorn, Stanley Zhu, Ansh Kishan, Thomas P. Cancian, Visakha Suresh, Pawel P. Jankowski, Sami H. Tuffaha and Dawn M. LaPorte in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447251336399 – Supplemental material for The Highs and Lows of Fracture Fixation: Complications After Wrist Fracture Fixation for Users of Cannabis, Tobacco, or Neither Substance
Supplemental material, sj-docx-2-han-10.1177_15589447251336399 for The Highs and Lows of Fracture Fixation: Complications After Wrist Fracture Fixation for Users of Cannabis, Tobacco, or Neither Substance by Arman Kishan, Victoria E. Bergstein, Blake Prieskorn, Stanley Zhu, Ansh Kishan, Thomas P. Cancian, Visakha Suresh, Pawel P. Jankowski, Sami H. Tuffaha and Dawn M. LaPorte in HAND
Supplemental Material
sj-docx-3-han-10.1177_15589447251336399 – Supplemental material for The Highs and Lows of Fracture Fixation: Complications After Wrist Fracture Fixation for Users of Cannabis, Tobacco, or Neither Substance
Supplemental material, sj-docx-3-han-10.1177_15589447251336399 for The Highs and Lows of Fracture Fixation: Complications After Wrist Fracture Fixation for Users of Cannabis, Tobacco, or Neither Substance by Arman Kishan, Victoria E. Bergstein, Blake Prieskorn, Stanley Zhu, Ansh Kishan, Thomas P. Cancian, Visakha Suresh, Pawel P. Jankowski, Sami H. Tuffaha and Dawn M. LaPorte in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors. The data used in this study were derived from the PearlDiver national insurance claims database, which contains de-identified patient information, and was deemed exempt from institutional review board (IRB) approval
Statement of Informed Consent
The data used in this study were obtained from the PearlDiver national insurance claims database, which contains de-identified health information of patients. Given that the data are anonymized and no direct patient contact was involved, individual informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.