
Abstract
Background:
Social determinants of health (SDOH) encompass various factors of one’s environment and have been shown to strongly influence patient health. The effect of SDOH has been evaluated in various medical specialties; however, a paucity of literature exists investigating the effects of SDOH on outcomes in hand surgery. As such, we completed a RAND/University of California Los Angeles (UCLA) Delphi Appropriateness process for the purpose of guiding the inclusion of SDOH domains and measurement constructs in hand surgery clinical research.
Methods:
A consortium of 9 academic upper-limb surgeons completed a RAND/UCLA Delphi Appropriateness process to evaluate the importance, feasibility, usability, and scientific acceptability of collecting SDOH domains and measurement constructs in hand surgery clinical research. The domains and measurement constructs were collated from frameworks and tools from the U.S. Department of Health and Human Services, the Centers for Medicare and Medicaid Services, and Cochrane. Panelists rated each domain/measurement construct on an ordinal scale between 1 (definitely not important/feasible/usable/supported) and 9 (definitely important/feasible/usable/supported) in 2 rounds with an intervening face-to-face discussion. Agreement and validity were determined according to previously validated and pre-defined criteria.
Results:
The consortium achieved agreement on the inclusion of 5 SDOH domains (Education Access and Quality, Health care Access and Quality, Neighborhood and Built Environment, Social and Community Context, and Economic Stability) and 21 measurement constructs.
Conclusions:
As there is growing evidence that SDOH can differentially impact patient health, these validated domains and constructs can help prioritize and guide hand surgery research to evaluate and better inform interventions related to SDOH and outcomes.
Keywords
Introductory
Social determinants of health (SDOH), factors that encompass aspects of one’s environment including where a person is born, grows, works, lives, learns, worships, and ages, are being increasingly recognized given their influence on health and quality of life. The effect of SDOH on health has been evaluated in various populations and medical specialties. For example, authors have demonstrated associations between SDOH factors like socioeconomic status (SES) and mortality and life expectancy. 1 Other variables (literacy, residence location) have been demonstrated to have strong associations with health outcomes.2,3 Although the causal mechanisms between SDOH and health outcomes are likely multifactorial and still being elucidated, it is widely accepted that their association with health outcomes is often stronger than of traditional health care. For example, medical care has been estimated to account for only 10% to 20% of the modifiable contributors to health outcomes, whereas the other 80% to 90% is attributable to SDOH. 4
Such phenomena are also seen across surgical specialties. For example, Bennett et al 5 demonstrated that a patient’s SES was a strong predictor of operative mortality with a single level increase in patient SES leading to a decrease in operative mortality risk of 7%. Jarman et al 6 demonstrated that the odds of patient death increased by 8% for every 5-mile increase in distance from the closest trauma center and by 81% when the nearest trauma center was publicly owned, highlighting disparities in community resources and access associated with a patient’s place of residence.
As a result, the Centers for Medicare and Medicaid Services (CMS) approved the measurement of SDOH on an inpatient basis in medical facilities that report to the Inpatient Quality Reporting Program. Specifically, reporting of variables including food insecurity, housing instability, and transportation needs have been recommended in 2023 but will be required in 2024. 7 Furthermore, CMS highlighted the importance of equity and SDOH with their inclusion in its “Universal Foundation” of performance measures for value-based care 8 and plan to implement and use equity-specific measures. 9 This information can be used not only for risk stratification and in understanding the impact of SDOH on quality, but also to inform interventions to improve care in an equitable manner.
Notably, however, a paucity of clinical research exists in hand surgery investigating the effect of SDOH domains on outcomes. Thus far, SDOH measurement constructs such as race/ethnicity and insurance status have been associated with disparate access and outcomes in hand surgery literature.10,11 These studies, however, are often conducted in isolation and lack the inclusion of other SDOH (e.g. food insecurity, patient language) that have been identified in other fields to have strong associations with health. Improved data collection of such SDOH variables in hand surgery clinical research may improve our understanding of the effects of SDOH on outcomes such that interventions can be developed and implemented to support equitable care. As such, we used a multistep Delphi process to evaluate the validity of assessing SDOH domains and measurement constructs to guide the inclusion of SDOH in hand surgery clinical research.
Materials and Methods
Identification of SDOH Domains and Measurement Constructs
Institutionally accepted SDOH frameworks were applied to this investigation. The U.S. Department of Health and Human Services’ Healthy People 2030 Initiative 12 categorizes SDOH into 5 discrete domains: Education Access and Quality, Health Care Access and Quality, Neighborhood and Built Environment, Social and Community Context, and Economic Stability. Domains are overarching categorizations that broadly describe how various underlying measurement constructs within that domain collectively assess SDOH. Measurement constructs are quantifiable subcategorizations within each domain that more discretely identify and define mechanisms by which SDOH domains can affect health. The SDOH measurement constructs used in this article were collated from the CMS’ Accountable Health Communities Health-Related Social Needs Screening Tool 13 and the Cochrane Equity PROGRESS-Plus health opportunities and outcomes framework 14 and subsequently subdivided into the domains based on definitions provided by the Healthy People 2030 Initiative for each of the 5 domains. In total, 21 SDOH measurement constructs were identified (Supplemental Table 1).
Systematic Review of 21 SDOH Measurement Constructs
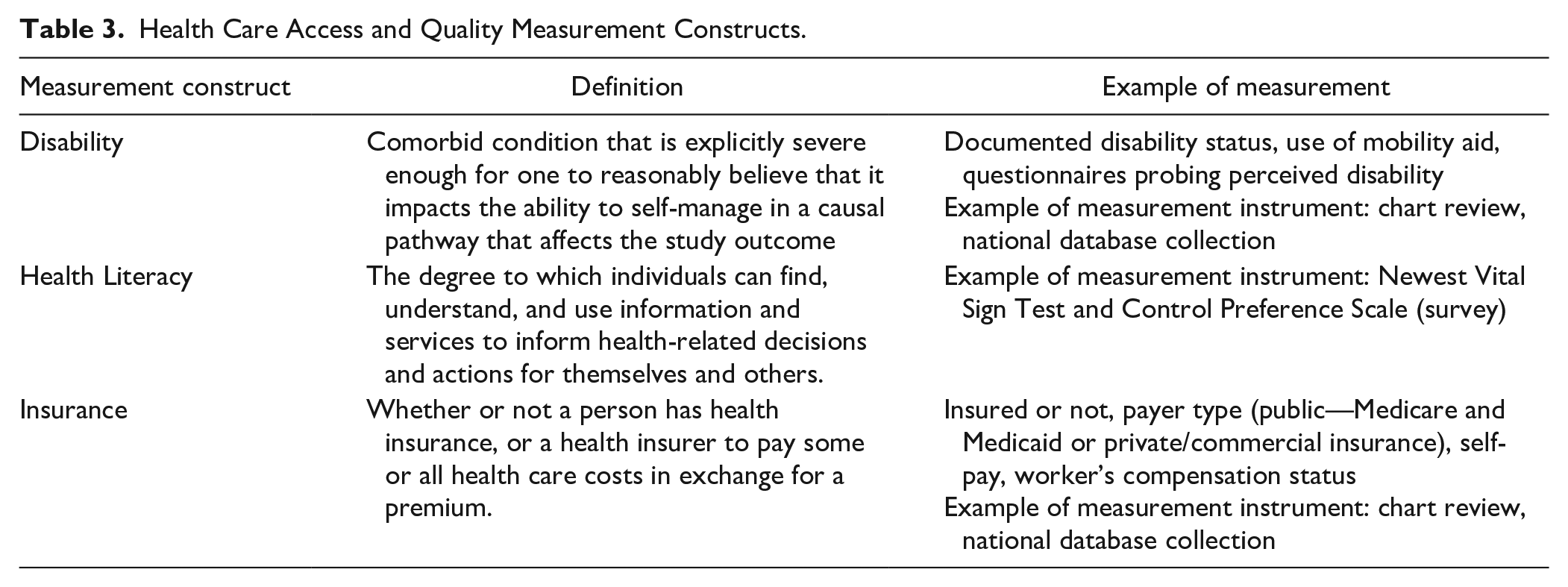
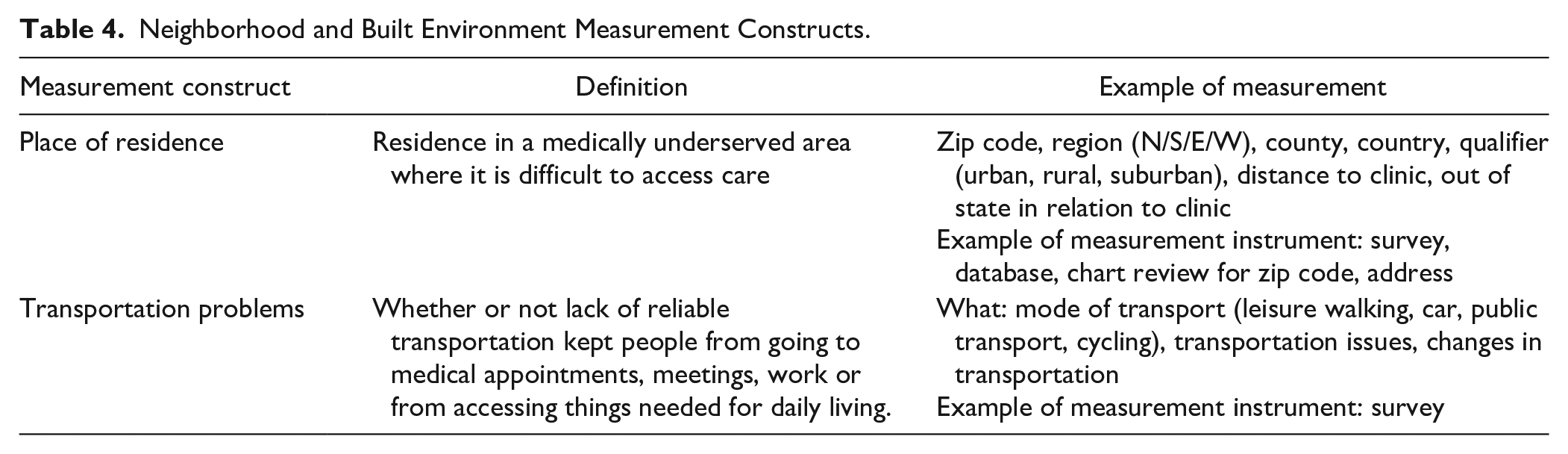
To assess the current understanding of SDOH in hand surgery clinical research, we aggregated the 21 SDOH measurement constructs and completed a systematic review of hand surgery literature using the MEDLINE/PubMed database in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15 We created and used a specific search algorithm that included terms such as “social determinants of health,” “adverse outcomes,” and common hand surgery conditions, along with similar terms related to SDOH, adverse outcomes, and hand surgery procedures. An initial search by the primary author (CO) yielded 4101 articles, from which 709 articles were included and reviewed, as they investigated at least one of the 21 SDOH measurement constructs as an explanatory variable in a hand surgery study. Systematic reviews were excluded, and a date restriction of only papers published after 2000 was applied. Each of the 709 articles was categorized by the SDOH measurement construct(s) they investigated and whether the study demonstrated adverse outcomes in association with differing categorizations within that measurement construct. For example, although age is routinely reported in clinical research, its differential effect on the outcome being studied was evaluated. Finally, summaries of measurement constructs, along with their supporting evidence from the systematic review, were provided to the Hand Surgery Quality Consortium (HSQC) members for their review and voting. Supporting evidence for each measurement construct included its source, definition, percent use in upper extremity literature based on the systematic review (Table 1), and examples of how the construct was measured (Tables 2-4 and Supplemental Tables 2-4).
Social Determinants of Health Construct Frequency and Associations with Adverse Outcomes in Hand Surgery Literature Based on Systematic Review.
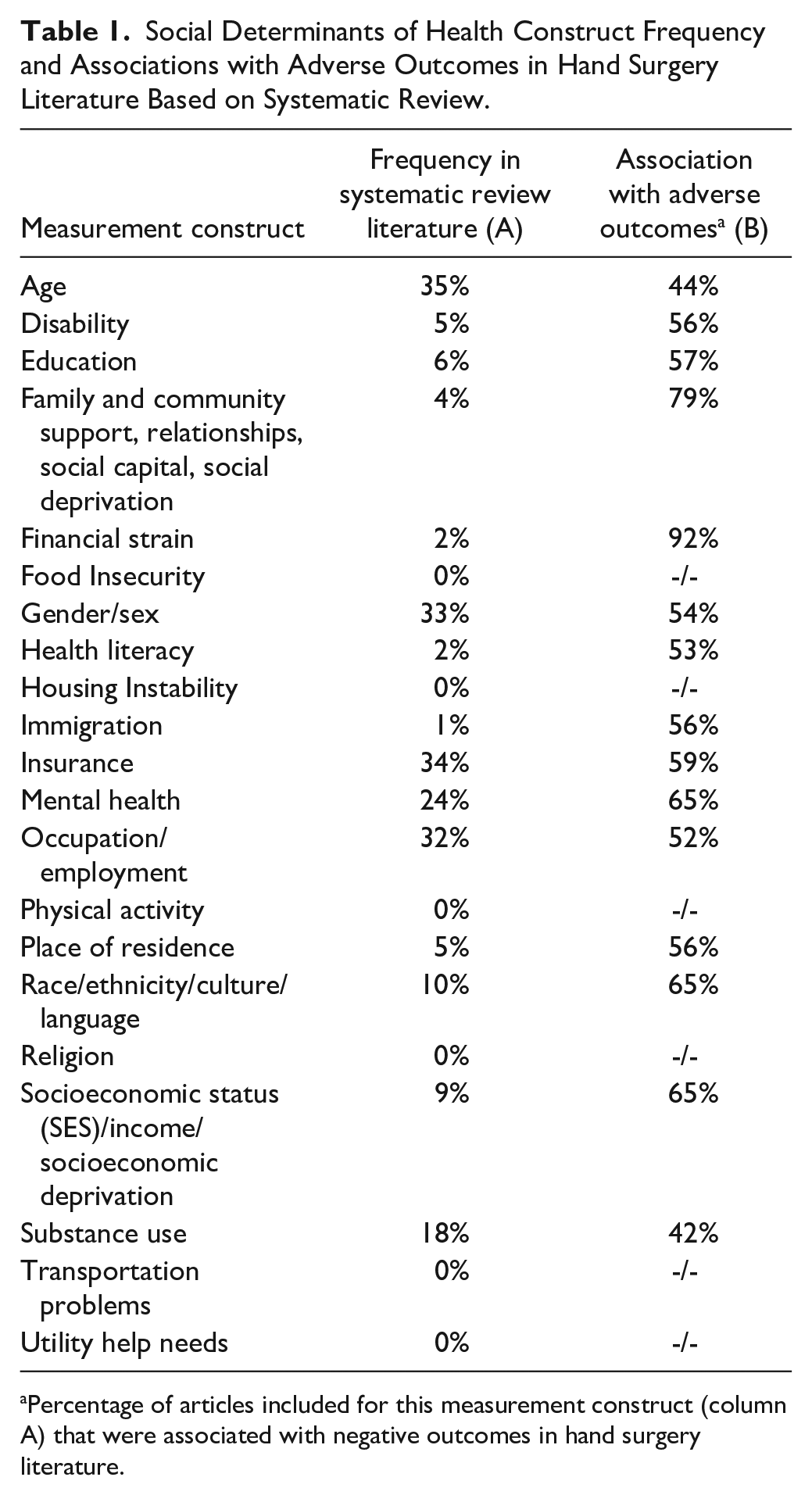
Percentage of articles included for this measurement construct (column A) that were associated with negative outcomes in hand surgery literature.
Education Access and Quality Measurement Constructs.

Health Care Access and Quality Measurement Constructs.
Neighborhood and Built Environment Measurement Constructs.
SDOH Domain and Measurement Construct Evaluation
We conducted a modified RAND Corporation/University of California Los Angeles (UCLA) Delphi Appropriateness process 16 to evaluate the 5 domains and 21 measurement constructs (within the 5 domains) (Figure 1), based on 4 voting criteria: importance, feasibility, usability, and scientific acceptability. The 9 members of the HSQC who served as panel experts in this study are fellowship-trained hand surgeons and experts in quality, with diverse practice patterns and geographic location and who have previously used the RAND/UCLA Delphi Appropriateness methodology.

The U.S. Department of Health and Human Services’ healthy people 2030 initiative categorizes SDOH into 5 discrete domains: Education access and quality, health care access and quality, neighborhood and built environment, social and community context, and economic stability.
The 4 voting criteria (importance, feasibility, usability, and scientific acceptability) that were originally outlined by the National Quality Forum (NQF), were modified such that they apply to a clinic research context instead of a clinical setting. The RAND/UCLA Appropriateness methodology gathers the collective opinion of experts and allows these experts to discuss their answers in a face-to-face meeting. Furthermore, the method produces appropriateness criteria that have face, construct, and predictive validity.17,18
RAND/UCLA Delphi Scoring for the Inclusion of SDOH Domains/Measurement Constructs in Hand Surgery Research
The RAND/UCLA Delphi process involves 2 rounds of independent ratings of SDOH domains and constructs (preliminary and final). An in-person face-to-face group discussion takes place between rounds. Scoring was completed according to the RAND/UCLA process. Each member rates each domain/measurement construct according to the 4 voting criteria on a scale of 1 to 9, (with 1 as definitely not important/feasible/usable/scientifically acceptable, 5 as uncertain or equivocal importance/feasibility/usability/scientifically acceptability, and 9 being definitely important/feasible/usable/scientifically acceptable) using an anonymous online survey platform (Qualtrics, Provo, Utah) (Table 5). For each domain and measurement construct, each panelist voted on the 4 criteria: importance, feasibility, usability, and scientific acceptability. The median score for importance, feasibility, usability, and scientific acceptability was calculated for each domain and measurement construct in the preliminary and final rounds. According to prior work, for any one criterion, if no more than 2 of the 9 ratings were outside of the 3-point range that included the median (1-3, 4-6, 7-9), panelists were considered to be in agreement. If 3 or more ratings fall within the 1 to 3 range whereas 3 or more ratings fall within the 7 to 9 range, panelists were considered to be in disagreement. All other scenarios were considered indeterminate. A domain or measurement construct was considered a valid domain or measurement construct to use in hand surgery research if the median score (calculated only from the final round of voting) was at least 7 (within the range of 7-9) for all 4 criteria, with no more than 2 panelists rating outside of the range of 7 to 9 for all 4 criteria. 19
National Quality Forum SDOH Domain/Measurement Construct Voting Criteria.
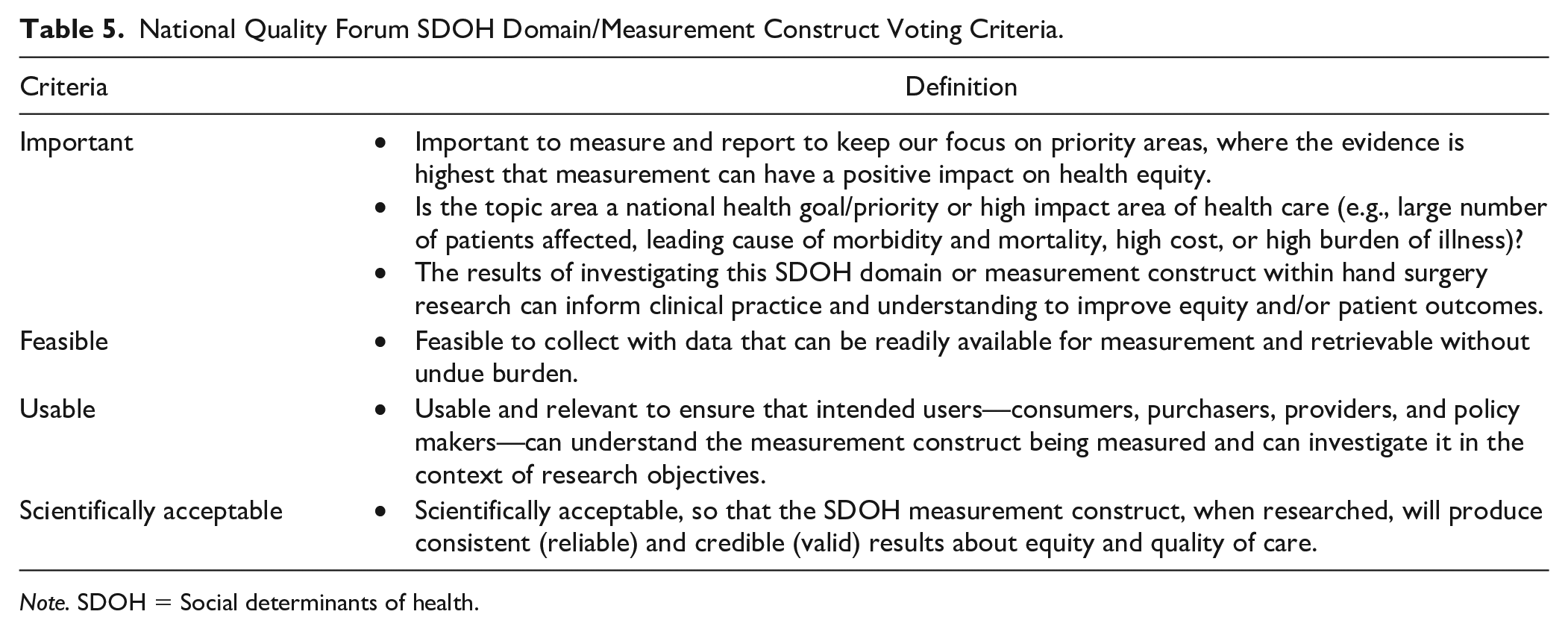
Note. SDOH = Social determinants of health.
Scoring Process
Before the preliminary round of voting and the face-to-face meeting, HSQC panelists were provided the opportunity to suggest additional domains and measurement, as well as the opportunity to provide open-ended commentary accompanying their votes for each of the 4 criteria pertaining to each domain and measurement construct. At the face-to-face meeting, panelists were provided with aggregate results, along with individual scores for each domain and measurement construct. The chair (RNK) facilitated an in-person discussion of the SDOH domains and measurement constructs based on the 4 criteria in the context of the relevant literature, as well as a presentation of the preliminary voting results and associated open-ended commentary for each SDOH domain and measurement construct. The chair of the discussion was a nonvoting member. Subsequently, panelists completed the second (final) round of independent ratings within 1 week of discussion using the same anonymous online voting platform. The results of the second round of the Delphi are reported as the final consensus of the group. Results were tabulated and analyzed according to the above criteria.
Results
The panel reached agreement that all 5 SDOH domains (Education Access and Quality, Health Care Access and Quality, Neighborhood and Built Environment, Social and Community Context, and Economic Stability) were important, feasible, usable, and scientifically acceptable in their use for hand surgery clinical research. Similarly, the 21 measurement constructs within each of the 5 domains reached agreement. As such, the 5 SDOH domains and 21 measurement constructs were deemed valid. For example, within the Health Care Access and Quality domain, all measurement constructs (disability, health literacy, and insurance) achieved agreement for importance, feasibility, usability, and scientific acceptability to be measured in hand surgery clinical research. The results of voting for each domain and measurement construct for all 4 criteria are shown in Supplemental Table 5.
Although all domains and SDOH measurement constructs achieved agreement in the final vote, panelists did not initially assess all SDOH variables as important, feasible, usable, and scientifically acceptable (Supplemental Table 6). Panelists expressed concerns about how SDOH constructs might be measured and whether certain constructs could potentially be confounded with others. For example, panelists highlighted that health literacy should be clearly delineated from a patient’s ability to read or write. Similarly, financial strain and utilities help might seem confounding. Panelists also expressed confusion about how a patient’s place of residence might be measured. The discussion also evolved to identify a potential scale for measuring family and community support. While panelists agreed that food insecurity is an important construct, they questioned the feasibility of its use in hand surgery. The importance of religion was noted to be region-specific and various constructs including mental health, substance use, and SES were highlighted as having sensitivities that may affect the accuracy of their measurements.
Discussion
While SDOH are institutionally recognized by the U.S. Department of Health and Human Services and within the medical field as having a strong influence on patient health, there remains a gap in understanding their effects on many common hand conditions, thus preventing the design and implementation of interventions to ensure equitable care. The 5 domains and 21 measurement constructs that were validated for collection in research elucidate the range of SDOH variables that can be included in hand surgery clinical research to address this gap. Researchers, funding agencies, and journals may use these results to support the collection of SDOH variables in hand surgery research. As different SDOH constructs are measured in hand surgery, understanding their effects on outcomes can help inform interventions to mitigate health care disparities.
Each SDOH domain has a demonstrated association with outcomes in various medical specialties, warranting further investigation in hand surgery. For example, education level, categorized within the Education Access and Quality domain, may correlate to poor long-term outcomes, such as the ability to return to work after an injury. A study of injured patients admitted to a level 1 trauma center demonstrated that low education levels were associated with functional limitations, long-term pain, and posttraumatic stress disorder. 20 Building upon the deleterious effects of education level on long-term outcomes, low health literacy, a Health Care Access and Quality construct was demonstrated by Mahoney et al 21 to be significantly associated with postoperative hospital visits among bariatric patients. Measurement constructs within the Neighborhood and Built Environment domain, such as transportation problems, also influence outcomes. Namely, Jiang et al 22 identified that transportation barriers increased patient mortality risk. Constructs classified under the Social and Community Context domain have similarly been associated with disparate postoperative outcomes. A study of food insecurity and postoperative colorectal surgery outcomes illustrated that patients experiencing high food insecurity had greater odds of nonelective surgery, 90-day readmission, and decreased odds of having standard postoperative outcomes. 23 Likewise, in a study of the Economic Stability domain, as measured through the SES construct, Barrie et al 24 demonstrated that patients with lower SES had greater rates of 3-month opioid prescription renewal and that SES was independently associated with longer length of stay and increased emergency room visits. The adverse outcomes associated with various SDOH domains/constructs demonstrate that studying these variables in hand surgery may further elucidate disparities in patient care and outcome heterogeneity in clinical research and unveil unaddressed phenomena that informs interventions to improve patient outcomes.
Guided by studies such as those previously discussed, numerous health care systems have begun incorporating screenings of SDOH variables into their clinical practices. Notably, a national study of SDOH screenings demonstrated that 79% of respondent hospitals screened for at least one health-related social need, with food security and interpersonal violence being the most frequently screened. 25 The New York Presbyterian Hospital at Columbia University implemented the Accountable Health Communities tool in 4 hospital-affiliated primary-care clinics. Using this tool, patients were screened for SDOH including depression and substance use. 26 Boston Medical Center has implemented electronic health record-based screening that identifies SDOH using International Classification of Diseases: 10th Revision (ICD-10) codes and generates resource referral guides that are relevant to social contexts upon patient request. 27 Similarly, in 2019, a tool that screened for SDOH variables such as food risk, intimate partner violence risk, social connection risk, alcohol risk, and transportation risk was implemented at Mayo Clinic, with results demonstrating that 59% of screenings were completed. 28
The integration of such screening protocols varies by system and should be tailored to the context. It is possible that in some contexts, screening may be best achieved prior to a new patient’s arrival to clinic (via email and/or electronic health record [EHR] message), while in some contexts, completion on a tablet or paper in clinic prior to seeing the physician may be best. Given the importance and sensitivity of the information obtained, it is critical that the results are reviewed by a team member and integrated into patient care as needed. Similar to PROM administration, 29 there is no one-size-fits-all approach to data collection, and we recommend that multiple options be available that are tailored to the clinical context and the patient.
Screening tools should be used to accurately measure the presence of SDOH constructs. While screening tools have been identified targeting almost every construct outlined in this article, only a few of these measurement constructs have been particularly emphasized in terms of their implications and importance for patient outcomes. Specifically, the U.S. Preventive Services identified housing instability, food insecurity, transportation difficulties, utility needs, interpersonal safety, education, and financial strain as important constructs to assess social risk. Furthermore, the Task Force collated screening tools and assessed the frequency of measurement of each SDOH construct. Through key informant interviews, they concluded that food security, housing instability, and transportation difficulties were the most important social risk factors to identify within health care. 30 This review demonstrates the importance of each domain on hand surgery outcomes (e.g. racial variation in the treatment of thumb amputations, 31 socioeconomic factors associated with outcomes after distal radius fractures, 32 the association of insurance type, 33 and patient preferred language 34 with time to surgery and outcomes). Given the importance of such variables, Appendix demonstrates a sample data collection that can be used to streamline collection in clinical and research scenarios.
Providers may also choose to focus on screening for one measurement construct at a time. Interpersonal safety, which would be categorized under the family and community support/relationships construct, can be measured using tools such as the Humiliation, Afraid, Rape, Kick (HARK) questionnaire and the Partner Violence Screen (PVS). 35 Similarly, the Homelessness Screening Clinical Reminder (HSCR) is a questionnaire used by the Veterans Health Administration to screen for housing instability. The 6-item and 18-item U.S. Household Food Security Survey Modules (HFSSM) screens for food insecurity by including prompts such as “In the last 12 months, were you every hungry but didn’t eat because there wasn’t enough money for food?”36,37 These tools can each be applied to measure the presence and impact of various SDOH constructs in clinical practice.
While SDOH can be assessed as identifiable proxies for disparate health outcomes, they may also serve as targets for designing practical interventions to address such disparities. For example, to address the language barriers within the Social and Community Context domain, Karliner et al 38 provided patients with limited English proficiency professional interpreters in the hospital and noted a significant decrease in 30-day readmission rates. This demonstrates a system-level modification that can help mitigate an SDOH leading to poor outcomes. Similarly, to address poor outcomes related to the Health Care Access and Quality domain, Enard and Ganelin 39 implemented a patient navigator program that decreased the odds of patients returning to the emergency department for conditions that were preventable or treatable with primary care. These examples highlight that beyond identifying SDOH as barriers to high-quality care, SDOH can also be targeted for tailored interventions addressing disparate clinical outcomes.
To begin designing interventions in hand surgery that address patient health disparities, understanding which SDOH domains are most impacting patients can inform the highest need(s). This model of studying SDOH to create frameworks for addressing them has been exemplified by prominent institutional bodies like the American Cancer Society, which has studied the impact of SDOH on outcomes after cancer diagnosis and has paired each with interventions (Figure 2). 40 For example, the transportation SDOH is paired with ridesharing as an intervention that may address access to care. This framework highlights the possible interventions that can be provided to benefit patient outcomes in hand surgery.
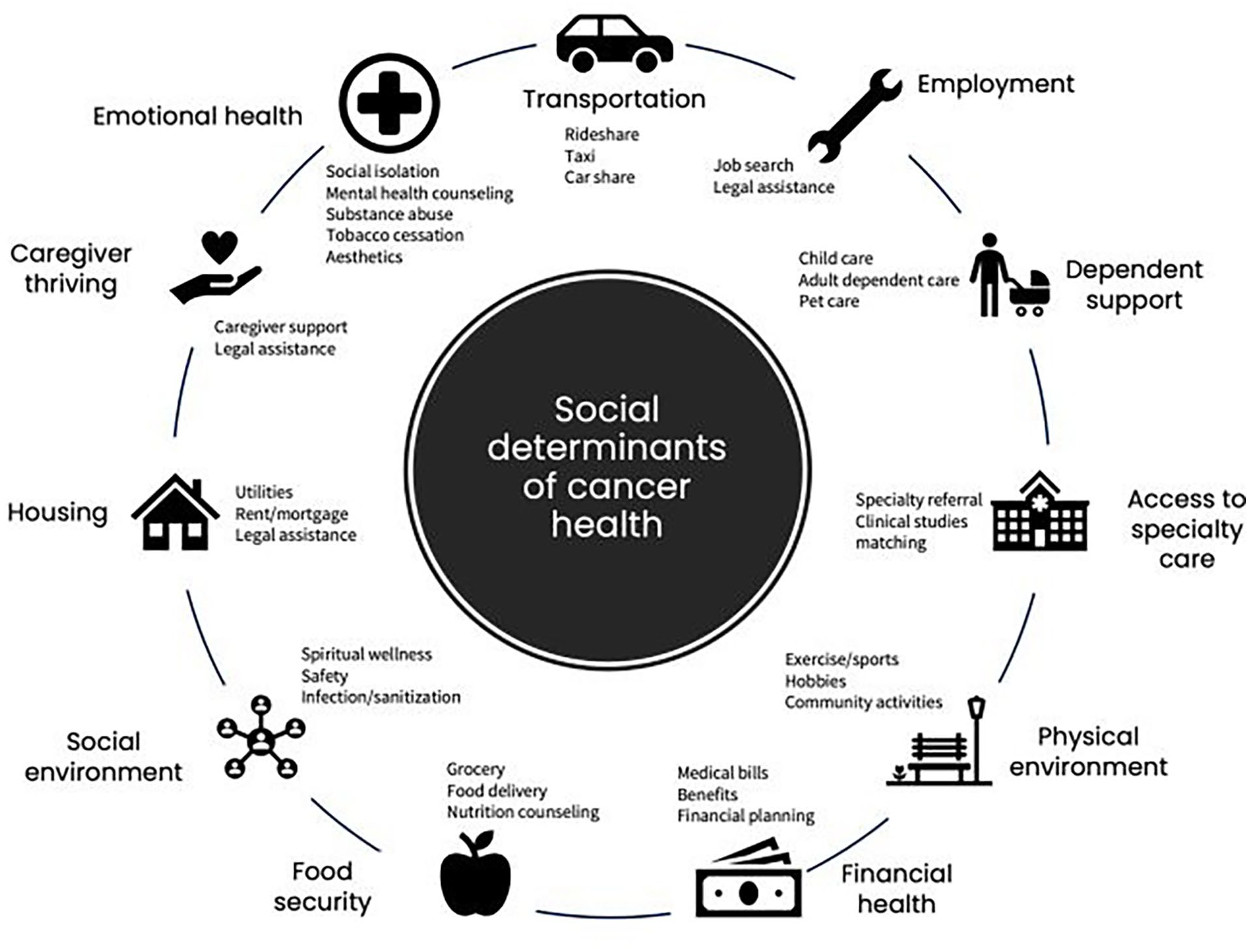
The American Cancer Society highlights various SDOH and specifies potential interventions to address each. Reprinted with permission from the American Cancer Society.
Although 5 domains and 21 constructs were validated, the comprehensive collection of all these variables in clinical research may not be feasible (e.g., time constraints). These results are meant to guide the collection of domains and constructs to illuminate associations between historically ignored SDOH variables in clinical research and outcomes in hand surgery. Furthermore, while solely collecting such data is unlikely to induce change, its reporting and analysis may generate improved understanding of drivers of health inequity and improved measurements/delivery of quality care. In practice, many constructs have various instruments by which they can be measured (i.e., multiple tools to measure literacy), some of which may be more readily available than others (i.e., coded variables vs patient report). Future work may focus on developing and validating a parsimonious and feasible measure set to assess SDOH in clinical research and practice.
These results should be viewed in the context of the study’s limitations. The modified Delphi approach introduces limitations, including panelist bias and the modification of the NQF criteria definitions. It is possible that differential results may have been demonstrated with a larger or different panel; however, we aimed to mitigate potential bias by including a diverse panel of 9 hand surgeons of varied sexes and ethnicities with various geographic and practice patterns (Supplemental Table 7) and modifying criteria definitions for utilization in the research context. Further investigation of the application of the domains and constructs will be necessary to elucidate appropriate measurement tools/methods for measuring specific constructs. Finally, as many domains and constructs are interrelated, additional work is needed to understand their interaction and association with outcomes.
Given the growing understanding of the association of SDOH with outcomes in various medical fields, the impact of such variables warrants further investigation in hand surgery. The validated SDOH domains and constructs serve as a foundation to evaluate and categorize their association more systematically with outcomes, thus generating knowledge that may be used to improve the understanding of drivers of health inequity and inform interventions to mitigate health care disparities.
Supplemental Material
sj-docx-1-han-10.1177_15589447251336401 – Supplemental material for National Agenda for Disparities Research in Hand Surgery: Validation of Social Determinant of Health Domains and Measurement Constructs
Supplemental material, sj-docx-1-han-10.1177_15589447251336401 for National Agenda for Disparities Research in Hand Surgery: Validation of Social Determinant of Health Domains and Measurement Constructs by Chiamaka Obilo, Robin N. Kamal and Lauren M. Shapiro in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447251336401 – Supplemental material for National Agenda for Disparities Research in Hand Surgery: Validation of Social Determinant of Health Domains and Measurement Constructs
Supplemental material, sj-docx-2-han-10.1177_15589447251336401 for National Agenda for Disparities Research in Hand Surgery: Validation of Social Determinant of Health Domains and Measurement Constructs by Chiamaka Obilo, Robin N. Kamal and Lauren M. Shapiro in HAND
Footnotes
Appendix
Please complete this form to help us understand how to best support your care needs.
Name: ________________________ Date of Birth: _______________ Date: _______________
Ethical Approval
This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and was carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act (HIPAA).
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This article does not involve the use of patient information or identifiable data.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.K. has financial involvements in Acumed and Restor3D. MR has financial involvements in Acumed, Bioventus, DJO, Field Orthopedics, and Medartis. DSR has financial involvements in Acumed, Anika/Arthrosurface, and Field Orthopedics. The remaining authors declare they have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The institution of one or more authors (LMS) has received funding from the National Institute of Health (grant no. K23AR082960; Principal Investigator) and the Orthopaedic Research and Education Foundation (Principal Investigator). This work has been aided by a Grant from the Orthopaedic Research and Education Foundation. Funding made possible by the Dr. Zachary B. and Mrs. Kathleen Friedenberg Endowment Fund. No benefits in any form have been received or will be received by the other authors related directly or indirectly to the subject of this article
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.