
Abstract
Background:
Whether sagittal and coronal plate placement influences the risk of flexor tendon complications after volar plating of distal radius fractures is debated. In this study, we tested the null hypothesis that sagittal and coronal plate position is not associated with flexor tendon irritation, rupture, or plate removal.
Methods:
We performed a retrospective review of 144 patients treated for distal radius fractures with a volar locking plate by 4 fellowship-trained hand surgeons. Patient, surgical, and radiographic factors were recorded, including measures of sagittal (Soong grade) and coronal (plate translation index) plate position and volar tilt. Outcomes assessed were flexor tendon irritation, rupture, and plate removal for any reason. We used multivariable logistic regression models to adjust for patient and surgical factors.
Results:
Of 144 patients treated with volar locking plates (mean follow-up: 18 months), 22 (15%) patients developed flexor tendon irritation, 2 patients (1%) developed flexor tendon rupture, and 18 (13%) patients underwent subsequent plate removal. In the univariable analysis, neither Soong grade nor plate translation index was associated with flexor tendon irritation, flexor tendon rupture, or plate removal. Even after adjusting for the effects of age, sex, laterality, and volar tilt, neither Soong grade nor plate translation index was associated with flexor tendon irritation or plate removal.
Conclusions:
Soong grade and plate translation index were not associated with the incidence of flexor tendon irritation, rupture, or need for plate removal. Plate placement in the coronal and sagittal planes can be determined based on the needs of the fracture pattern.
Keywords
Introduction
In the treatment of distal radius fractures, volar plate placement has received much attention due to its association with flexor tendon complications. In the original study, Soong et al 1 postulated that volar plate prominence at the watershed line was associated with a higher risk of flexor tendon rupture in a series of patients treated between 2005 and 2008. Based on their results, the authors developed a method for measuring plate prominence by referencing plate placement relative to a critical line drawn through the most volar extent of the volar rim parallel to the radial shaft, with plate placement volar and distal to this line hypothesized to be associated with an increased risk of flexor tendon rupture. 1 The reliability of the Soong grading system for determining volar plate prominence has been validated. 2 However, subsequent studies have shown mixed results on the association between Soong grade and the risk of flexor tendon rupture, which could be either from improved plate technology (eg, lower profile plates with improved anatomic fit) or from unmeasured variables (eg, plate placement in the coronal plane) in the original study.3 -6 Volar locking plate design, which varies between manufacturers, can affect plate position relative to the watershed line. 7 Such changes in design to newer volar locking plates raise the question of whether Soong grading and sagittal position remain relevant in evaluating the risk of flexor tendon irritation, rupture, and subsequent plate removal.
Furthermore, a recent study has suggested that coronal plane plate alignment is also critical in influencing the risk of flexor tendon irritation. 8 The watershed line of the distal radius extends more distally at the ulnar aspect compared with the radial aspect,9,10 which should be taken into consideration during plate placement. For example, a magnetic resonance imaging–based study has shown that distal radius plate placement in the coronal plane within the 40% to 60% central region of the distal radius within 3 mm proximal to the watershed line may place the flexor tendons at risk for irritation and rupture. 11 Thus, suboptimal coronal plate positioning may contribute to an increased risk of tenosynovitis, 8 which could predispose to tendon rupture. However, coronal plate placement is not accounted for in the Soong grading system which focuses on sagittal plane alignment only. Thus, whether coronal plate position influences the risk of flexor tendon complication also remains to be explored.
In this study, we tested the null hypothesis that in patients with distal radius fractures treated with a volar locking plate, neither sagittal nor coronal plate placement is associated with the incidence of flexor tendon irritation, rupture, or plate removal.
Methods
Data Collection
After institutional review board approval, we performed a retrospective review of our institutional databases to identify distal radius fractures treated with open reduction and internal fixation (ORIF) between August 2013 and August 2021. All procedures were performed at 2 institutions by fellowship-trained hand surgeons. Data from 4 attending surgeons were included. Inclusion criteria included patients of age ≥18 years with distal radius fractures managed with volar locking plate fixation. We excluded patients who were treated with non-volar locking plates, such as dorsal bridge plates and percutaneous Kirschner wires (K-wires). We collected patient demographic information, surgical characteristics, and radiographic parameters from postoperative radiographs. Specifically, plate positioning in the sagittal plane was measured using the Soong grade, 1 and plate positioning in the coronal plane was measured using the plate translation index. We use the plate translation index to measure plate placement in the medial-to-lateral (coronal) plane. 12 Volar tilt was also measured. To evaluate outcomes, we identified cases of documented flexor tendon irritation, flexor tendon rupture, and hardware removal for any reason. We were unable to ascertain the reason for plate removal, and plate removal was not necessarily representative of flexor tendon pathology due to the plate. These outcomes were determined via review of the clinical record. Specifically, for flexor tendinopathy, we assessed for documentation of the presence of pain or crepitation in the wrist with finger flexion and extension. This was a purely clinical diagnosis and has previously been used to define tendinopathy in a prior study. 13 Standard postoperative practice was for postoperative visits at 6 weeks, 3 months, 5 months, and 12 months, and patients were followed for a mean of 18.2 months (standard deviation [SD]: 17.2). However, compliance with this practice was not evaluated.
Radiographic Assessment
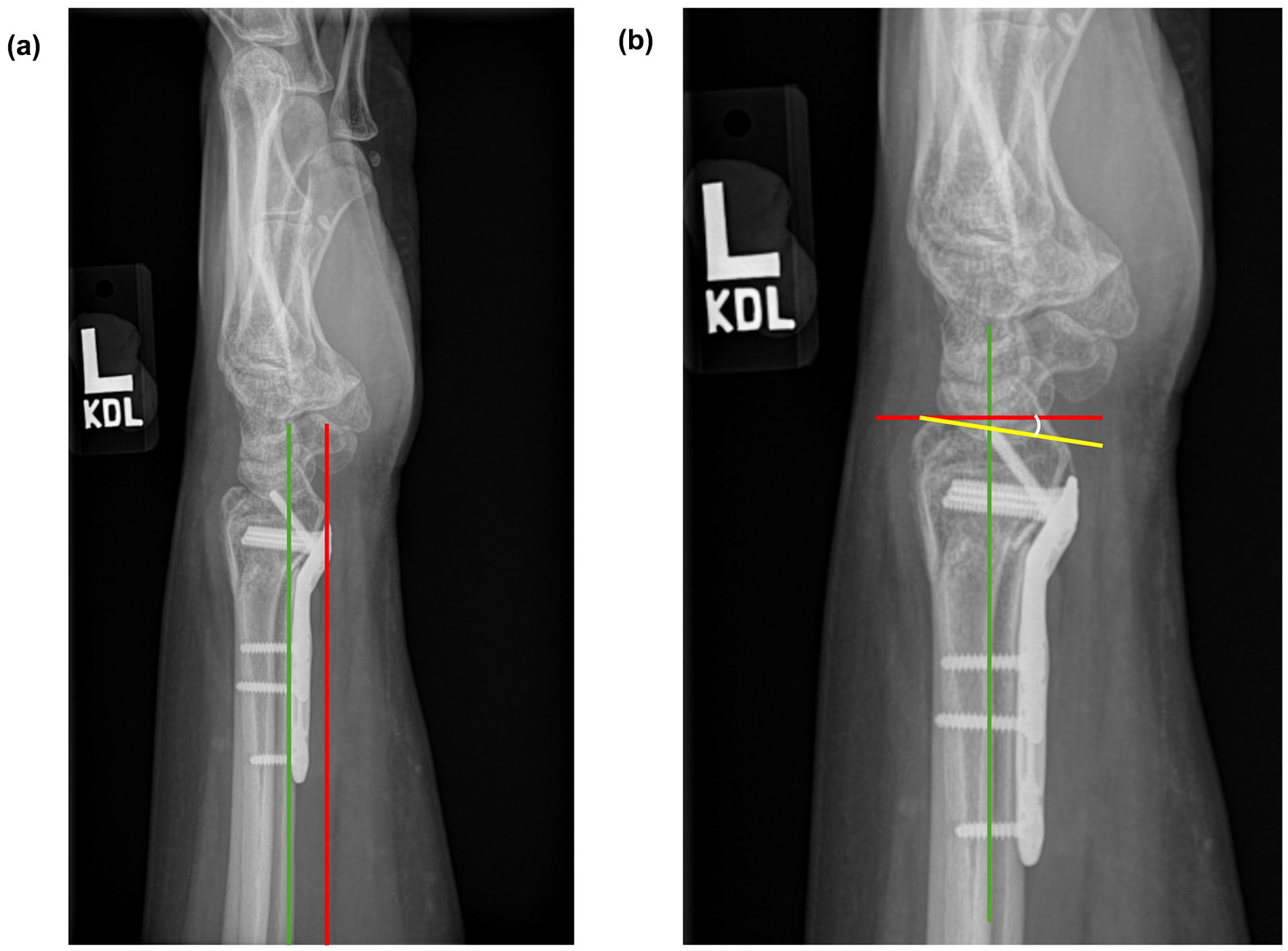
Soong grade was determined according to the method outlined by the original authors. 1 On a lateral radiograph, a line was drawn parallel to the volar cortex of the radial diaphysis. The critical line was then drawn tangential to the most volar extent of the volar rim, parallel to the radial diaphyseal line (Figure 1a). Plates that did not extend volar to the critical line were considered grade 0. Plates that extended volar to the critical line but were proximal to the volar rim were considered grade 1. Plates that extended onto or distal to the volar rim were considered grade 2.
Radiographic assessment.
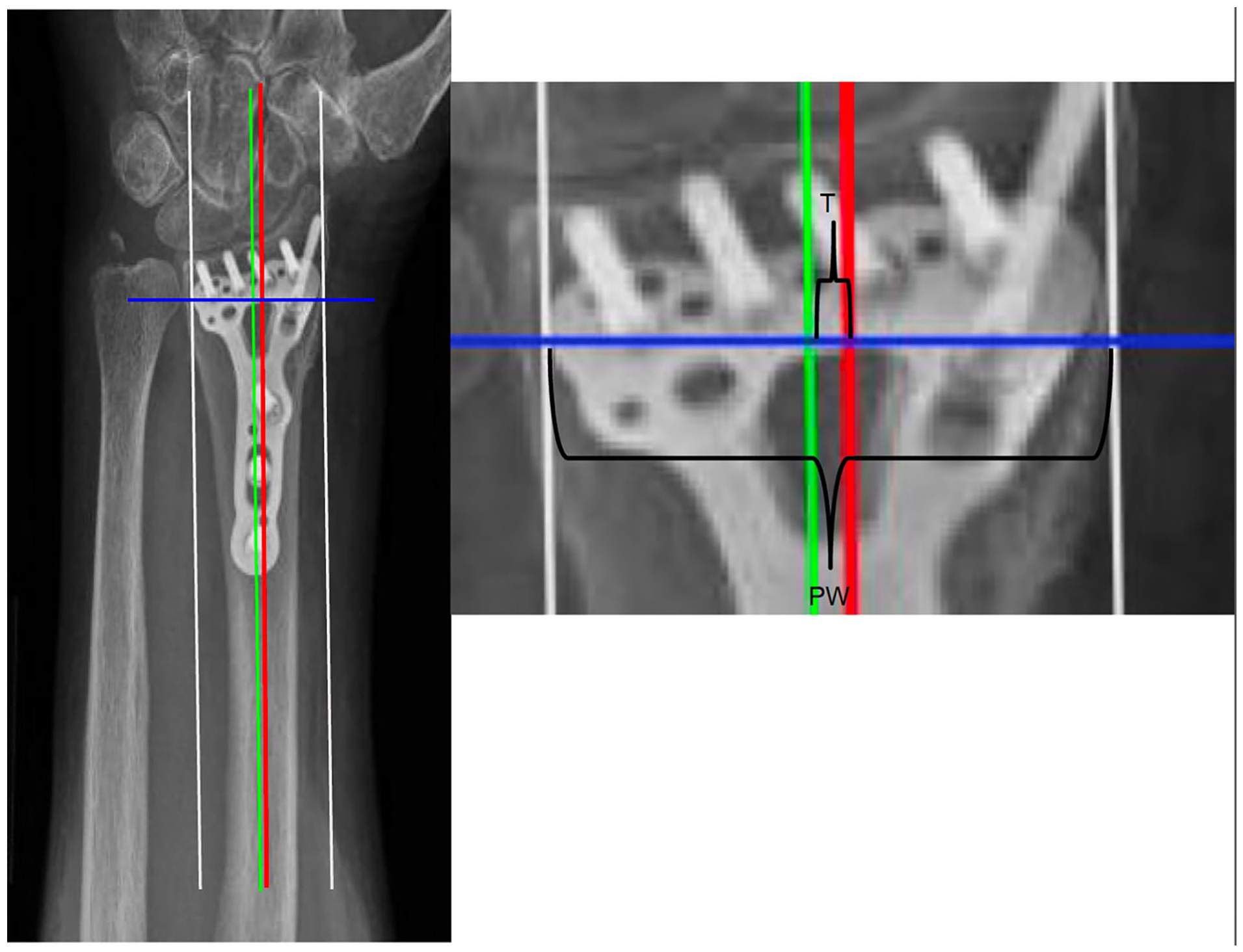
The plate translation index was determined as follows (Figure 2): on the anterior-posterior radiograph, a line was drawn parallel to the long axis of the radius. Lines were drawn tangential to the most ulnar and radial aspects of the plate, parallel with the long axis line. A bisecting line was then drawn halfway between the lines that identified the most ulnar and radial aspects of the plate. A final line was drawn perpendicular to the long axis line at the level of the proximal aspect of the sigmoid notch. Plate width was then measured from the most ulnar to radial aspects of the plate along the perpendicular line at the level of the proximal aspect of the sigmoid notch. Plate translation was measured as the distance between the long axis line and the bisecting line, with positive values denoting cases where the bisecting line was radial to the long axis line and negative values denoting cases where the bisecting line was ulnar to the long axis line. The plate translation index was then calculated as plate translation divided by plate width. This standardized measure has previously been used to characterize coronal plate position, 12 which is of interest due to data showing that central plate placement in the coronal plane within 3 mm proximal to the watershed line may increase the risk of flexor tendon irritation. 11
Determination of plate translation index.
Volar tilt was assessed on a lateral radiograph (Figure 1b). A line was drawn along the long axis of the radius. Another line was drawn perpendicular to the first line, at the level of the dorsal rim. A third line was drawn between the dorsal and volar rims of the distal radius. The angle between the second and third lines was measured as the volar tilt. Positive values correspond to volar tilt, whereas negative values correspond to dorsal tilt.
All radiographs were rated by 2 of the authors, and disagreements were resolved by a direct meeting and discussion with the senior author.
Statistical Analysis
Continuous variables were compared using independent t-tests. Categorical variables were compared using χ2 tests. We constructed multivariable logistic regression models to evaluate the association between the Soong grade or plate translation index and the incidence of flexor tendon irritation or plate removal, while adjusting for patient age, sex, laterality of fracture, and volar tilt. Due to the low incidence of flexor tendon rupture (n = 2), we were unable to create a multivariable model that accurately assesses associations with that outcome.
Results
We included 144 patients treated for distal radius fractures with a volar locking plate with an average follow-up of 18.2 months (SD: 17.2). Cohort demographics are shown in Table 1. Most patients (70%) had a Soong grade of 1 after distal radius ORIF (Table 1). Plate translation index ranged from −0.63 to 0.31 with a mean of −0.03 (Table 1). Twenty-two (15%) patients developed flexor tendon irritation and 2 patients (1%) developed flexor tendon rupture.
Overall Cohort Characteristics.
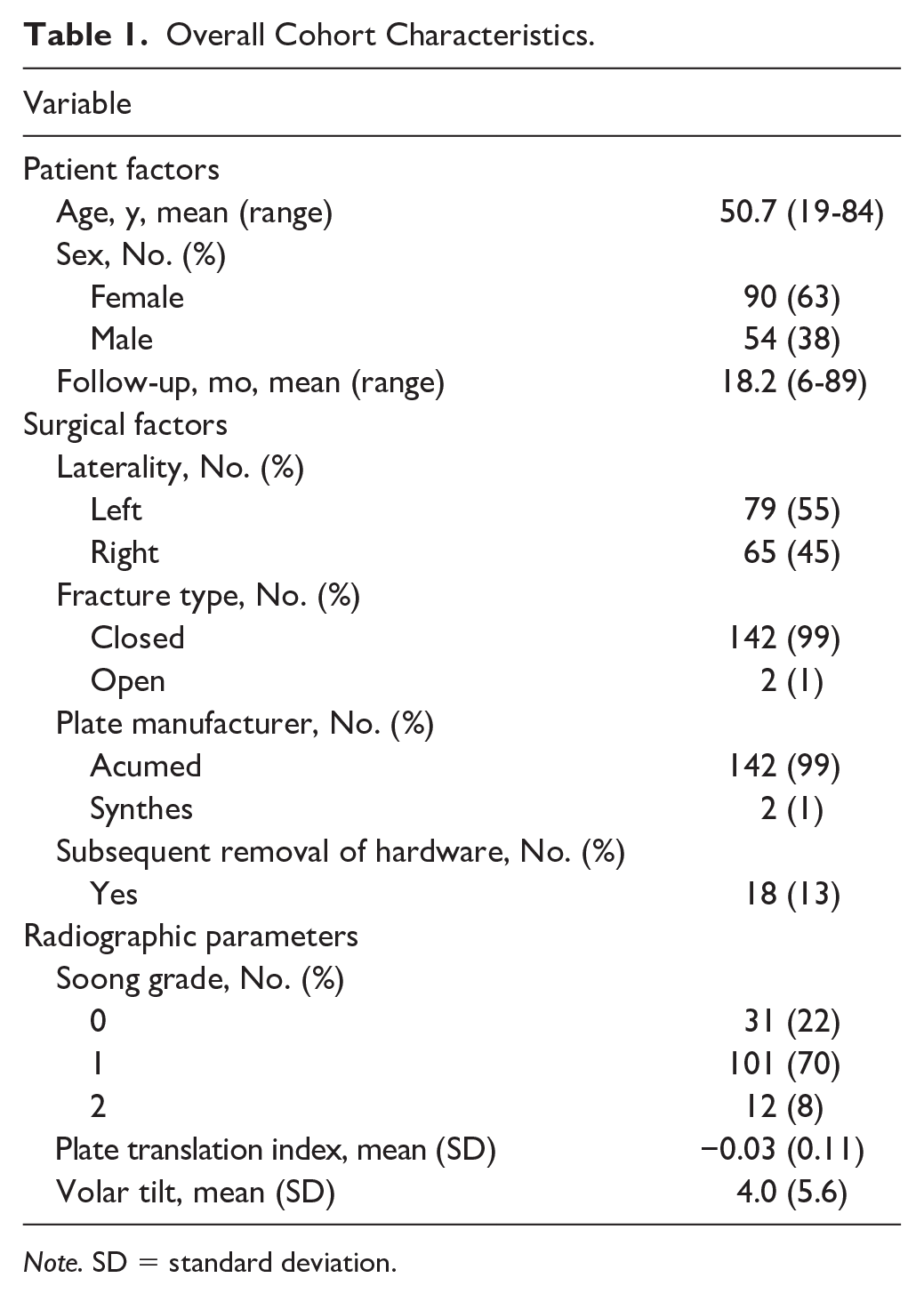
Note. SD = standard deviation.
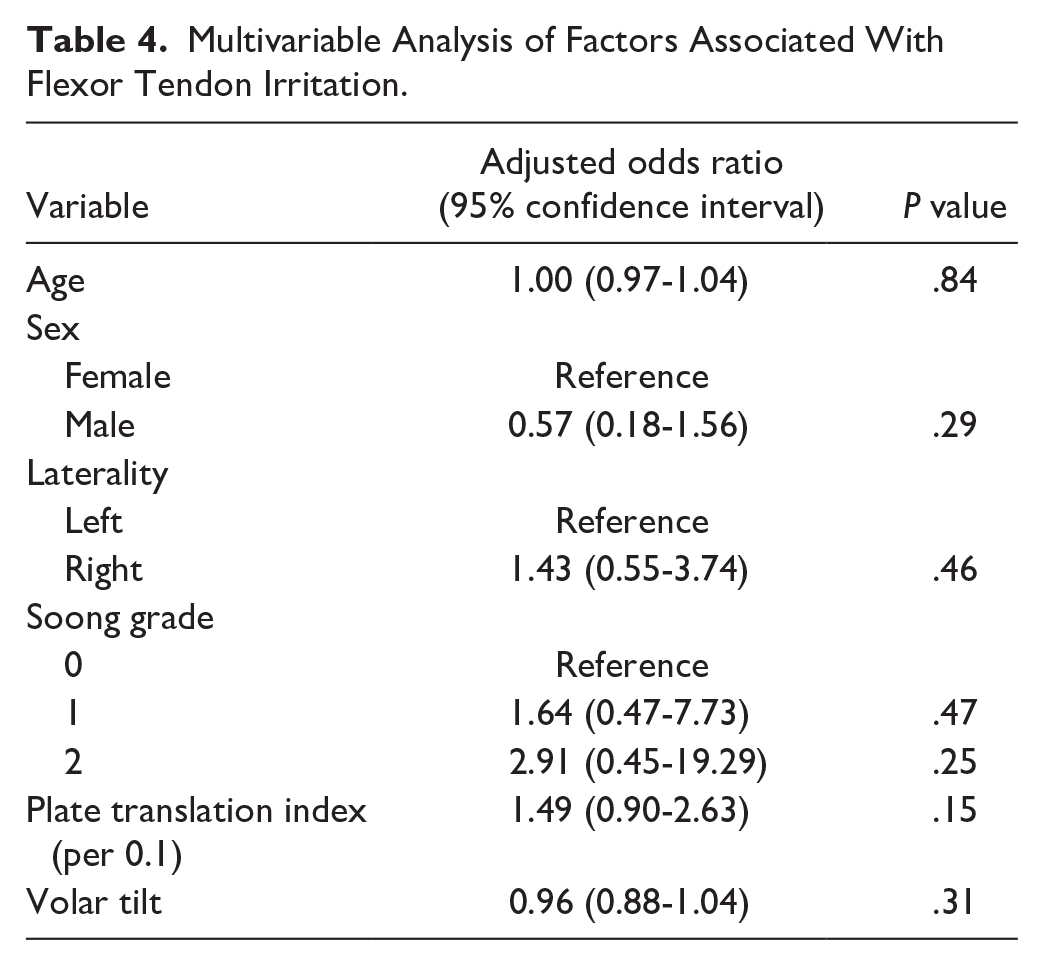
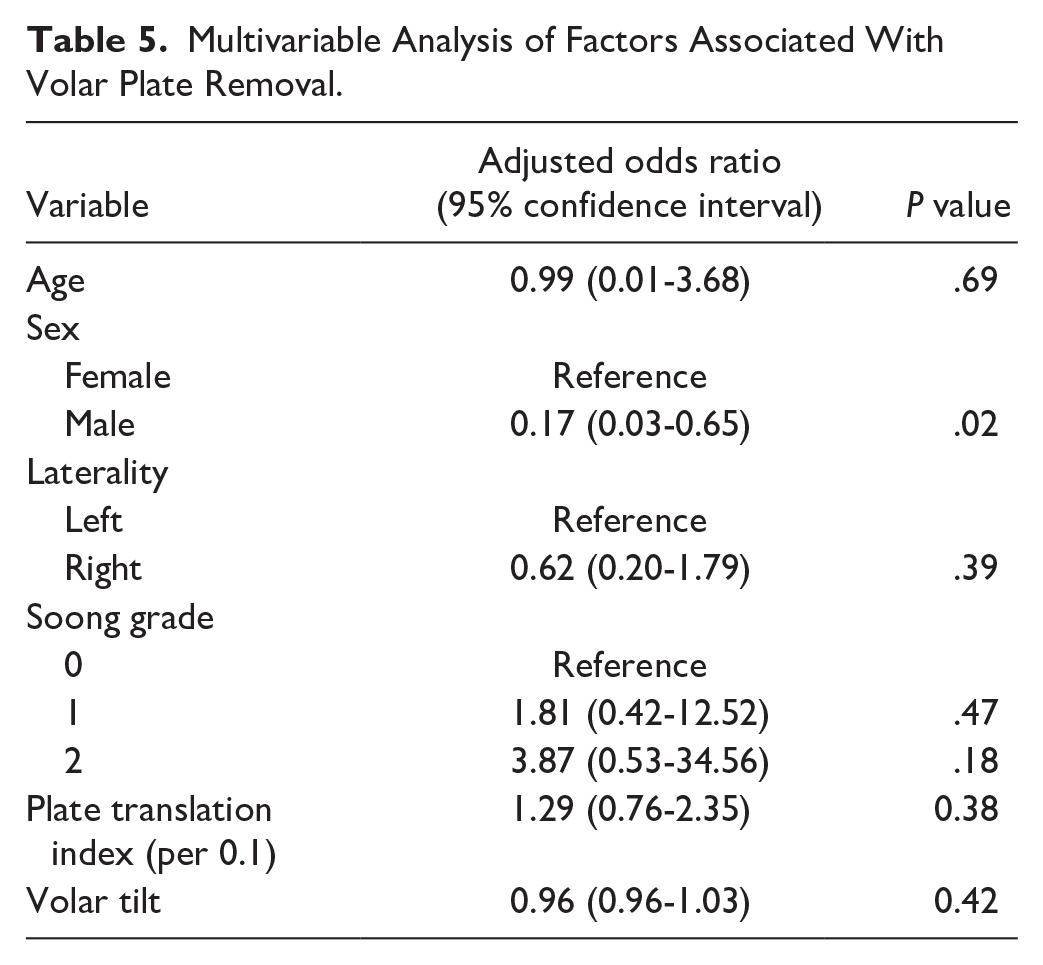
When patients who developed flexor tendon irritation were compared with those who did not, there was no difference in patient (age, sex, laterality) or surgical (volar tilt, plate translation index, Soong grade) factors (Table 2). When patients who developed flexor tendon rupture were compared with those who did not, there was no difference in patient or surgical factors, including Soong grade and plate translation index (Supplemental Table 1). When patients who underwent plate removal were compared with those who did not, there was no difference in patient or surgical factors other than sex distribution, with a greater proportion of females undergoing plate removal (Table 3). After adjusting for the effects of age, sex, laterality, volar tilt, and plate translation index, neither Soong grade nor plate translation index was associated with flexor tendon irritation or plate removal (Tables 4 and 5).
Comparison of Patients With and Without Flexor Tendon Irritation.

Note. SD = standard deviation.
Comparison of Patients With and Without Plate Removal.
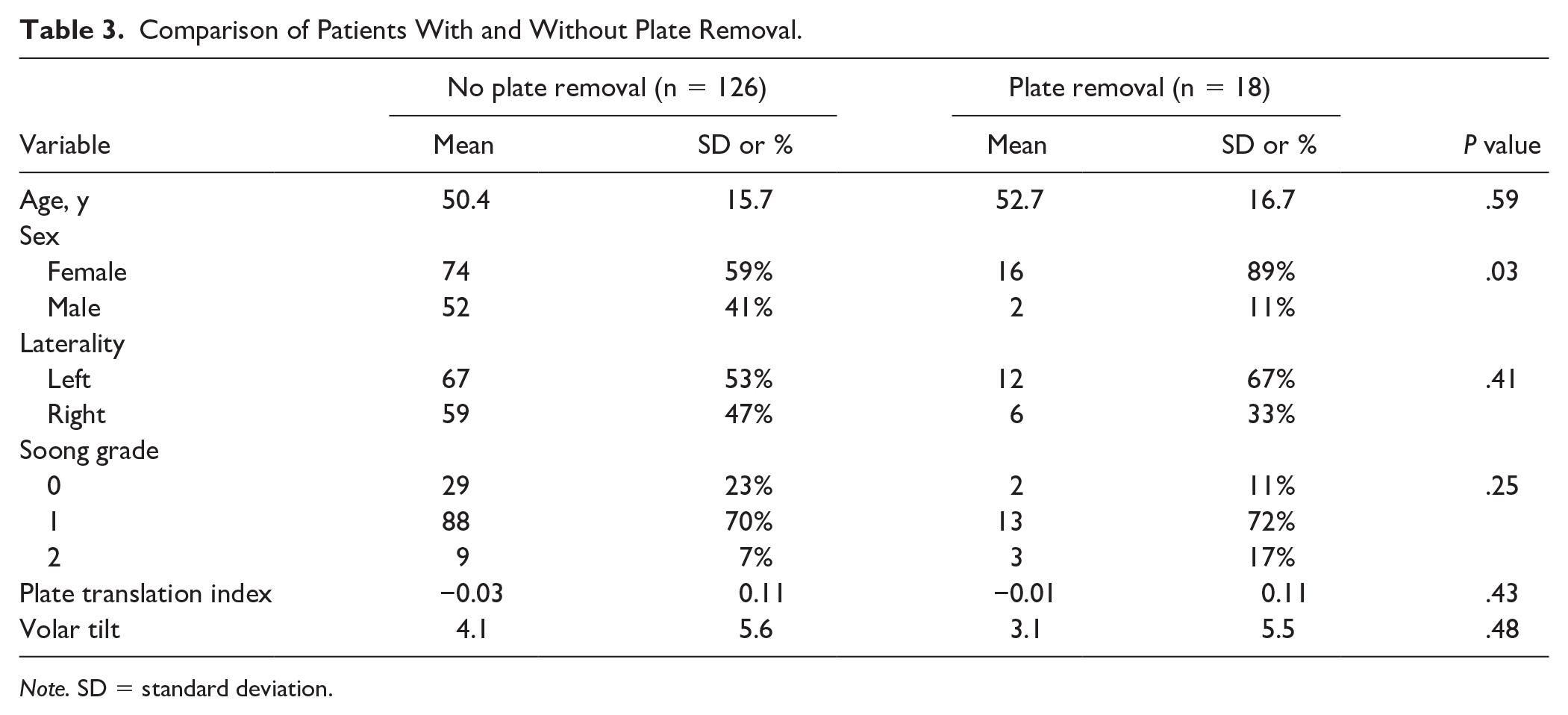
Note. SD = standard deviation.
Multivariable Analysis of Factors Associated With Flexor Tendon Irritation.
Multivariable Analysis of Factors Associated With Volar Plate Removal.
Discussion
In this study, we found no association between Soong grade or plate translation index and flexor tendon irritation or rupture in patients undergoing distal radius ORIF. While a higher Soong grade has been suggested to be associated with a higher risk of flexor tendon rupture and need for volar plate removal, this association was not observed in our cohort, which could be related to advancements in volar locking plate design or unmeasured variables in the suggested model. Moreover, we showed that coronal plate position, as measured by the plate translation index, was also not influential in determining the risk of flexor tendon irritation or rupture, suggesting that plate placement can be used based on the needs of the fracture pattern in both the sagittal and coronal planes.
The Soong grading system was based on a series of 165 patients with distal radius fractures treated with a volar locking plate between 2005 and 2008, in which the authors showed that plate prominence at the watershed line was associated with the risk of flexor tendon rupture. 1 This grading system has guided volar plate placement and further studies have reinforced this proposed association with flexor tendon complications and the need for subsequent plate removal.5,6,14,15 Those findings stimulated further work that has characterized the clinical consequences of plate design and plate placement relative to the watershed line.9,16 However, advancements in volar locking plate design since the original Soong et al. study have resulted in the development of lower profile plates with more optimal anatomic fit at the distal radius surface (eg, ulnar side–based plating), 17 which challenges the relevance of Soong grading in volar plate placement. Indeed, later studies have failed to find an association between Soong grade and the risk of flexor tendon complications.3,4 For example, in a large retrospective study, DeGeorge et al 4 found that while Soong grade was associated with the adequacy of fracture reduction, it was not an independent predictor of flexor tendon rupture or tendinopathy. Similarly, no flexor tendon ruptures were found in another large series of patients treated with volar locking plates between 2012 and 2015. 3 Our data provide additional evidence to suggest that with modern plate designs, Soong grade may not be an independent predictor of flexor tendon irritation, rupture, or need for plate removal.
Anatomic studies conducted since the development of the Soong grading system have revealed nuanced features of distal radius anatomy and its relationship with volar plate placement that have driven redesign of key plate features. 18 The watershed line has been identified as a critical reference point for plate placement, corresponding to the distal aspect of the pronator fossa in the lateral aspect of the volar distal radius and a location between the distal aspect of the pronator fossa and a bony line distal to that in the medial aspect of the volar distal radius. 9 At a point 3 mm proximal to the watershed line, the flexor pollicis longus and flexor digitorum profundus to the index finger tendons are, on average, 2 to 3 mm anterior to the volar cortex of the radius, leading to direct contact with a volar plate if plate thickness exceeds 2 mm. 11 Volar plate placement distal to the distal radial watershed line has been shown to cause increased contact pressure between the distal edge of the plate and the flexor pollicis longus tendon, leading to a predisposition for rupture.19,20 Even with optimal volar plate placement, plate design substantially influences contact area and prominence, 16 with newer plates having lower profiles and exhibiting improved anatomic contouring. 21 Therefore, modern plate designs that are thinner and offer better anatomic fit with the distal radius in which the ulnar column sits more distal than the radial column (ie, ulnar side–based plating) might account for the lack of association between Soong grade and flexor tendon complications or need for plate removal in our study.
Furthermore, coronal plate placement has recently been suggested as a determinant in the risk of flexor tendon complications, 8 which is consistent with an imaging-based study showing that plate prominence in the coronal plane, specifically outside of the 40% to 60% volar central area within 3 mm of the watershed line, may lead to flexor tendon irritation. 11 In contrast, another study found no association between coronal plate positioning, measured as translation in the coronal plane, and the odds of flexor tendon rupture. 12 Our data provide additional credence to the latter notion that coronal plate placement is not associated with flexor tendon irritation or rupture, suggesting that other, unmeasured risk factors for rupture remain to be identified.
Several key limitations to our study exist. Due to the relative infrequency of flexor tendon complications, we may lack power to detect subtle differences in complication rates. Thus, large, multicenter studies are needed to further evaluate whether sagittal or coronal plate positioning is associated with flexor tendon complications with the use of newer generation volar locking plates. While we only collected data from 2013 onward, we were unable to ascertain the exact implants used in each case, which was based on surgeon preference. The majority of implants used in this study were from one manufacturer, which may limit generalizability. However, an earlier generation of this plate designed by the same manufacturer, which was prominent at the watershed line, was featured in the original Soong et al 1 study. Thus, in some ways, bias toward plates designed by this manufacturer might have been expected to exaggerate any potential association between tendon irritation/rupture and distal plating. We acknowledge there can be variability in anatomic fit even between implants within similar generations of design. 21 We were also unable to characterize indications for plate removal, although historically the majority of these are performed due to pain or stiffness. 15 Although flexor tendinopathy could develop beyond the follow-up period in this study (average of 18 months), a prior study showed that the average time from volar plate fixation to flexor tendinopathy was 11 months. 13
In conclusion, this study did not find an association between Soong grade or plate translation index and the incidence of flexor tendon irritation, rupture, or need for plate removal. Our results might be attributable to improved plate technology and design, leading to lower plate profiles and improved anatomic contouring. Our results suggest that distal plate placement can be used based on the needs of the fracture pattern in both the sagittal and coronal planes.
Supplemental Material
sj-docx-1-han-10.1177_15589447251338533 – Supplemental material for Sagittal and Coronal Plate Position Is Not Associated With Flexor Tendon Irritation, Rupture, or Need for Plate Removal After Volar Locking Plate Fixation of Distal Radius Fractures
Supplemental material, sj-docx-1-han-10.1177_15589447251338533 for Sagittal and Coronal Plate Position Is Not Associated With Flexor Tendon Irritation, Rupture, or Need for Plate Removal After Volar Locking Plate Fixation of Distal Radius Fractures by Thompson Zhuang, Kaveh Mansuripur, Lauren M. Shapiro, Suhail K. Mithani, David S. Ruch, Marc J. Richard and Robin N. Kamal in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Animal and Human Rights
This article does not contain any studies with human or animal subjects as defined by 45 CFR 46.
Statement of Informed Consent
This study was a retrospective chart review and therefore informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The institution of one or more authors has received funding from the National Institutes of Health (#K23AR082960; PI: LMS) and the Orthopaedic Research and Education Foundation (PI: LMS). Funding made possible by the Dr. Zachary B. and Mrs. Kathleen Friedenberg Endowment Fund.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.