
Abstract
Background:
Lateral antebrachial cutaneous nerve neuropathy (LABCN) is a known complication following distal biceps tendon repair; however, potential risk factors leading to this are not well described. This retrospective study of distal biceps repairs seeks to determine associations between patient demographics, surgical technique, and injury characteristics associated with postoperative LABCN.
Methods:
A retrospective chart review was performed on 275 patients with partial- or full-thickness biceps tendon ruptures who underwent operative repair. Patient characteristics were recorded including utilization of tobacco, alcohol, age, and body mass index, along with surgical factors including tourniquet time, approach, prior shoulder surgery, and tendon repair techniques. Lateral antebrachial cutaneous nerve neuropathy was identified by description of “numbness, tingling, burning, or decreased sensation” at postoperative visits. Chi-square and t tests were used to analyze differences in LABCN development rate for the listed variables.
Results:
Sixty-three of 275 (22.9%) patients were identified as having some form of LABCN postoperatively. Age, body mass index, and tourniquet time were not correlated with LABCN (P > .05). The 2-incision technique and the use of corkscrew anchor fixation correlated with lower LABCN rates (P < .05). Chronic biceps rupture, partial thickness tear, and history of prior ipsilateral shoulder surgery correlated with higher LABCN rates (P > .05).
Conclusions:
Multiple factors affect the risk of LABCN after distal biceps repair. Patient-related factors do not appear to be associated with increased risk, except in cases where patients have a history of shoulder surgery or chronic distal biceps rupture. Surgical factors such as approach and method of tendon fixation demonstrate differences in the rate of postoperative LABCN.
Keywords
Introduction
Lateral antebrachial cutaneous neuropathy (LABCN) is a peripheral nerve pathology of the upper extremity, most frequently arising as a postoperative complication of distal biceps repair.1-3 Symptoms include numbness, paresthesia, pain, and allodynia along the volar aspect of the lateral forearm. 4 Current management strategies range from rest and pain medications to surgical decompression. 4 Resolution of symptoms typically occurs within weeks to months after the inciting incident; however, some patients continue to suffer long-term symptoms despite appropriate management.
Currently, the majority of LABCN literature exists as case reports and case series documenting its presenting symptoms and rate of occurrence, ranging from 6% to 32% depending on the study and operative technique. 5 Retrospective cohort studies have previously focused on either surgical management 3 or strategies to achieve symptom resolution. 4 However, patient demographics and other perioperative factors such as tourniquet time and fixation method have not yet been investigated with regards to LABCN development, duration, or resolution and could provide greater insight into risk factors for this pathology. The purpose of this study is to identify demographic and operative factors that impact the incidence of LABCN after distal biceps repair. We further sought to better characterize the frequency of symptom resolution and duration of symptoms following surgery.
Methods
Demographics
Following institutional review board approval, our institutional database was queried utilizing CPT codes 24342 and 24340 to identify patients undergoing distal biceps repair between January 01, 2018, and December 31, 2023. Patients were excluded if they did not undergo distal biceps repair, were <18 years of age, suffered distal biceps injury secondary to laceration, had a history of cervical radiculopathy, or did not have postoperative follow-up information available. Patients that had documented preoperative symptoms consistent with LABCN were also excluded.
Patient information, including age, gender, body mass index (BMI), tobacco and alcohol use, and prior upper-extremity surgery, was recorded from the electronic medical record. History related to the injury including rupture chronicity, tear thickness, and preoperative symptoms of pain or paresthesia were additionally recorded. Surgical approach, method of fixation, tourniquet time, and need for unplanned additional intraoperative incisions were extracted from the operative note. Finally, postoperative information including the need for reoperation, presence of symptoms consistent with LABCN, and duration of these symptoms was recorded from postoperative follow-up appointments. LABCN was identified by symptoms of numbness, tingling, burning, or decreased sensation in the distribution of the lateral antebrachial cutaneous nerve and noted in postoperative visit notes. Duration of LABCN was defined as the first postoperative office note describing LABCN symptoms to the office note describing resolution of LABCN symptoms.
Statistical Analysis
We performed 2-tailed independent t tests to assess mean differences of continuous data from patient characteristics between those with and those without LABCN, with Welch’s correction factor for unequal variance applied. Chi-squared tests were used to assess significant differences in categorical variables. Significance was set at an alpha value of 0.05.
Results
A total of 484 patients undergoing distal biceps repair were initially identified. Following exclusion, a total of 275 were included in our final cohort (Figure 1). Patient characteristics can be found in Table 1.
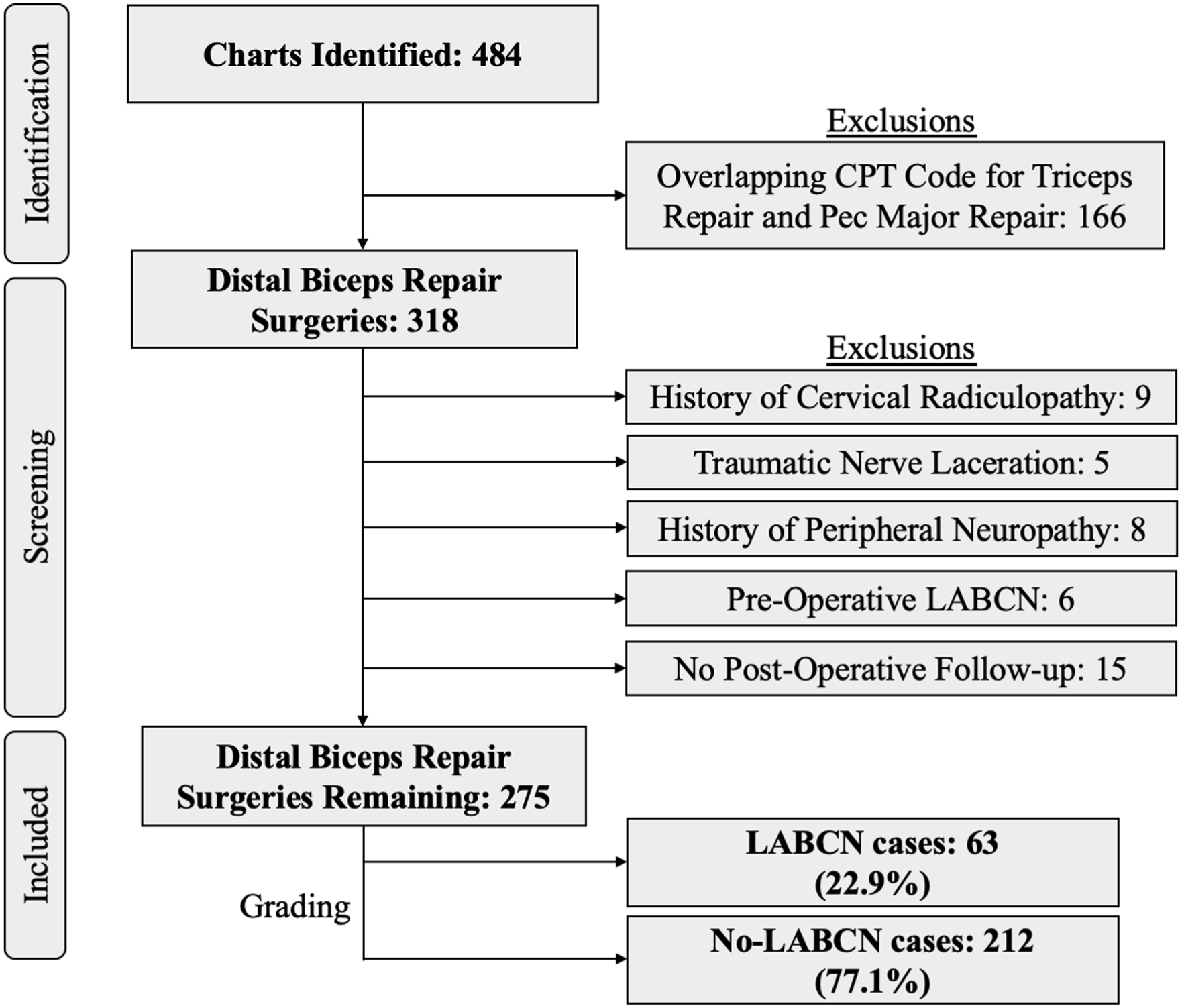
Identification of patients experiencing LABCN symptoms after distal biceps reconstruction.
Preoperative Patient and Injury Characteristics.
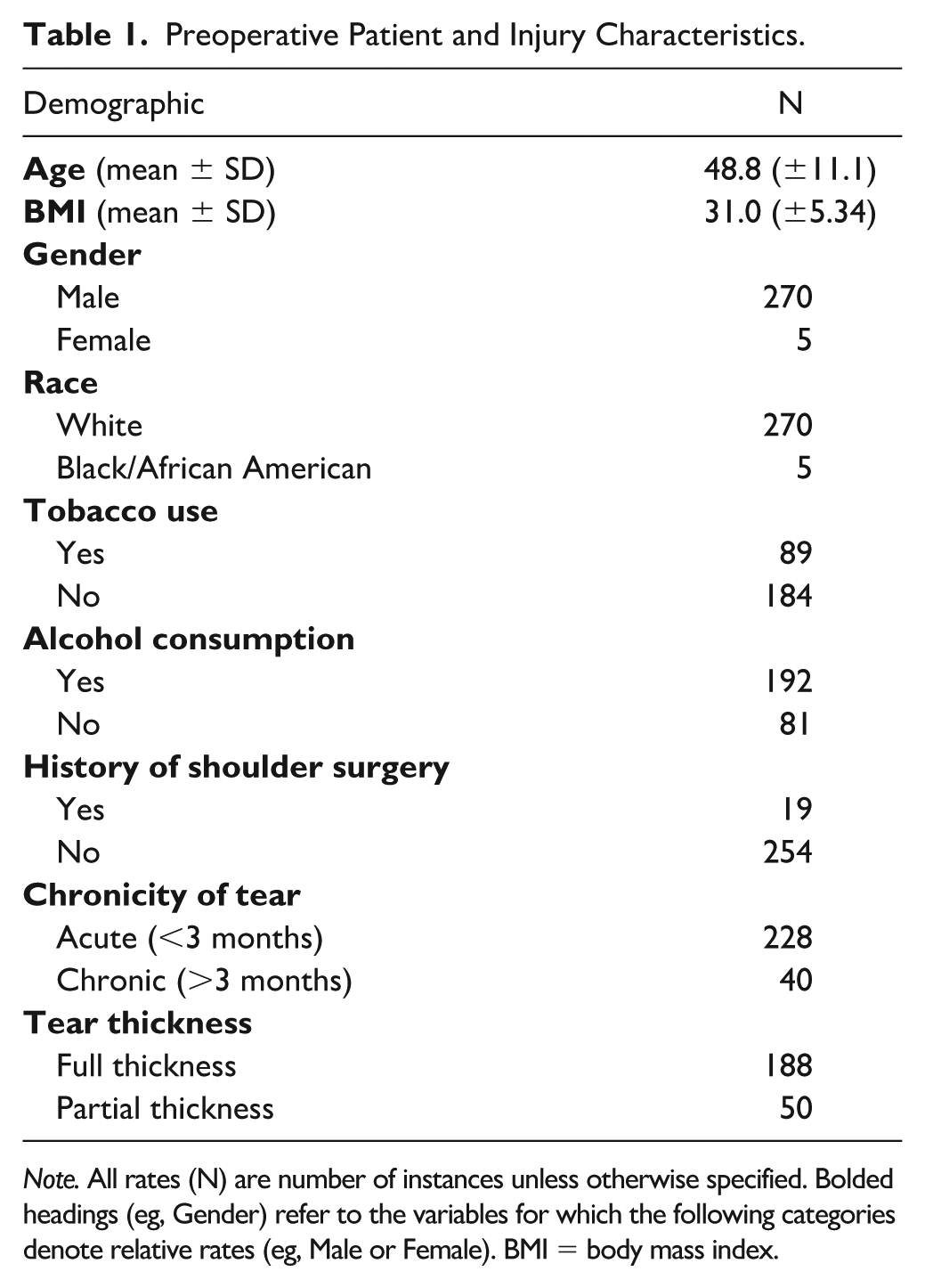
Note. All rates (N) are number of instances unless otherwise specified. Bolded headings (eg, Gender) refer to the variables for which the following categories denote relative rates (eg, Male or Female). BMI = body mass index.
Sixty-three (22.9%) patients were identified to have postoperative LABCN in our cohort. Eighteen (28.6%) cases resolved within 3 months, while 45 (71.4%) cases remained unresolved after 3 months.
Patient Characteristics
Patient-specific characteristics such as age, BMI, smoking history, and alcohol consumption did not vary significantly between the groups with and without LABCN after distal biceps repair (Figures 2a-2c).
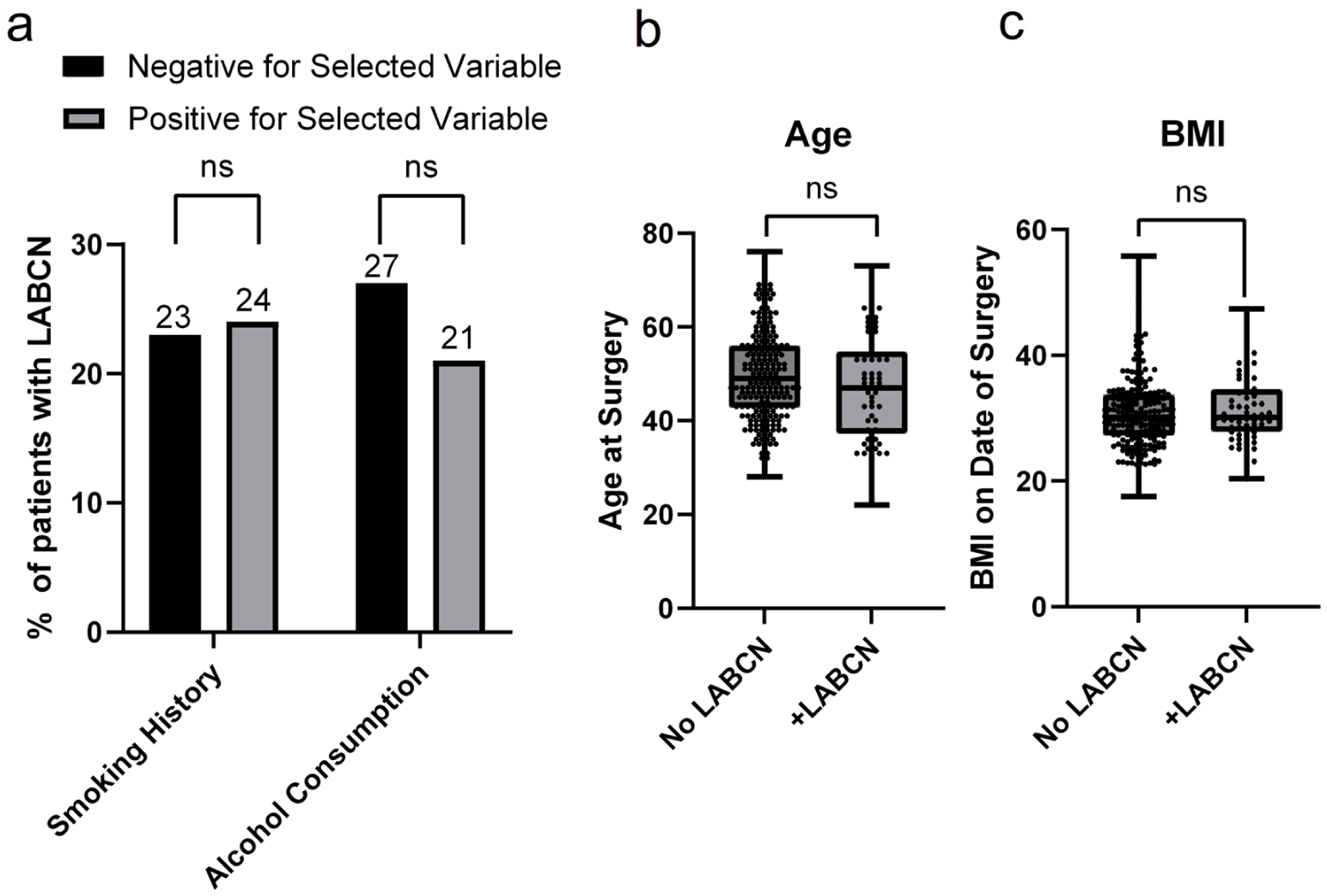
Patient-level demographic risk factors of tobacco and alcohol use (a), age (b), and BMI (c) and the development of postoperative LABCN. Ns denotes no significant difference.
Rupture chronicity was categorized as acute if it appears less than 6 weeks from time of injury or chronic if over 6 weeks between the initial injury and surgery. 6 A significantly higher incidence of LABCN was found in patients with chronic distal biceps rupture (40%) than in those with acute biceps tears (21%) (P = .008, Figure 3). Patients with a history of upper-extremity surgery, either ipsilateral shoulder arthroplasty or rotator cuff surgery prior to the distal biceps reconstruction, had a significantly greater incidence of LABCN (47%) relative to patients with no history of upper-extremity surgery (21%) (P = .009, Figure 3). Furthermore, incidence rates of LABCN were significantly different between patients with complete rupture of the biceps tendon (22%) or a partial tear (42%) (P = .004, Figure 3).
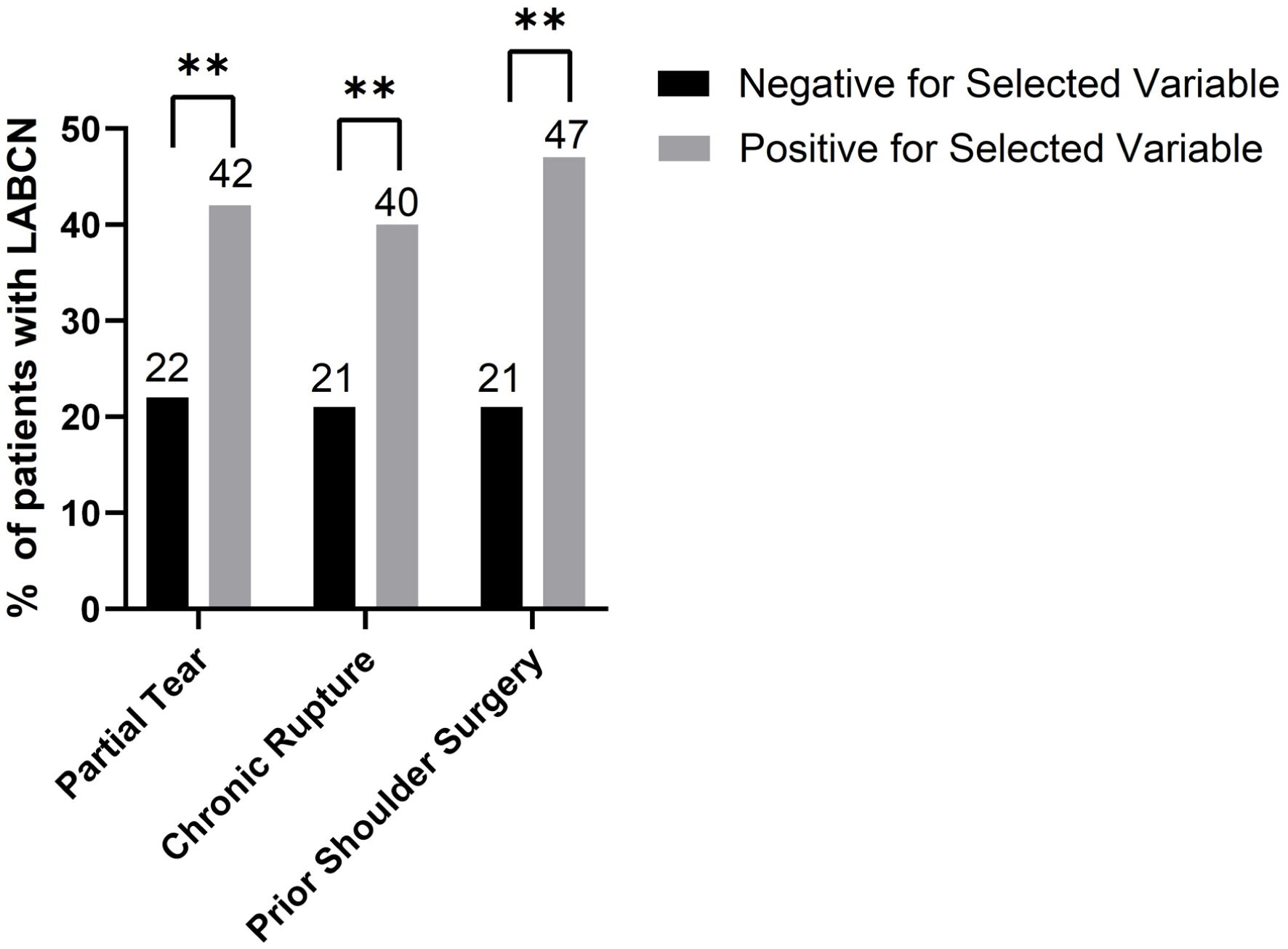
Preoperative injury characteristics for the development of LABCN after distal biceps reconstruction.
Perioperative Demographics
Operative characteristics can be found in Table 2. Surgical approach, categorized as either dual or single incision, did display a difference in the incidence of LABCN with a greater incidence in single incision (27%) relative to dual incision (8%) (P = .039, Figure 4a). The method of tendon repair, either with an Endobutton or corkscrew anchor, also demonstrated significant differences in the incidence of postoperative LABCN (P = .019). The use of corkscrew anchors was associated with a reduced rate of postoperative LABCN (4%) relative to fixation with an Endobutton (24%) (Figure 4a).
Intraoperative Characteristics.
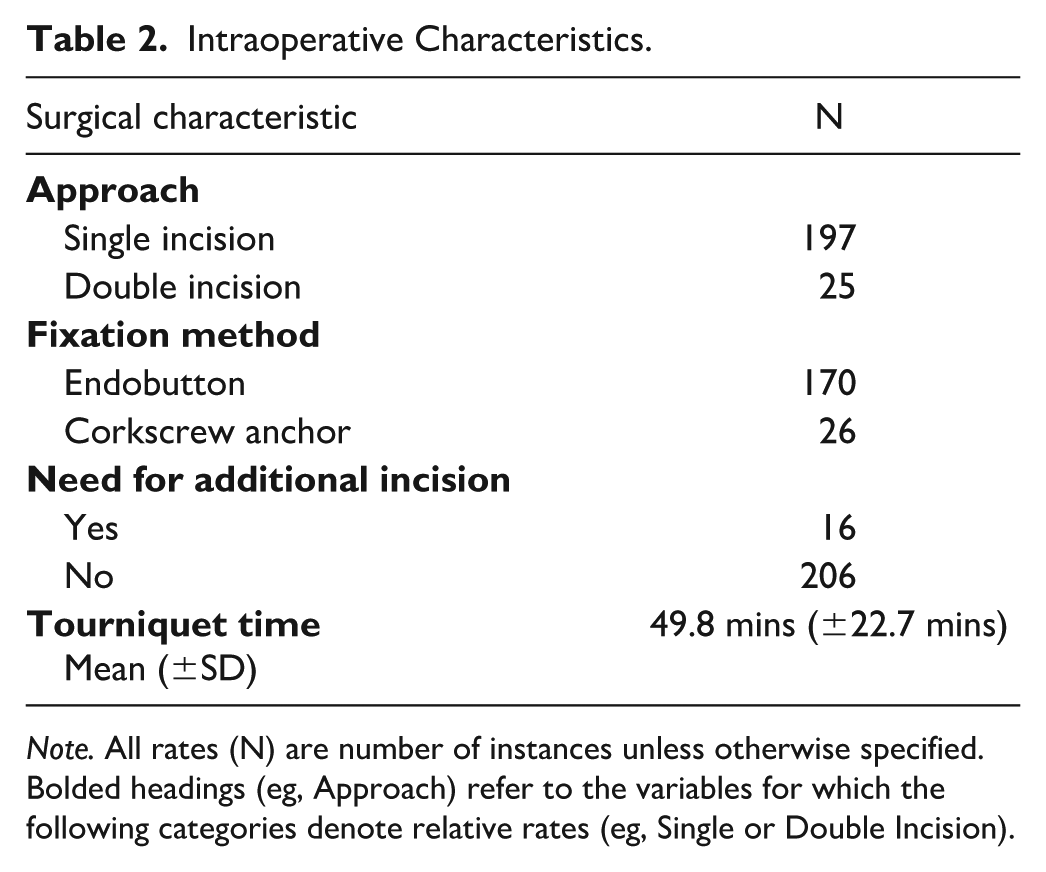
Note. All rates (N) are number of instances unless otherwise specified. Bolded headings (eg, Approach) refer to the variables for which the following categories denote relative rates (eg, Single or Double Incision).
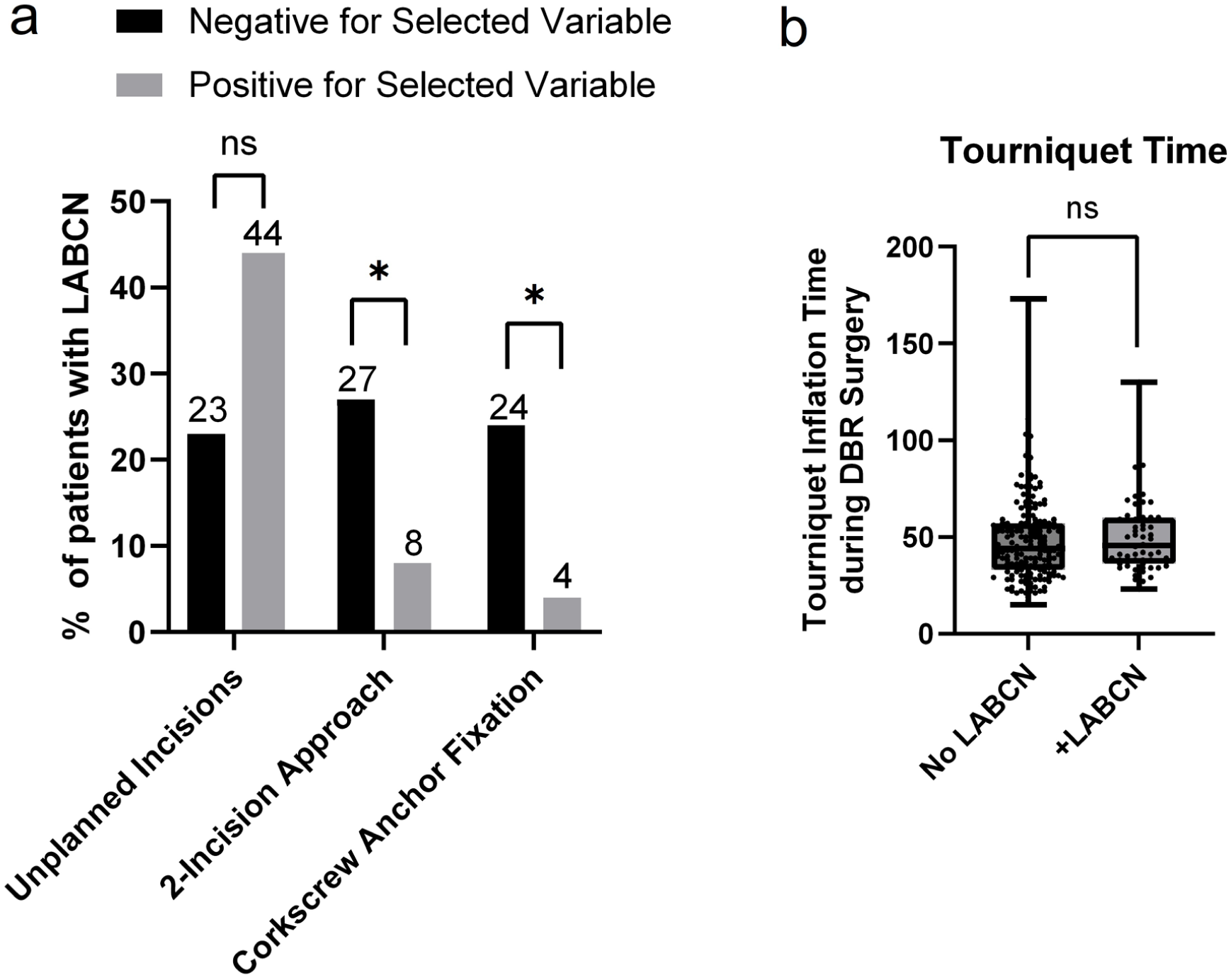
Perioperative risk factors of unplanned incisions, surgical approach, and fixation method (a), tourniquet time (b), and the development of postoperative LABCN.
Tourniquet duration was not a statistically significant factor in the rate of postoperative LABCN (Figure 4b). The incidence of unplanned incisions, identified as operative notes detailing additional incisions that were not planned prior to the operation and made due to excessive scar tissue or difficulty locating the distal end of the ruptured tendon, did not affect the rate of LABCN occurrence (Figure 4a).
Discussion
The overall rate of LABCN identified by our study was 22.9%. While this is consistent with previous literature, 5 our findings may be influenced by the exclusion of patients who did not return for follow-up appointments. We identified several preoperative patient characteristics that were risk factors for the development of LABCN. Prior shoulder surgery, chronic biceps rupture, and partial thickness tears all increased the likelihood of LABCN development, aligning with the proposed mechanism of LABCN hypersensitivity due to local edema and fibrosis. 6 Scar tissue, fibrosis, or a history of trauma likely obliterates the typical anatomical planes used to safely identify the nerve and increases risk of injury. Regional inflammation secondary to chronic or partial rupture in proximity to the nerve may also contribute to a sensitized nerve that is more susceptible to injury with surgical manipulation. Unlike these injury characteristics, patient demographics such as age, BMI, tobacco use, and alcohol consumption did not show any effect on the incidence of LABCN.
In addition to preoperative demographics, our results demonstrate that perioperative factors influence the incidence of LABCN. In accordance with existing literature, the rate of LABCN was lesser in the two-incision approach cohort relative to those who had a single-incision approach.7-10 Regarding fixation methods, while efficacy in terms of fixation strength and reoperation rates is similar between different fixation methods, 5 this dataset demonstrated that the use of corkscrew anchors resulted in a reduced rate of LABCN relative to Endobutton techniques. The significance of these findings is unclear, but it may reflect subtle differences in surgical technique attributable to the surgeons performing the operation, perhaps secondary to the amount of soft-tissue retraction or technique for operative dissection. While incision and fixation techniques had an impact on the incidence of LABCN, tourniquet time did not have a significant effect on the development of LABCN, nor did the presence of additional unplanned incisions.
Beyond risk factors for the development of LABCN after distal biceps repair, our study sought to better report the duration of postoperative LABCN. Previous literature has focused primarily on the existence of LABCN as a binary variable following surgery, with limited discussion of persistent LABCN symptoms beyond its identification.11-13 A majority of patients (71.4%) had symptoms lasting for longer than 3 months, consistent with a higher-grade injury and increasing the need for possible decompression in the future.6,14 In addition to postoperative duration, we identified 6 cases of preoperative LABCN symptoms in patients with no prior neuropathic symptoms. These are notable given that they demonstrate a potential predisposition for the LABC nerve to be irritated from the biceps rupture itself. Further investigation is needed to evaluate the incidence of preoperative LABCN symptoms after distal biceps rupture, as well as in patients that may have suffered traumatic lacerations due to nerve-tendon proximity. 15 Future studies should also expand on long-term clinical outcomes, incorporating other risk factors not evaluated here including pre-existing neuropathic disorders such as diabetes and patients with cervical radiculopathy.
The primary limitation of both of our study and of current literature is the lack of uniformity in reporting guidelines for postoperative LABCN. Our study relies heavily on the documentation of providers during postoperative and follow-up appointments. The threshold for reporting neuropathic symptoms following surgery may vary between providers, a factor we sought to address by including multiple provider evaluations and all postoperative notes for possible mention of these findings. However, as a retrospective study with each participant self-reporting their neuropathic symptoms, recall bias remains a limitation; for example, some patients who had milder cases or had differing understanding of the descriptions of LABCN may not have reported. Conversely, pain exacerbated by difficult musculotendinous recovery or coexisting psychosocial challenges may have been attributed to neuropathic LABC pain. This variance in reporting persists as a challenge for all retrospective analyses, regardless of study power. Moreover, even with a sample size of 275, the relative rarity of certain operative events limits the predictive nature of specific trends like those found with unplanned intraoperative incisions. Larger-scale investigation is warranted to clarify this relationship, along with other perioperative factors such as duration of operative retraction and location of retraction on postoperative LABCN incidence.
Conclusions
Preinjury patient demographics did not impact the incidence of postoperative LABCN following distal biceps repair. Injury characteristics of chronicity, tear thickness, and prior upper-extremity surgery had a significant impact on rates of LABCN following surgery. Intraoperative parameters of surgical approach and tendon fixation technique also affect the development of LABCN and suggest a dual-incision approach and the use of corkscrew anchors as potential protective measures. Patient counseling prior to surgical intervention should include discussions of patient’s injury characteristics to appropriately prepare for the possibility of postoperative LABCN. Ultimately, surgeons should use this work to evaluate relative risk factors in the process of choosing their approach and method of fixation to minimize the potential for LABCN.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This study complies with appropriate ethical standards for research as defined in the Declaration of Helsinki.
Statement of Informed Consent
This is a minimal risk retrospective study, therefore informed consent was waived by the institutional review board.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.