
Abstract
Background:
Cold therapy devices (CTDs) have been shown to provide analgesia, reduce swelling, and improve outcomes following orthopedic procedures. However, comparative data on postoperative narcotic use and pain control between CTDs and traditional ice packs remain limited. This study evaluates patient satisfaction and opioid use among those using CTDs after carpometacarpal (CMC) arthroplasty or distal radius open reduction internal fixation (ORIF).
Methods:
A prospective analysis was conducted on 124 patients who underwent hand surgery by a single fellowship-trained surgeon between June 2023 and February 2025. A total of 92 patients who underwent CMC arthroplasty or distal radius ORIF were included. Patient-reported outcomes on pain relief, cryotherapy use adherence, and opioid usage were compared between CTD users and those using traditional ice packs.
Results:
In CMC arthroplasty patients, CTD users reported significantly higher pain relief scores (9.56/10 vs 3.42/10, P < .001) and greater adherence (>3 sessions/day: 94.4% vs 36.8%, P < .001) than ice pack users. Similar patterns were observed in distal radius ORIF patients, with higher CTD usage at both 3 and 7 days postoperatively (96% vs 11% and 88% vs 11%, respectively; P < .001). In distal radius ORIF patients, CTD users demonstrated a significant increase in 6-week Single Assessment Numeric Evaluation (SANE) score. No significant difference in oxycodone consumption was observed between groups for either procedure.
Conclusion:
CTD use following CMC arthroplasty and distal radius ORIF is associated with improved pain relief and adherence with cryotherapy. Although opioid use did not differ significantly, CTDs show promise as an adjunct for postoperative pain management in hand and wrist surgery.
Keywords
Introduction
Cold therapy, also known as cryotherapy, is routinely used for both acute and chronic musculoskeletal sport injuries in addition to rest, compression, and elevation. 1 The use of localized application of cold therapy has been extended to the management of postoperative swelling, pain, and inflammation in an effort to improve function, rehabilitation, and patient outcomes. 2 The analgesic effect of cold therapy is associated with the slowing of pain signal transmission and reduction of muscle spasms and edema formation.1,2 The clinical application of cold therapy has been widely studied with regards to ankle sprains, knee ligament repair, and total knee arthroplasty.3-8 Despite heterogeneous data, these studies collectively report improved clinical outcomes with cold compression therapy compared to no treatment at all, with some authors even suggesting that the effects of cold and compression are additive and reduce analgesic requirements.8-10 A more recent meta-analysis has demonstrated that the application of cryotherapy over incisions in the postoperative period has a moderate effect on pain reduction and opioid use, without increasing hospital length of stay or risk of surgical site infection. 11
Hand and upper-extremity surgeries are among the most common procedures performed in the United States, with patients often prescribed opioid medication for postoperative pain management. 12 Approximately one-third of hand surgery patients complain of moderate to severe pain after outpatient surgery, with postoperative pain serving as one of the most common reasons for readmissions or emergency department visits.12-14 Given that up to 17% of patients undergoing upper-extremity surgery report chronic opioid use, hand surgeons should consider nonpharmacologic measures such as cold therapy when addressing postoperative pain.15-17 The application of cold therapy has been sparsely studied in the field of hand and upper-extremity surgery. A randomized, prospective study of patients following shoulder surgery found continuous cryotherapy to be associated with decreased opioid consumption and pain intensity. 18 Similarly, a 2021 study by Pouedras et al 19 demonstrated significantly lower in-hospital morphine consumption and lower at-home use of nonsteroidal anti-inflammatory drugs among patients administered cryotherapy after surgery of the wrist and/or base of the thumb.
Technological strides have been made in cryotherapy devices over the years, with Polar Care©, Breg Inc.©, Game Ready©, and CoolSystems Inc.© becoming popular cryopneumatic devices. 20 These systems include a wrap that snuggly fits around the operative extremity, then maintains a steady, precise cooling level. 20 However, there remains a scarcity of mainstream hand-specific cryotherapy devices; some products include the Aircast Cryo Cuffs© and Aircast Gravity Cuffs© offered by DONJOY manufacturing, which range anywhere from $58.99 to $169.99, a substantial cost that is often not covered by insurance.21-24 Despite the well-known advantages of cold application, there is a substantial gap in the literature regarding its impact on patient satisfaction and narcotic use following hand surgery. A recent study by Henn et al 25 found that ice applied over plaster splints does significantly reduce skin temperatures underneath splinted wrists, but its clinical significance and comparison to ice applied underneath the splint remain unknown. This is the first known study to investigate the short-term effect of using a postoperative cold therapy device (CTD) following hand surgery on pain relief, patient experience, and narcotic intake. We hypothesize that continuous CTDs applied under splints will lead to improved postoperative pain control, adherence, and decreased opioid use compared to standard instructions to apply ice over splints.
Materials and Methods
Following approval from the University of Connecticut’s institutional review board, a prospective cohort study was conducted of patients undergoing either open reduction internal fixation (ORIF) of distal radius fractures or carpometacarpal (CMC) joint arthroplasty during an enrollment period of February 2023 to April 2025. All patients were indicated for surgery by one senior author, a fellowship-trained orthopedic hand surgeon. All patients underwent a period of immobilization in a plaster splint in the immediate postoperative period. Patients who underwent distal radius ORIF were immobilized in a volar wrist plaster splint and patients undergoing CMC joint arthroplasty in a thumb spica plaster splint. At the time of splint application, they were selected by the senior author to either have the CTD applied underneath their splint or not at all. Participants in the CTD group had agreed to pay any additional copay for the CTD preoperatively and were indicated for the treatment group. If CTD was applied, the incisions were initially dressed in xeroform and gauze, 3 layers of cast padding, followed by the CTD, plaster splint, and ace wrap (Figure 1). The NICE© iceless hand and wrist recovery compression system was selected as it is the system most widely used in our institution following orthopedic surgeries. All patients administered CTD were given instructions on how to safely use the device by the nurses in the recovery area. They were instructed to refill with water, then turn on and use the ice machine 20 minutes at a time at least 5 times a day, but more was encouraged. Those that did not receive the CTD were advised to apply ice packs directly over their splints for the same frequency. This was discussed with them prior to discharge and provided with their discharge instructions. All patients were seen for a 2-week follow-up visit where splints and sutures were removed, and they were recommended to start gentle wrist or thumb range of motion but remain non-weight-bearing for an additional 4 weeks.
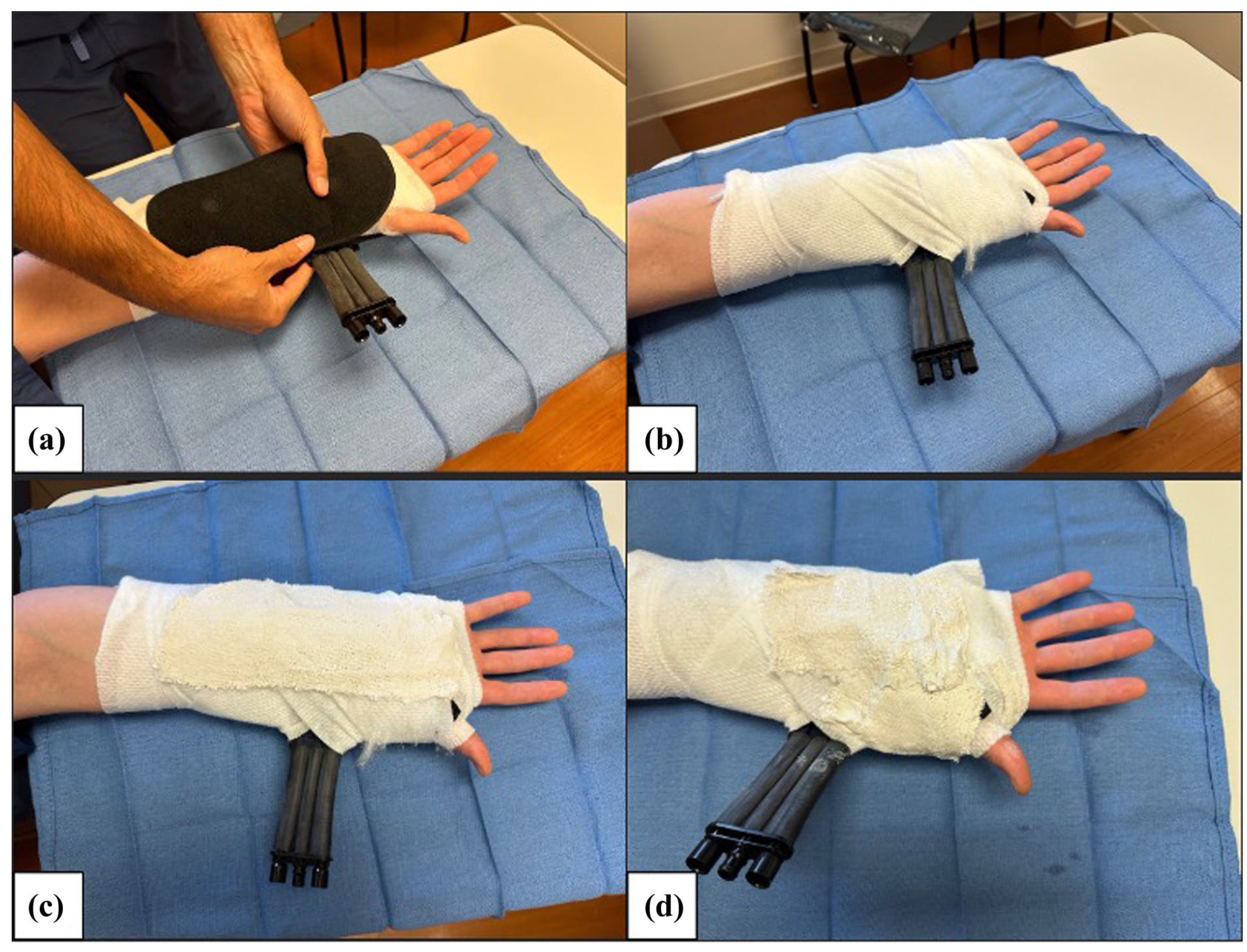
Demonstration of post-operative cold therapy device application. (a) Application of NICE© cold therapy device over standard postoperative dressing. (b) Cast padding wrapped around cold therapy device prior to splint placement. (c) Volar slab plaster application following distal radius open reduction internal fixation. (d) Thumb spica plaster application following carpometacarpal arthroplasty.
Inclusion criteria included all patients aged 18 years or older indicated for an elbow-distal upper-extremity surgery who were immobilized in a form of splint temporarily in the immediate postoperative period. Exclusion criteria included patients younger than 18 years, failure to fill out the postoperative questionnaire, non-English-speaking, patients undergoing revision surgery, and patients undergoing procedures besides distal radius ORIF or CMC arthroplasty. All surgeries were performed in the outpatient surgery center, and all patients were discharged on the same day. Postoperative pain control included recommendations for over-the-counter ibuprofen and tylenol as needed, and each patient was prescribed 25 tablets of 5 mg of oxycodone.
Patient satisfaction and postoperative pain control surveys adapted from previously published questionnaires were administered at the first postoperative visit to all patients at approximately 2 weeks postoperatively. Patients were not incentivized to complete the surveys or participate in the study. The surveys included 7 questions assessing the patients’ confidence in using the device, pain relief satisfaction, frequency of device or ice pack use, and number of narcotic tablets used during the postoperative period (Supplemental 1). All surveys were administered either by qualified medical assistants or advanced practice registered nurses. Single Assessment Numeric Evaluation (SANE) score was collected preoperatively and at the 6-week postoperative visit. To assess this, patients are asked to rate their extremity as a “percentage of normal” from 0 to 100; higher SANE scores indicate better hand performance. The single-item SANE score is a reasonable outcome measure of global hand function and has been utilized in prior upper-extremity studies. 26 The surgeon was not present during survey administration or SANE score collection to avoid potential response bias. The primary outcome measures included pain relief satisfaction with using the CTD, the frequency of CTD or over-the-counter ice pack use, number of oxycodone tablets utilized, and change in preoperative and postoperative SANE score between these two cohorts.
Deidentified data was extracted into a Microsoft Excel spreadsheet version 16.16.21 (Microsoft Corporation, Redmond, Washington; 2016). All statistical analyses were performed by the lead author using SPSS version 26 (IBM Corporation, Armonk, New York). Student t-tests were used to compare data for continuous variables between the CTD and non-CTD groups. The threshold for statistical significance was determined by a P-value of less than or equal to .05.
Results
There was a total of 124 patients who met inclusion criteria during this time. The majority of patients underwent CMC arthroplasty (57) and distal radius ORIF (35), with the remaining surgeries including distal biceps repair, distal humerus ORIF, olecranon ORIF, elbow ligament repair, wrist fusion, and olecranon ORIF. Because the majority of patients underwent CMC arthroplasty or distal radius ORIF, the 32 patients who underwent alternative procedures were excluded. Among the 57 patients (12 males) who underwent CMC arthroplasty, 36 patients utilized a CTD postoperatively, while 21 patients were in the control group. For the 35 patients (5 males) who underwent distal radius ORIF, 25 patients utilized CTD while 10 were in the control group. The average age of the CMC arthroplasty group was 58.3 years, and the average age of the distal radius ORIF group was 56.3 years (Table 1).
Demographics of Patient Cohort.
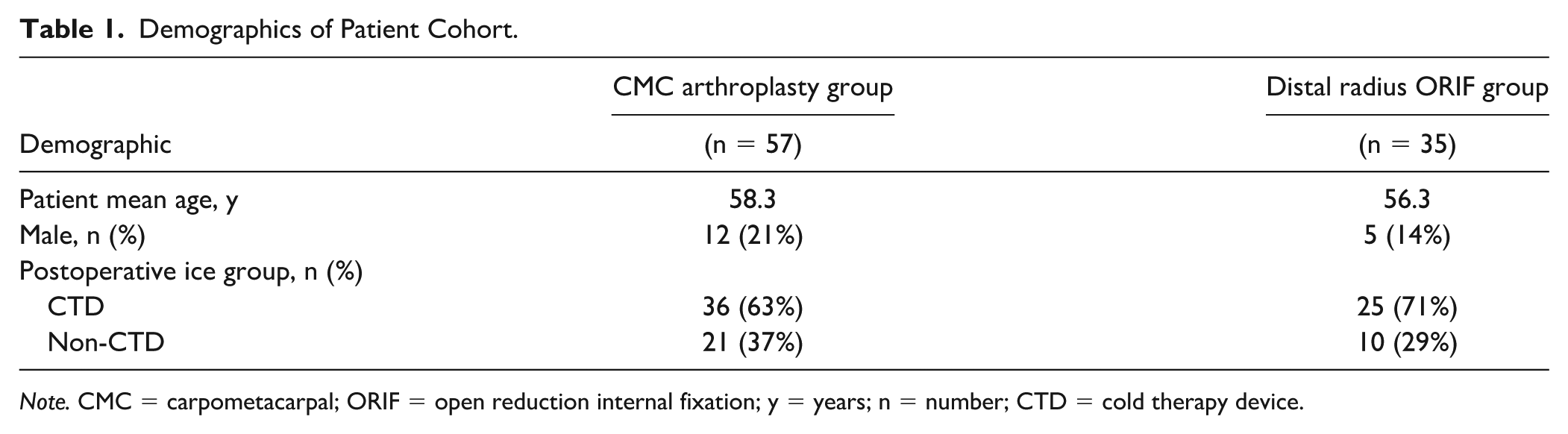
Note. CMC = carpometacarpal; ORIF = open reduction internal fixation; y = years; n = number; CTD = cold therapy device.
Of the patients who underwent CMC arthroplasty, CTD users reported an average of 9.75 (8.57-10.93) out of 10 on a Likert scale (95% CI: 9.36-10.14) in overall pain relief satisfaction postoperatively (Table 2). When further asked to clarify how much they believed the CTD directly helped in alleviating their postoperative pain, they reported an average of 9.56 (8.26-10.86) out of 10 (95% CI: 9.14-9.98) (Table 2). Those assigned to CTD had greater adherence with ice therapy at both 3 and 7 days postoperatively compared to those without CTD (100% vs 47.62%, 91.67% vs 19.05%, P < .001) (Table 3). The CTD patients also endorsed a significantly greater daily use of CTD compared to the ice pack group (P < .001). The 3 or more sessions per day rate of CTD use was 94.44% compared to 36.84% in the ice pack group (Table 3). Similarly, 77.78% of patients used CTD for more than 7 sessions on any given day compared to 5.26% in the ice pack group (Table 3). Patients with CTD reported significantly increased effectiveness in how much ice therapy alleviated their pain (average 9.56 [8.26-10.86] out of 10) compared to those without CTD (3.42 [0.19-6.65] out of 10) (P < .001) (Table 3). Cold therapy device users consumed less oxycodone tablets on average (8.51 tablets) than non-CTD users (13.38 tablets) by their first postoperative visit, though this did not reach statistical significance (P = .0687) (Table 3). Twenty-eight patients in the CTD group and 12 patients in the non-CTD group completed both preoperative and postoperative SANE scores. The average change in SANE score at the 6-week postoperative visit was 14.46 (−10.87 to 39.79) in CTD users and 14.58 (−10.60 to 39.76) in non-CTD users (P = .98) (Table 4).
Patient-Reported Outcomes and CTD Utilization Following CMC Arthroplasty.
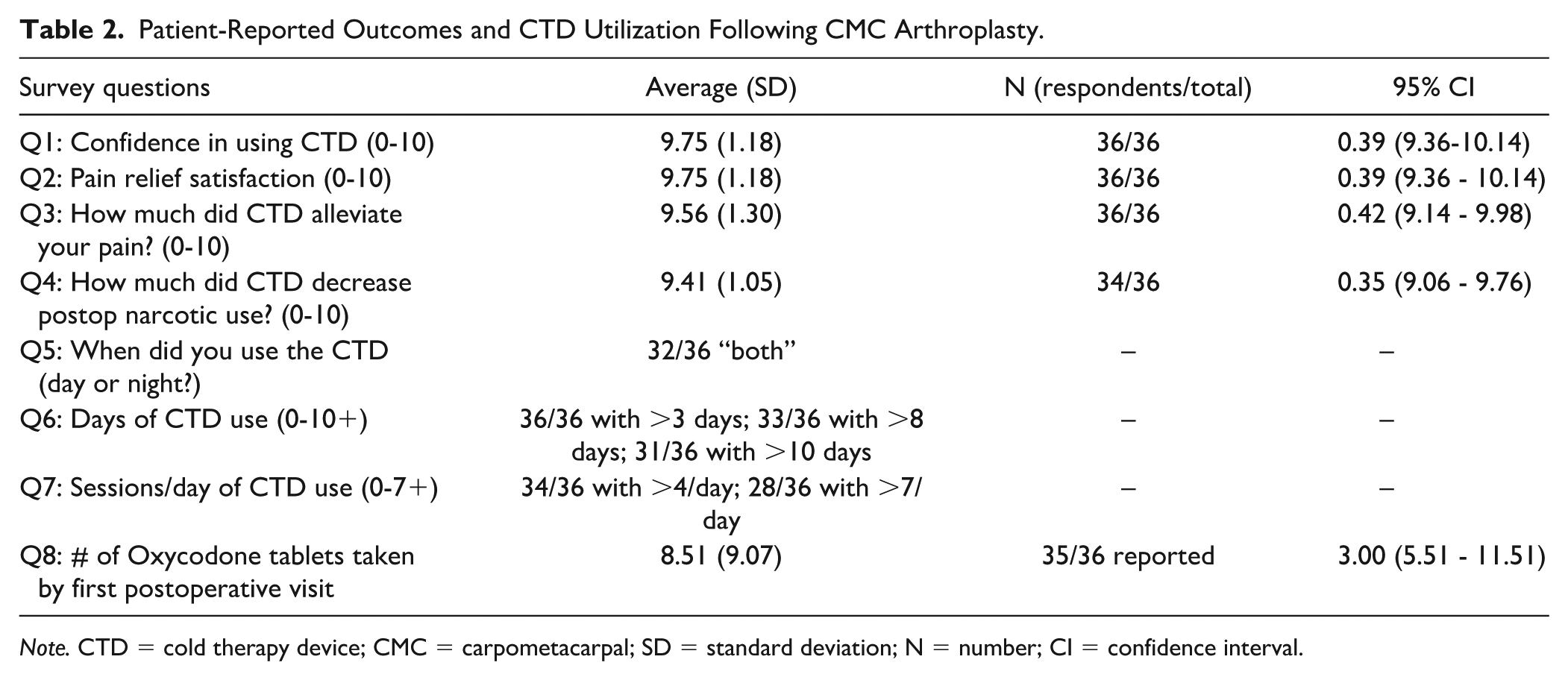
Note. CTD = cold therapy device; CMC = carpometacarpal; SD = standard deviation; N = number; CI = confidence interval.
Comparative Analysis of Postoperative Pain Relief and Analgesic Use in Cold Therapy.
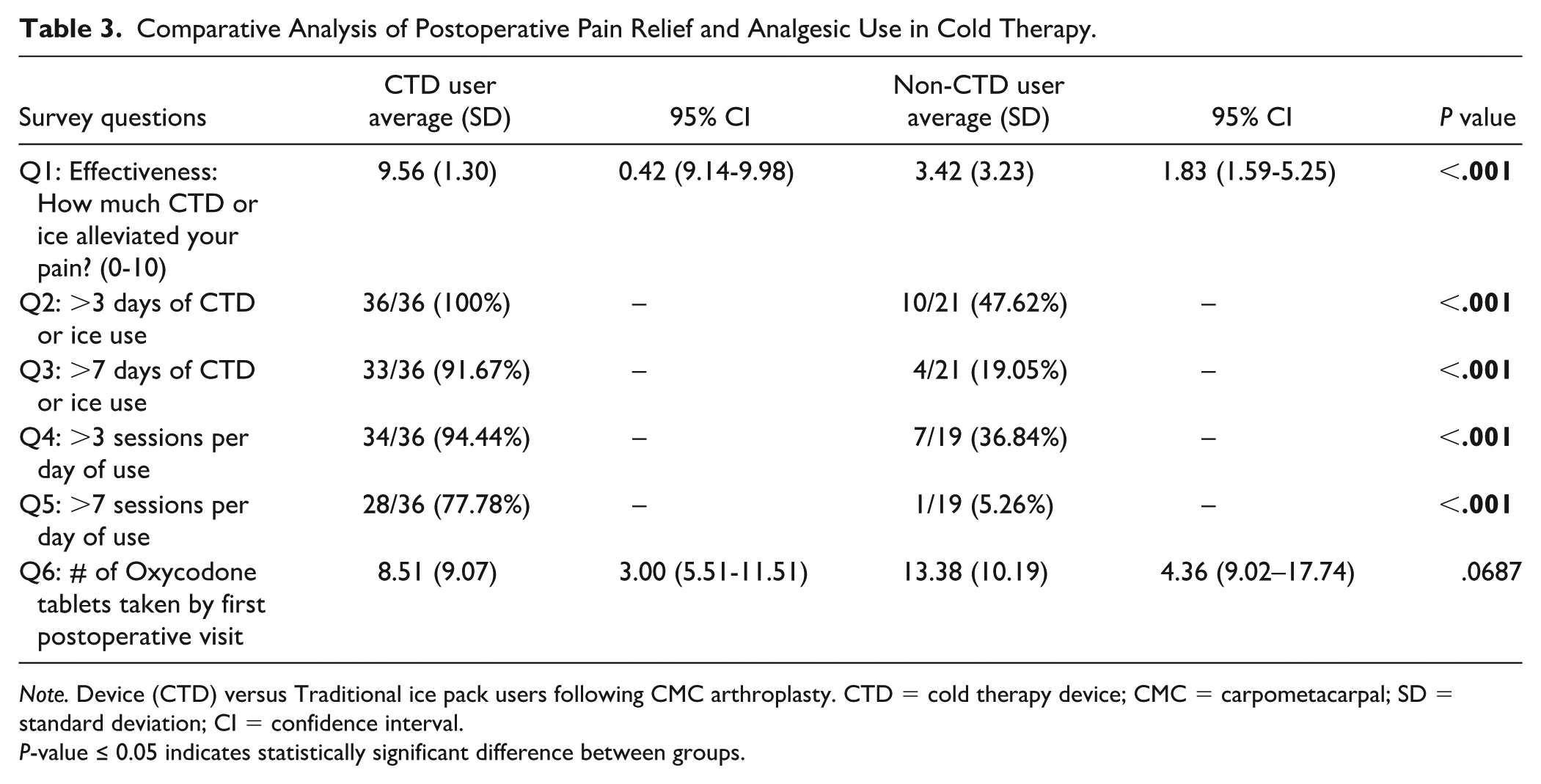
Note. Device (CTD) versus Traditional ice pack users following CMC arthroplasty. CTD = cold therapy device; CMC = carpometacarpal; SD = standard deviation; CI = confidence interval.
P-value ≤ 0.05 indicates statistically significant difference between groups.
Average Change in SANE Score Following CMC Arthroplasty.

Note. SANE = Single Assessment Numeric Evaluation; N = number; CTD = cold therapy device; CMC = carpometacarpal.
Among patients who underwent distal radius ORIF, CTD users reported an average of 9.68 (8.99-10.37) out of 10 (95% CI: 9.41-9.95) in pain relief satisfaction with CTD and average of 9.4 (8.40-10.40) (95% CI: 9.01-9.79) when asked to rate how much CTD alleviated their postoperative pain (Table 5). Those who used CTD had greater adherence of CTD use than those assigned to ice pack therapy alone at both 3 and 7 days postoperatively (CTD 96% vs non-CTD 11%, 88% vs 11%, P < .001) (Table 6). The CTD group also reported more frequent use of CTD within any given day than those who used ice packs alone, with 100% patients using the CTD more than 3 sessions per day and 72% more than 7 sessions per day compared to 12.5% of patients using ice packs more than 3 times per day and 0% using the ice pack more than 7 times per day (P < .001) (Table 5). Unfortunately, only 1 non-CTD user reported on the effect of ice packs alone on pain relief (rating 4 out of 10) which was too low to compare efficacy between groups. There was no significant difference in number of oxycodone tablets consumed at the time of the first postoperative visit between the two cohorts (P = .784) (Table 6). The average change in SANE score was 71.94 (54.11-89.77) in the CTD group and 50 (26.91-73.09) in the non-STD group which reached significance (P = .018) (Supplemental 2).
Patient-Reported Outcomes and CTD Utilization Following Distal Radius ORIF.
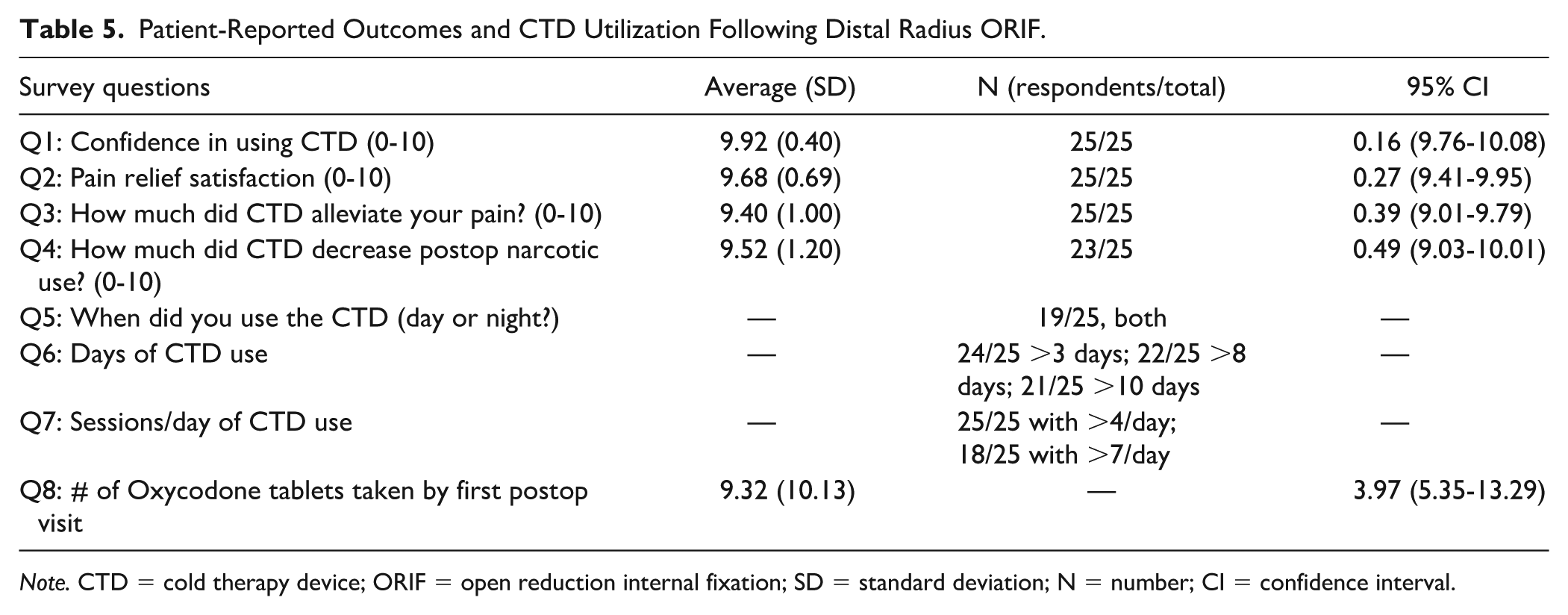
Note. CTD = cold therapy device; ORIF = open reduction internal fixation; SD = standard deviation; N = number; CI = confidence interval.
Comparative Analysis of Postoperative Pain Relief and Analgesic Use in CTD Versus.
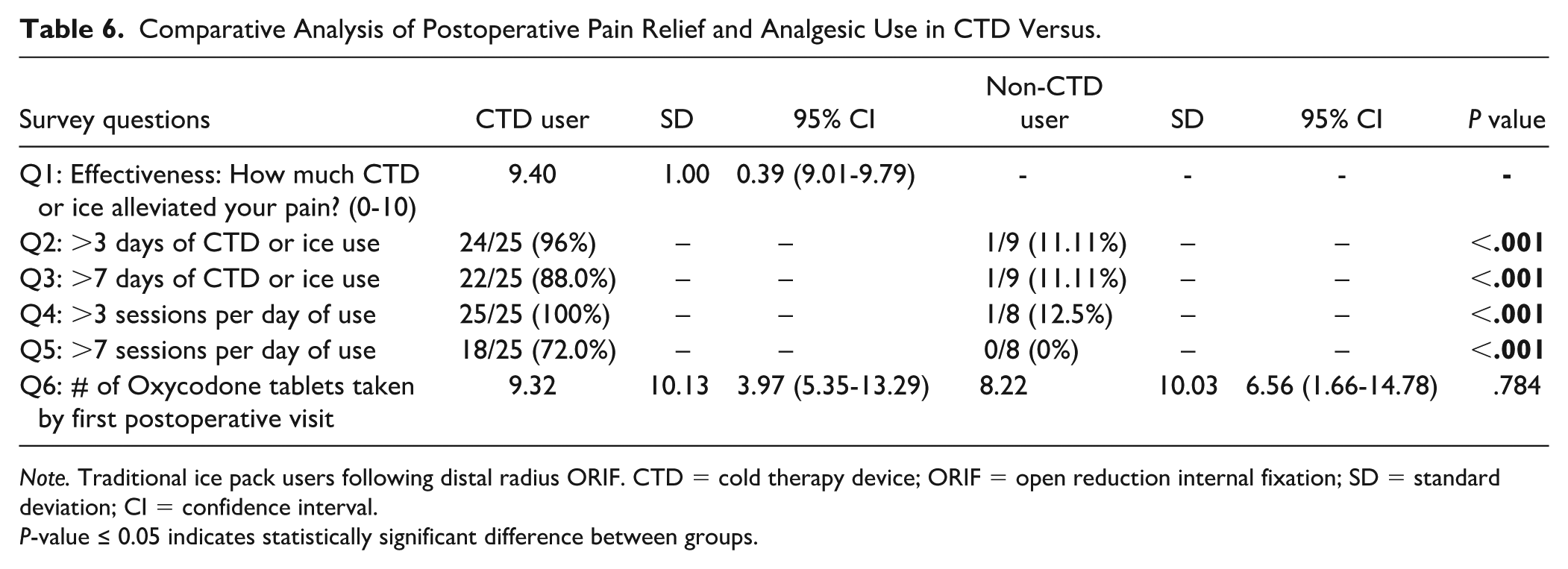
Note. Traditional ice pack users following distal radius ORIF. CTD = cold therapy device; ORIF = open reduction internal fixation; SD = standard deviation; CI = confidence interval.
P-value ≤ 0.05 indicates statistically significant difference between groups.
One patient with CTD returned to clinic on postoperative day 1 because of a faulty ice connection, causing water to leak onto their splint. This was replaced without incident. No other complications were noted.
Discussion
Postoperative pain control is an important concern for both patients and surgeons. Inadequate pain control can lead to postoperative complications and decreased patient satisfaction, as well as stiffness and lower recovery of function. 27 Despite the high number of hand procedures performed in the United States, there remains little consensus on the most appropriate pain-control regimen after common hand surgeries. The majority of current hand literature focuses on postoperative medicinal use.27,28 Hand and upper-extremity surgeons are generally high-volume surgeons who routinely prescribe opioids postoperatively. 28 Opioid abuse and dependence increased 152% in hand surgery patients between 2002 and 2011 and are associated with complications such as respiratory failure, infection, cardiac complications, hyperalgesia, and gastrointestinal issues.12,28 Fortunately, there has been a trend toward reducing opioid overprescription by hand surgeons, 28 but few studies on alternative nonmedicinal forms of postoperative pain control are known to exist.
As an alternative to pain medications, cryotherapy has been used for many years to relieve pain following trauma to bones or soft tissues. 20 Its postoperative use has been well studied, most frequently in arthroplasty and arthroscopic cases,18,29 but its reported efficacy in hand procedures remains limited. This study demonstrated that the addition of a CTD under the postoperative splint in patients undergoing distal radius ORIF or CMC arthroplasty was utilized by patients at a higher rate and demonstrated considerable efficacy in reducing postoperative pain control. Patients in the CTD group who underwent distal radius ORIF also demonstrated a significant improvement in SANE score at the 6-week postoperative visit compared to their non-CTD counterparts. This suggests that CTD may improve short-term patient-reported outcomes when treating traumatic distal radius injuries. This may be secondary to increased preoperative inflammatory mediators and soft-tissue injury in traumatic cases compared to cases for chronic arthritic pain. 30 However, additional studies would be needed to compare efficacy in postoperative pain between operative cases for trauma versus elective cases. There was also a trend toward decreased opioid use in the immediate postoperative period, particularly for CMC arthroplasty, though this did not reach statistical significance.
Additional studies on cryotherapy in hand surgery also demonstrated mixed results with small sample sizes. Pouedras et al 19 performed a prospective study on 60 patients who had undergone wrist or base of thumb bony procedure, and half were managed with cryotherapy. They found that postoperative morphine and nonsteroidal antiinflammatory drug consumption was significantly lower in the cryotherapy group, but the overall pain score was not significantly different between groups. Meyer-Marcotty et al 31 randomized 54 patients undergoing wrist arthroscopy to either use a cryo/cuff or standard care over 3 weeks postoperatively and discovered increased postoperative pain reduction in the cryo/cuff group, although this did not reach statistical significance. Similar to these prior studies, our studies demonstrate a trend toward improved postoperative ice adherence, decreased narcotic use, and improved postoperative pain in patients using CTD following distal radius ORIF and CMC arthroplasty. We believe this is related to increased convenience of having a continuous cooling system that is easily refillable underneath the splint. Furthermore, although Henn et al 25 found that ice applied over the splint significantly decreased skin temperature, we believe having an ice machine underneath the splint likely increases cooling capabilities as well as surface area of efficacy. They also acknowledged that their study was not designed to analyze the clinical significance of these temperature changes. 25
Overall, cryotherapy is a relatively low-risk and safe postoperative tool. Complications related to cryotherapy are often secondary to poor patient understanding or prolonged duration of use. 30 The most published complications include skin reactions such as frostbite injuries and skin necrosis; however, these can often be avoided by proper patient counseling and avoiding direct skin contact. 30 Only one patient in our study had a complication secondary to faulty tubing of their cryotherapy causing their postoperative splint to get wet. This was promptly recognized and replaced without further complication.
This study has several limitations. First, we are limited by our small study size and did not perform a power analysis which possibly impacted the ability of our results to achieve statistical significance. There was also a difference in size and demographics between the two cohorts as well as the treatment groups within them. The inability to randomize and blind these patients to their treatment group also likely produced an element of selection bias, as participants in the treatment group had to agree to pay any additional copay for the CTD preoperatively. The generalizability of our data was limited to 2 hand procedures, distal radius ORIF and CMC arthroplasty, although these are two of the most common hand procedures that require postoperative splint immobilization. Furthermore, the survey-based nature of this study inevitably creates recall bias as well as inconsistent completion of some portions of the surveys included, limiting the generalizability of our results. Lastly, the patient administered surveys did not inquire about amount and frequency of nonnarcotic pain medication use in the postoperative period, such as acetaminophen and ibuprofen which may lead to additional bias. Larger, prospective studies on the effect of CTDs on postoperative pain control, patient satisfaction, and longer-term rehabilitation are necessary.
Conclusion
This study demonstrates that cryotherapy provided in the form of a CTD was associated with significantly higher patient-reported pain relief and improved ice adherence compared to traditional ice pack use following CMC arthroplasty and distal radius ORIF. Although the reduction in opioid consumption did not reach statistical significance, the data suggests a correlation with CTD and decreased postoperative narcotic use, especially among patients undergoing CMC arthroplasty. These findings support the use of CTD as a tool for postoperative pain management of common upper-extremity procedures. Larger, randomized control studies are needed to confirm these results and better elucidate long-term functional outcomes. Future goals include creating more data to support the complete coverage of CTDs by insurance companies and incentivizing more companies to create hand- and wrist-specific devices.
Supplemental Material
sj-docx-1-han-10.1177_15589447251404961 – Supplemental material for A Cold World: Pain Outcomes and Patient Experiences Utilizing an Iceless Cold Compression System After Hand Surgery
Supplemental material, sj-docx-1-han-10.1177_15589447251404961 for A Cold World: Pain Outcomes and Patient Experiences Utilizing an Iceless Cold Compression System After Hand Surgery by Francine Zeng, Seema M. Patel, Brian Ford, Dillon Neumann and Anthony Parrino in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Animal and Human Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.