
Abstract
Background:
Flexor tendon injuries remain a challenge for hand surgeons. The constraints of the pulley system with the need for a strong repair require a delicate balance. Suture repair has been the gold standard. The 4-strand locked cruciate stitch is the technique of choice for many. This can be laborious and technically difficult. Tendon stapler devices (TSDs) aim to provide fast, strong, low-profile repairs. Industry data have shown stronger TSD repairs compared with suture repair techniques. We aim to further explore the relative strengths of TSD and 4-strand locked cruciate repairs in cadavers.
Methods:
Twenty-four flexor tendons were used for 12 suture repairs and 12 TSD repairs. Four-strand locked cruciate repairs used 3-0 braided composite suture. The TSD repairs used CoNextions devices. Specimens were analyzed on a uniaxial load frame and distracted at 0.5 mm/s. Tension was recorded at 100 Hz. A camera system measured reference point positions at 10 Hz. Maximum tension and tension at 2-mm gap formation were recorded. Independent t-tests were used to compare groups, with significance noted by P < .05.
Results:
Load to failure for the staple group and suture group were 70.6 ± 20.5 N and 49.9 ± 14.1 N, respectively. Load to 2-mm gap for the staple group and the suture group were 57.5 ± 21.1 N and 38.6 ± 13.7 N, respectively. Mean load to failure and load to 2-mm gap were significantly greater in the TSD group.
Conclusions:
In this study, TSD repairs were stronger than the 4-strand locked cruciate suture repair. Further clinical studies and cost analyses are necessary to support their widespread use.
Introduction
Flexor tendon injuries can present a challenging clinical scenario for hand surgeons. They occur from either sharp lacerations or blunt trauma and can result in complete, partial, or avulsion type injuries. With an incidence of 33.2 per 100 000 person years, strict rehabilitation protocols, and associated other bony and soft tissue injuries, flexor tendon injuries incur a burden on the hand surgeon’s practice and the system at large.1,2
From a surgical perspective, flexor tendon injuries can be difficult to treat due to the need to maximize repair strength to allow early motion while maintaining a low profile and smoothly gliding tendon surface to avoid adhesions. The ideal primary flexor tendon repair coapts tendon ends, allows postoperative tendon gliding, avoids damage to the complex pulley system, minimizes peritendinous adhesion, and allows for early range of motion with a low risk of repair gapping and/or failure.3,4 Complications include stiffness most commonly with repair failure occurring less frequently. 5 The mainstay of flexor tendon repair involves placement of an adequate number of core sutures via a number of proposed techniques. The 4-strand locked cruciate stitch is the technique of choice at some institutions and has shown superior biomechanical strength to several other repair techniques (mattress, modified Kessler, Strickland).2,6 -11
Tendon stapler devices (TSDs) have been developed to provide a strong and low-profile repair that can be quickly and easily used by experts and novices. Industry sponsored studies have shown stronger repairs, less gliding friction, and easier user learning curve compared with traditional suture repairs. This study aims to provide biomechanical analysis for flexor tendon repair using a TSD compared with a standard 4-strand locked cruciate suture repair. We hypothesize that repairs with a TSD will withstand higher forces for 2-mm gap formation and failure compared with 4-strand locked cruciate suture repair.
Methods
Twenty-four flexor digitorum profundus and flexor digitorum superficialis tendons were transected and repaired to make 12 four-strand locked cruciate (control) repairs and 12 staple (CoNextions, Salt Lake City, Utah) repairs. Tendons were prepared in 7-cm lengths and transected at the midpoint. This allowed for 2 cm at either end for fixation to the testing apparatus and 3 cm between them. The suture repairs utilized a 3-0 braided composite suture (FiberWire; Arthrex, Naples, Florida) using the standard described technique. 12 Tendon stapler device repairs were completed according to manufacturer recommendations using an approximating 3-0 simple absorbable stitch prior to device deployment. The device deploys a stainless steel staple to either end of the cut tendon connected by strands of high-strength polyethylene. All repairs were performed by 1 hand surgery fellow in his last 3 months of fellowship training and inspected for quality by the senior author. The width (largest dimension) and thickness (smallest dimension) of the tendons were measured at the transection site with a calibrated caliper. An oval shape was assumed and a cross-sectional area for each tendon was calculated. Fiducials were applied as close to the transection site as possible with pins through the tendon ends. The repairs were loaded into a load frame (Bionix 858; MTS, Eden Prairie, Minnesota) and distracted at 0.5 mm/s until failure occurred (Figure 1). Applied tension was recorded at 100 Hz. A camera system synchronized with the applied tension (DMAS; Spica Technology Corporation, Fox Island, Washington) measured the fiducial 3D positions at 10 Hz. The camera system was calibrated to reference positions based on manufacturer recommendations prior to recording. The maximum tension applied during a trial was extracted and recorded as the failure tension. The distance between the fiducials was calculated and used to determine the load required to create a 2-mm gap. Maximum load to failure and load to 2-mm gap formation were used for comparison in line with previous biomechanical studies comparing repair techniques.9 -11 Separate independent t-tests were used to compare the 2 repair groups for differences in cross-sectional area, maximum tension, and the tension prior to the formation of a 2-mm gap. A significant difference was indicated by a P value less than .05.
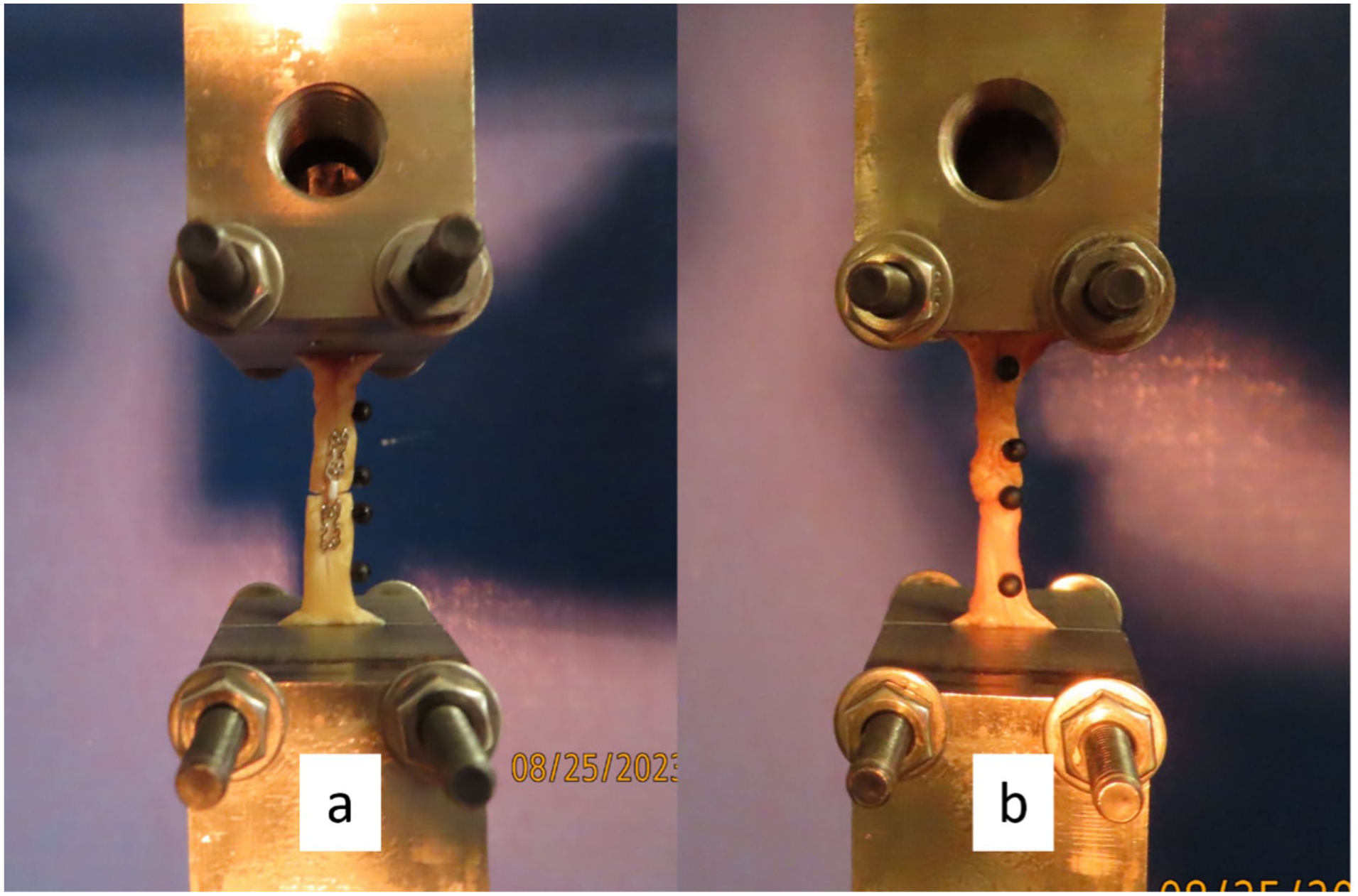
The (a) staple and (b) cruciate repairs mounted in the load frame with fiducials attached prior to testing.
Results
The load to failure (P = .008) and load to 2-mm gap (P = .016) means were significantly larger in the staple group than in the cruciate group (Figure 2). The load to failure for the staple group and cruciate group were 70.6 ± 20.5 N and 49.9 ± 14.1 N, respectively. The load to 2-mm gap for the staple group and the cruciate group were 57.5 ± 21.1 N and 38.6 ± 13.7 N, respectively. The cross-sectional areas for the staple group (11.3 ± 4.0 mm2) and the cruciate group (11.1 ± 4.3 mm2) were not significantly different (P = .904).
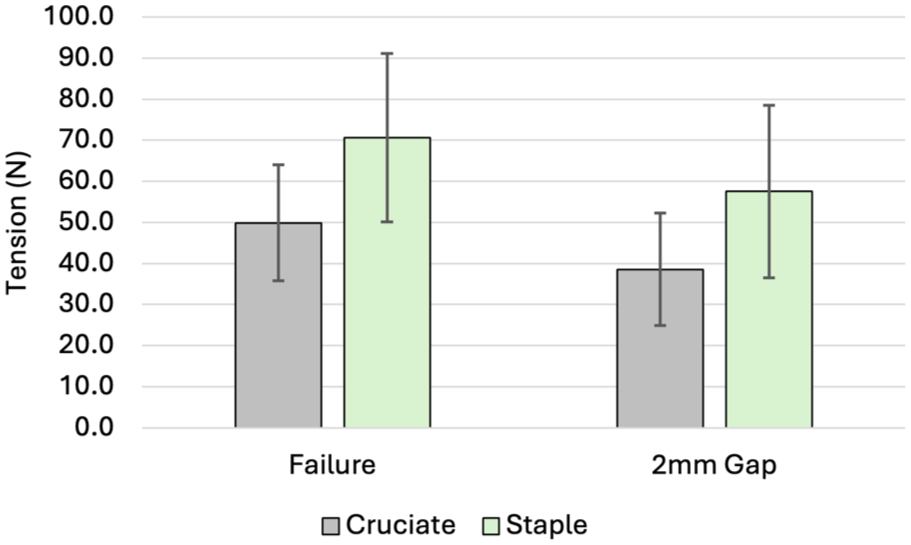
Comparison of cruciate and staple flexor tendon repairs by load to failure and load to 2-mm gap. Error bars represent standard deviations.
Discussion
Flexor tendon injuries continue to be a clinical burden. The challenge is only compounded when these injuries occur in zone 2. The tightly organized anatomy of the flexor pulley system requires a low-profile repair, while the tensile forces through the repair site during early motion, which is needed to decrease tendon adhesions, demand adequate strength.4,13,14 This balance is often difficult to strike and has driven hand surgeons in the search for an optimal solution.
The strength of any tendon repair technique is most dependent on the number and caliber of crossing strands of core suture.2,7 Epitendinous suture can confer additional repair strength, but not as substantial as additional core strands. There have been several suture techniques aiming to incorporate as many core strands as possible at the repair site, but increased strands and knots can increase bulk and therefore friction at the repair site causing failure.2,15 Commonly, a 4-strand cruciate technique has been used to provide excellent strength without excessive bulk. 16 Many efforts have been made to summarize the needs of a successful tendon repair. These include a stable fixation to avoid gapping and allow early active motion, low-profile repairs to allow for smooth tendon gliding, clear physician-patient communication, and strict hand therapy regimens.17,18
Any suture repair technique must also consider the mechanisms by which tendons heal. Tendon healing occurs through both intrinsic and extrinsic processes. Intrinsic healing entails the reformation of the internal tendon collagen structure providing tensile strength as the severed ends reunite. Extrinsic healing involves contributions from the flexor tendon sheath and can result in adhesions and scar formation, limiting motion and ultimately function.19,20 A balance between protecting the repair and early rehabilitation is crucial in maximizing intrinsic healing and minimizing extrinsic scarring which will limit motion and contribute to poor outcomes.
Previous tendon repair devices using stainless steel implants have been proposed in the past. 21 Some studies have shown them to be safe and effective with acceptable patient outcomes.21,22 Others have disputed these results citing no biomechanical advantage and call for strategic use of various tendon fixation methods depending on the clinical scenario and patient needs. 23 Tendon stapler devices represent a novel option in the care of flexor tendon injuries. The device-assisted repairs have been shown to have twice the load tension to failure as FiberLoop suture repairs in industry-sponsored testing. The peak tension achieved and tension to 2-mm gap formation in the TSD repair group was 89.2 N and 75.3 N, respectively, compared with 57.6 N and 33.0 N in the suture repair group.24 -26 The present study findings of TSD and suture repair load to failure (70.6 N and 49.9 N, respectively) and load to 2-mm gap formation (57.5 N and 38.6 N, respectively) are comparable and differences may be attributed to quality of cadaver tissue and the use of a different suture technique. In a study comparing TSDs with modified Kessler suture repairs, Reed et al also showed faster repair times, less variability based on level of experience, and lower friction of motion.27,28 The present study comparing the device to locked cruciate suture repairs shows similar load to failure improvements in the device repairs relative to suture repairs. Clinical trials have also shown the device to be safe and effective in human use. 29
Among the myriad of described suture repair techniques, the common thread of necessitating time and technical precision runs throughout. While experienced hand surgeons may be exceedingly proficient with their preferred technique, the time required can add up, especially in the case of multiple tendon lacerations. This problem can be compounded in the hands of someone less experienced or a trainee. One clinical scenario where time savings may be particularly important is in the case of multiple injured tendons. For instance, in a so-called “spaghetti wrist” many or all of the flexor tendons are injured at the level of the wrist or distal forearm. 30 A technique or device that could decrease the time of each individual tendon repair could add up to save significant time in the operating room for the patient and the surgeon. Previous tendon repair devices have been advocated in similar scenarios. 31 Another case in which time savings could be of significant value would be in finger or hand replantations and revascularizations. In these situations, meticulous microsurgical reconstruction of the vessels and nerves can be time-consuming as well as physically and mentally demanding. 32 By decreasing the time and effort required for the tendinous repair, surgical time and surgeon fatigue can potentially be diminished.
There are several limitations to the study. The tendons were not tested in situ and thus gliding friction in the pulley system could not be measured. All repairs were performed by a single surgeon and, thus, there is no ability to compare time to repair or repair quality based on experience as in previous studies. The use of cadaveric specimens may entail poorer tissue quality than that seen in vivo, which may alter the loads to failure that were measured. Biomechanical analysis was performed ex vivo and may not be as generalizable to actual clinical scenarios where surrounding anatomy and gliding forces are more applicable. We utilized the 4-strand locked cruciate repair as it is the technique of choice at our institution and has shown biomechanical advantages. However, additional comparisons between different repair techniques and using different suture materials (Ethibond, Supramid, etc.) would provide additional useful information.
Conclusions
Tendon stapler devices represent an intriguing new tool in the arsenal of the hand surgeon in the treatment of flexor tendon injuries. Additional research is necessary to further demonstrate strength, gliding, ease of use characteristics, as well as patient outcomes to support its more widespread use. Similarly, exploring dynamic failure at lower loads with cyclic testing may also prove useful. The study, however, shows promising evidence that the device can provide stronger tendon repairs with respect to 2-mm gap formation and ultimate failure compared with the 4-strand locked cruciate suture repair. The speed of deployment and quick learning curve of these devices may make them especially useful in the care of multiple tendon injuries.
Footnotes
Authors’ Note
The authors received CoNextions Tendon Stapler devices directly from the distributor free of charge. The manufacturer/distributor DID NOT have the right to review the data or manuscript prior to publication.
Author Contributions
Richard W. McKinney, MD—experimental design, data collection, manuscript authoring, manuscript editing.
Anna Barclay, MD—experimental design, data collection, manuscript authoring.
Jacob Sneddon, MD—experimental design, data collection.
Patrick J. Schimoler, PhD—experimental design, data collection, manuscript authoring, manuscript editing.
Alexander Kharlamov—experimental design, data collection.
Boyle Cheng, PhD—experimental design.
Peter Tang, MD—experimental design, data collection, manuscript editing.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This study contains no human or animal subjects.
Statement of Informed Consent
Informed consent was obtained when necessary.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no external or grant funding for the present study. Tendon stapler devices were supplied by CoNextions.