
Abstract
Background:
Carpal tunnel release (CTR) is one of the most commonly performed hand surgeries, with both open and endoscopic techniques widely used. This study analyzes US historical trends in CTR utilization among Medicare beneficiaries and projects future procedural volumes through 2040.
Methods:
Medicare Part B National Summary data from 2000 to 2022 were used to estimate annual procedural volumes for open (Current Procedural Terminology [CPT] 64721) and endoscopic (CPT 29848) CTR. Adjustments were made to account for the increasing proportion of Medicare Advantage enrollees. Four forecasting models—log-linear, Poisson regression, negative binomial regression, and auto-regressive integrated moving average (ARIMA)—were applied. Model performance was evaluated using mean absolute error and root mean square error, with ARIMA selected for its superior predictive accuracy.
Results:
From 2000 to 2022, the annual volume of open CTR increased by 180%, while endoscopic CTR grew by 959%. Auto-regressive integrated moving average projections indicate that open CTR will continue to grow at an average annual rate of 2.0%, reaching an estimated 424 271 procedures by 2040. Endoscopic CTR is projected to increase at a faster rate of 2.42% annually, with a forecasted volume of 184 723 by 2040. Despite this growth, open CTR is expected to remain the predominant approach.
Conclusions:
Carpal tunnel release utilization has increased substantially in the United States, with endoscopic techniques growing at a faster rate than open CTR. Despite this trend, open CTR is projected to remain the predominant approach. Future research should assess the economic impact, patient-reported outcomes, and factors influencing the adoption of each technique.
Introduction
Carpal tunnel syndrome (CTS) remains one of the most common neuropathies in the United States and can negatively affect quality of life, work productivity, and recreational capability in those affected.1,2 Carpal tunnel release (CTR) is the most common hand surgery procedure, likely due to its safety, efficacy, and relative ease. Roughly 3% to 5% of the US population is affected by CTS, and up to 600 000 CTR procedures are performed annually, with higher prevalence among employed people.3-5 These procedures are exceedingly effective at treating the condition; randomized trials have reported success rates to 90%.6,7 Due to their prevalence, these procedures represent a substantial cost and time burden on the American health care system and the patients it serves. 8 As CTR procedures have moved out of costly hospital operating rooms with patients under general anesthesia and into free-standing ambulatory surgery centers or medical offices with providers utilizing wide-awake, local anesthetic no tourniquet (WALANT) techniques, their prevalence continues to grow.9,10
There is ongoing debate regarding the optimal treatment approach for CTS, leading to a variety of management strategies. Non-surgical interventions, including physical or occupational therapy and corticosteroid injections, are often effective for symptom relief. However, for patients with persistent symptoms or those seeking definitive treatment, surgical CTR is indicated. Traditionally, the procedure has been performed via an open approach, which provides direct visualization of the transverse carpal ligament but results in a larger incision and increased scar burden. Recently, endoscopic CTR has gained significant popularity due to its potential to reduce postoperative complications such as infection and wound dehiscence.11-13 However, the increased use of instrumentation and higher personnel costs make endoscopic CTR more expensive for both patients and payers.14,15 Despite these cost differences, long-term outcomes are generally comparable between the 2 techniques, though endoscopic CTR allows patients to return to work up to 8 days sooner than those undergoing open CTR.16,17
Given the increasing utilization of endoscopic CTR, this study aims to evaluate recent and future trends in the adoption of open versus endoscopic CTR among Medicare patients in the United States using predictive modeling, quantifying the projected procedural burden of CTR and the expected balance between open and endoscopic techniques through 2040. These forecasts may help surgeons, health systems, and policymakers anticipate future demand, plan training and capital investments, and design cost-effective care pathways as CTR volume continues to grow.
Methods
Database
The data for this study were obtained from the Centers for Medicare and Medicaid Services (CMS) Medicare Part B National Summary, spanning the years 2000 to 2022. This publicly accessible dataset includes information on patients enrolled in traditional Medicare. To account for the increasing proportion of Medicare-eligible patients enrolled in Medicare Advantage plans, annual procedure volumes were adjusted using a previously published methodology. Specifically, a ratio of traditional Medicare to Medicare Advantage patients, as determined by the Kaiser Family Foundation, was applied to estimate the true prevalence of procedures. This adjustment resulted in uplifted annual volumes for both open carpal tunnel release (Current Procedural Terminology [CPT] code 64721) and endoscopic carpal tunnel release (CPT code 29848).
Statistical Analysis
Statistical analyses were conducted using R statistical software (version 4.4.0; R Project for Statistical Computing, Vienna, Austria). Uplifted annual procedure volumes from 2000 to 2022 were used as the basis for time-series forecasting through 2040. Four forecasting models, including log-linear (exponential growth), Poisson regression, negative binomial regression, and auto-regressive integrated moving average (ARIMA), were applied to generate forecasts. The log-linear model treats calendar year as a continuous predictor of the logarithm of annual procedure volume and assumes a constant proportional (exponential) growth rate over time. Poisson and negative binomial regression models both treat annual procedure counts as discrete events and model rates over time, with the negative binomial model allowing for overdispersion when variability exceeds the Poisson assumption. In contrast, the ARIMA framework models each year’s volume as a function of its own past values and random shocks, allowing for flexible representation of underlying trends and autocorrelation in the time series.
Model Evaluation and Selection
The performance of each model was evaluated using mean absolute error (MAE) and root mean square error (RMSE) to quantify the goodness of fit by measuring the error between observed and predicted values. Among these models, ARIMA was selected for its superior performance, as it demonstrated the lowest MAE and RMSE values, indicating the highest predictive accuracy. Although these models rely on different assumptions and functional forms, they all produced qualitatively similar forecasts, with steadily increasing volumes for both open and endoscopic CTR. The main differences were in the smoothness and precision of the projected curves, particularly at the extremes of the forecasting horizon, with ARIMA providing the most stable and least error-prone estimates. This agreement across methods supports the robustness of the overall projected growth trajectory despite methodological differences. Using the ARIMA model, point forecasts and 95% forecast intervals (FIs) were generated for annual procedure volumes from 2023 to 2040. Forecasted volumes were subsequently used to calculate annual and biennial growth rates for both open and endoscopic CTR procedures. Graphical representations of historical trends and future projections were created to illustrate differences in utilization patterns between the 2 techniques.
Results
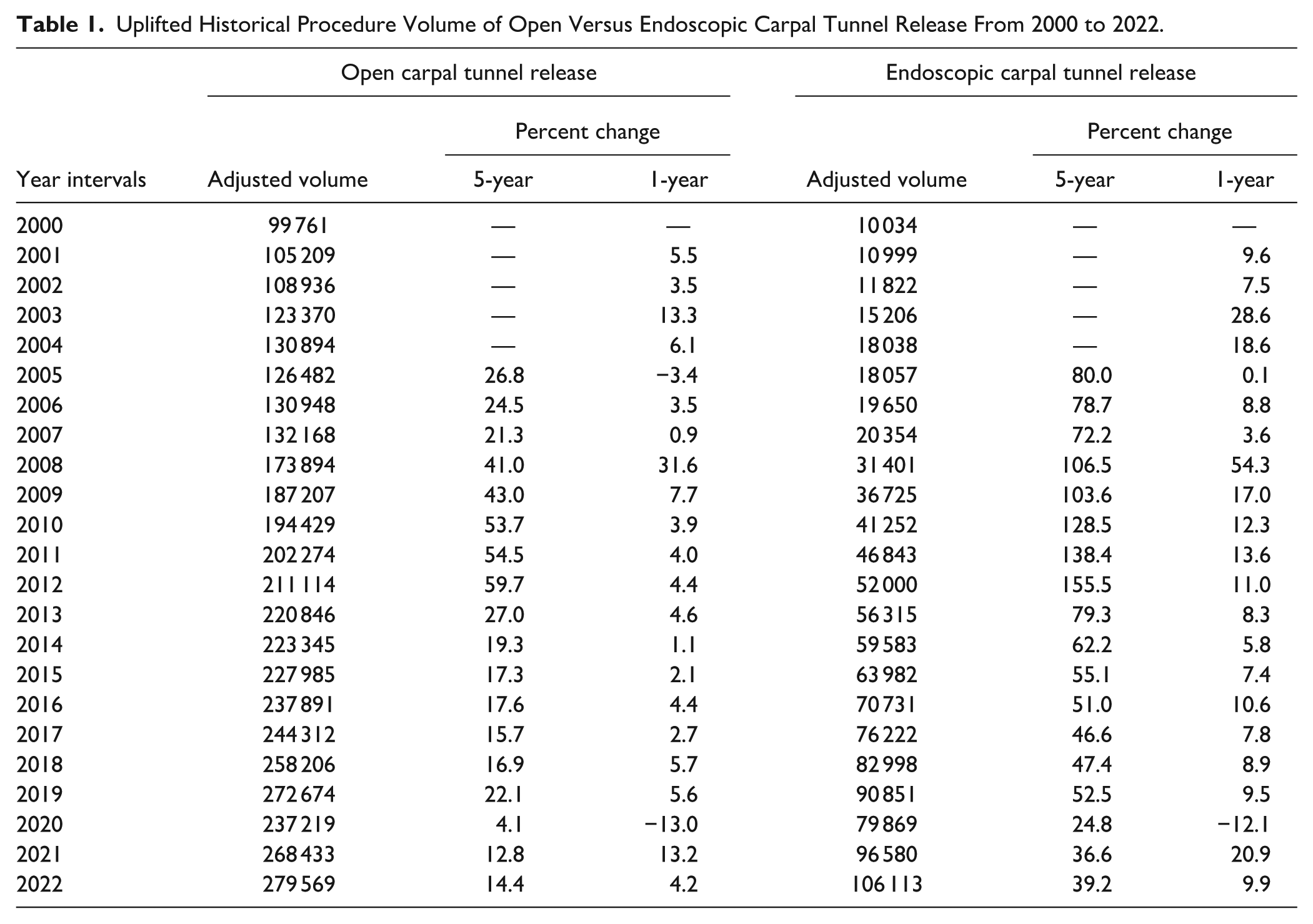
From 2000 to 2022, the uplifted annual volumes of open CTR procedures increased from 99 761 to 279 569, reflecting a 180% overall growth during this period. The highest annual growth occurred between 2008 and 2009, with a 31.6% increase. Conversely, a significant decline of 13.0% was observed between 2019 and 2020, coinciding with the COVID-19 pandemic. Similarly, endoscopic CTR procedures demonstrated substantial growth, rising from 10 034 in 2000 to 106 113 in 2022, representing a 959% increase. The most significant annual growth for endoscopic procedures was observed from 2007 to 2008, with a 54.3% increase (Table 1).
Uplifted Historical Procedure Volume of Open Versus Endoscopic Carpal Tunnel Release From 2000 to 2022.
Four forecasting models—log-linear, Poisson, negative binomial regression, and ARIMA—were applied to project the future utilization of open and endoscopic CTR procedures from 2023 to 2040. Auto-regressive integrated moving average demonstrated the best predictive performance, with the lowest MAE and RMSE across both procedure types. For open CTR, ARIMA achieved an MAE of 8046 and an RMSE of 12 129, outperforming the log-linear model (MAE: 191 169; RMSE: 199 863), Poisson model (MAE: 14 414; RMSE: 16 516), and negative binomial regression (MAE: 13 843; RMSE: 17 601; Table 2). Similarly, for endoscopic CTR, ARIMA yielded an MAE of 3196 and an RMSE of 4916, significantly lower than those of the log-linear (MAE: 48 495; RMSE: 56 987), Poisson (MAE: 5812; RMSE: 6680), and negative binomial models (MAE: 6316; RMSE: 9479; Table 3).
Forecast Model Outputs for Open Carpal Tunnel Release.
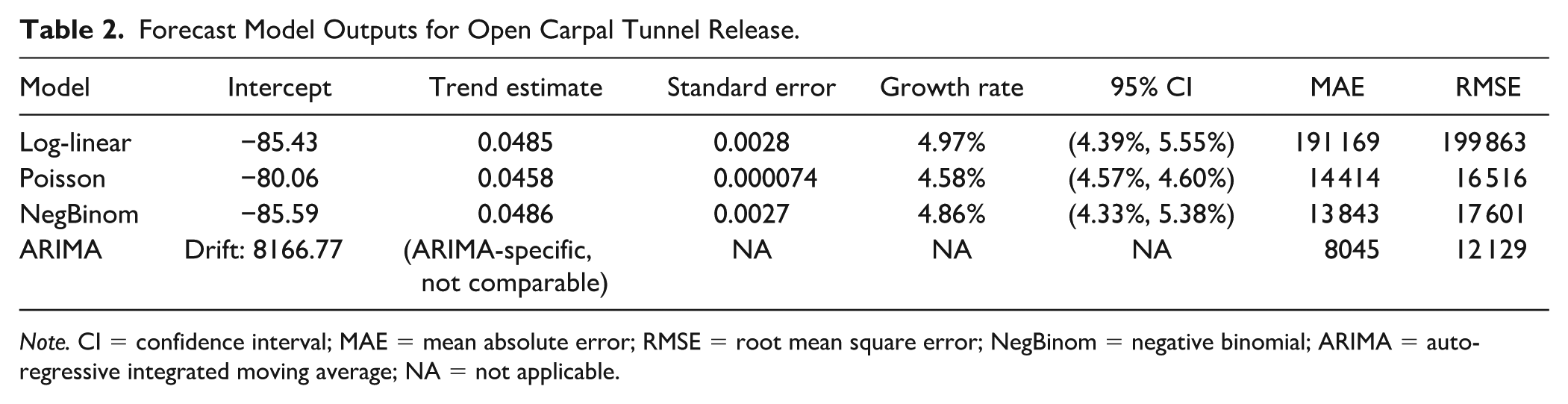
Note. CI = confidence interval; MAE = mean absolute error; RMSE = root mean square error; NegBinom = negative binomial; ARIMA = auto-regressive integrated moving average; NA = not applicable.
Forecast Model Outputs for Endoscopic Carpal Tunnel Release.
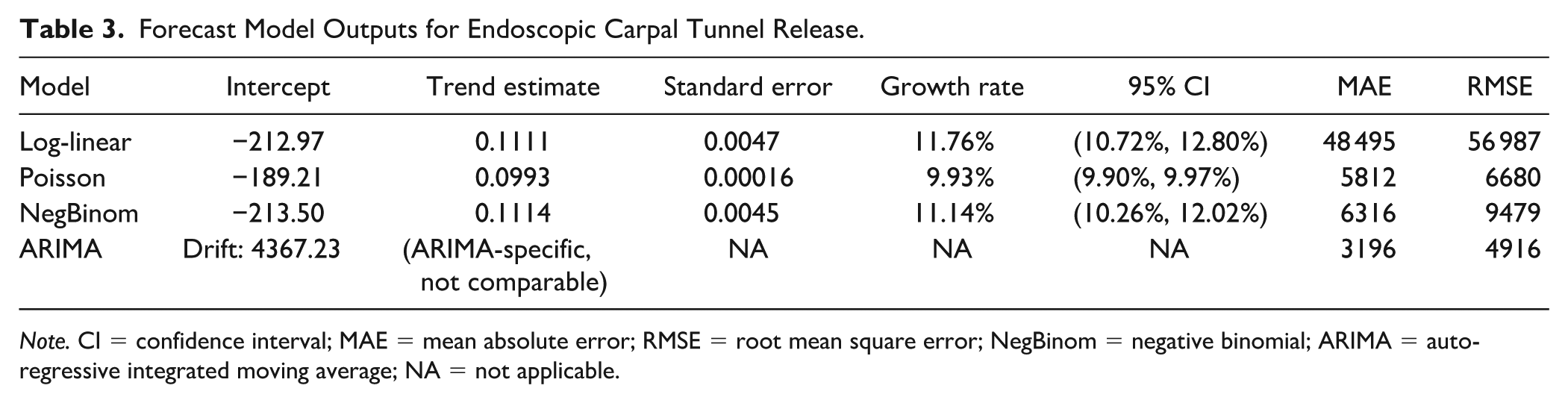
Note. CI = confidence interval; MAE = mean absolute error; RMSE = root mean square error; NegBinom = negative binomial; ARIMA = auto-regressive integrated moving average; NA = not applicable.
Using ARIMA, point forecasts and 95% confidence intervals (CIs) were generated for annual procedure volumes, providing projections for both open and endoscopic CTR procedures from 2023 to 2040. For open CTR, the annual growth rate is projected to average 2.0% from 2023 to 2039, with a slight deceleration to 1.96% in 2040, reflecting the continued dominance but slower growth trajectory of this technique. Endoscopic procedures, on the other hand, are projected to experience a faster annual growth rate, averaging 2.42% by 2040, consistent with increasing adoption in clinical practice. By 2040, the projected annual volume for open procedures is estimated to reach 424 271 (95% CI: 366 977-481 564), representing a 50.3% increase from 2022 volumes. For endoscopic procedures, the annual volume is forecasted to reach 184 723 (95% CI: 141 939-227 507), marking a 74% increase from 2022 levels, further highlighting the accelerating adoption of minimally invasive techniques (Table 4). Graphical representations in Figure 1 visualizes these historical trends and future forecasts, clearly delineating the differences in projected growth trajectories for the 2 techniques.
Projections of Open Versus Endoscopic Carpal Tunnel Release.
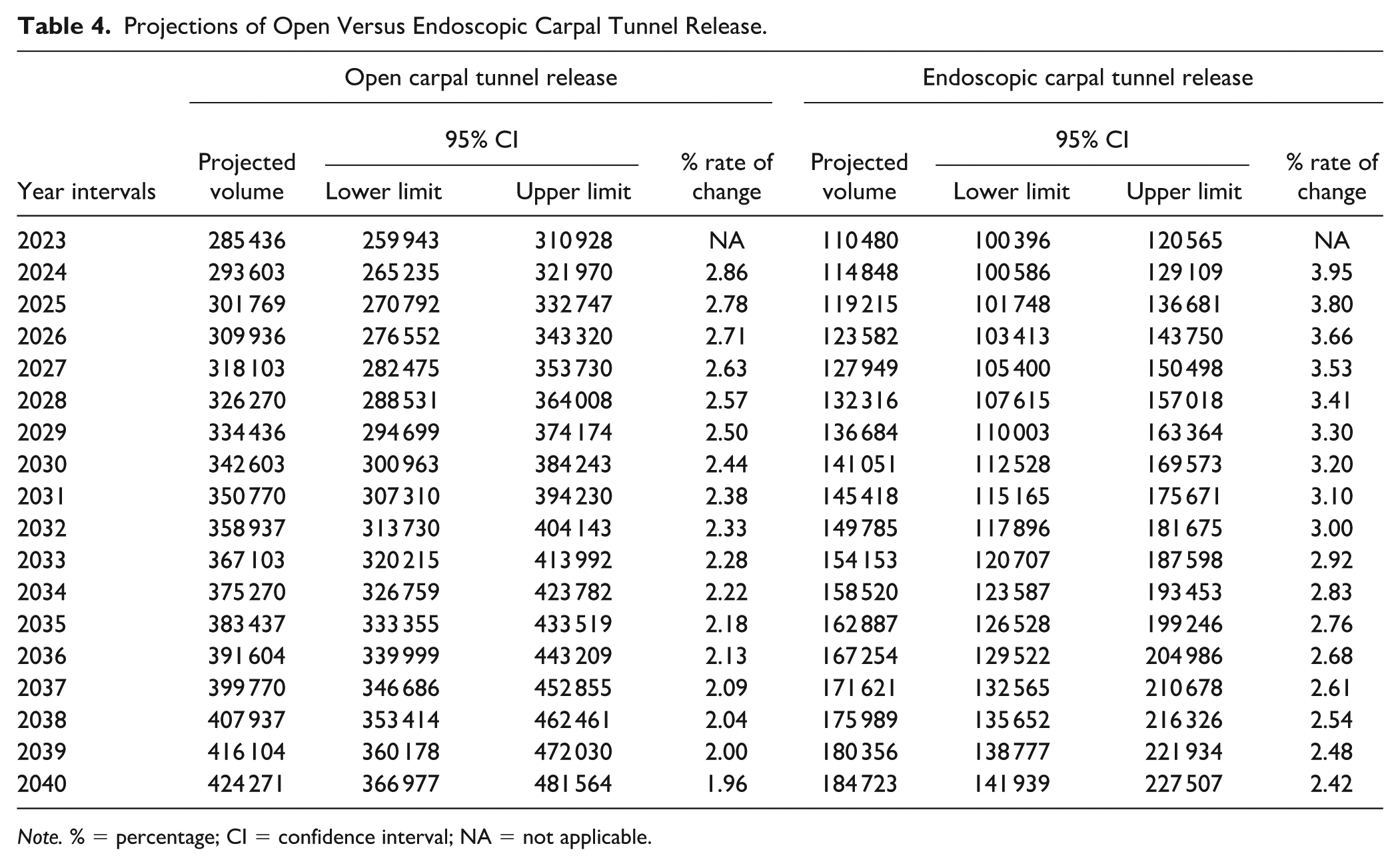
Note. % = percentage; CI = confidence interval; NA = not applicable.
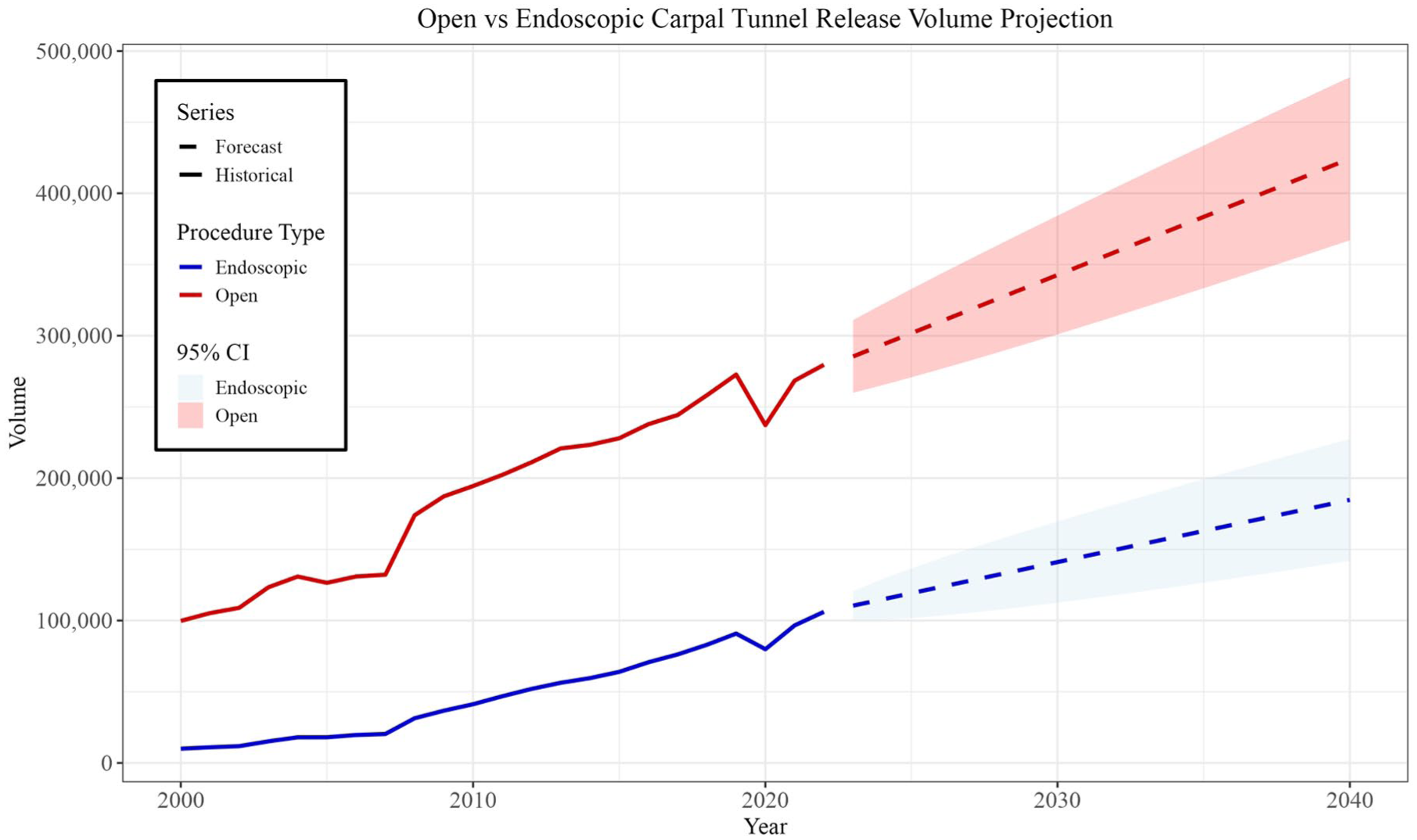
Historical trends and projected volumes for open versus endoscopic carpal tunnel release procedures (2000-2040).
Discussion
Carpal tunnel release remains one of the most commonly performed procedures in hand surgery, with both open and endoscopic techniques widely used. Our findings demonstrate substantial growth in both approaches, with endoscopic CTR expanding at a significantly faster rate. Auto-regressive integrated moving average modeling projects this trend to continue, with open CTR remaining the predominant approach but at a slower growth rate, while endoscopic CTR adoption accelerates. These trends align with prior studies indicating a shift toward minimally invasive techniques, though open CTR remains the primary approach among US Medicare patients.
Prior studies support our findings that the expansion of endoscopic CTR is influenced by demographic and geographic trends. O’Leary et al 18 identified an increase in both open and endoscopic CTR, while Ratnasamy et al 19 highlighted significant predictors of endoscopic CTR selection, including higher utilization in the southern United States, a greater likelihood among female patients, and a preference for endoscopic CTR among those with fewer comorbidities. Insurance status also plays a role, with Medicare beneficiaries being slightly less likely to receive endoscopic CTR compared with privately insured patients. In addition, while endoscopic CTR is associated with higher initial procedural costs, its faster recovery times and reduced postoperative morbidity may offset long-term financial differences. 19 These cost considerations, along with patient preference for minimally invasive approaches, may continue to drive the adoption of endoscopic CTR. However, institutional factors, such as surgeon availability and hospital reimbursement policies, likely contribute to the variability in procedural selection across different health care settings.
Surgeon training is a major factor driving endoscopic CTR adoption. Smetana et al and Bellaire et al20,21 found that hand fellowship-trained surgeons were 4.5 times more likely to perform endoscopic CTR than non-fellowship-trained orthopedists, a trend expected to continue with the expansion of Accreditation Council for Graduate Medical Education (ACGME)-accredited hand surgery programs. Geographic differences also contribute to procedural trends, with Baron et al 22 noting the highest concentration of hand surgeons in the southern United States, correlating with increased endoscopic CTR utilization. The availability of specialized training programs and institutional preferences further shape these trends, as academic centers with high surgical volumes often serve as early adopters of newer techniques. As specialized training increases, endoscopic CTR may become more common, particularly in regions with higher hand surgery expertise, potentially leading to further shifts in surgical practice patterns over time.
Despite the growing adoption of endoscopic CTR, its superiority over open CTR remains nuanced. Meta-analyses by Li et al 23 and Vasiliadis et al 24 indicate that while endoscopic CTR offers early advantages such as faster return to work, reduced postoperative scarring, and improved grip strength in the short term, long-term functional outcomes remain comparable between the 2 techniques. In addition, endoscopic CTR carries a higher risk of iatrogenic complications, including superficial palmar arch injury, transient neurapraxia, and incomplete ligament release, all of which can contribute to postoperative morbidity. 25 These risks, coupled with the higher procedural costs associated with specialized instrumentation, underscore the importance of balancing the potential benefits of endoscopic CTR with its technical demands and complication profile. Given these findings, the choice between open and endoscopic CTR should be based on patient characteristics, surgeon experience, and institutional resources rather than an assumption of inherent superiority. As endoscopic techniques continue to evolve, future studies should focus on refining patient selection criteria and optimizing surgical safety to maximize outcomes.
This study has several limitations. First, our analyses are restricted to Medicare beneficiaries in the United States, and our projections pertain only to this US health care context; therefore, our findings may not generalize to international settings with different health systems, reimbursement structures, or practice patterns. Our projections rely on Medicare Part B data, which, while nationally representative of the Medicare population, may not fully capture utilization trends among younger, privately insured individuals or those covered under Medicaid. In addition, the Medicare Part B National Summary dataset provides aggregated procedure counts rather than patient-level information and therefore does not include clinical outcomes, complications, or patient-reported measures. As a result, we were unable to directly compare outcomes between open and endoscopic CTR in this analysis, and our forecasts should be interpreted as utilization projections rather than statements about comparative effectiveness. Future studies linking procedure volume trends with detailed clinical and functional outcomes would meaningfully complement the present work. Given that private insurance plans often reimburse procedures at different rates and may have different authorization requirements, utilization patterns in non-Medicare populations could differ significantly. In addition, forecasting models are inherently limited by their dependence on historical trends and cannot account for policy shifts, reimbursement changes, or advancements in surgical technology that may influence future CTR utilization.26,27 Sudden disruptions, such as regulatory changes affecting reimbursement for endoscopic procedures or the introduction of novel surgical techniques, could significantly alter the projected trajectory of CTR utilization. In addition, because the Medicare Part B National Summary dataset does not include geographic identifiers, we were unable to examine regional variation in CTR utilization. Detailed assessment of regional differences will require future studies using geographically resolved claims data. Furthermore, large database studies are subject to coding inaccuracies, variability in procedural reporting, and potential misclassification, all of which could affect the precision of our estimates. Despite these limitations, our study provides valuable insights into long-term trends in CTR utilization and highlights the factors that may shape future practice patterns.
Conclusions
Carpal tunnel release utilization has increased substantially over the past 2 decades, with endoscopic techniques demonstrating a faster growth rate than open CTR. Despite this trend, open CTR is projected to remain the predominant approach among Medicare patients through 2040. Our findings highlight the ongoing shift toward minimally invasive techniques while underscoring the continued role of traditional open CTR. Future research should explore the economic impact, patient-reported outcomes, and factors influencing the adoption of each technique. Understanding these dynamics will be essential for optimizing surgical decision-making and resource allocation in the evolving landscape of hand surgery.
Footnotes
Ethical Approval
No institutional review board approval was required for performance of this review.
Statement of Human and Animal Rights
This study did not involve human participants or animal subjects.
Statement of Informed Consent
Informed consent was not required for this study as it did not involve human participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.