
Abstract
Background:
Distal radius fractures are common in adults. Surgical fixation seeks to restore anatomical alignment, but the relationship between radiographic correction and functional recovery remains uncertain.
Methods:
A cross-sectional study of 201 patients treated with distal radius plate fixation at Hospital Universitario de la Samaritana E.S.E. (2014-2018) was conducted. Patients with incomplete records, poor-quality radiographs, or reintervention were excluded. Radiographic parameters assessed preoperatively and postoperatively included radial height, radial shift, ulnar variance, and palmar tilt in extraarticular fractures, and teardrop angle, lunate-lunate facet ratio, and capitate-to-axis-of-radius distance (CARD) in intraarticular fractures. Functional outcomes were measured with the Quick Disabilities of the Arm, Shoulder, and Hand questionnaire, and associations with radiographic indices were analyzed.
Results:
Among patients, 70.1% had extraarticular and 29.8% intraarticular fractures. In extraarticular cases, the combination of radial shift >3 mm, palmar tilt >8°, and radial height >10 mm predicted favorable outcomes. In intraarticular fractures, postoperative CARD >6.4 mm correlated with significantly better functional results.
Discussion:
Radiographs remain essential in distal radius fracture management, but their correlation with function is inconsistent. Radial height and palmar tilt were the most relevant predictors for extraarticular fractures, while CARD was the strongest predictor in intraarticular cases. Notably, higher CARD values, even outside standard ranges, were paradoxically associated with better outcomes, likely reflecting biomechanical adaptations or subgroup-specific tolerance to deformity.
Conclusions:
Complete radiographic restoration was not consistently associated with function. Instead, specific measures—radial height and palmar tilt in extraarticular fractures, and CARD in intraarticular fractures—emerged as key predictors of favorable recovery.
Introduction
Distal radius fractures (DRF) represent one of the most frequent skeletal injuries in adults, second only to hip fractures in prevalence. In older individuals, these fractures typically result from bone fragility, whereas in younger patients, they are more commonly associated with high-energy trauma. 1
Treatment strategies for DRF vary significantly, ranging from conservative orthopedic management to surgical fixation using percutaneous screws or volar locking plates. Over the past two decades, advancements in osteosynthesis materials have led to a notable increase in the use of anatomical volar locking plates, applied through diverse surgical approaches. 2
Historically, 4 radiographic parameters have been used to guide treatment decisions and assess the quality of fracture reduction: radial height (RH), radial inclination, ulnar variance (UV), and palmar tilt. 3 More recently, three additional measurements have been proposed to enhance the assessment of intraarticular fracture alignment: the capitate-to-axis-of-radius distance (CARD), lunate-lunate facet ratio (LLFR), and teardrop angle (TDA).4-6
Despite numerous studies attempting to correlate specific radiographic parameters with favorable functional outcomes, the evidence remains inconclusive. For instance, in a 2007 study, Barton et al 7 analyzed 60 patients treated with closed reduction and percutaneous pinning and identified radial shortening as the most significant predictor of poor functional outcome, as measured by the Patient-Rated Wrist Evaluation (PRWE) score. In contrast, a 2013 study by Beumer et al 8 found that positive UV was the strongest predictor of unsatisfactory postoperative results. Nevertheless, a 2018 systematic review conducted by the British Society for Surgery of the Hand concluded that the existing literature lacks sufficient high-quality evidence to definitively link any single radiographic parameter with functional recovery. 9
Although achieving anatomical alignment has traditionally been considered a key objective of fracture reduction, it remains unclear whether radiographic improvements reliably translate into better functional outcomes. Therefore, the aim of this study was to investigate the relationship between anatomical reduction (as assessed by standard radiographic parameters) and functional recovery, as measured by the Disabilities of the Arm, Shoulder, and Hand (DASH) score.
Methods
Study Design
Cross-sectional study in patients managed with distal radius plate fixation. The scale was administered at the 6-month time point after the treatment, when fracture healing was expected to have occurred.
Population Selection and Data Collection
Patients were enrolled between January 2014 and September 2018. Inclusion criteria were patients over 18 years of age taken to surgical management with distal radius plating, with preoperative radiographs, as well as postoperative radiographs taken 6 months after the treatment. Patients needing reintervention or with poor-quality radiographs or incomplete information for follow-up were excluded. While the exact number of excluded patients was not systematically recorded, review of the available clinical records showed that their demographic and clinical characteristics did not differ substantially from those of the 201 patients included in the final analysis.
Variables
The assessed variables included sociodemographic information, comorbidities, and fracture characteristics (intraarticular/extraarticular). Preoperative and postoperative conditions of the distal radius were assessed, and radiographic measurements were made, taking into consideration RH, radial shift (RS), UV, palmar tilt (PT) in extraarticular fractures, and TDA, LLFR, and CARD measurements in intraarticular fractures. Measurements were made and entered in the database by a single reviewer.
Measurements considered normal or anatomic in intraarticular and extraarticular fractures on the radiographs were assessed at the time of the fracture and after fixation. Measurement ranges are shown in Figure 1.3,10
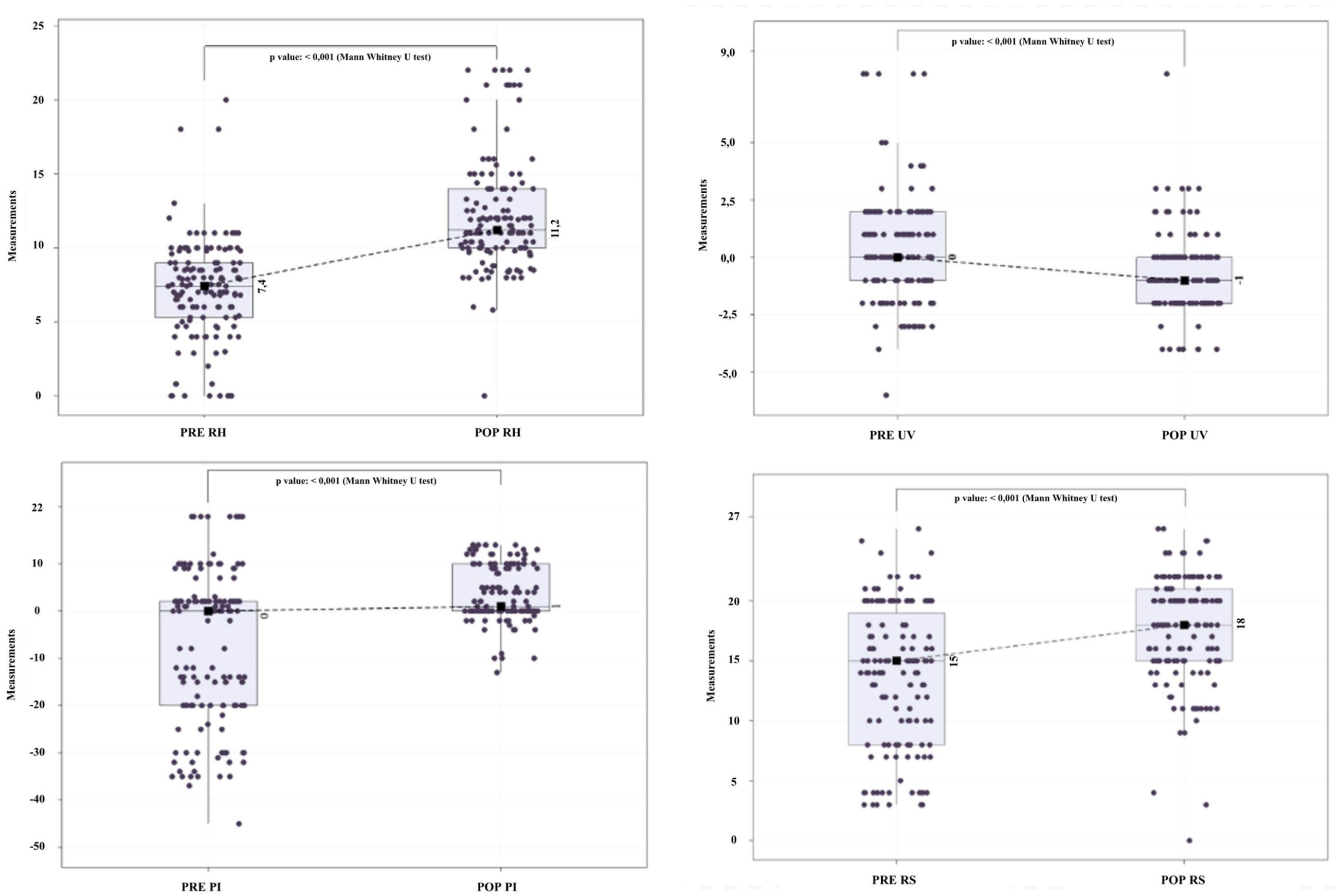
Box-and-whisker plots comparing the distribution of each parameter before and after surgery. Medians are shown as solid lines. The figure highlights that radial height and palmar tilt demonstrated the most pronounced improvements postoperatively, while changes in radial shift and ulnar variance were less marked.
In addition, through a telephone call to each patient, a subjective functional result was obtained by applying the quickDASH survey validated for Colombia.
Biases
Information bias is the main bias associated with this retrospective study, considering that data were derived from the clinical record. The surgical note as well as the surgical description were validated in order to mitigate this risk, and patients with incomplete information in the clinical record were excluded. In addition, patients who required reintervention for loss of radiographic reduction were excluded from the study. This exclusion is acknowledged as a potential source of selection bias.
Sample Size
Sample size was calculated using the finite population formula, with α = 0.05 and power = 0.90. Because reliable prevalence estimates for the primary outcome category (Good/Excellent QuickDASH) were not available a priori, we adopted a conservative assumption of P = .50 (maximum variance) to ensure adequate precision, which yielded a minimum sample size of 169. The final analytic cohort comprised 201 patients, exceeding the target.
Statistical Methods
Data were expressed in medians (25-p75), counts, and proportions. The Z test with binomial approximation was used to compare two independent proportions, and the Chi square test (X2) was used to compare three or more proportions. Normality was rejected using the Shapiro-Wilk test, and the U Mann-Whitney test was used to compare three or more variables or subgroups of numerical variables. A P value less than .05 was considered significant (Minitab® 19.2020.1).
Variables were grouped into the categories of poor, satisfactory, and good/excellent to improve efficiency while exploring “statistical associations” between the explanatory variables (anatomic parameters) and the outcome (Quick Disabilities of the Arm, Shoulder, and Hand [Q-DASH classification). Moreover, decision trees with binary ramifications (95% CI) with no more than 5 levels were made to identify potential cutoff points or thresholds that could enhance the likelihood of identifying patients classified as Q-DASH Good/Excellent (Orange Data Mining & Fruitful, Version 3.27.1).
Radiographic Measurement Protocol and Reliability
All measurements were obtained on standardized PA and lateral radiographs using a predefined protocol with the central reference point described by Medoff to ensure consistent landmarking in the sagittal plane. A single trained reviewer performed all measurements using digital calipers on the hospital’s Picture Archiving and Communication System (PACS) viewer. Inter-observer reliability (ICC, 95% CI) was not determined in this cohort and is acknowledged as a limitation; however, prior studies have reported good-to-excellent reliability for these parameters when standardized protocols are used. We provide the measurement checklist and examples in Supplemental Material.
Statistical Analysis
Continuous variables are summarized as medians (p25-p75) or means (SD) as appropriate; categorical variables as counts (%). In the primary analysis, both QuickDASH and the radiographic parameters (RH, RS, UV, PT, LLFR, CARD, TDA) were treated as continuous. We fitted multivariable linear regression models with QuickDASH as the dependent variable and included demographics (age, sex), fracture pattern (intraarticular: yes/no), and radiographic parameters. We assessed multicollinearity using variance inflation factors (VIF) and report semi-partial R² to quantify the unique variance explained by each significant predictor. As an exploratory analysis, we retained prior decision-tree cutoffs in the Supplemental Material for hypothesis generation only.
We also performed a sensitivity analysis with postoperative therapy exposure (supervised, home-based, none), using indicator variables. Two-sided P < 0.
Results
During the study period, a total of 201 patients underwent surgical management for DRF, of which 70.1% were extraarticular, and 29.8% intraarticular. Most patients were in their fifth decade of life and predominantly right-handed. Extraarticular fractures were more commonly observed in male patients, whereas intraarticular fractures were more frequently diagnosed in females.
Among patients aged 65 years and older, osteoporosis was the most common comorbidity associated with both fracture types, followed by a history of prior surgeries related to multiple traumas.
Overall, 34.3% of cases were related to polytrauma. In addition, 25% of patients presented with concurrent fractures at other anatomical sites, 20% had a stable fracture pattern, and approximately two-thirds of the cohort completed a full postoperative physical therapy program.
Comparisons Between Anatomical Parameters Before and After Surgical Management
Extraarticular and intraarticular anatomical parameters are expressed in medians (quartiles, p25-p75) and displayed in box and whisker diagrams given that normality was rejected with the Shapiro Wilk test at both time periods (before and after surgery) (Table 1).
Statistics of Anatomical Parameters Measured Before and After Surgery for Intraarticular or Extraarticular Distal Radius Fractures.
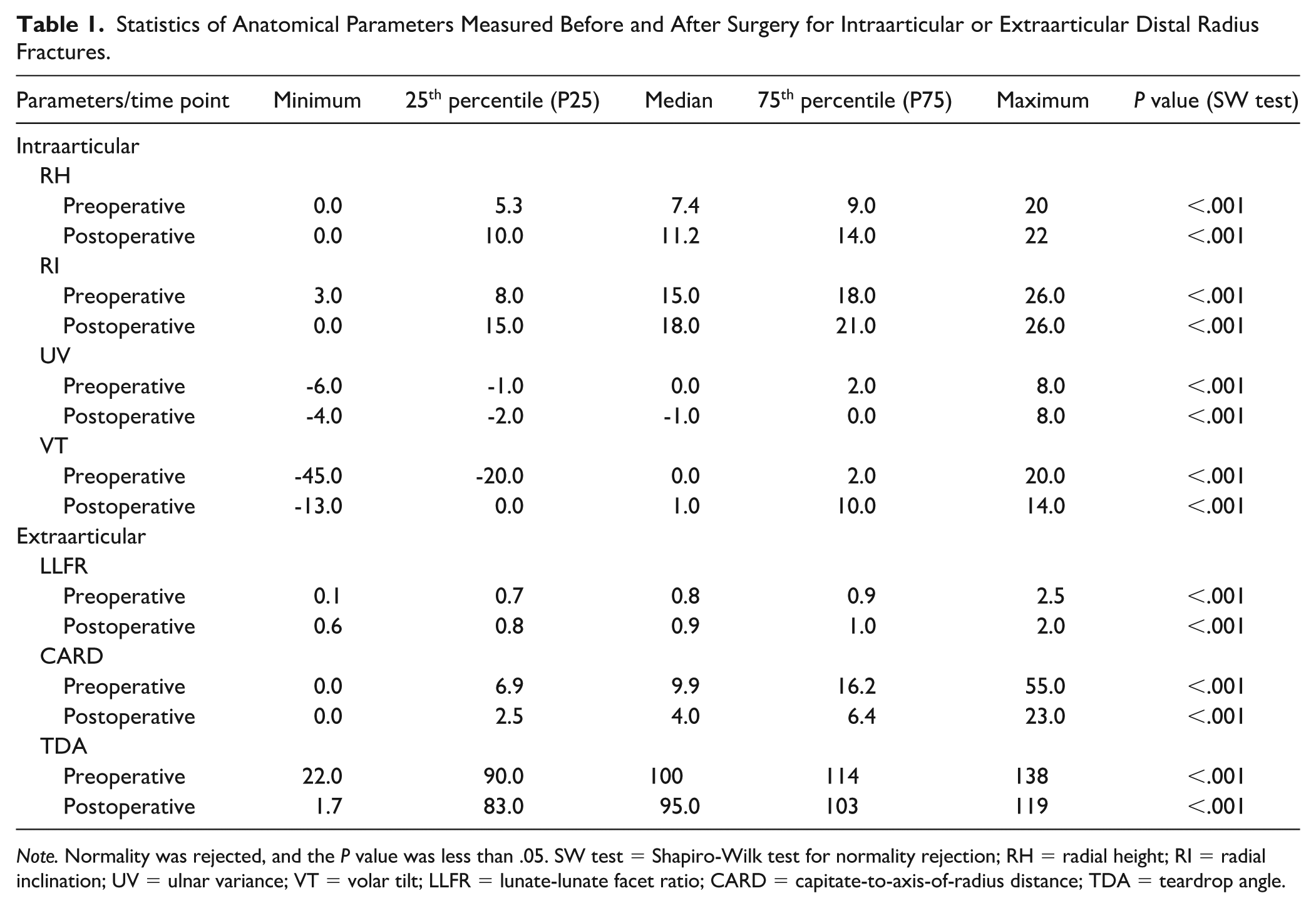
Note. Normality was rejected, and the P value was less than .05. SW test = Shapiro-Wilk test for normality rejection; RH = radial height; RI = radial inclination; UV = ulnar variance; VT = volar tilt; LLFR = lunate-lunate facet ratio; CARD = capitate-to-axis-of-radius distance; TDA = teardrop angle.
Extraarticular DRF
When comparing the anatomical parameters recorded preoperatively and postoperatively for each patient, a notably greater change was observed in RH and PT measurements, compared to the changes documented for RS and UV.
Statistical differences were found for each of the medians before and after the surgical procedure (Figure 1). However, the main effects were found for RH and RS.
Intraarticular DRF
In patients with intraarticular fractures, notable changes were observed in three of the anatomical parameters following surgical intervention, with the most pronounced differences seen in the LLFR and CARD.
Similarly, in the intraarticular fracture group, statistically significant differences were identified in the median values of all parameters before and after surgery (Figure 2); however, the most substantial changes were again observed in CARD and LLFR.
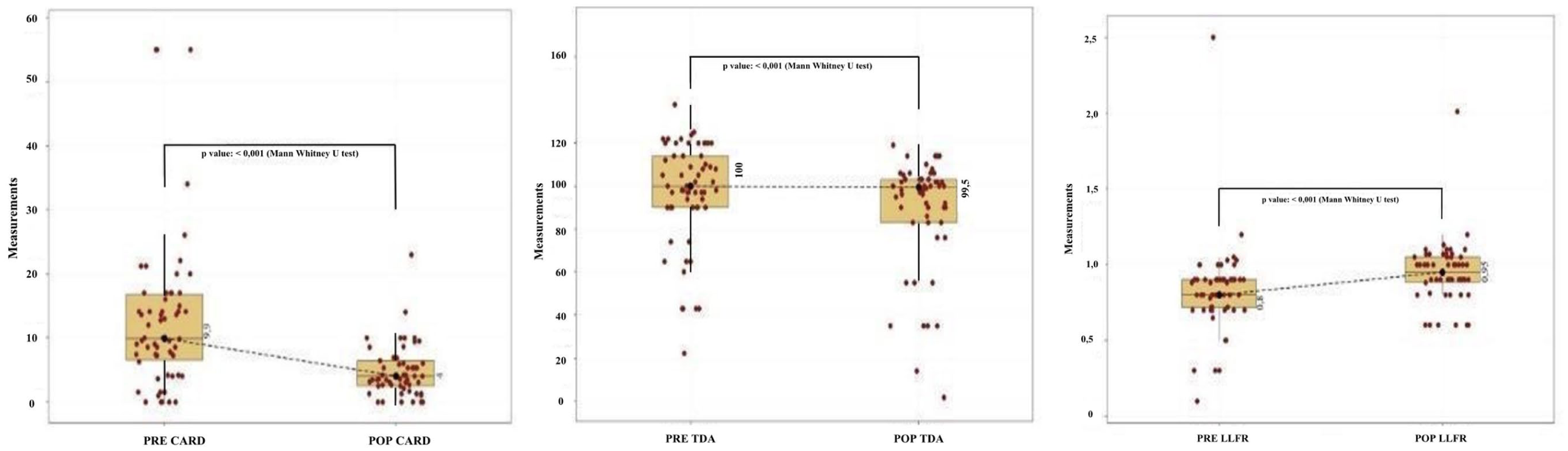
Box-and-whisker plots showing distributions of teardrop angle (TDA), lunate-lunate facet ratio (LLFR), and capitate-to-axis-of-radius distance (CARD) preoperatively and postoperatively. Medians are marked with solid lines. The plots demonstrate significant improvements in LLFR and CARD after fixation, while changes in TDA were less pronounced.
Statistical differences were identified for RH, RS, and UV measured in extraarticular DRF when comparing the frequency of patients with changes in standard anatomical parameters. Moreover, statistical differences were found for LLFR and CARD, measured in intraarticular DRF (Table 2).
Radiological Parameters Within the Standard Anatomical Range Before (Preoperative) and After (Postoperative) Surgical Management.
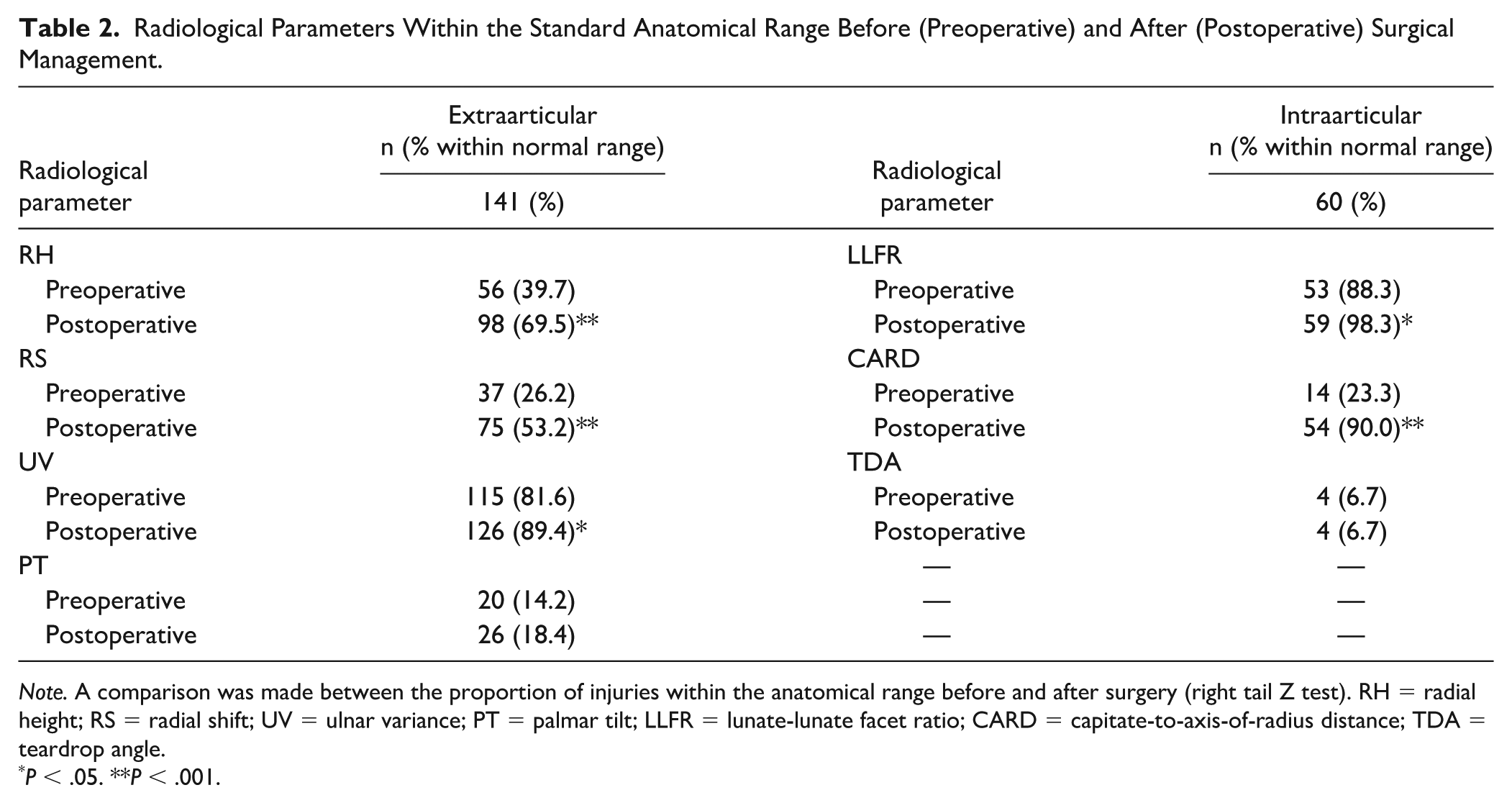
Note. A comparison was made between the proportion of injuries within the anatomical range before and after surgery (right tail Z test). RH = radial height; RS = radial shift; UV = ulnar variance; PT = palmar tilt; LLFR = lunate-lunate facet ratio; CARD = capitate-to-axis-of-radius distance; TDA = teardrop angle.
P < .05. **P < .001.
Anatomical Parameters of DRF Associated With Q-DASH Categories
Among the 201 patients included in the study, 50.7% (102/201) achieved an Excellent outcome according to the Q-DASH score, followed by Satisfactory in 25.8% (52/201), Good in 11.9% (24/201), and Poor in 11.4% (23/201). No statistically significant differences were observed in the distribution of these outcome categories between patients with extraarticular and intraarticular fractures (χ² = 1.263, P = .738).
Furthermore, no significant associations were found between the median values of any anatomical parameters—whether intraarticular or extraarticular—and the four Q-DASH outcome categories (Table 3). Likewise, no statistically significant relationship was observed between achieving a Good/Excellent Q-DASH outcome and having postoperative anatomical parameters within the standard reference range (“in-range”), for either fracture type.
Relationships Between Medians of Postoperative Anatomical Parameters and Q-DASH Category of Distal Radius Fractures.
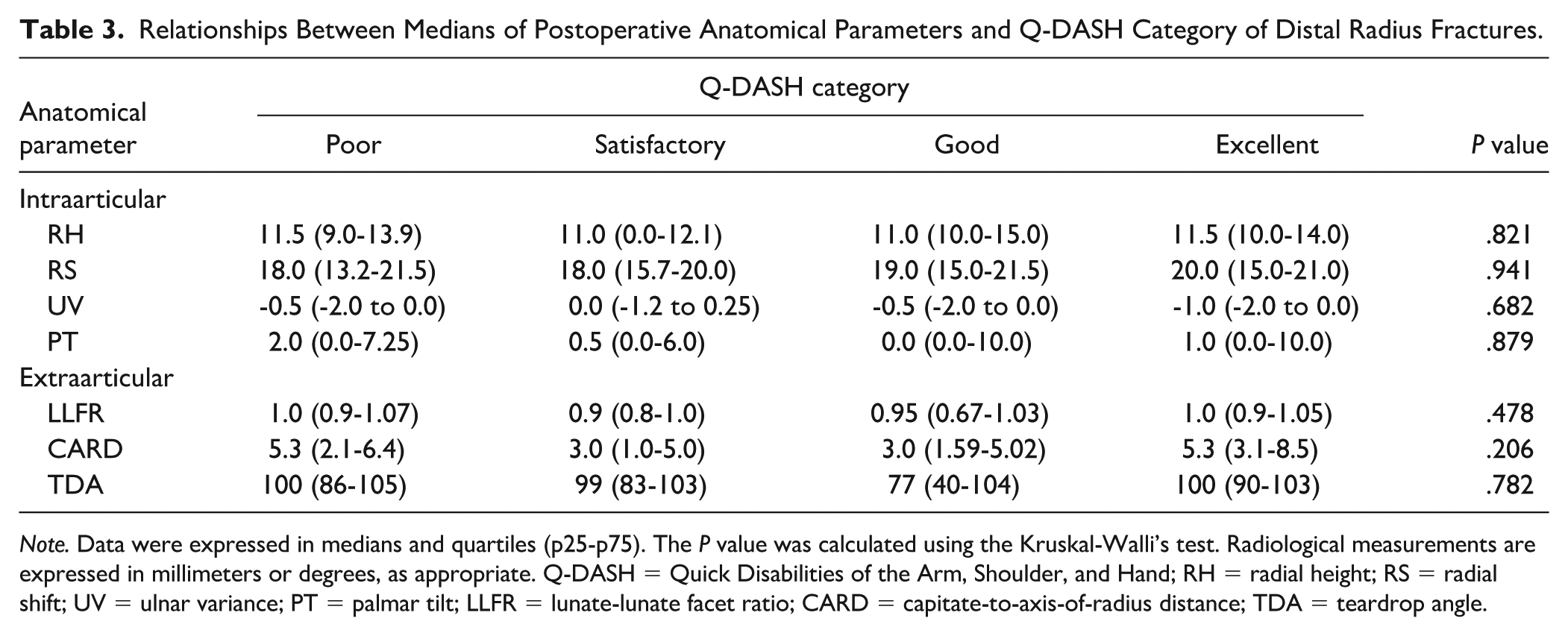
Note. Data were expressed in medians and quartiles (p25-p75). The P value was calculated using the Kruskal-Walli’s test. Radiological measurements are expressed in millimeters or degrees, as appropriate. Q-DASH = Quick Disabilities of the Arm, Shoulder, and Hand; RH = radial height; RS = radial shift; UV = ulnar variance; PT = palmar tilt; LLFR = lunate-lunate facet ratio; CARD = capitate-to-axis-of-radius distance; TDA = teardrop angle.
Given the lack of statistical association between the medians of postoperative anatomical parameters of DRF and the Q-DASH categories with the finding described previously of favorable anatomical changes in the medians of all the measured parameters, our thinking was that “some subcategories consisting of intervals or cutoff points of intraarticular or extraarticular anatomical parameters” might increase the likelihood of identifying patients who could be classified Q-DASH Good/Excellent (composite outcome) versus Q-DASH Satisfactory/Poor (composite outcome).
To explore potential predictors of favorable functional outcomes, two hypotheses were evaluated:
Whether postoperative anatomical parameters within standard reference ranges for intraarticular and extraarticular DRF were associated with a higher probability of classification in the Good/Excellent Q-DASH category.
Whether alternative cutoff points for these parameters could better discriminate patients with favorable Q-DASH outcomes.
Among patients with extraarticular DRF, 64.5% were classified as Good/Excellent. Interestingly, statistical analysis showed that patients with postoperative anatomical parameters outside the standard range were more likely to be classified in the Good/Excellent category, contrary to traditional assumptions.
In patients with intraarticular fractures, 58.3% achieved Good/Excellent outcomes. However, no consistent association was found between the standard ranges of anatomical parameters and functional recovery. The only notable finding was for the CARD: patients with a postoperative CARD value greater than 6.4 mm had a 75% likelihood of being classified as Good/Excellent on the Q-DASH.
This association was statistically significant (P = .032), with an odds ratio of 5.14 (95% CI, 1.12-37.3), suggesting that a CARD value above 6.4 mm may serve as a potential predictor of favorable functional outcomes in intraarticular DRF.
Discussion
Radiographic measurements are a fundamental tool in the management of DRF, as they provide valuable information on initial alignment, fracture healing, and implant positioning following treatment. The traditional parameters used to assess outcomes include RH (12.3 mm), radial inclination (22°), volar tilt (11°), and UV (0.4 mm), obtained from posteroanterior and lateral views with the forearm in a neutral position.11,12 Several authors have proposed criteria to define malunion, such as radial inclination <10°, volar tilt >20° or dorsal tilt >20°, RH <10 mm, UV >2 mm, or intraarticular gap >2 mm. While these parameters serve as a useful guide for therapeutic decision-making, multiple studies have shown that radiographic indices do not always correlate with functional outcomes, particularly in elderly patients. 13 Therefore, radiographs should be regarded as complementary to clinical measures such as pain and Patient-Reported Outcome Measures, but not as primary endpoints. 14
This study highlights the complex relationship between radiographic parameters and functional outcomes after surgical management of DRF. Although no consistent direct correlation was observed between conventional radiographic measurements and postoperative function, multivariate analysis highlighted specific anatomical parameters with predictive value for favorable functional recovery. In extraarticular fractures, restoration of RH and PT was associated with better outcomes, reinforcing prior findings that emphasize the importance of anatomical alignment in this fracture subtype. For intraarticular fractures, the CARD emerged as a more reliable predictor, suggesting that parameters reflecting carpal alignment and congruency may be critical for functional restoration in more complex injuries.
Importantly, the combination of RS (>3 mm), PT (>8°), and RH (>10 mm) may serve as a composite radiographic criterion for anticipating good postoperative results in extraarticular fractures. This multidimensional approach to radiographic assessment could guide surgeons in intraoperative decision-making and postoperative evaluation, potentially optimizing patient counseling and rehabilitation planning. For intraarticular fractures, a postoperative CARD value greater than 6.4 mm may be clinically useful for prognosis and could be incorporated into routine radiographic assessments to better predict functional outcomes measured with the QuickDASH.
An unexpected and somewhat counterintuitive finding was that patients with reductions outside conventional parameters, or with higher CARD values, achieved better functional outcomes. This paradox may reflect biomechanical adaptations in carpal alignment or differences in the tolerance to residual deformity across distinct patient subgroups, consistent with the bimodal distribution of DRF. Younger patients sustaining high-energy trauma may require stricter anatomical correction, whereas older patients with fragility fractures may attain satisfactory function despite deviations from standard radiographic norms.
Finally, modeling predictors as continuous variables reduced information loss and provided a more nuanced interpretation across the observed spectrum, avoiding the pitfalls of arbitrary thresholds. The counterintuitive association between higher CARD values and better outcomes persisted after adjustment in selected models. This paradox likely reflects carpal alignment adaptations and subgroup-specific differences. Future research should prospectively stratify patients by age and injury mechanism, while employing standardized Medoff referencing and reliability testing, to better define the role of carpal alignment metrics in DRF recovery.
Conclusion
This study found no consistent association between overall radiographic restoration and functional recovery following distal radius fixation. Nevertheless, specific parameters showed predictive value: RH and PT in extraarticular fractures and CARD in intraarticular fractures. These findings suggest that rather than relying on conventional “in-range” thresholds, emphasis should be placed on targeted parameters most relevant to fracture type. Future prospective studies, with stratification by age, fracture mechanism, and rehabilitation strategies, are needed to validate these predictors and refine clinical decision-making.
Limitations and Future Directions
This study’s restriction to patients treated exclusively with internal plate fixation limits the generalizability of these findings across other fixation methods such as external fixation or percutaneous pinning. Moreover, the absence of subgroup analyses considering patient-specific factors like osteoporosis, comorbidities, and fracture severity leaves open questions regarding the interplay of these variables with radiographic predictors.
Future prospective studies should incorporate diverse fixation techniques and stratify patients by bone quality and comorbid conditions to refine predictive models further. In addition, integration of advanced imaging modalities and functional outcome metrics, including patient-reported outcome measures beyond the QuickDASH, may provide a more comprehensive understanding of recovery trajectories.
Recommendation
Based on the study, postoperative radiographic assessment of height and tilt for extraarticular fractures and of CARD for intraarticular fractures is recommended as best radiographic predictors for satisfactory clinical outcomes.
Footnotes
Ethical Approval
According to Article 11 of Resolution 8430 of 1993, this study was classified as minimal risk, as it involved the review of medical records, interviews, and questionnaires that did not include or observe sensitive aspects of behavior. The Ethics Review Committee at Hospital Universitario de la Samaritana E.S.E. approved our interviews (approval: CIE-1010-14).
Statement of Human and Animal Rights
All procedures performed in this study involving human participants were conducted in accordance with institutional and national research committee ethical standards, as well as with the 1964 Declaration of Helsinki and its later amendments. This study did not involve animal subjects.
Statement of Informed Consent
Written informed consent was obtained from all participants before the interviews and data collection procedures. Including a detailed explanation of the study objectives, voluntary nature of participation, confidentiality of the information provided, and the right to withdraw at any time without consequences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.