
Abstract
Introduction
Hand surgical procedures can be performed under local anesthesia (LA) due to the hand’s detailed sensory innervation and compact functional anatomy. However, the use of an upper-arm tourniquet, which conscious patients tolerate only briefly, traditionally limited longer and more complex surgeries to general or plexus anesthesia.
Wide Awake Local Anesthesia No Tourniquet (WALANT) has emerged as a paradigm shift, offering an alternative to LA with tourniquet, plexus, or general anesthesia. Provided that contraindications like Raynaud’s or severe vascular diseases are considered, the safety of WALANT anesthesia has been proven in large patient cohorts.1 -6
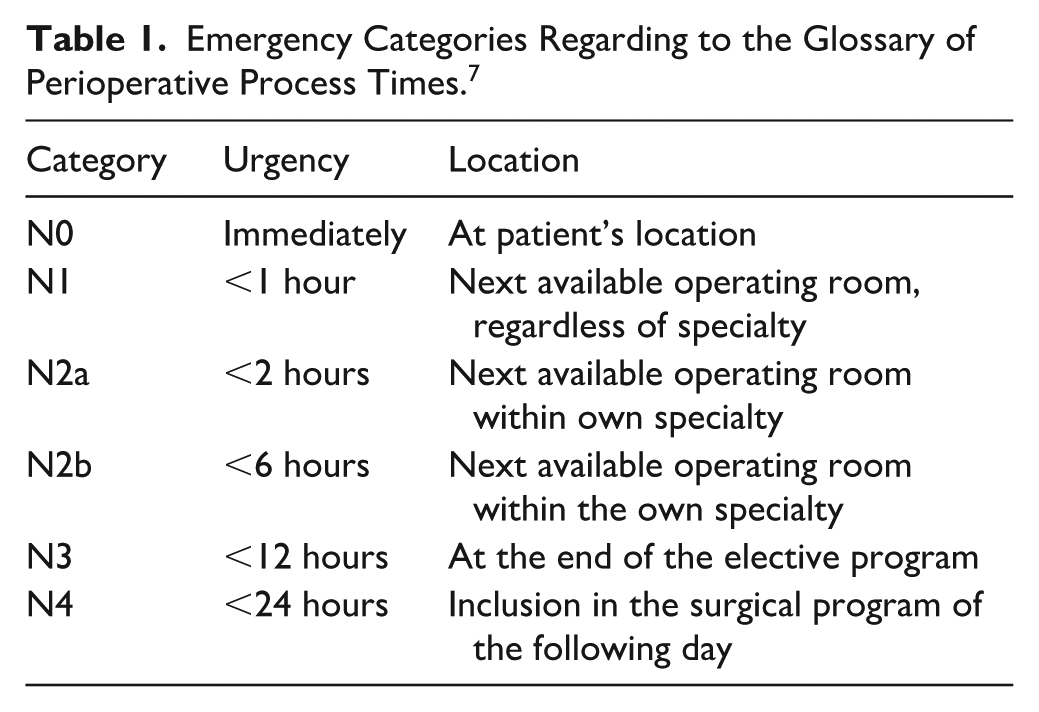
Emergency surgical interventions are categorized into 4 urgency levels, which are comparable to the new timing in acute care surgery (new TACS) classification (Table 1).7,8 Hand injuries with preserved blood flow, such as nerve/tendon injuries, open fractures, and infections, fall into category 2b. Studies suggest these procedures can be performed with equivalent quality under LA, eliminating the need for anesthesia personnel and associated resources.
Emergency Categories Regarding to the Glossary of Perioperative Process Times. 7
This single-center retrospective study investigates emergency category 2b hand surgeries, focusing on the time from operation notification to start and postoperative surgical complications. We compared surgeries performed without anesthesia personnel (LA, including WALANT) to those with anesthesia personnel, focusing on the time from operation notification to start and postoperative surgical complications. This research aims to assess WALANT’s efficacy in emergency care, potentially improving treatment processes and resource utilization. The study will provide data on time efficacy and safety of WALANT in emergency hand surgery, complementing existing data on elective procedures and providing insights into the use of WALANT in time-sensitive situations.
Methods
Study Population
This single-center, retrospective study was conducted at the Department of Plastic and Hand Surgery, University of Freiburg, Germany. The initial dataset comprised all hand surgery emergencies classified as N2b, treated in the Central Operating Theater between January 1, 2018, and March 9, 2024, resulting in 1316 cases. This list was generated from the surgical planning program based on emergency categorization N2b. Exclusion criteria, identified using diagnosis codes, were applied to refine the study population (Figure 1).
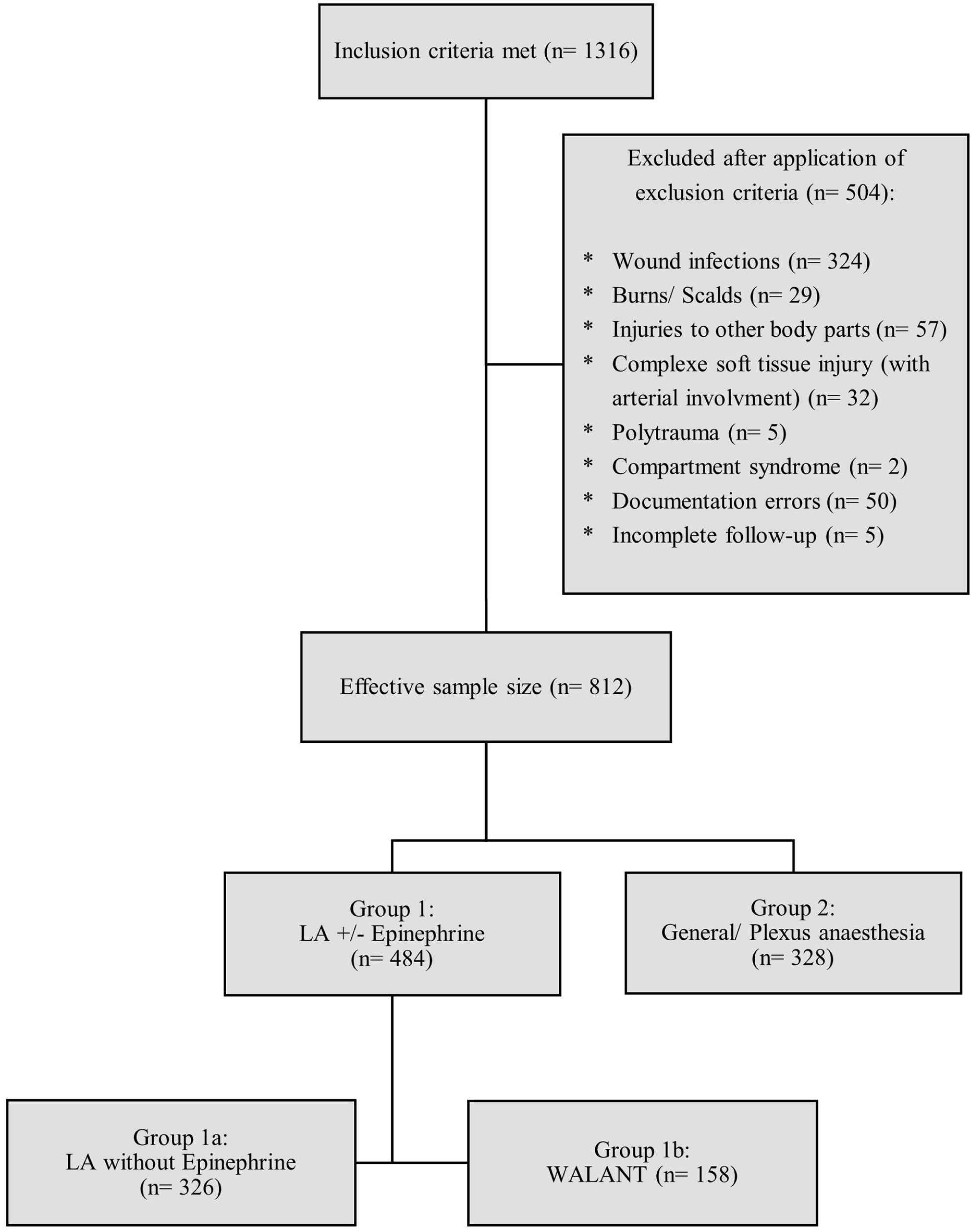
Dropout chart with sample numbers.
Absolute contraindications for LA in hand surgery included patient refusal, lack of cooperation, and allergy to local anesthetics. A manifest Raynaud’s syndrome was considered a contraindication for WALANT. For this study, several relative contraindications were defined as exclusion criteria. Active infectious processes were excluded due to potential reduction in local anesthetic efficacy. 9 Polytrauma requiring multidisciplinary management were excluded, as these cases necessitate general or plexus anesthesia. Severe forearm injuries with arterial involvement were also excluded due to existing ischemia and reflex vasoconstriction. Incomplete follow-up and compartment syndromes were also excluded. After applying all exclusion criteria, the final study population consisted of 812 cases.
Data Collection
The following epidemiological data were collected: gender, age, treatment modality (inpatient/outpatient), diagnosis, procedure, anesthesia type, comorbidities, smoking status, compliance, perioperative and postoperative antibiotic administration, postoperative surgical complications, and operative times. Poor compliance was defined by the recording of noncompliance, such as “patient is not wearing the splint,” in the postoperative documentation. To ensure comparability of procedures, they were categorized into the following therapeutic subgroups, shown in Table 2. Anesthesia type was classified as LA without epinephrine (group 1a), LA with epinephrine (WALANT, group 1b), and general/plexus anesthesia (group 2). In group 1a, a finger tourniquet was typically used. The method used was based on the surgeon’s preference, and the operations were performed by multiple surgeons. The considered comorbidities are listed in Table 2.
Study Population.
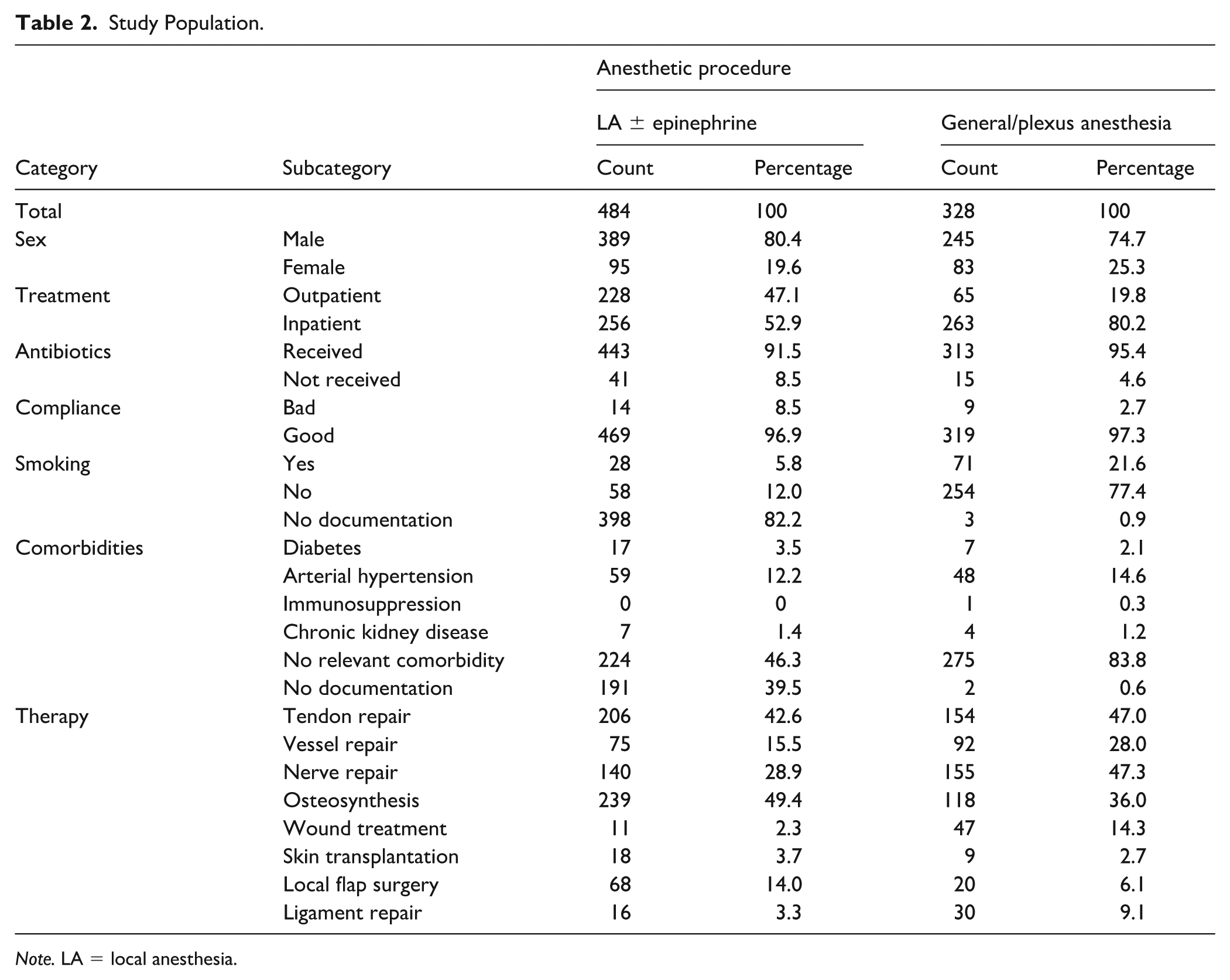
Note. LA = local anesthesia.
Predefined categories of postoperative complications included wound-healing disorders, infection, sensory disturbances, neuroma, excessive scarring, limited mobility, insufficient soft-tissue coverage, tendon suture insufficiency, secondary dislocation, pseudoarthrosis, and complex regional pain syndrome (CRPS), no complications and incomplete follow-up. Incomplete follow-up was recorded if a patient failed to attend any of the scheduled appointments. Multiple complications could be assigned. Each documented complication was classified as either major (requiring surgical revision) or minor (treated conservatively) based on the Clavien-Dindo classification of postoperative surgical complications. 10 Follow-up was typically 2 weeks and 3 months after surgery.
The following time parameters were recorded:
Operation registration, which means the entry of the operation into the system
Initiation of surgical procedure
Skin incision
Final skin suture
From these, “time to intervention” (difference between “Initiation of surgical procedure” and “Operation registration”) and “operative time” (difference between “Suture” and “Skin incision”) were calculated.
Data Sources and Software
Epidemiological data were extracted from electronically stored documents within Meona (Meona GmbH, Freiburg im Breisgau, Germany) and Prometheus (Prometheus Medical Management GmbH, Bad Wörishofen, Germany). The radiological image archive DeepUnity (Dedalus Healthcare System Groups, Milan, Italy) was utilized for the assessment of complications. Statistical analysis was performed using Excel 2409 (Microsoft, Redmond, Washington) and SPSS 29.0.2.0 (IBM, Armonk, New York).
Statistical Analysis
The confirmatory part of the analysis focused on the “time to intervention” and the relevant risk difference in postoperative surgical complication rates between group 1 and 2. A relevant risk difference was defined a priori as greater than 5% after consulting with the statistical and biomedical institute. Both parameters were tested using a sequential testing procedure at a multiple significance level of 0.05. Initially, “time to intervention” was tested for statistical significance. The difference was statistically significant; therefore, postoperative surgical complication rates were evaluated inferentially. This approach was chosen to test the hypothesis that using local anesthetics, compared to surgery with general anesthesia, leads to earlier care while maintaining quality.
In the first step, the equality of mean log-transformed “time to intervention” between the 2 groups was assessed using a 2-sided independent t-test at a significance level of 0.05. Because comparator groups had different sample sizes, Cohen’s d effect size was used. The difference in postoperative complication rates between the 2 groups was calculated using Gart and Nam’s continuity-corrected method. 11
In addition, a descriptive analysis of the study population was conducted. Consequently, no significance testing could be performed in this section. Data on the study population were presented as absolute and relative frequencies. Metric variables were reported as means and standard deviations. A matched-pair analysis was performed to ensure comparability between group 1a, 1b, and 2 regarding performed procedures. Matching variables were the therapeutic subgroups. A 1:1 match was performed without matching tolerance (“inexactness”) and with random case order during matching.
Ethics and Study Registration
The study received ethical approval from the local ethics committee (24-1229). The trial was registered in the University of Freiburg Clinical Trials Register under the number FRKS005233.
Results
Table 2 presents a comparative overview of the study population, detailing key characteristics with both absolute and relative frequencies (percentages) based on the total number of cases within each group.
Time to Intervention
The mean “time to intervention” was 2.21 ± 2.15 hours in group 1 and 4.09 ± 2.8 hours in group 2. This resulted in an absolute mean difference of 1.88 hours (P < .001), indicating a statistically significant reduction of approximately 46%. The data were initially transformed by taking the natural logarithm to generate a more homogeneous distribution with fewer extreme outliers (Figure 2).
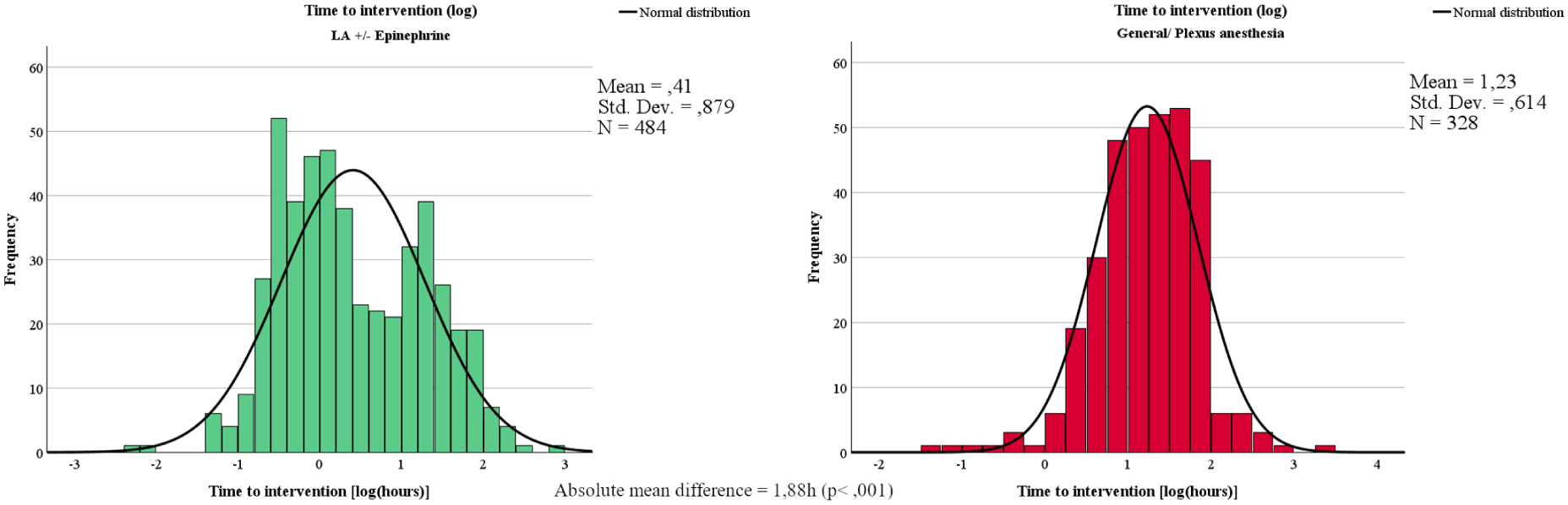
Histogram: distribution of the log-transformed “time to intervention” [hours] in the LA with/without epinephrine group (green, left) and the plexus/general anesthesia group (red, right).
The effect size, calculated at 0.77, signifies a medium to large effect according to Cohen’s original conventions and thus has a significant practical relevance. 12
Surgical Complication Rates
As a significant difference in “time to intervention” was demonstrated between the 2 groups, the complication rate was also evaluated inferentially at a significance level of 0.05, according to the principles of sequential testing. The complication rate was 8.5% in group 1 and 8.2% in group 2, resulting in a risk difference of approximately 0.24% (Table 3).
Overview of Complication Rates by Groups and Subgroups.
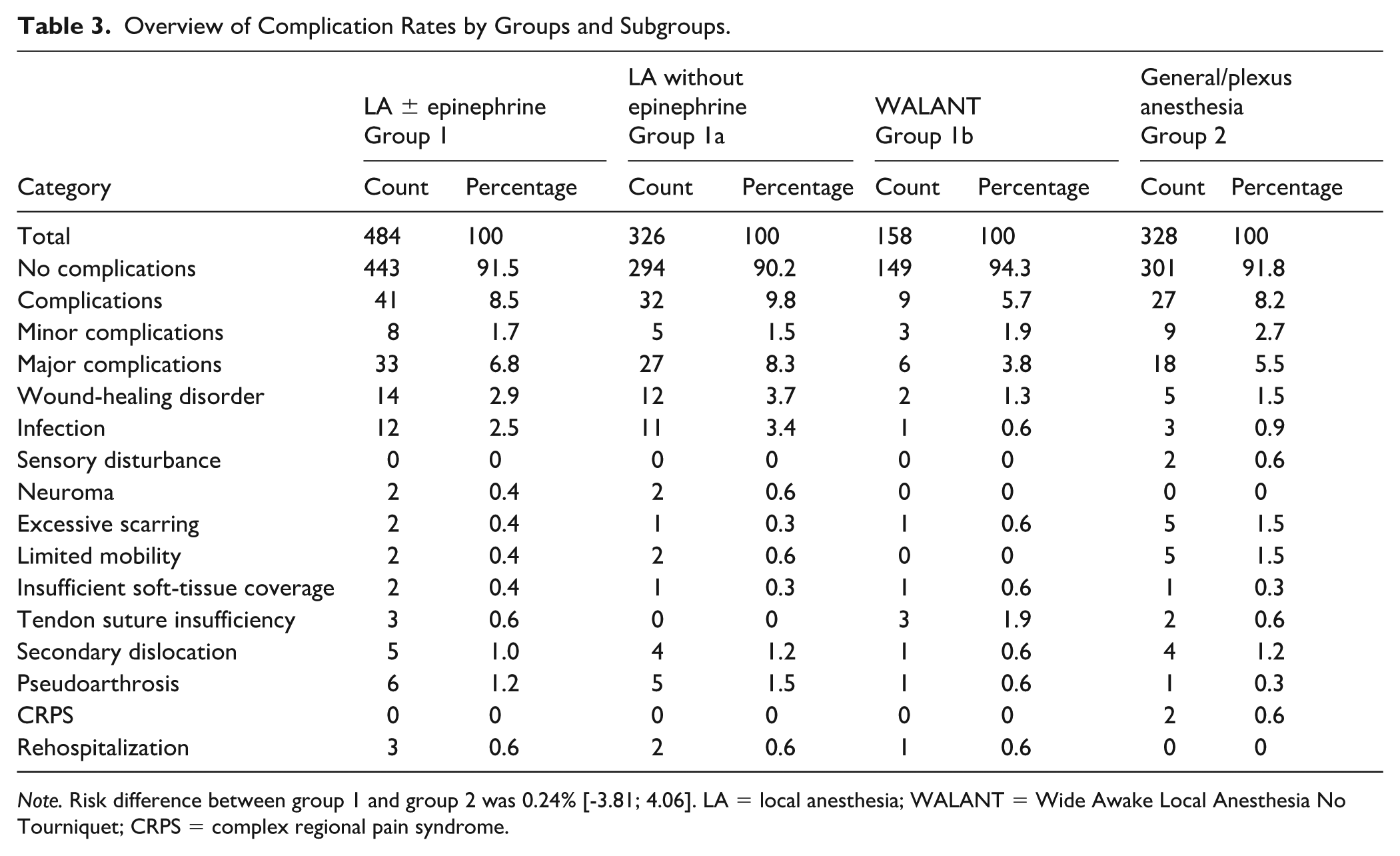
Note. Risk difference between group 1 and group 2 was 0.24% [-3.81; 4.06]. LA = local anesthesia; WALANT = Wide Awake Local Anesthesia No Tourniquet; CRPS = complex regional pain syndrome.
A 95% confidence interval, using Gart and Nam’s method, considering sample sizes (484 in group 1, 328 in group 2) and complication cases (41 in group 1, 27 in group 2), showed no significant difference, as the interval (-3.81 to 4.06) fell within the −5% to +5% equivalence limits. 11
Complications Within Subgroups
The LA group (group 1) was further subdivided into those without epinephrine (group 1a) and with epinephrine (group 1b) to assess a potential negative impact of epinephrine on complication rates and types.
Severity of complications were divided into major complications, which required surgical revision, and minor complications, which were managed conservatively. Table 3 shows that major complications occurred in 3.8% and 5.5% of cases in group 1b and 2, respectively, compared to 8.3% in group 1a and specific complications separately for the subgroups. This was done as post-hoc analysis; therefore, no P-values are given.
Analysis of Injury Complexity and Matched-Pair Analysis
Injury complexity, potentially biasing results, was addressed via matched-pair analysis. Hypothesizing group 2’s rates were more complexity-influenced, matching was done using therapeutic procedures, as complexity proxies. Statistically, a 1:1 matching procedure without tolerance (“inexactness”) regarding the matching variable was performed. For example, individuals with nerve and tendon repair in group 1 were matched to individuals with nerve and tendon repair in group 2.
Each matched group had 229 cases. Group 1’s complication rate decreased from 8.5% to 7.0% (0.9% minor, 6.1% major), group 2’s increased from 8.2% to 10.5% (3.5% minor, 7.0% major). In both groups, the ratio of major to minor complications remained largely unchanged. Table 4 confirmed balanced characteristics and 100% therapy variable agreement.
Study Population After Case-Control Matching.
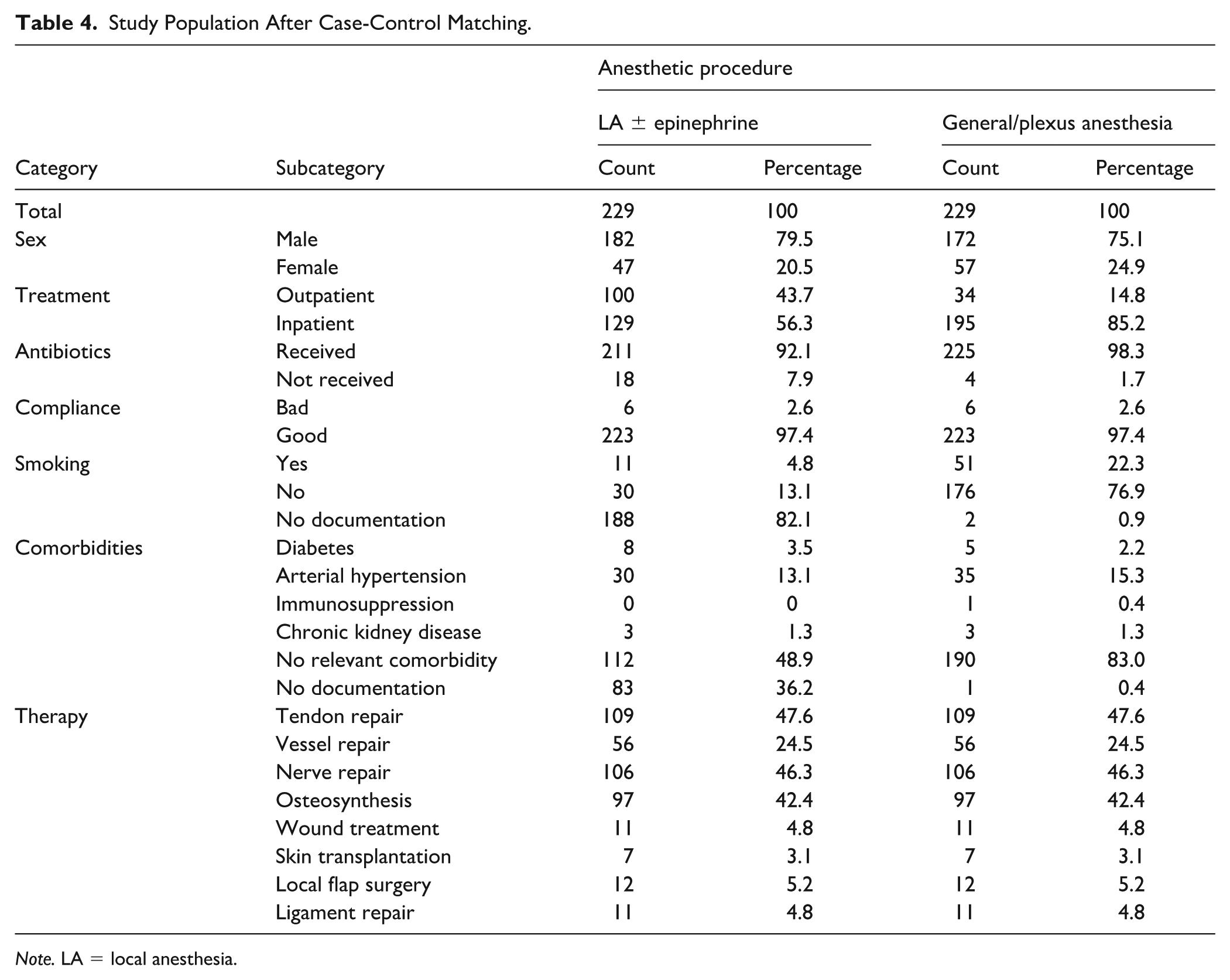
Note. LA = local anesthesia.
Time Management
This study focused on the operative management of hand injuries classified as urgency category N2b. These are emergencies that, according to national recommendations, 7 should be treated within 6 hours. The analysis aimed to assess whether the recommended standards were met. Group 2 had 16.2% of patients treated beyond 6 hours, and group 1 had 6.6% (Figure 3), indicating a time management difference.
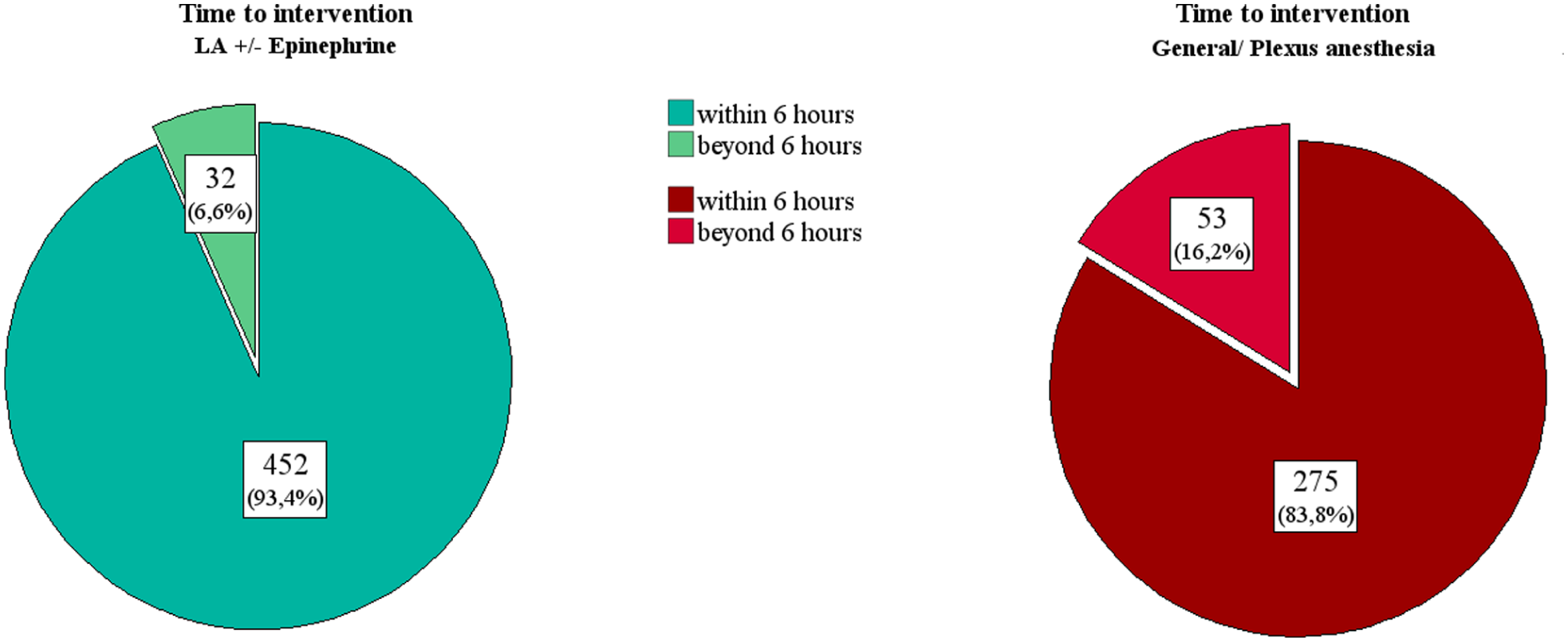
Time to intervention.
Discussion
WALANT use in hand surgery has risen significantly, driven by the low risk rate of acral necrosis and proven superior pain control compared to other anesthesia methods.1,5,6,13 -15 Its cost-effectiveness and high patient satisfaction are well-documented.16 -18 However, research largely focuses on elective cases, neglecting time management in emergencies. This study addresses this gap by investigating “time to intervention” and complication rates in acute hand surgery, focusing on urgency category 2b injuries, which are suitable for both local and general anesthesia. The study’s strengths include its emergency focus, large sample size, and sequential testing, overcoming limitations of prior studies with heterogeneous methodologies and small samples. 18 The limitations of this study primarily stem from its retrospective nature. This inherent characteristic introduces several challenges, including the risk of bias, difficulties in determining causality, and a reliance on potentially incomplete or inaccurate data. Furthermore, due to the diversity of injury patterns within the study population, a uniform collection of Patient-Reported Outcome Measures (PROMs) and ranges of motion was not performed. In addition, our analysis focused primarily on surgical complications. We did not systematically record anesthetic-related complications, such as postoperative nausea and vomiting (PONV), which occur in approximately 20% of cases following general anesthesia. 19 Since the risk of PONV is virtually non-existent with the WALANT technique, its impact on patient satisfaction and the potential risk of postoperative hematoma could not be quantified in this study. Importantly, PONV is known to increase the risk of postoperative hematoma due to spikes in blood pressure during vomiting. 20 Therefore, the omission of these events likely underestimates the overall complication rate of the general anesthesia group.
WALANT and Complications
LA offers a method to avoid systemic side effects and risks associated with sedation, including PONV, dizziness, aspiration, pneumonia, malignant hyperthermia, thromboembolism, and respiratory failure. It represents a safe alternative for hand surgery interventions, particularly in multimorbid patients.
Large-scale studies have investigated the impact of anesthesia type on complications in hand surgery. Hustedt et al 21 analyzed 27 041 cases, demonstrating lower complication rates in local/regional anesthesia with and without sedation than in general anesthesia, especially for elderly patients.
Our study found comparable complication rates between group 1 and 2 (8.5% vs. 8.2%). However, the WALANT subgroup showed a lower complication rate (5.7%), even compared to group 1a. This might be due to the fact that more injuries of the distal middle phalanx and distal phalanx were treated with LA and a finger tourniquet. Since these areas are in the end-arterial circulation, there might be a higher complication rate here. Existing literature on WALANT complication rates varies significantly (1.7% to 12.8%),17,22 often focusing on elective procedures. Emergency surgeries are thought to carry higher complication risks.
WALANT and Time Management
Numerous studies have highlighted the resource-saving benefits of WALANT in hand surgery.16,17 However, time-related metrics are rarely reported, likely due to the elective nature of most studied procedures. This study provides novel data on process times in emergency hand surgery, complementing existing literature on WALANT’s time efficiency.
Studies have shown that WALANT can significantly reduce time to intervention. 23 For example, during the COVID-19 pandemic, a clinic in Manchester reduced the median time from injury to surgery from 5 to 2 days. 24 Other studies have demonstrated shorter procedure times and turnover times with WALANT.17,25
Our study found that 16.2% of patients treated in group 2 exceeded the recommended 6-hour treatment window, compared to only 6.6% in group 1. However, the clinical significance of this delay and the applicability of national urgency categories to hand surgery are debated.7,26
While the “golden 6-hour rule” for infection risk is no longer strictly applied, timely intervention remains a priority. Studies have shown varying results regarding the impact of delayed surgery on infection rates.26,27
This study demonstrates that WALANT reduces perioperative process times, leading to resource savings and increased patient throughput. It can be assumed that more time-efficient emergency care is associated with economic advantages, as previously demonstrated for the WALANT technique in other studies.28,29 However, this study did not include a formal cost-effectiveness analysis.
Footnotes
Author Note
Meetings at which the paper has been presented: Annual meeting of the German Society of Hand Surgery (Deutsche Gesellschaft für Handchirurgie, DGH), 2024 in Hannover, Germany.
Consent to Participate
No written informed consent was needed to participate in this study due to the approval of the ethics committee. The required data has already been routinely collected (e.g. standard recording of patient data for planning the operation, postoperative follow-up using x-ray diagnostics) and was analyzed pseudonymously without direct traceability to individual persons.
Consent for Publication
No personal images or data were used for this publication.
Author Contributions
A.A.H. and N.L. designed the study; R.M., A.A.H. and N.L. analyzed the data; S.U.E. supervised the data analysis and gave critical input for the study design; A.A.H., R.M., C.T.N., M.F. and N.L. wrote the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
The study involving human participants were reviewed and approved by Ethics Committee, approved number: 24-1229. There are no animal experiments in this study.