
Abstract
Background:
Little is known about how silicone metacarpophalangeal (MCP) arthroplasty outcomes compare between rheumatoid arthritis (RA) and osteoarthritis (OA) patients.
Methods:
Using our single institutional data from 2000 to 2022, we propensity matched 46 primary silicone MCP arthroplasties in 33 OA patients 1:2 to 92 arthroplasties in 54 RA patients based on age, sex, body mass index, operative digit, and if the surgery was on the dominant hand. We used Kaplan-Meier estimates and cluster-robust Cox proportional hazard models to compare survival free from revision, all-cause reoperation, and development of coronal plane deviation >10°.
Results:
There was comparable 10-year survival free of revision (94% OA, 91% RA) and all-cause reoperation (91% OA, 87% RA), with no difference in risk for each outcome between groups. Revision in OA patients occurred early (mean 0.6 years) for recurrent deformity (n = 2) and periprosthetic joint infection (n = 1). Revision in the RA cohort occurred later (mean 6.3 years postoperatively) for recurrent deformity (n = 3) and dislocation (n = 1). Osteoarthritis patients had less coronal plane deviation at the final radiographic follow-up (6.5° vs 16.2°, P < .001), higher 10-year survival free from coronal deviation > 10° (79% vs 17%), and lower risk of progressive coronal deformity (hazard ratio 0.15, P < .001).
Conclusions:
Silicone MCP arthroplasty remains a durable option with low reoperation rates for RA and OA. Osteoarthritis patients experience less coronal deviation and late reoperation for deformity than RA patients, likely due to their more robust soft-tissue stabilizers and noninflammatory disease process.
Keywords
Introduction
Progressive arthritis of the metacarpophalangeal (MCP) joints can cause disability, deformity, and patient dissatisfaction.1-3 A variety of nonoperative treatments exist for MCP arthritis due to inflammatory and noninflammatory conditions.2,4 When patients fail nonoperative treatment and have persistent pain and debility, arthroplasty of the MCP joint is an established option. 5 Among the implant choices for replacement of the MCP joint, silicone is the longest established and most widely used.5 -7 Other implant types such as pyrocarbon may be used when soft-tissue support is adequate, although outcomes for this implant type are similarly sparse in OA patients. 8 Silicone implants function as a spacer in the resected joint space and allow for a secondary fibrous encapsulation to provide additional stability. 7 The procedure is most often performed for rheumatoid arthritis (RA), which often affects the MCP joints.5,9 -11 Silicone MCP arthroplasty offers RA patients improvement in self-reported outcome measures, increased range of motion and functionality, and reduction in pain.5,12-15 The use of silicone MCP implants for primary osteoarthritis (OA) of the MCP joints is less well established, with sparse reports of outcomes in this population.12,16-21
Osteoarthritis involvement of the MCP joint is rare and often mild but can lead to significant pain and loss of motion.18,22 Metacarpophalangeal joint involvement is noted in between 8.2% and 13.5% of OA patients compared to 79% of RA patients.23-26 Preliminary investigations into the efficacy of silicone MCP arthroplasty for OA patients have yielded mixed results.12,16-21 Patients often experience pain relief, preserved or improved range of motion, and improvement in Disabilities of Arm, Shoulder and Hand (DASH) and Michigan Hand Questionnaire (MHQ) scores, with patient satisfaction upward of 80% to 90%.10,16,17,19 However, silicone implants in OA patients can experience complications that are also known to affect RA patients, including implant fracture. 17 Boe et al 12 have reported that OA patients are at higher risk of implant fracture and coronal plane deviation than other indications for silicone arthroplasty. However, these radiographic findings were in an unmatched cohort with a small number of OA patients, and the clinical survivorship of silicone implants in OA patients is significantly higher than radiographical survivorship.12,17,18 Mid-term revision rates following silicone implants use in OA patients have been reported to be between 1.7% and 11%, which is similar or slightly lower than reports in RA.12,16-18,21,27
The reports of clinical and radiographic survivorship in OA and RA patients have predominantly been in separate series, with only small series of OA patients. Thus, drawing comparisons between silicone outcomes in RA and OA patients is challenging given the significant differences in these two patient populations. We sought to address this gap by assessing silicone implant survivorship in a propensity-matched cohort of OA and RA patients. We hypothesized that OA patients would have lower rates of revision, all-cause reoperation, and development of coronal plane instability.
Materials and Methods
Data Source and Collection
Institutional review board approval was obtained prior to commencing this study. Using our institution’s prospectively collected Total Joint Registry (TJR), we retrospectively identified all patients who underwent primary MCP arthroplasty with silicone implants for RA or OA between 2000 and 2022. We did not include posttraumatic arthritis in the OA group and only considered patients with primary OA. We identified 46 silicone arthroplasties in 33 patients with OA and 421 arthroplasties in 121 patients with RA.
Propensity Matching
A combination of data available in our TJR and manual review of these medical records was used to collect data on patient demographics, preoperative measurements, operative details, and postoperative reoperations. Joints in patients with RA were then propensity matched 2:1 using the nearest neighbor to joints in patients with OA based on age, sex, body mass index, operative digit, and if the surgery was on the dominant hand. Exact matching was forced for patient sex to ensure equal balance. This resulted in a cohort of 92 joints in 54 RA patients and 46 joints in 33 OA patients. The resulting matched cohort was well balanced, with no statistically significant differences in baseline characteristics (Table 1).
Comparison of Propensity Score Matching Variables Between Groups.
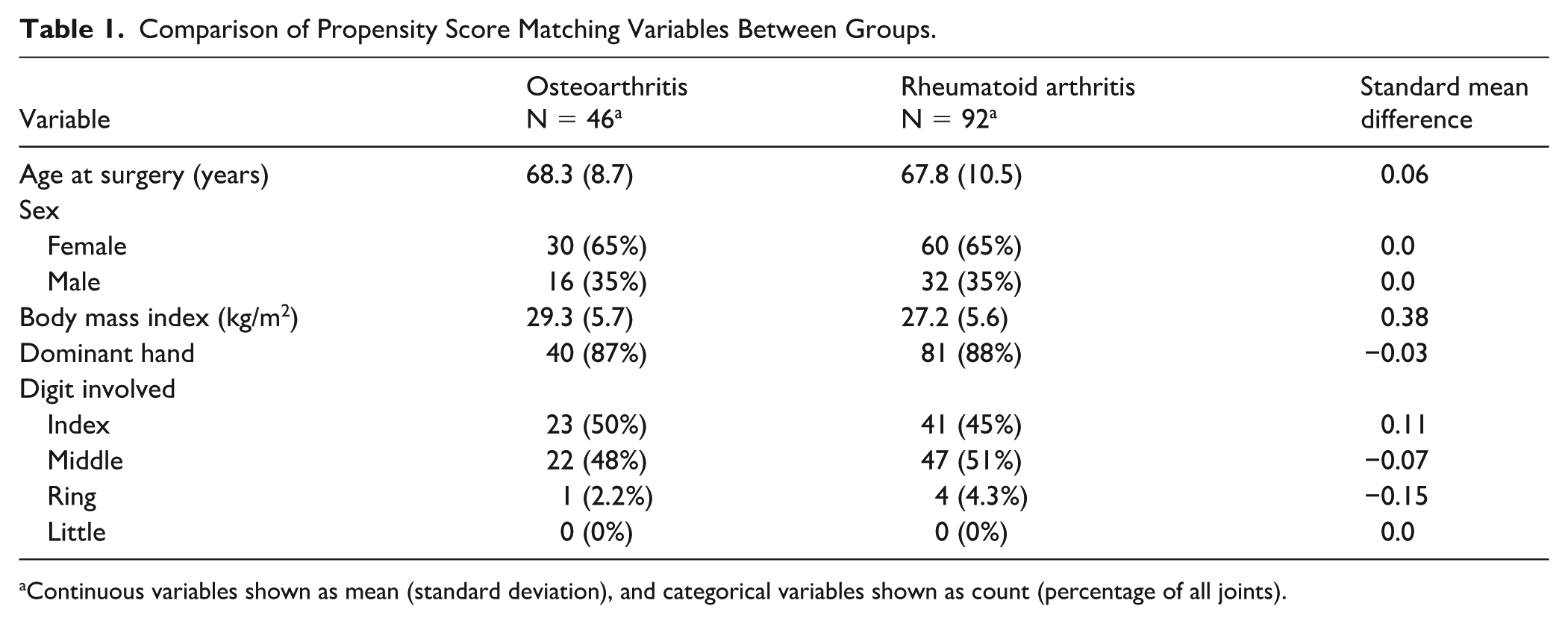
Continuous variables shown as mean (standard deviation), and categorical variables shown as count (percentage of all joints).
Outcomes
Our primary outcomes of interest were revision, all-cause reoperation, and development of coronal plane deviation exceeding 10° on postoperative radiographs. We considered patients to have a revision if they had the silicone implant removed or replaced. For all-cause reoperation, we considered revision and nonrevision reoperations. Coronal plane deviation was measured from postoperative posteroanterior radiographs as the degrees away from neutral between the diaphysis of the metacarpal and proximal phalanx. There were 6 joints in RA patients and 3 joints in OA patients without available postoperative radiographs, leaving 86 RA joints and 43 OA joints for radiographic analysis.
Statistical Analysis
Cohort characteristics were reported using descriptive statistics. Survival free from revision, all-cause reoperation, and development of coronal plane deviation was compared between RA and OA cohorts using Kaplan-Meier estimates. We also assessed OA as a risk factor for each outcome using univariate Cox proportional hazard models. We use cluster-robust variance estimates to account for multiple joints replaced in some patients. Results of Cox models were reported as hazard ratios (HR) with 95% confidence intervals. Low event numbers prevented an additional multivariable analysis. All analyses were conducted using R version 4.5.1.
Results
Summary of Cohort
There were 46 joints in 33 patients with OA (mean follow-up 7.2 years) and 92 joints in 54 patients with RA (mean follow-up 7.4 years) after matching (Table 1). Preoperatively, the RA cohort had greater coronal plane deformity (26.3° vs 10.7°) and lower grip strength (10.4 kg vs 15.1 kg). The OA and RA cohorts were both predominantly female (65%), with an average age of 68. The index (46%) and middle (50%) fingers were most commonly the operative digits. The cohorts were well-matched with no significant differences between groups (Table 1).
Revisions
The overall rate of revision was 6.5% in the OA group and 4.3% in the RA group. In the OA cohort, there were 2 revisions in a single patient for recurrent deformity, and 1 revision for periprosthetic joint infection (Table 2). In the RA cohort, there were 3 revisions in 3 patients for recurrent ulnar deformity and 1 revision for dislocation (Table 3). The 2-, 5-, and 10-year survivals free from revision were 94%, 94%, and 94% in the OA cohort and 99%, 99%, and 91% in the RA cohort, respectively (Figure 1). In univariate analysis, a primary diagnosis of OA did not affect hazard for revision (HR 1.6, 95% CI 0.29-8.8, P = .58) (Table 4).
Revisions and Reoperations in Osteoarthritis Patients.
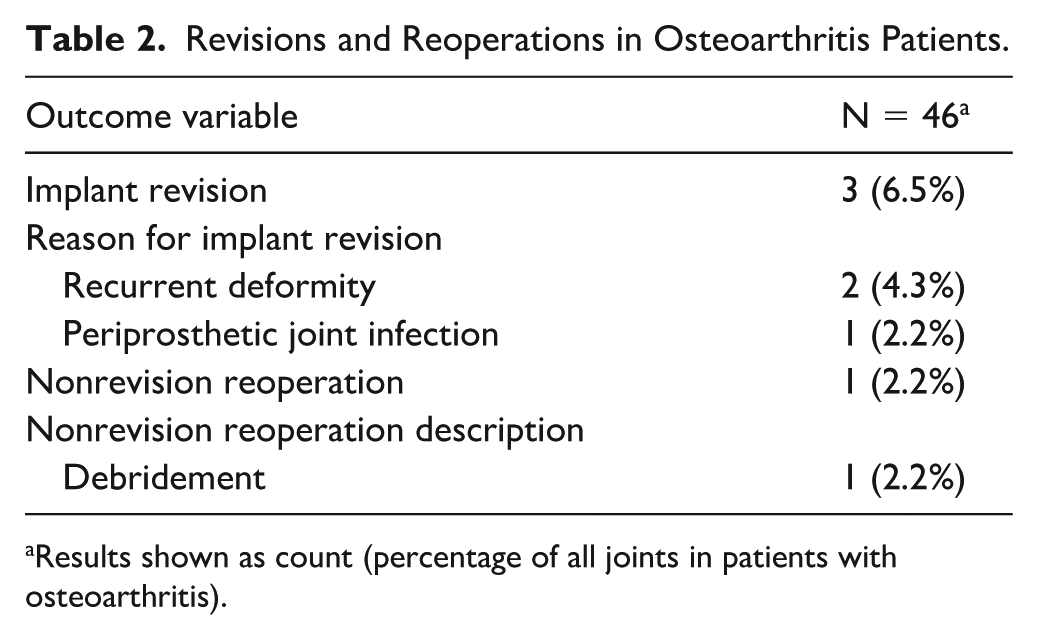
Results shown as count (percentage of all joints in patients with osteoarthritis).
Revisions and Reoperations in Rheumatoid Arthritis Patients.
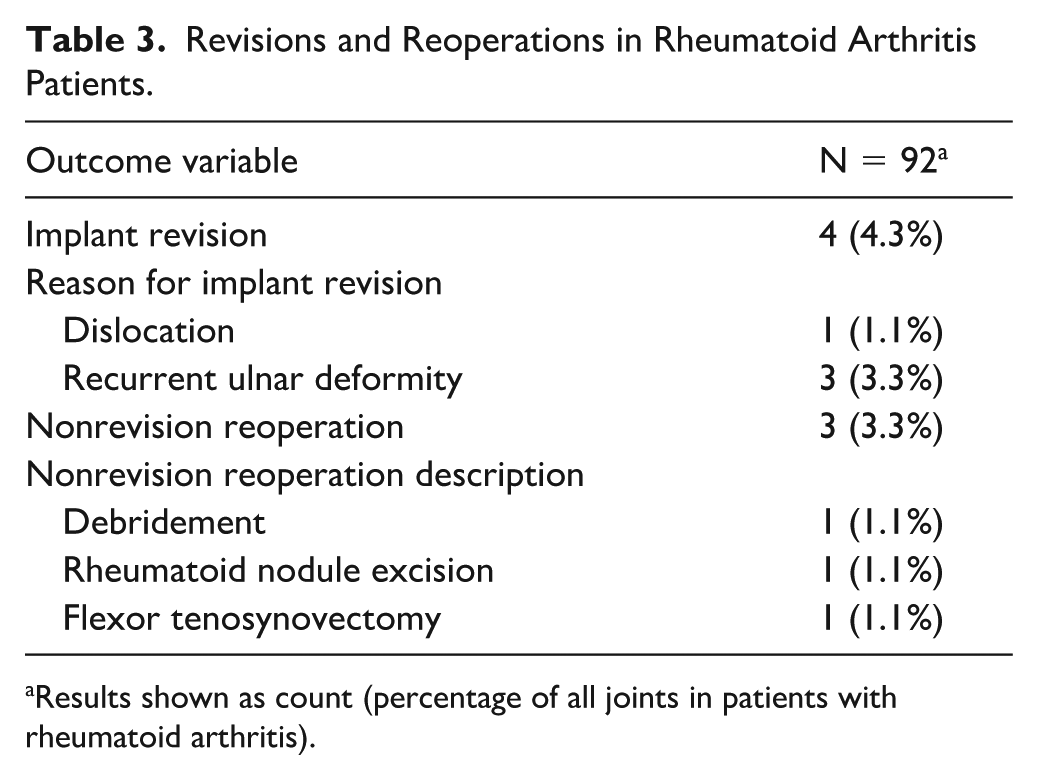
Results shown as count (percentage of all joints in patients with rheumatoid arthritis).
Univariate Cox Proportional Hazard Model Results for Survival Endpoints.
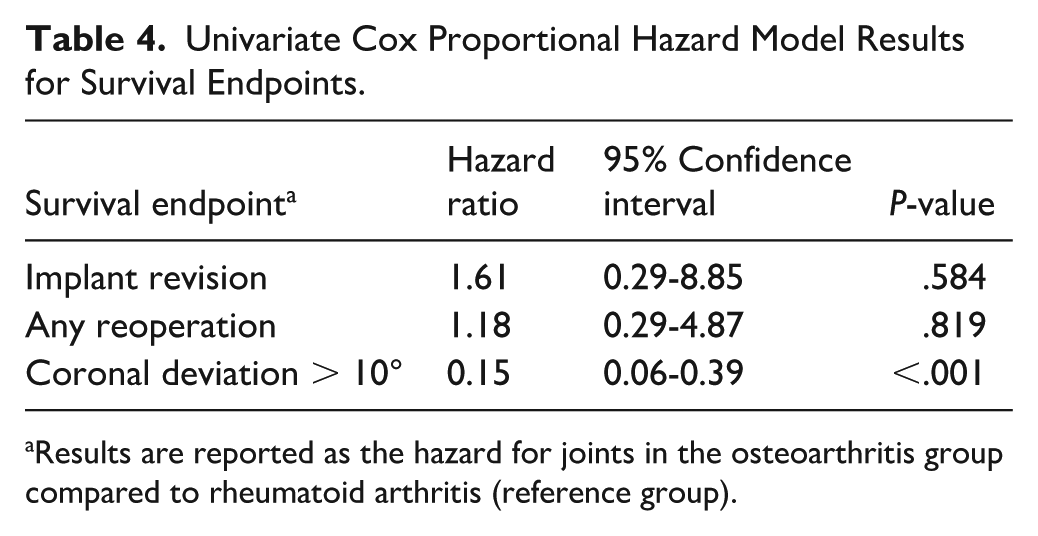
Results are reported as the hazard for joints in the osteoarthritis group compared to rheumatoid arthritis (reference group).
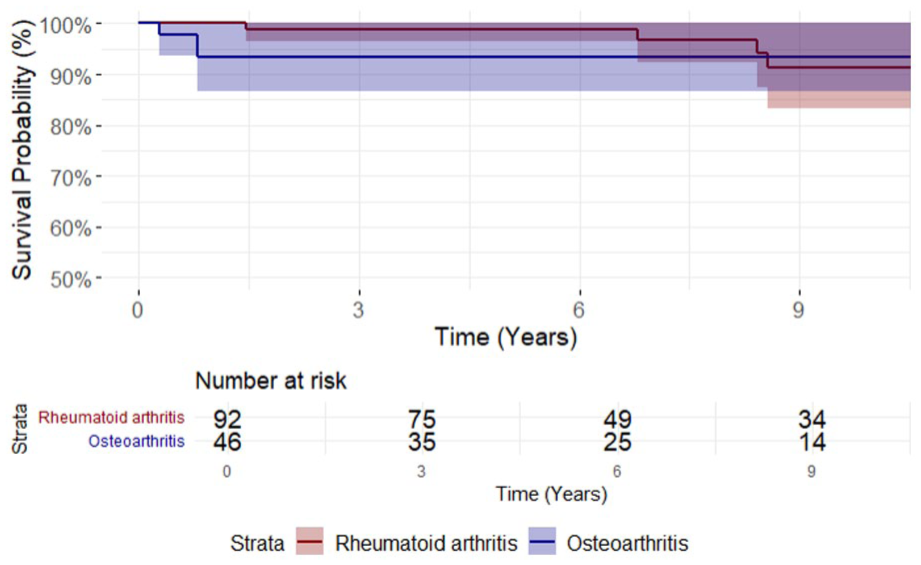
Survival free from revision in osteoarthritis and rheumatoid arthritis cohorts. Revision counted as any removal or replacement of the original silicone implant placed.
Reoperations
The overall rate of all-cause reoperation was 8.7% in the OA group and 7.6% in the RA group. Nonrevision reoperations in the OA cohort included 1 debridement for infection concern, which left the implant in place (Table 2). Nonrevision reoperations in the RA cohort included 1 flexor tenosynovectomy, 1 removal of a rheumatoid nodule overlying the MCP, and 1 debridement for infection concern (Table 3). The average time to first reoperation was 0.5 years in the OA cohort and 4.9 years in the RA cohort (P = .01). The 2-, 5-, and 10-year survivals free from all-cause reoperation were 91%, 91%, and 91% in the OA cohort and 98%, 97%, and 87% in the RA cohort, respectively (Figure 2). In univariate analysis, a primary diagnosis of OA did not affect hazard for all-cause reoperation (HR 1.2, 95% CI 0.29-4.9, P = .82).
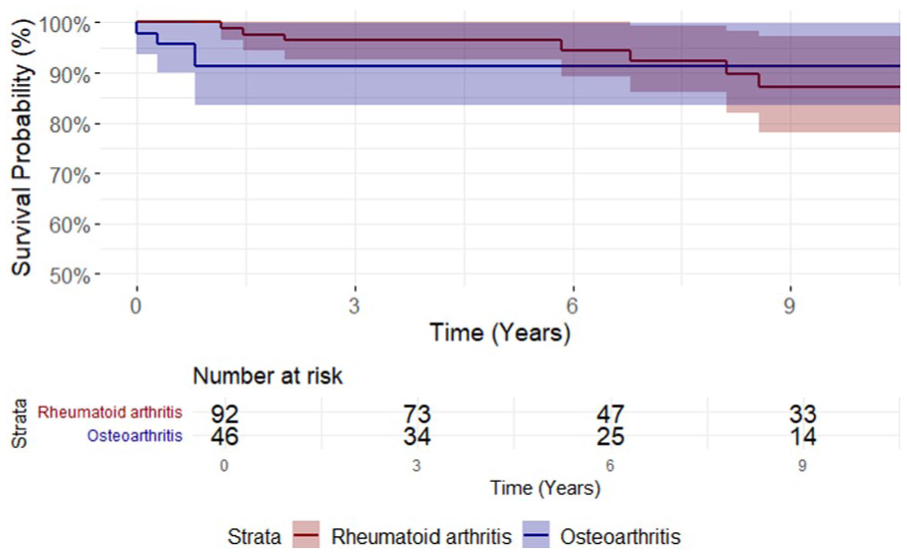
Survival free from all-cause reoperation in osteoarthritis and rheumatoid arthritis cohorts. Reoperations included revisions and nonrevision reoperations.
Radiographic Outcomes
The average radiographic follow-up obtained was 4.7 years in the OA group and 3.8 years in the RA group. At the final radiographic follow-up, average coronal plane deviation was 6.5° in the OA group and 16.2° in the RA group (P < .001). In the OA group, 8 joints (19%) developed progressive coronal plane deviation > 10°, compared to 53 joints (62%) in the RA group (P < .001). The 2-, 5-, and 10-year survival free from recurrent coronal deviation > 10° were 93%, 86%, and 79% in the OA group and 52%, 37%, and 17% in the RA group, respectively (Figure 3). In univariate analysis, OA patients were at lower risk of recurrent coronal plane deviation > 10° than RA patients (HR 0.15, 95% CI 0.06-0.39, P < .001).
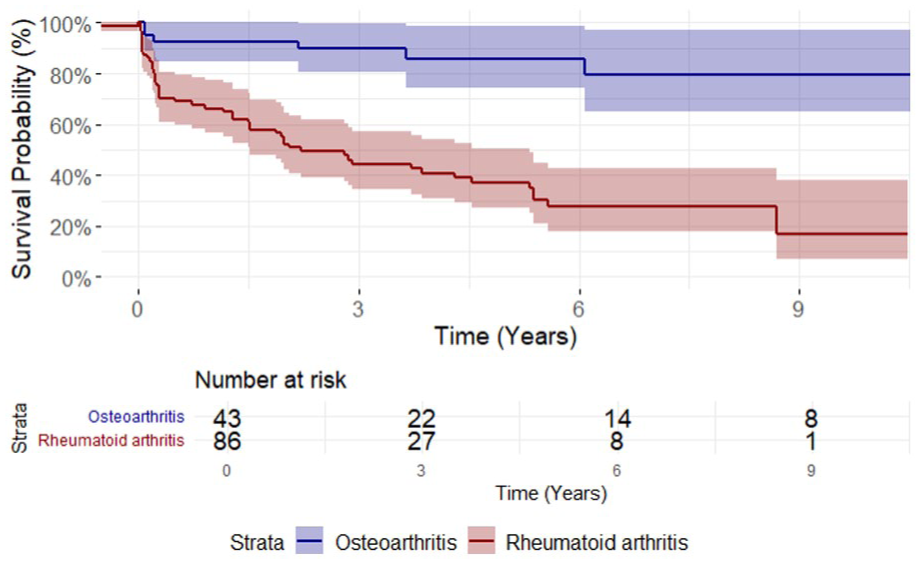
Survival free from coronal deviation greater than 10° in osteoarthritis and rheumatoid arthritis cohorts.
Discussion
Silicone implants are considered by many to be the gold standard for MCP arthroplasty in RA patients, but outcomes in OA patients remain sparsely reported in comparison. The rarity of primary MCP OA has contributed to limited data available regarding small joint arthroplasty in these patients. In our matched cohort, we found that OA patients had comparable survivorship free from revision and all-cause reoperation and higher survival free from recurrent coronal plane deformity than RA patients.
Among the OA cohort in our study, we report a revision rate of 6.5% at mean follow-up of 7.2 years, which lies in the middle of other reports between 1.7% and 11% in smaller cohorts.12,17 -19,21 Revision in our OA patients occurred twice for early (average 0.6 years postoperatively) complications of recurrent deformity and periprosthetic joint infection. There was only one additional nonrevision reoperation for infection in this group. These reoperations can be attributed to rare, early postoperative complications that are mitigated by careful intraoperative sterility measures and achievement of soft-tissue balance. 28 Notably, there were no late revisions or reoperations in our OA cohort for recurrent deformity.
This contrasts with our RA cohort, who had 4 revisions (4.3%) at an average of 6.3 years after the index surgery, all for recurrent deformity or dislocation. This is similar to other reported revision rates in the RA population that fall between 2.9% and 9.1%, often for recurrent deformity.12 -14,27 Many studies in the RA population have noted high rates of implant fractures, which do not always lead to revision. Our findings suggest that revisions in the RA population tend to be for recurrent joint deformity, which could be due to a combination of poor soft-tissue stability, mechanical implant failure, and progressive erosive disease around the implant. Rheumatoid arthritis patients in our cohort had higher preoperative MCP deviation and lower grip strength, which may indicate a more deformed and functionally limited joint that is more prone to recurrent instability.
We found a notable difference in risk of progressive coronal plane deviation, with OA patients being over 6-times less likely to develop deviation greater than 10° during follow-up. Coronal plane instability is an issue known to affect the RA population who undergo silicone arthroplasty, though reports in the OA population are somewhat contradictory. This study found that progressive coronal plane deformity > 10° occurred in 62% of RA patients and in 19% of OA patients. Our OA cohort had an average of 6.5° of coronal plane deviation at the final follow-up. This is higher than the 2.7° reported by Namdari et al but nearly identical to reports of 5° and 6° in other small cohorts.16,17 Conversely, Boe et al 12 found that OA patients had increased risk of coronal plane deviation > 10° and silicone implant fracture compared to inflammatory arthritis and posttraumatic arthritis patients. This surprising finding was thought to be due to increased functional demands in OA patients or less frequent soft-tissue-balancing procedures, though these factors were not assessed. A noted limitation of their study was the inclusion of only 11 OA joints in an unmatched and uncontrolled cohort with predominantly inflammatory arthritis patients. Overall, our findings support that OA patients are at significantly less risk of postoperative coronal plane deformity and instability than RA patients. Stability in the coronal plane after silicone arthroplasty is primarily provided by remaining collateral ligaments and the fibrous encapsulation that occurs in response to the implant. 7 The implant itself provides little long-term stability in this manner and is found fractured in up to two-thirds of patients.12-14 The difference in achieving coronal plane stability between RA and OA patients is likely driven by the very different disease processes, with RA patients often having less robust collateral support. Recurrent deviation and coronal deformity remain prevalent among RA patients undergoing MCP arthroplasty and are valuable goals of future investigation to optimize outcomes for these patients.
Our findings overall support that silicone arthroplasty remains a durable option with low long-term revision rates in the setting of advanced OA and RA. Osteoarthritis patients can be counseled of their decreased risk of long-term coronal instability due to the noninflammatory nature of the condition. Early postoperative complications such as infection may occur in OA patients and necessitate reoperation, though this remains rare.
Our study is limited by its retrospective scope. In addition, the small cohort sizes and low number of survival events limited our ability to control for additional covariates, leading to potential residual confounding. Factors such as bone density, disease-controlling medications in the RA cohort, and other patient-specific characteristics may impact outcomes and were unable to be assessed. This study only evaluated silicone implants. Pyrocarbon implants, which may be used if there is robust soft-tissue support, were not assessed and would be valuable goals of future investigation. Additional limitations include a basis at a single institution and tertiary referral center bias. The study did not include subjective patient-reported outcome measures, which could provide additional insight into differences in patient satisfaction between RA and OA patients.
Conclusions
This study found that rates of revision and all-cause reoperation after silicone MCP arthroplasty remain comparably low in both OA and RA patients. Osteoarthritis patients experience less frequent coronal plane deformity and late reoperation for deformity than RA patients, likely due to their more robust soft-tissue stabilizers and noninflammatory disease process.
Footnotes
Acknowledgements
The authors have no acknowledgements to make in the creation of this work.
Ethical Considerations
This study was approved by our institutional review board (IRB #24-013045).
Consent for Publication
Not applicable.
Author Contributions
ZP: data collection, manuscript writing and review. AS: study conceptualization, data collection, statistical analysis, manuscript writing and review. AB: data collection, manuscript review. MR: study conceptualization, manuscript writing and review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study. This article does not contain any studies with animal subjects.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
AI Disclosure
No generative AI tools were used in the creation of the work.