
Abstract
Keywords
Introduction
The formation of tendon adhesions after tendon injury and surgery has been well described in the literature as the most common complication following tendon repair 1 and as greatly limiting functional outcomes. 2 Adhesions occur in approximately 30% of flexor tendon injuries1,2 due to excessive collagen production from traumatized cells surrounding the tendons; adhesions can form regardless of whether flexor tendon injuries are treated operatively or nonoperatively. 1 Tendon adhesions tend to form more densely where there is less differential glide between the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. 3
Preventative measures such as early therapy with active motion and nonsteroidal anti-inflammatory drugs have been found to reduce rates of adhesion formation requiring secondary procedures.4 -7 Early active motion approaches are favored over early passive motion and immobilization protocols worldwide due to superior results and recovery speed. 6 There has been extensive literature regarding relative motion orthosis (RMO) or immediate controlled active motion in management of extensor tendon injuries. These protocols allow simple and effective early active motion to lessen adhesion formation while protecting tendon repairs. Since then, research and proof-of-concept cadaveric studies have been conducted to broaden the use of these treatment modalities to both flexor and extensor tendon injuries.8,9 Studies have shown RMO to be valuable to improve range of motion, return to work, early initiation of postoperative therapy, ease of use, and financial burden of treatment. 10 Relative motion orthoses have been successfully integrated into practices around the world.
Tendon adhesions are difficult to manage, resulting in literature focusing on their prevention. Tenolysis is the only described surgical management of postinjury adhesions2,11,12 and is accompanied by inherent risks of surgery that are not suitable for all patients. Therefore, nonsurgical treatment with occupational therapy is typically exhausted before proceeding with surgical intervention. The goals of therapy are to achieve tendon excursion and especially differential glide between tendons, but often with limited efficacy. Methods of nonsurgical treatment are worthy of further exploration.
Anecdotal evidence from occupational therapists who work directly in the postoperative rehabilitation of tendon injuries suggests that incorporation of relative motion extension splints (RMES) can improve outcomes of nonoperative treatment of flexor tendon adhesions. Regional occupational therapists have been using RMES to increase flexor tendon excursion during exercises aimed to lyse adhesions for the past 6 years with good clinical results. Differential glide is assessed clinically and functionally in occupational therapy. It is assessed by selective motion, composite motion, functional excursion, and whether there are clinical signs of restriction. Occupational therapists asses if there is smoothness of “catching” with motion, pain with tendon motion, blocking at specific joint ranges, or if there is an increased effort to isolate motion. The purpose of this study is to provide proof of concept for this modality in a cadaveric model. The authors hypothesize that incorporation of RMES splints during active range of motion (AROM) exercises will place the tendons in a relatively extended position, resulting in greater total flexor tendon excursion during flexion exercises and greater differential tendon glide; this could theoretically increase likelihood of lysing tendon adhesions during therapy exercises.
Materials and Methods
An 84-year-old male fresh-frozen right-upper-extremity cadaver specimen was obtained and thawed. Skin and soft tissue was removed from the volar aspect of the middle-finger ray to expose the flexor tendons and pulleys. The A1 pulley and 30% of the proximal portion of the A2 pulley were resected for better visualization of the differential glide of the FDS and FDP tendons. A3 and A4 pulleys were left intact. A longitudinal incision was made over the volar wrist and distal forearm to dissect and expose the middle-finger FDS and FDP tendons. 0-Ethibond Krakow sutures were placed individually to the FDS and FDP tendons at the wrist exposure to hold a 1-kg weight to approximate 10 N. The 10-N force was chosen to replicate therapeutic motion without compromising the integrity of the specimen.8,13 A fiberglass cast was applied to the wrist to maintain it in a neutral position. A dorsal finger splint was applied to the middle finger to maintain metacarpophalangeal joint (MCPJ) and proximal interphalangeal joint (PIPJ) digital extension when needed for isolated movements. The material used for orthotics fabrication is 1/8” solid Polyform Thermoplastic material. The material is heated in water at 120°F. The affected finger is placed in approximately 20° of extension relative to nearby digits. A pen or item of that size is used as a marker. The material is then molded with a pen, holding the finger in extension. The material requires several minutes to cool, after which is becomes firm and nonmoldable. The specimen was mounted on a testing apparatus to hold the forearm vertically (Figure 1). An RMES was fabricated from flat sheets of moldable plastic splint material that were heated and molded directly to the patient. The splint was custom fit to the middle finger to achieve relative extension at the MCPJ of approximately 20° to 30°.
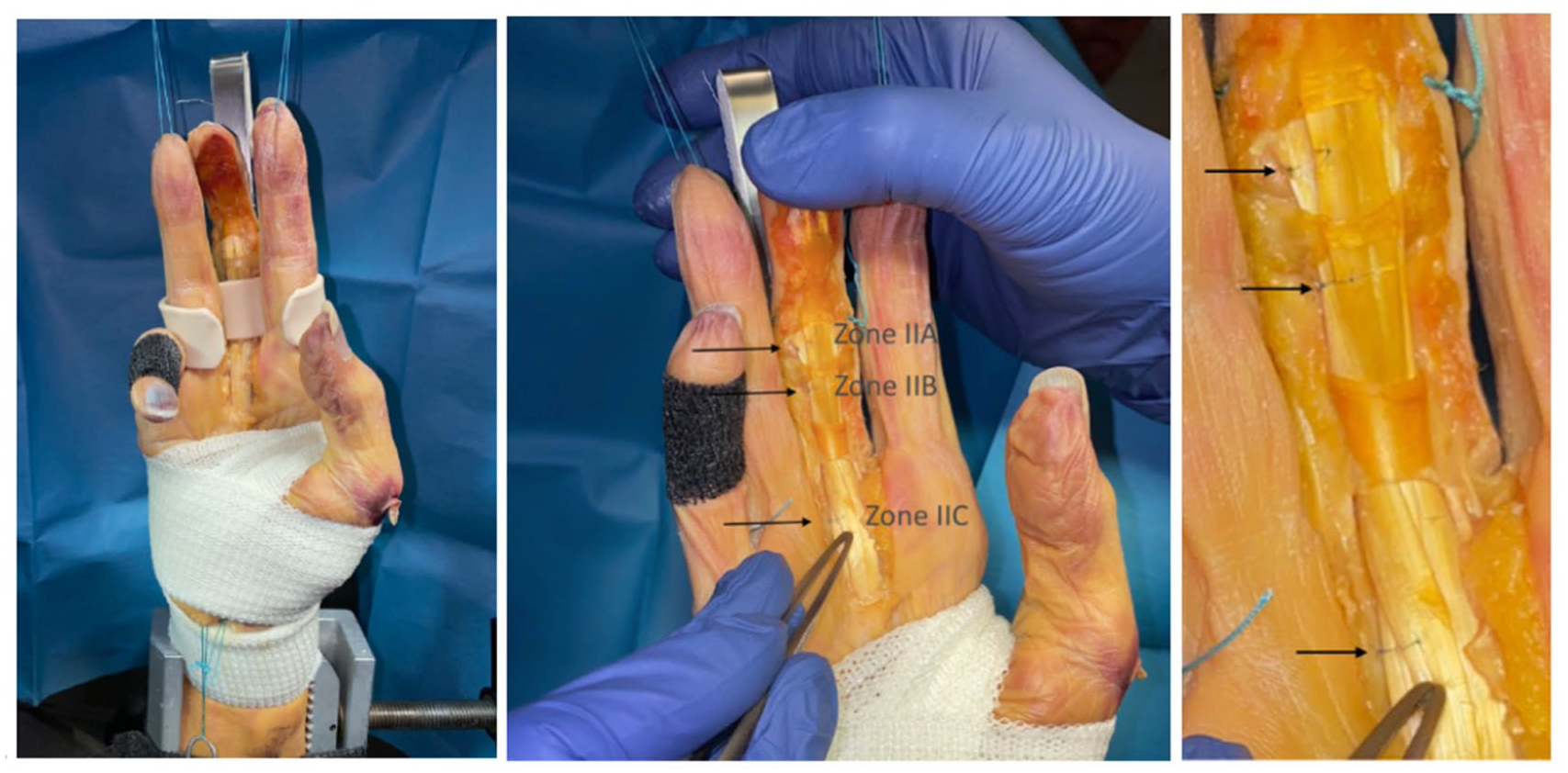
(a) Vertical mounting apparatus. (b) Zones IIA, IIB, and IIC marked with baseline sutures on cadaveric upper extremity. (c) Closer view of baseline sutures.
A 7-0 Prolene suture was used to mark the relative starting positions of the FDS and FDP tendons at various levels (IIA, IIB, IIC) with the finger held in full extension at the MCPJ, PIPJ, and distal interphalangeal joint (Figures 2 and 3). Zone IIA is distal zone II, where FDS is dorsal to FDP. Zone IIB is mid-zone II, where the FDS slips are positioned on either side of FDP. Zone IIC is proximal zone II, where FDS is volar to FDP (Figure 2). Cadaveric studies have shown that these subzones have different tendencies for adhesion formation and require specific attention during rehabilitation, as described by Chinchalkar et al. Tendon excursion and differential glide between the FDS and FDP tendons were measured at each level under 6 test conditions: isolated FDS motion with and without RMES, isolated FDP motion with and without RMES, and combined FDP and FDS motion with and without RMES. A force of 10 N was applied to the Krakow sutures in the distal forearm to replicate active contraction of the FDS or FDP muscle bellies. 8 Isolated FDS motion was tested while immobilizing the adjacent digits in extension (Figure 3). Isolated FDP motion was tested while immobilizing the PIPJ; this was achieved by passing a 0-Ethibon through the soft tissue at the middle phalanx level of the third digit and securing it to the dorsal finger splint to maintain PIPJ extension (Figure 4). Combined FDS and FDP motion was tested by placing weight to the FDP with the PIPJ unrestricted; this was included to represent active composite fist motion.

Schematic of zone IIA/B/C.
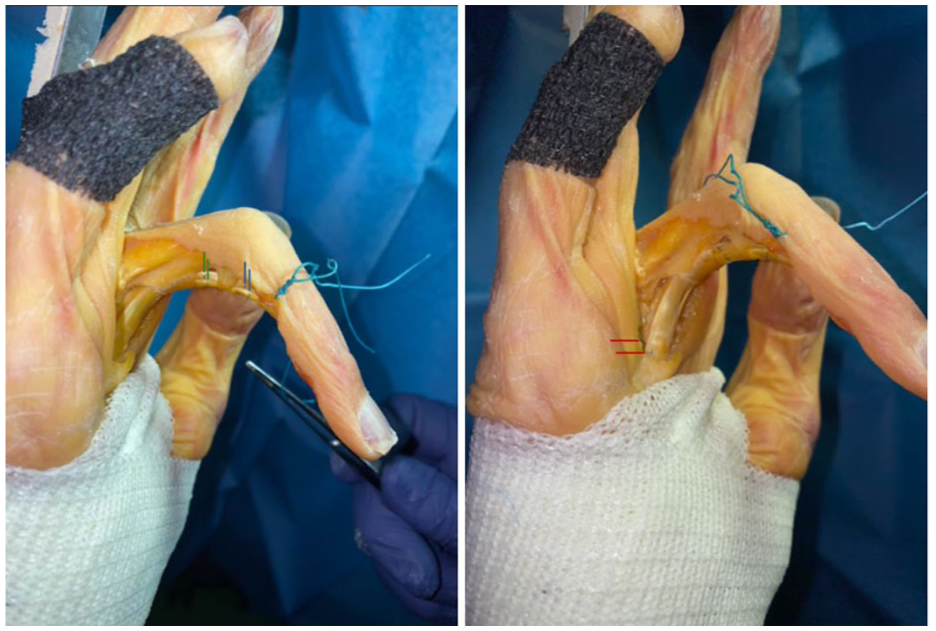
Suture position changes after isolated FDS exercise without RMES, demonstrating differential glide from different views (zone IIA in blue, IIB in green, and IIC in red). FDS = flexor digitorum superficialis; RMES = relative motion extension splints.

Suture position changes after isolated FDP exercise without RMES, demonstrating differential glide in each zone (zone IIA in blue, IIB in green, and IIC in red). FDP = flexor digitorum profundus; RMES = relative motion extension splints.
Prior to each testing condition, the marking sutures on the FDS and FDP tendons were in the same positions. After the tendons were loaded for each test condition, the distances between the marked starting points were measured to determine the distance of differential glide between the tendons at each level (Figures 3 and 4). Each condition was measured 3 times by 3 separate individuals to confirm consistency, and the resulting measurements were averaged.
Each condition was tested 9 times with and without the RMES, and measurements were averaged within each condition. Paired comparisons were performed using a paired t-test, with statistical significance set at P < .05.
Results
The application of weight to the FDS and FDP tendons effectively replicated muscle activation for AROM exercises. Isolated FDS exercises with RMES in place resulted in increased differential glide in zones IIA and IIB when compared to isolated FDS exercises without RMES in place. Zone IIA displayed differential glide of 1 mm without RMES and 3 mm with RMES. Zone IIB displayed a differential glide of <1 mm without RMES and 3 mm with RMES. No difference was seen in zone IIC during this exercise, where differential glide was 3 mm with and without RMES (Table 1).
Gliding Differential Between FDS and FDP Markers During Tension (Millimeters).
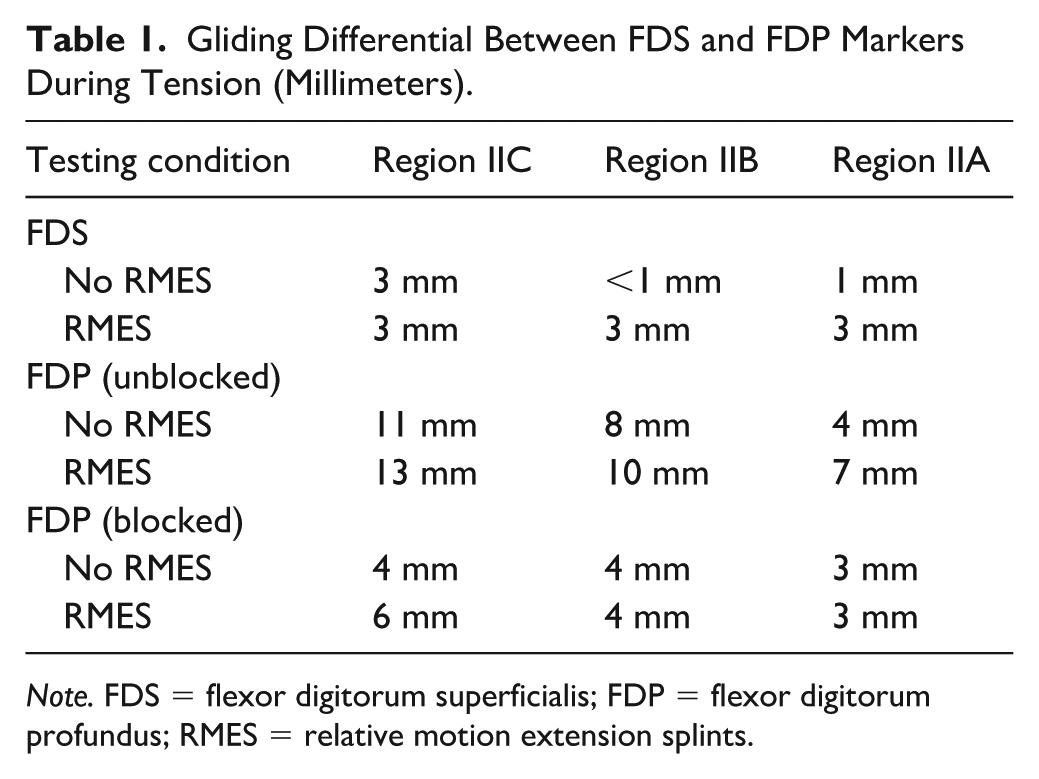
Note. FDS = flexor digitorum superficialis; FDP = flexor digitorum profundus; RMES = relative motion extension splints.
Isolated FDP exercises with RMES in place resulted in increased differential glide in zone IIC when compared to isolated FDP exercises without RMES in place. Zone IIC displayed differential glide of 4 mm without RMES and 6 mm with RMES. Zone IIA displayed differential glide of 3 mm with and without RMES. Zone IIB displayed differential glide of 4 mm with and without RMES (Table 1).
Combined FDS and FDP exercises with RMES in place resulted in increased differential glide in zones IIA, IIB, and IIC when compared to combined FDS and FDP exercises without RMES in place. Zone IIA displayed differential glide of 4 mm without RMES and 7 mm with RMES. Zone IIB displayed differential glide of 8 mm without RMES and 10 mm with RMES. Zone IIC displayed differential glide of 11 mm without RMES and 13 mm with RMES (Table 1).
The mean differential glide without RMES was 4.23 mm while the splinted condition had a mean differential glide of 5.78 mm (Table 2).
Comparison of Differential Glide With and Without Relative Motion Extension Splinting.
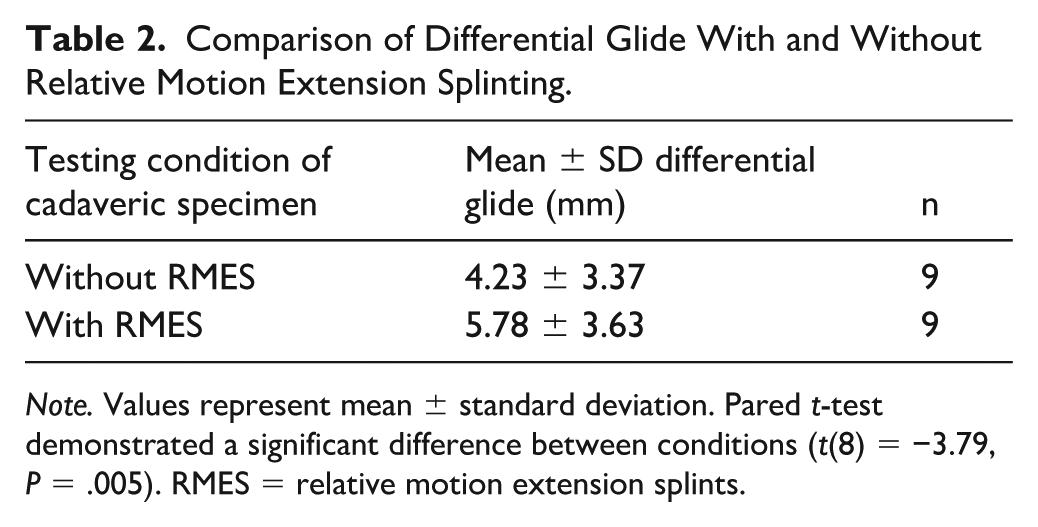
Note. Values represent mean ± standard deviation. Pared t-test demonstrated a significant difference between conditions (t(8) = −3.79, P = .005). RMES = relative motion extension splints.
Discussion
Various exercises are utilized by occupational therapists to improve range of motion and to prevent or lyse flexor tendon adhesions. Blocking exercises of each flexor tendon allows the isolated tendon to glide independently over the other inactivated tendon, as well as surrounding tissues (e.g., overlying tendon sheath and underlying bone). Composite fist exercises achieve maximal FDP glide across surrounding tendon sheath and bone, whereas straight fist position achieves maximal FDS glide (Royal United Hospital). Currently, occupational therapy followed by surgical tenolysis is the common treatment for flexor tendon adhesions as they are often resistant to conservative measures. However, occupational therapists have been using RMES to enhance range-of-motion exercises for 6 years with promising clinical results. Relative motion extension splints increase tendon excursion, theoretically increasing efficacy of conservative treatment options to lyse tendon adhesions.
Relative motion flexion splinting (RMFS) has been used to reduce tension across flexor tendons during treatment of flexor tendon injuries. Since the FDP tendons share a common muscle belly, when one of the digits is splinted in relative flexion compared to the other digits, the splinted flexor tendon is effectively tension-offloaded, and excursion is reduced. This concept is similar to the quadriga effect and has been used to protect flexor tendon injuries and repairs while allowing early active motion. 14 Reduction of flexor tendon elongation with RMFS has been further observed in cadaveric models. 8 It can therefore be hypothesized that placing the treated digit in relative extension with RMES will have the opposite effect on flexor tendons, resulting in greater tendon elongation and excursion during exercises compared to digits without RMES.
Differential glide between FDS and FDP tendons is thought to be critical to prevention and lysing of flexor tendon adhesions. 3 Our cadaveric study measured the differential glide between FDS and FDP tendons in zone II with and without RMES and showed increased differential glide when RMES were in place (Table 2). The mean differential glide was significantly greater with the RMES (5.78 ± SD) than with the unsplinted condition (4.2378 ± SD) (paired t-test, t(8) = −3.79, P = .005). However, this study also shows that differential glide is not uniform throughout zone II. Zones IIA, IIB, and IIC were found to have different degrees of differential glide, which may explain why some zones are more prone to adhesion formation than others and why some adhesions are more resistant to therapy. Isolated FDS exercises were found to result in 3 mm of differential glide in zone IIC and little to no differential glide in zones IIA and zones IIB. Addition of RMES improved differential glide in zones IIA and IIB (increased from 1 mm to 3 mm), whereas no change was seen in zone IIC; RMES improved differential glide in the zones where it was most limited during isolated FDS exercises. Isolated FDP exercises resulted in a 3 to 4 mm of differential glide among zones. Addition of RMES improved differential glide in zone IIC to 6 mm but had no effect on the other zones. Combined FDS and FDP exercises resulted in the greatest amount of differential glide in all zones (4 mm in IIA, 8 mm in IIB, 11 mm in IIC), and addition of RMES almost uniformly increased differential glide in all zones by 2 to 3 mm (7 mm in IIA, 10 mm in IIB, and 13 mm in IIC). Figure 5 shows the overall distribution and pattern of gliding differential between FDS and FDP markers of each testing condition. This data can help to better understand where adhesions are most likely to form in relation to the location of the tendon injury, and which exercises will be most effective to treat the zone at the greatest risk.

Plotted gliding differential between FDS and FDP markers during tension (mm). FDS = flexor digitorum superficialis; FDP = flexor digitorum profundus; RMES = relative motion extension splints.
The observed variability in differential glide across zones IIA, IIB, and IIC can be attributed to anatomic and biomechanical differences inherent to each region. Zone II is a complex area due to the interplay of the FDS and FDP tendons and their close relationship to the pulley system. In our study, the variability in differential glide highlights how local tendon mechanics and anatomical constraints may influence tendon mobility and the likelihood of adhesion formation. Zones IIA and IIB demonstrated more limited differential glide during isolated FDS exercises, likely due to constraints from the A2 and A3 pulleys and limited FDS tendon excursion near its insertion. In contrast, zone IIC exhibited greater baseline differential glide, potentially due to a relatively freer proximal environment. Isolated FDP exercises exhibited more uniform differential glide among zones at baseline, likely because its insertion is more distant and less restrictive within zone II (Figure 5).
The responsiveness to RMES during isolated FDS exercises suggests that mechanical assistance is more impactful where natural glide is restricted, specifically in zones IIA and IIB. The increase in differential glide with RMES in these areas may be due to its ability to reduce extrinsic tethering and promote separation between the tendons, which mimics the physiologic conditions needed to break down adhesions. The data also suggests that zones with lower baseline differential glide (IIA and IIB) are more prone to adhesion formation and may be less responsive to isolated tendon mobilization, which would require more targeted or combined therapy in the form of RMES and active motion. Zone IIC, with a higher intrinsic glide, may be more resilient to adhesion formation but still benefits from combined or RMES-reinforced exercises. Relative motion extension splints during isolated FDP exercises were found to have a positive impact in zone IIC where it was lacking during isolated FDS exercises.
This study has multiple limitations. The release of A1 and partial A2 pulleys was performed for visualization, and this could affect tendon excursion and the differential glide seen. The tendons in this model have also lost normal gliding surface with the removal of the skin and subcutaneous tissue, and motion is tested in direct contact with the RMES. In addition, the current findings are based off of testing of a single finger, rather than pooling data across digits, as only 1 specimen was available for use. Flexor tendon and differential glide are known to vary by digit due to differences in tendon anatomy (length), moment arms, and joint kinematics. These inherent digit-specific differences may influence the magnitude of excursion observed across fingers and should be considered for future studies. Flexor tendon adhesions were not replicated; therefore, the documented distance of differential tendon glide is not comparable to that in patients with adhesions, and it is not known what force and excursion would be required to lyse adhesions. Finally, our model of combined FDS and FDP motion does not perfectly replicate the more complicated composite fist motion or the complex physical condition following tendon repair. In regard to the proposed treatment, it is important to note that there is no direct evidence in the existing medical literature that a differential glide between flexor tendons can lyse established adhesions. This concept, however, is well-established in hand therapy as a means to promote tendon excursion and prevent adhesion formation. The potential for this treatment to help lyse adhesions, however, is supported by anecdotal experience of occupational therapists.
This study demonstrates that the use of RMES during AROM exercises increases tendon excursion and the differential glide between the FDS and FDP tendons. RMES has been used in practice for treatment of flexor tendon adhesions with promising results. This practice should be limited to patients with well-healed flexor tendons until additional studies are done to determine the potential risk of rupture. Studies are needed to determine the force across the tendon during exercises with RMES so that clinicians can implement a timeline of when it is appropriate to introduce this practice. Additional studies are also needed to replicate adhesions under the stress of AROM with RMES to give further insight into the efficacy of this practice.
Conclusion
The application of relative motion extension splinting is effective in increasing the differential glide between FDP and FDS tendons. The use of RMES resulted in a statistically significant increase in differential glide compared to the unsplinted condition (mean difference = 1.55; paired t-test, P = .005). The responsiveness to RMES suggests that mechanical assistance is more impactful where natural glide is restricted. Additional studies are needed to provide evidence that increased differential glide promotes lysis of adhesions. Additional studies are also needed to determine the tendon forces in vivo and when it is safe to implement this practice in a healing tendon to avoid the risk of rupture.
Footnotes
Authors’ Note
The cadaveric specimen used was temporarily donated by the university anatomy lab.
Ethical Considerations
This study was approved by our institutional review board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
The use of cadaveric specimens during this study followed all ethical guidelines. No living humans or animals were involved in this study.
Statement of Informed Consent
No formal informed consent was required as no living patients were involved in this study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).