
Abstract
Background:
Distal interphalangeal joint (DIPJ) osteoarthritis is a frequent and disabling condition commonly treated with arthrodesis. Traditional fixation methods include headless compression screws (HCSs) and angled compression screws (ACSs), but newly developed snap-off compression pins (SCPs) offer a low-profile alternative. This study compares outcomes of DIPJ arthrodesis using HCS, ACS, and SCP fixation.
Methods:
A retrospective review of DIPJ arthrodesis patients using SCP, HCS, and ACS implants was conducted. Patients aged 18 to 89 years were eligible for inclusion. Those with a proximal interphalangeal joint (PIPJ) arthrodesis or multiple traumas to the ipsilateral arm. The primary outcome was Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) scores at final follow-up, with baseline scores reported for context. Secondary outcomes were peri- and postoperative factors including operative time, tourniquet time, complications, and rate of additional surgeries.
Results:
A total of 149 fusions were analyzed in the study: 18 in the SCP, 112 in the HCS, and 19 in the ACS groups. Baseline characteristics were similar between all groups. The average final QuickDASH score was significantly improved from baseline for the SCP and HCS group, but not for the ACS group. The complication profiles and rates for additional surgery were comparable between all 3 cohorts. Average operative and tourniquet times were comparable between all groups as well.
Conclusion:
Patient-reported outcomes, complications, and additional surgery rates in DIPJ arthrodesis patients treated with SCP are comparable with those in patients treated with HCS or ACS. Snap-off compression pins are therefore a viable option for DIPJ arthrodesis.
Keywords
Introduction
Osteoarthritis (OA) of the hand is most prevalent in the distal interphalangeal joint (DIPJ), affecting nearly 35% of individuals by age 40. 1 Distal interphalangeal joint OA presents with pain, stiffness, joint instability, and eventually deformity in severe cases. 2 Treatment typically starts with nonoperative measures, such anti-inflammatories, corticosteroid injections, and supportive bracing, for relief of pain inhibiting function. 3 When nonoperative management fails, the mainstay surgical treatment is DIPJ arthrodesis with the goal of pain relief, deformity correction, and stabilization of an unstable joint in the hand. 4
Numerous arthrodesis implant options exist, including Kirschner wires (K-wires), and headless compression screw (HCS).4,5 Kirschner wires are a cost-effective alternative; however, they are associated with a higher risk of pin tract infection and external prominence. Wires also do not provide compression across the fusion site. These complications have contributed to the gradual decline in K-wire use for DIPJ arthrodesis. 6 Headless compression screw and a specific curved compression screw, the angled compression screw (ACS; ArcPhix, Acumed, Hillsboro, OR), have both demonstrated successful arthrodesis outcomes, but their sizes are relatively large and can lead to hardware irritation, bone loss, as well as increased hardware prominence and impingement.5,7,8 Despite these complications, HCS is the most common option for arthrodesis due to the compression it gives at the fusion site which is integral for adequate arthrodesis. A novel alternative for DIPJ arthrodesis is the snap-off compression FT pin (SCP; Arthrex, Naples, FL). The SCP is a small-diameter, fully threaded, subcortical implant designed to provide interfragmentary compression through a variable-stepped thread pitch. Compared with large-caliber headless compression screw constructs, the SCP may offer the theoretical advantage of preserving bone stock during implantation while still providing stable fixation for small-joint arthrodesis. However, there is a paucity of studies examining the outcomes of SCP in direct comparison to HCS and ACS, which are both commonly used in DIPJ arthrodesis.
The purpose of this study was to evaluate the outcomes of SCP as an implant compared with HCS and ACS in DIPJ arthrodesis. The primary objective was to compare each implant using the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) scores. The secondary objective was to compare intraoperative and postoperative outcomes, such as operative time, tourniquet time, and rates of complications and additional surgeries. We hypothesized that DIPJ arthrodesis patients implanted with SCP would have superior outcomes across all studied endpoints compared with those with HCS or ACS.
Methods
A retrospective review of all patients who underwent DIPJ arthrodesis using SCP, HCS, or ACS at a single tertiary institution was performed. All surgery was performed by hand fellowship trained surgeons. Prior to the conduct of the study, institutional review board approval was obtained.
Patients treated between January 1, 2020, and October 31, 2024, were identified using a surgical billing database at a single orthopedic surgical institute using Current Procedural Terminology (CPT) code 26860. A total of 198 patients were identified during this period. Inclusion criteria required patients to be in the age range of 18 to 89 and to have undergone DIPJ arthrodesis using either an SCP, HCS, or an angled ACS. Exclusion criteria were the following: inadequate postoperative follow-up (defined as less than approximately 3 months) and the presence of active or concurrent surgical pathology in the ipsilateral upper extremity beyond the DIPJ that could confound outcome assessment. After applying the inclusion and exclusion criteria, a total of 149 DIPJ fusions were included in the study. The SCP group included 15 patients (18 digits), the HCS group included 98 patients (112 digits), and the ACS group included 12 patients (19 digits). Implant selection was determined by the treating surgeon based on clinical judgment, with consideration including surgeon preference, digit size and anatomy, desired fusion angle, and implant characteristics (Figure 1). Angled compression screws were more commonly selected when a greater fusion angle was desired, while SCP were often chosen for smaller digits due to their lower profile. Headless compression screws were used based on surgeon familiarity and availability.
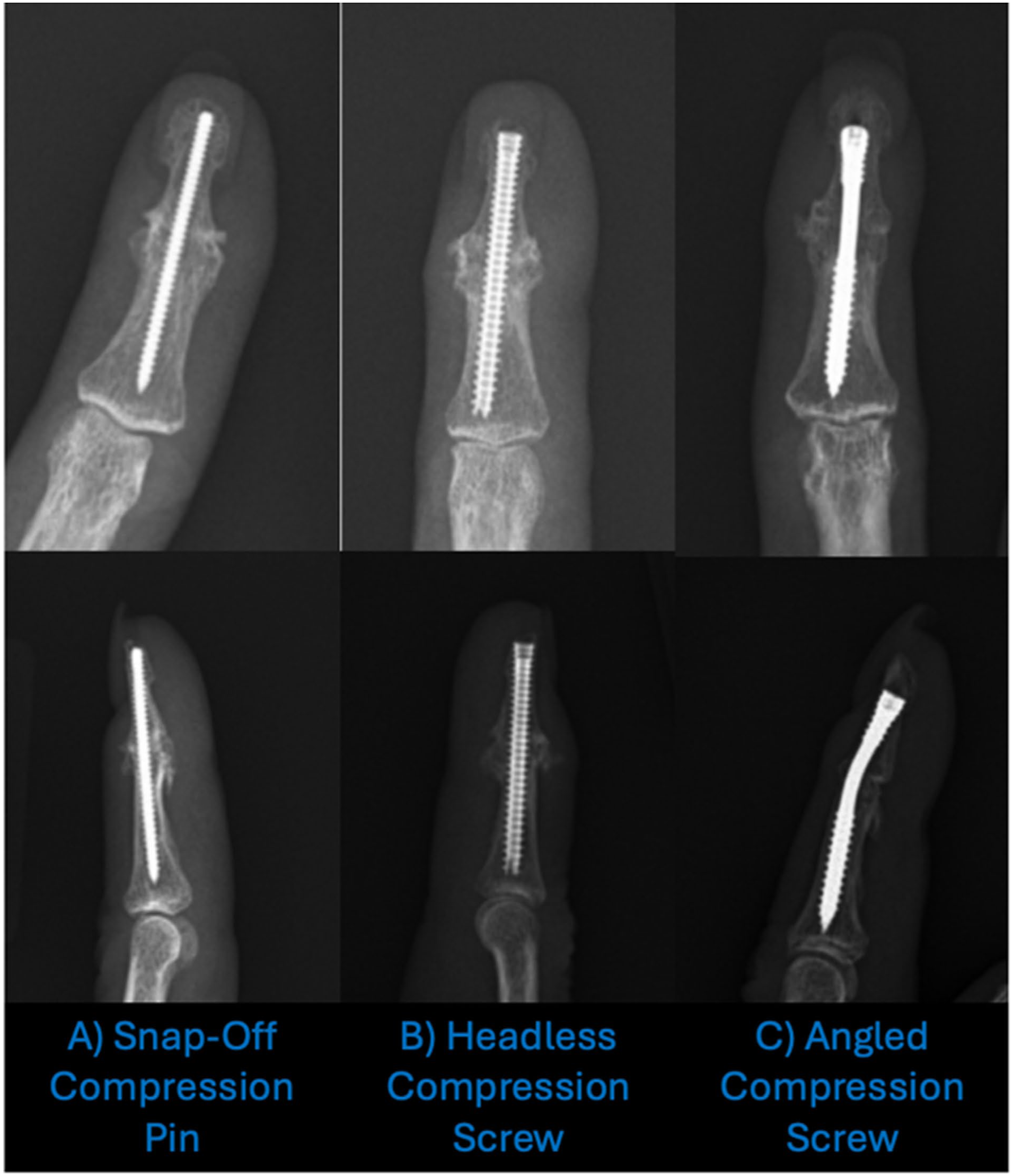
Posteroanterior and lateral radiographs of a patient who underwent right small finger distal interphalangeal joint arthrodesis using: (A) fully threaded snap off compression pin; (B) headless compression screw; and (C) angled compression screw.
Outcome Measures
To assess patient-reported disability following successful DIPJ arthrodesis, the primary outcome measure was the QuickDASH score. The QuickDASH is a validated, region-level measure of patient-reported upper-extremity disability, reflecting the extent to which individuals perceive difficulty performing activities due to their condition. 9 As a disability-based patient-reported outcome measure, the QuickDASH captures patient-perceived limitations in daily activities and was consistently available across this retrospective cohort, allowing for comparison of group-level outcomes before and after surgery. Although not joint-specific and not expected to discriminate between fixation methods once union is achieved, the QuickDASH was used to provide a patient-centered assessment of perceived disability following arthrodesis. Secondary outcomes included operative time, tourniquet time, complications, and the need for additional surgery. Objective outcomes such as union and complications were therefore considered complementary endpoints to contextualize patient-reported disability findings.
Surgical Technique
General Setup and Exposure
The patient is positioned supine with a hand table. Anesthesia and preoperative antibiotics are administered at the discretion of the surgeon. After standard sterile preparation and draping, a dorsal approach to the DIP joint is performed using the surgeon’s preferred incision. The extensor tendon is incised, and the joint is exposed in flexion. Eburnated bone and osteophytes are removed until cancellous bone contact is achieved for arthrodesis preparation.
Implantation of Compression Pins or Screws
We recommend generally removing 2 to 6 mm from the measured length of the screw to allow for compression across the arthrodesis site and avoid penetration of the proximal interphalangeal joint. Prior to insertion, we hold the pin or screw above the skin and take a fluoroscopic image to ensure the correct length.
HCS and ACS
Following preparation with the appropriate drill, the compression screw is advanced across the arthrodesis site in the desired alignment, maintaining subchondral placement to minimize hardware prominence.
Fully Threaded SCP
The bones are held in the appropriate position, the guidewire is removed, and the FT Compression Pin is inserted. The senior author does not routinely drill to preserve more bone. Fluoroscopy is used to confirm correct alignment. Once appropriate positioning of the pin is confirmed with threads buried in a subchondral location, the arthrodesis site is stabilized and the end of the wire of the pin is snapped off. The pin driver should be snapped off with the threaded portion buried within the subchondral bone to a depth of 1 to 3 mm. A counterforce fulcrum point at the snap-off point should be applied with fingers. To date, we have not had any SCP cases requiring removal; however, the manufacturer provides an SCP removal tool if necessary. It is important to ensure that the pin is not buried too deeply because this can create a lever arm and bend the driver part of the pin instead of snapping off at the desired position.
Closure
After final radiographs are taken of the arthrodesis in multiple planes, the wound is irrigated and closed with the suture of choice.
Rehabilitation for DIPJ Arthrodesis
Patients are typically monitored in the clinic for up to six months, if necessary, but they are prescribed a standard 12-week postoperative protocol following DIPJ arthrodesis. During the acute postoperative period (1-2 weeks), patients are instructed to perform a proximal gentle range of motion which includes the metacarpophalangeal joint and proximal interphalangeal joint while avoiding heavy lifting or gripping. Patients are provided with a tip-protector splint fabricated by occupational therapists if their insurance allows. If insurance coverage is insufficient, they are instead given a Stax splint, which they are instructed to use regularly until the 6-week mark. Between 6 and 12 weeks, patients continue progressing in therapy with the goal of improving strength and achieving pain-free ROM in the more proximal joints, and the rest of the affected hand. Beyond the 12-week mark, additional therapy is generally not required, but it may be prescribed if needed to support further patient recovery.
Statistical Analysis and Sample Size Calculation
Averages and standard deviations were reported for continuous variables, and percentages were reported for categorical variables. Given the retrospective nature of the study, a post hoc sample size adequacy analysis was performed to assess whether the available cohort was sufficient to detect a clinically meaningful difference in QuickDASH scores. Prior studies of DIPJ arthrodesis have reported a minimally clinically important difference (MCID) of 15.9 with a standard deviation of approximately 15.0, reflecting the variability of these scores. 10 Preliminary data from the senior author available before database query and analysis, suggested a mean improvement of 15 points in QuickDASH scores with use of the snap-off compression pin, yielding an estimated effect size of d = 0.94. At α = .05 and 80% power, a total sample size of 30 patients (15 per group) was estimated to be sufficient to detect a clinically meaningful difference under these assumptions.
For continuous variables, a 1-way analysis of variance (ANOVA) with a Tukey’s Honestly Significant Difference test for post hoc analysis or a paired 2-tailed t test was used for statistical analysis where appropriate. For categorical data, Fisher exact test was used to determine statistical differences between the groups. Statistical significance set at α = .05.
Results
Demographics
Table 1 summarizes age, operated side, digit distribution, and surgical indications for each group.
Demographics of Patients Who Underwent Distal Interphalangeal Joint Arthrodesis With Fully Threaded Snap Off Compression Pin, Headless Compression Screw, or Angled Compression Screw.
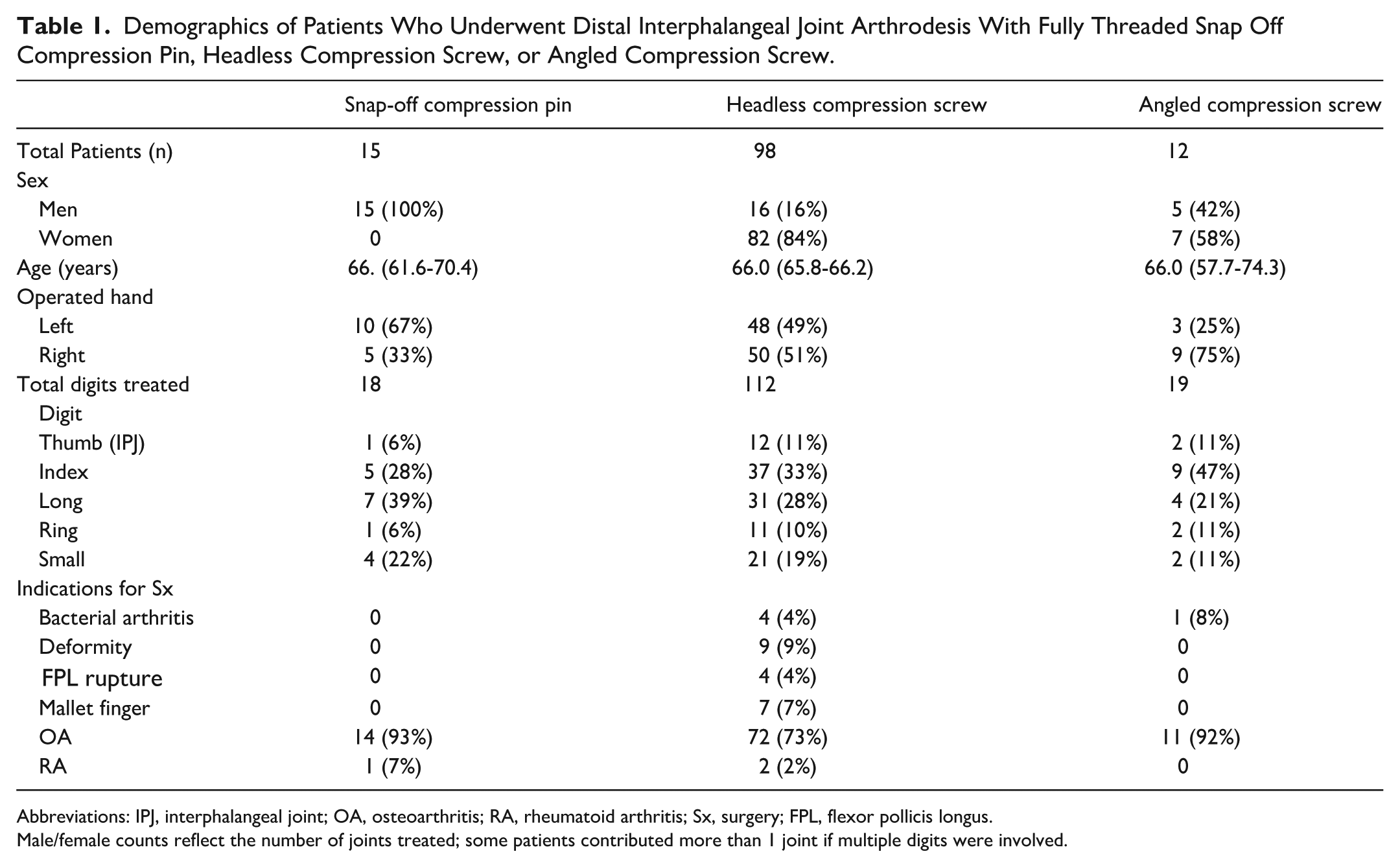
Abbreviations: IPJ, interphalangeal joint; OA, osteoarthritis; RA, rheumatoid arthritis; Sx, surgery; FPL, flexor pollicis longus.
Male/female counts reflect the number of joints treated; some patients contributed more than 1 joint if multiple digits were involved.
Primary Outcome
The SCP and HCS groups demonstrated statistically significant improvements in QuickDASH scores from baseline to final follow-up (ANOVA, p = 0.016), whereas the ACS group did not demonstrate a statistically significant within-group change. Final QuickDASH scores were similar among all three groups, and no statistically significant differences were observed between fixation methods at final follow-up (ANOVA P = .20) (Table 2).
Intra- and Postoperative Outcomes of Patients Who Underwent Distal Interphalangeal Joint Arthrodesis With Snap-Off Compression Pin, Headless Compression Screw, or Angled Compression Screw.
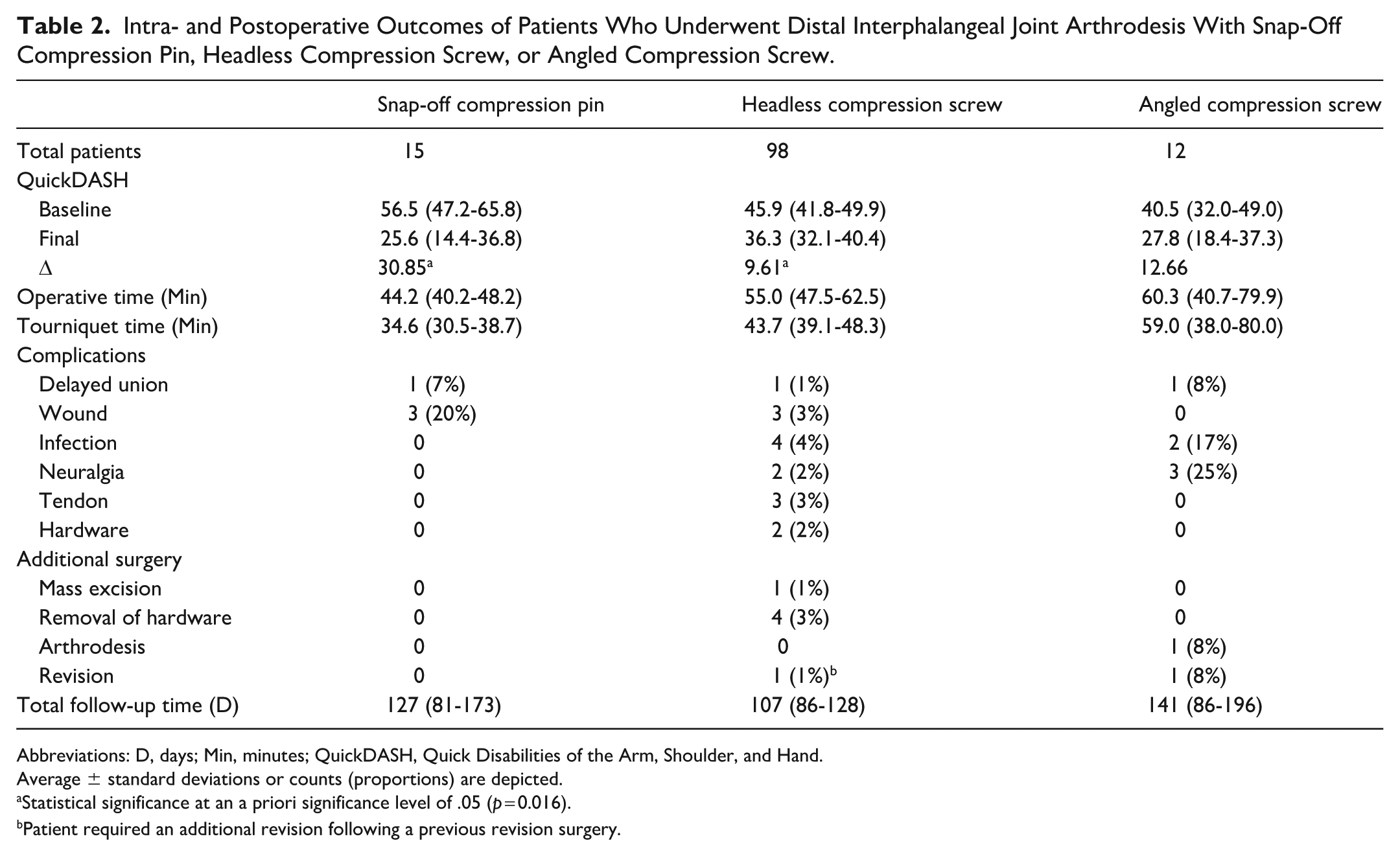
Abbreviations: D, days; Min, minutes; QuickDASH, Quick Disabilities of the Arm, Shoulder, and Hand.
Average ± standard deviations or counts (proportions) are depicted.
Statistical significance at an a priori significance level of .05 (p = 0.016).
Patient required an additional revision following a previous revision surgery.
Secondary Outcome
Operative time and tourniquet time varied across fixation methods, with shorter mean times observed in the SCP group and longer mean operative times in the ACS group (Table 2). Postoperative complications and the need for additional surgery were observed in all groups and are summarized descriptively in Table 2.
Discussion
Distal interphalangeal joint arthrodesis using HCS is a commonly reported contemporary fixation method, with multiple studies demonstrating high fusion rates and reliable outcomes, although the optimal fixation method and implant choice have not been definitively established.4,11,12 However, the relatively larger profile of HCS and ACS implants within the confined distal phalanx space may contribute to implant prominence. This is particularly true of the ACS as there is currently only one size that is 3 mm in diameter and one length. These implant limitations impart restriction on use based on the size of the patient’s distal phalanx, especially the more ulnar digits. Unfortunately, the ulnar digits are where it is more beneficial to have a flexed DIP joint fusion construct. Newer, small-caliber implants such as the SCP are designed to minimize implant profile, though limited data exist evaluating their clinical outcomes (Figure 1). In this retrospective cohort, patients undergoing DIPJ arthrodesis with SCP, HCS, or ACS demonstrated comparable final patient-reported disability in the form of QuickDASH scores, as well as similar perioperative and postoperative findings. No fixation method was associated with clearly superior patient-reported outcomes following successful arthrodesis.
Compression at the arthrodesis site is essential for adequate stability and bone contact for fusion. The SCP is a small-diameter, fully threaded, subcortical implant designed to provide compression through a variable-stepped thread pitch. This may have a theoretical advantage of preserving bone stock during implantation while still providing stable fixation for small-joint arthrodesis. The senior author has found ease of implantation of the SCP without the need for bone drilling, and this may also lead to better fixation and preserved bone for fusion. While the larger HCS and ACS are designed for compression, there is more bone loss in the implantation of these screws, and this may affect the amount of bone left for arthrodesis and also create a larger screw tract with less fixation in often already low bone density.
In this study, improvement in QuickDASH scores was observed across fixation methods, with the SCP group demonstrating a larger mean change from baseline. However, interpretation of change scores must acknowledge the substantial variability in baseline disability and the region-level nature of the QuickDASH. Although average improvements in the SCP group exceeded the published MCID and substantial clinical benefit (SCB) thresholds for QuickDASH, these patient-reported outcome thresholds reflect perceived change rather than normalization of function and should not be equated with a return to “normal” upper-extremity status.10,13 Final QuickDASH scores were similar across all three fixation methods, indicating comparable patient-reported disability at final follow-up. These findings suggest that when union is achieved, patient-reported disabilities following DIPJ arthrodesis is largely comparable regardless of fixation strategy. The SCP group achieved similar final outcomes despite having higher baseline disability on average, which may reflect differences in patient characteristics rather than implant performance.
Of note, baseline QuickDASH scores in this cohort were relatively high, underscoring an important limitation of using a region-level disability measure for isolated joint disease. Because the QuickDASH score captures patient-reported disability across the entire upper extremity, it has been shown to yield elevated scores even in localized hand conditions such as thumb carpometacarpal arthritis.14,15 These findings highlight that QuickDASH scores may reflect perceived disability influenced by factors beyond the index joint, including task avoidance, symptom burden, and comorbid upper-extremity pathology. The extent to which baseline disability was attributable to DIPJ pathology versus unrelated conditions cannot be determined in this study. Therefore, absolute QuickDASH values in this study should be interpreted with caution, and emphasis should be placed on final scores and group-level comparability rather than assumptions regarding the origin of baseline disability.
Published data comparing operative and tourniquet times among fixation methods for DIPJ arthrodesis are limited. In the present study, operative and tourniquet times varied across fixation methods and are summarized descriptively in Table 2. Given the limitations of this study, no formal comparative conclusions can be drawn regarding intraoperative time differences between implants.
In this study, complications and additional surgeries were observed across all three DIPJ arthrodesis implants and are reported descriptively. The SCP group experienced three wound complications postoperatively, which were resolved with wound care treatment. One SCP patient experienced a delayed union, which eventually resolved as confirmed by computed tomography. Of note, this patient received an adjunct bone stimulator in the process of recovery; however, the impact of bone stimulators on fusion outcomes is still inconclusive. 16 In this study, no additional surgery was required for the SCP group. The HCS group also exhibited delayed union and wound complications, along with infection, neuralgia, tendon-related problems, and hardware complications. In some cases, these complications necessitated further surgical intervention for hardware removal and mass excision, with one patient requiring multiple subsequent revision surgeries. These findings are consistent with reported complications in the literature, where hardware irritation and tendon-related issues sometimes require additional secondary surgery. Kocak et al 17 reported on 64 cases of HCS DIPJ arthrodesis, in which 8% of patients required removal of symptomatic hardware. The ACS group experienced delayed union, infection, and neuralgia complications as well, with two patients requiring an additional surgery for arthrodesis or revision. Given the small number of events in a small sample size, along with the limitations of the study design, no conclusions can be drawn regarding differences in complication rates or mechanisms between fixation methods. Accordingly, these findings should be interpreted as descriptive observations rather than evidence of differential implant-related risk. The snap-off compression pin represents an alternative fixation option for DIPJ arthrodesis. In this study, patient-reported disability outcomes, operative characteristics, and complication profiles were similar across fixation methods.
Limitations
This study is limited by its retrospective design and a fixed cohort, precluding formal prospective sample size planning. Consequently, the study was powered only to detect large between-group differences in the primary outcome, and smaller but potentially clinically meaningful effects, as well as differences in secondary outcomes, may not have been identified due to insufficient power. Group sizes were unbalanced, and implant selection was based on surgeon judgment rather than randomization, introducing the potential for selection bias and confounding by indication, which limits the generalizability of the findings. As a result, comparable outcomes across fixation methods should not be interpreted as evidence of equivalence between implants but rather may reflect appropriate implant selection tailored to individual patient and digit characteristics by experienced surgeons. In addition, the QuickDASH is a region-level outcome measure influenced by factors beyond isolated DIPJ pathology, including psychosocial variables such as mental health, which were not captured and represent an important unmeasured confounder. Further studies using joint-specific outcome measures and larger, balanced cohorts may better characterize differences between fixation methods.
Conclusion
Patient-reported outcomes, complications, and additional surgery rates in DIPJ arthrodesis patients treated with SCP are comparable with those in patients treated with HCS or ACS. Snap-off compression pins are therefore a viable option for DIPJ arthrodesis.
Footnotes
Ethical Considerations
Prior to the initiation and conduct of this study, approval was obtained from the local Institutional Review Board (IRB) (IRB no. STUDY008501).
Consent for Publication
After IRB approval, a waiver of informed consent was granted because this retrospective study involved only the review of existing medical records, posted no more than minimal risk to participants, and all data were collected from pre-existing records, so written informed consent for participation and publication was not required.
Author Contributions
Every author contributed to the work with all aspects of the ICMJE Authorship Criteria.
Funding
The authors would like to acknowledge Tampa General Hospital, Department of Orhtopaedic Surgery for fudning support for this research.
Declaration of Conflicting Interests
This project was supported by Tampa General Hospital, Department of Orthopaedic Surgery.
Data Availability Statements
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).