
Abstract
Background:
In severe cases of carpal tunnel syndrome (CTS), compound muscle action potential (CMAP) and sensory nerve action potential (SNAP) may be absent on preoperative nerve conduction studies (NCS), reflecting advanced nerve damage. Although clinical improvement after carpal tunnel release is common, early electrophysiological recovery in this subgroup and its predictive factors remain poorly defined. This study investigated reappearance of CMAP and SNAP within 3 months after surgery and explored predictors of recovery.
Methods:
This study included 53 patients with CTS who demonstrated absent CMAP and/or SNAP preoperatively and underwent open carpal tunnel release. All patients had NCS performed within 3 months before surgery and again at 3 months postoperatively. Patients were categorized into recovery and nonrecovery groups based on reappearance of CMAP and/or SNAP. Demographic variables, disease duration, and laboratory parameters were compared between groups. A multivariable logistic regression analysis was performed to identify independent predictors of electrophysiological recovery.
Results:
At 3 months postoperatively, a subset of patients demonstrated recovery of CMAP and/or SNAP. In the multivariable analysis, younger age (P < .01) and higher body weight (P = .04) were independently associated with SNAP recovery, whereas age showed the strongest association with CMAP recovery but did not reach statistical significance. Symptom duration and metabolic laboratory parameters were not independently associated with recovery.
Conclusions:
Early electrophysiological recovery is achievable even in severe cases of CTS with absent preoperative nerve potentials. Younger age is the strongest predictor of early recovery. These findings provide clinically relevant prognostic information for patients undergoing surgical treatment for advanced CTS.
Keywords
Introduction
Carpal tunnel syndrome (CTS) is the most prevalent peripheral entrapment neuropathy and constitutes a major source of hand numbness, pain, and disability worldwide. Epidemiological studies indicate that the lifetime risk of CTS is substantial, particularly among older adults and women, reflecting both occupational and systemic contributors to disease susceptibility.1-3 Carpal tunnel syndrome results from compression of the median nerve within the rigid confines of the carpal tunnel, leading initially to segmental demyelination and, in advanced stages, secondary axonal degeneration. As disease severity increases, nerve conduction studies (NCS)—the diagnostic gold standard—demonstrate progressively reduced amplitudes and prolonged latencies, and in the most severe cases, compound muscle action potential (CMAP) and sensory nerve action potential (SNAP) may be entirely absent. 4
Surgical decompression through carpal tunnel release is effective in symptom relief and is considered the definitive treatment for moderate to severe CTS. Prior studies have reported improvements in clinical and electrophysiological measures after surgery, especially when performed early in the disease course.5-7 However, the prognosis for patients presenting with absent CMAP or SNAP remains uncertain. Although symptomatic improvement is common even in high-grade CTS, the extent and timing of neurophysiological recovery—particularly the re-emergence of measurable nerve potentials—are poorly defined. Some reports have examined postoperative recovery in this subgroup. These studies suggest that postoperative recovery is variable and may be related to preoperative neurological severity, including the extent of axonal involvement.8,9
Age, chronicity of compression, and systemic metabolic factors have been proposed as determinants of postoperative recovery in CTS. Younger individuals generally demonstrate superior peripheral nerve regeneration, whereas prolonged compression can induce irreversible intraneural fibrosis and impair axonal regrowth.10,11 Systemic factors such as diabetes, dyslipidemia, and renal dysfunction are increasingly recognized as modifiers of peripheral nerve health and may influence both susceptibility to CTS and the biological capacity for postoperative recovery.12-14 Despite these insights, no prior study has comprehensively evaluated clinical and biochemical predictors of early electrophysiological recovery specifically among patients who initially lack measurable nerve potentials. A clearer understanding of such predictive factors would be highly valuable for surgical decision-making, patient counseling, and prognosis. Identifying which patients are likely to exhibit early electrophysiological recovery after decompression may also provide insights into the pathophysiological thresholds beyond which nerve damage becomes irreversible.
Accordingly, the aim of the present study was to determine whether CMAP and SNAP responses reappear within 3 months after carpal tunnel release in patients with severe CTS who demonstrate absent preoperative electrophysiological responses. We also sought to compare demographic, clinical, and metabolic variables between patients who experienced recovery and those who did not. We hypothesized that younger age, shorter disease duration, and favorable systemic characteristics would be associated with a higher likelihood of early neurophysiological recovery.
Materials and Methods
The study was performed in accordance with the Declaration of Helsinki and approved by the institutional review board. Reporting followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for observational research. This retrospective observational study included 53 patients (15 men, 38 women; mean age, 69.8 years; range, 44-88 years) with CTS who underwent open carpal tunnel release. Eligible patients met the following criteria: (1) absence of a detectable CMAP of the abductor pollicis brevis and/or absence of a SNAP on preoperative NCS; and (2) availability of NCS performed within 3 months before surgery and again at 3 months postoperatively. Patients with chronic renal failure or systemic neuropathies were excluded. The diagnosis of CTS was based on characteristic clinical symptoms and delayed NCS. Typical symptoms included hand numbness and pain, worsening in the early morning or at night, exacerbation with hand use, sensory deficits in the median nerve distribution (particularly ring-finger splitting), positive Phalen’s and/or Tinel’s sign, and muscle weakness or atrophy in the abductor pollicis brevis and thenar muscles. The strength of the abductor pollicis brevis muscle was evaluated using manual muscle testing (MMT), and the grade was recorded for each patient. Based on patient-reported postoperative symptom changes, recovery status was classified into 4 categories according to previously defined criteria. 15 Excellent was defined as complete resolution or marked improvement of pain and numbness without any limitation in daily activities. Good was defined as partial improvement of pain and numbness with mild limitation in daily activities. Fair was defined as no noticeable change in symptoms compared with the preoperative condition. Poor was defined as worsening of pain or numbness compared with the preoperative status.
Clinical and Laboratory Data
Baseline demographic and clinical variables were extracted from structured electronic medical records. Collected parameters included age, sex, height, weight, and body mass index (BMI). Laboratory measurements obtained within 3 weeks prior to surgery included hemoglobin A1c (HbA1c), estimated glomerular filtration rate (eGFR), total cholesterol (T-chol), and serum albumin (Alb), which provided metabolic and nutritional background data for subsequent subgroup analyses.
Disease duration was calculated in months, based on the time between the patient-reported onset of initial symptoms—such as numbness, tingling, or functional decline—and the date of surgery. This estimate was derived from standardized interviews conducted during the preoperative assessment and cross-referenced with previous clinical documentation when available.
Electrophysiological Assessment
Electrophysiological studies were performed using a standard electromyography system (Neuropack MEB-2208, Nihon Kohden Co.). All studies were conducted by a clinical technician who was blinded to clinical symptoms. Room temperature was maintained at 27 °C, and in patients with cold hands, the hands were warmed to bring the skin temperature closer to room temperature. For the motor conduction study, CMAPs of the abductor pollicis brevis muscle were recorded (Figure 1A). Stimulation was applied 7 cm proximal to the recording electrode. For the sensory conduction study, a recording electrode was placed on the index finger, and a stimulating electrode was placed 14 cm proximal to the recording site (Figure 1B). The median nerve was examined antidromically, and SNAPs of the index finger were recorded. Latencies and amplitudes of both CMAPs and SNAPs were measured, and absent responses were categorized as unmeasurable.
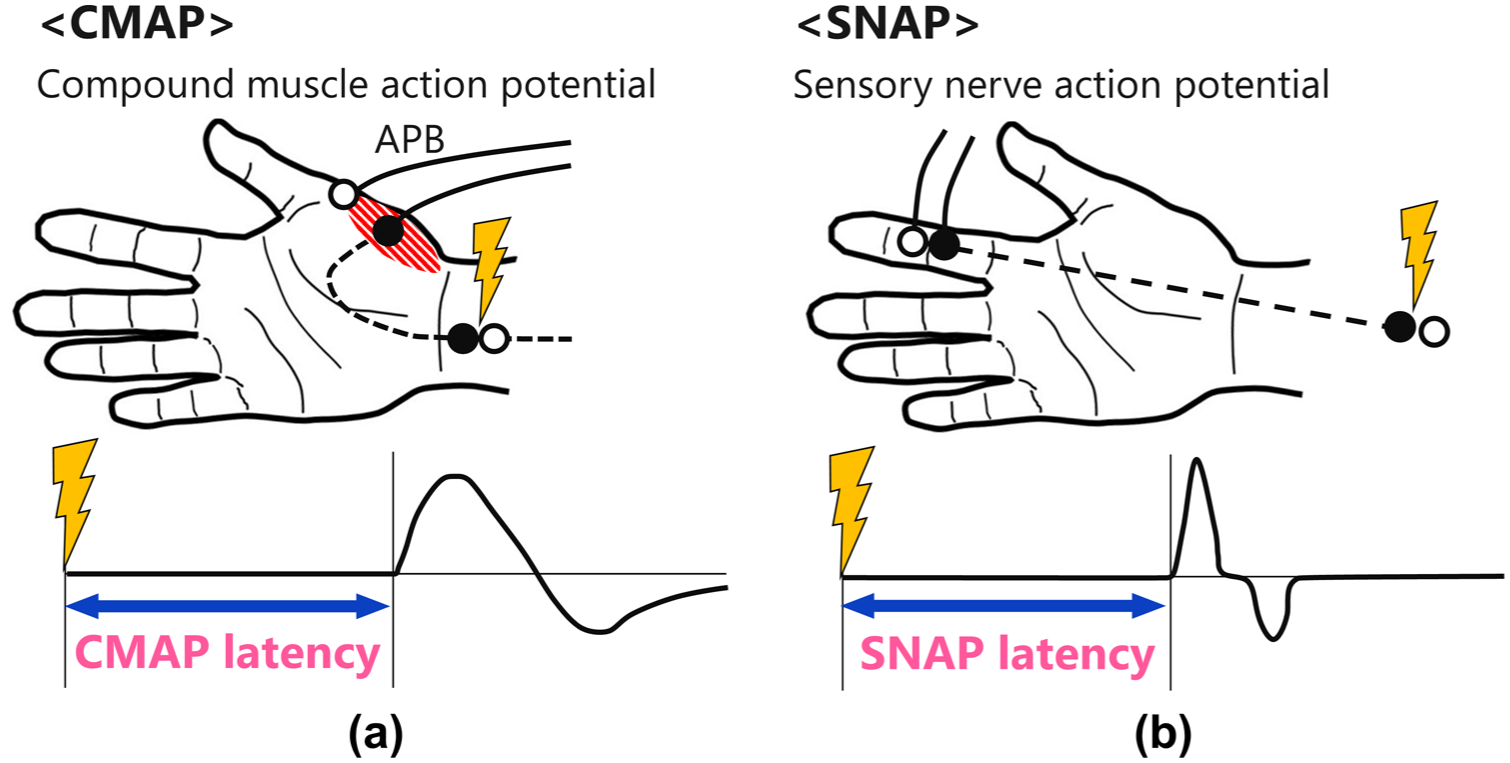
Methods for nerve conduction study.
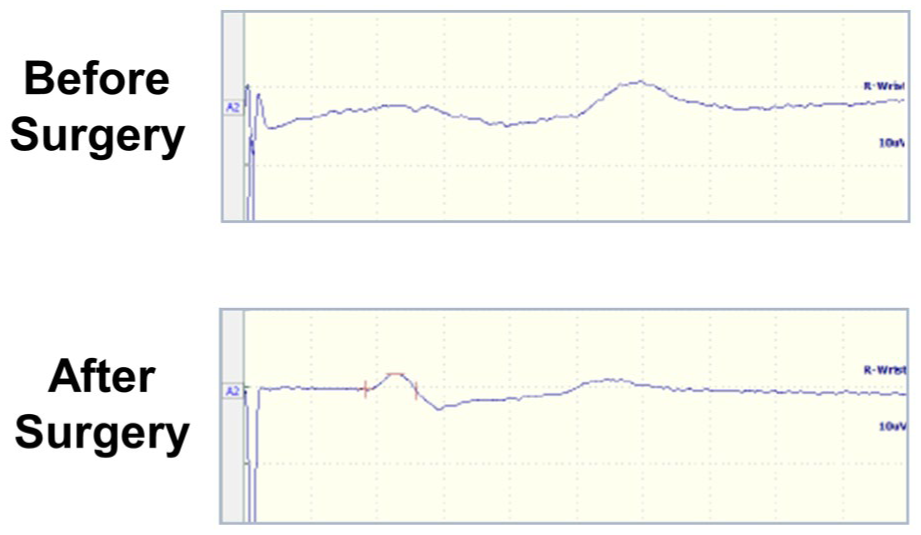
Representative waveforms in the recovery case. An example of recovery case of sensory nerve action potentials.
At 3 months after surgery, all patients underwent repeat NCS using identical recording protocols. Based on the presence or absence of recovered responses, patients were categorized into 2 outcome groups: (1) Recovery group—presence of detectable CMAP and/or SNAP at the 3-month postoperative evaluation; (2) Nonrecovery group—persistently absent CMAP and SNAP at 3 months. Motor and sensory outcomes were analyzed independently to account for potential differences in recovery patterns between motor and sensory fibers.
Statistical Analysis
All continuous variables were summarized as mean and standard deviation. Comparisons between the electrophysiological recovery and nonrecovery groups were made using unpaired t-tests for continuous data. For clinical outcomes, patients with excellent or good results were classified as the clinical recovery group, whereas those with fair or poor results were classified as the nonclinical recovery group. Categorical variables, including sex distribution (male/female) and clinical outcome categories, were compared using the chi-square test.
To identify independent predictors of electrophysiological recovery, a multivariable logistic regression analysis was performed. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to assess the strength of association between each variable and electrophysiological recovery. Variables included in the multivariable model were selected based on clinical relevance and results of univariate analysis.
Three patients underwent bilateral carpal tunnel release at different time points during the study period. Because each wrist met the inclusion criteria independently and electrophysiological outcomes were assessed separately, each wrist was treated as an independent analytical unit.
A P-value < .05 was considered to indicate statistical significance. Statistical analyses were performed using SPSS (v31.0, IBM Corp.).
Results
A total of 54 patients completed both preoperative and 3-month postoperative NCS and were included in the final analysis. Among them, 18 wrists of 18 patients exhibited an absent CMAP preoperatively, and 52 wrists of 49 patients demonstrated an absent SNAP, including 2 patients who contributed bilateral wrists treated at different time points. Postoperative testing allowed classification into recovery and nonrecovery groups for both motor and sensory evaluations.
CMAP Recovery
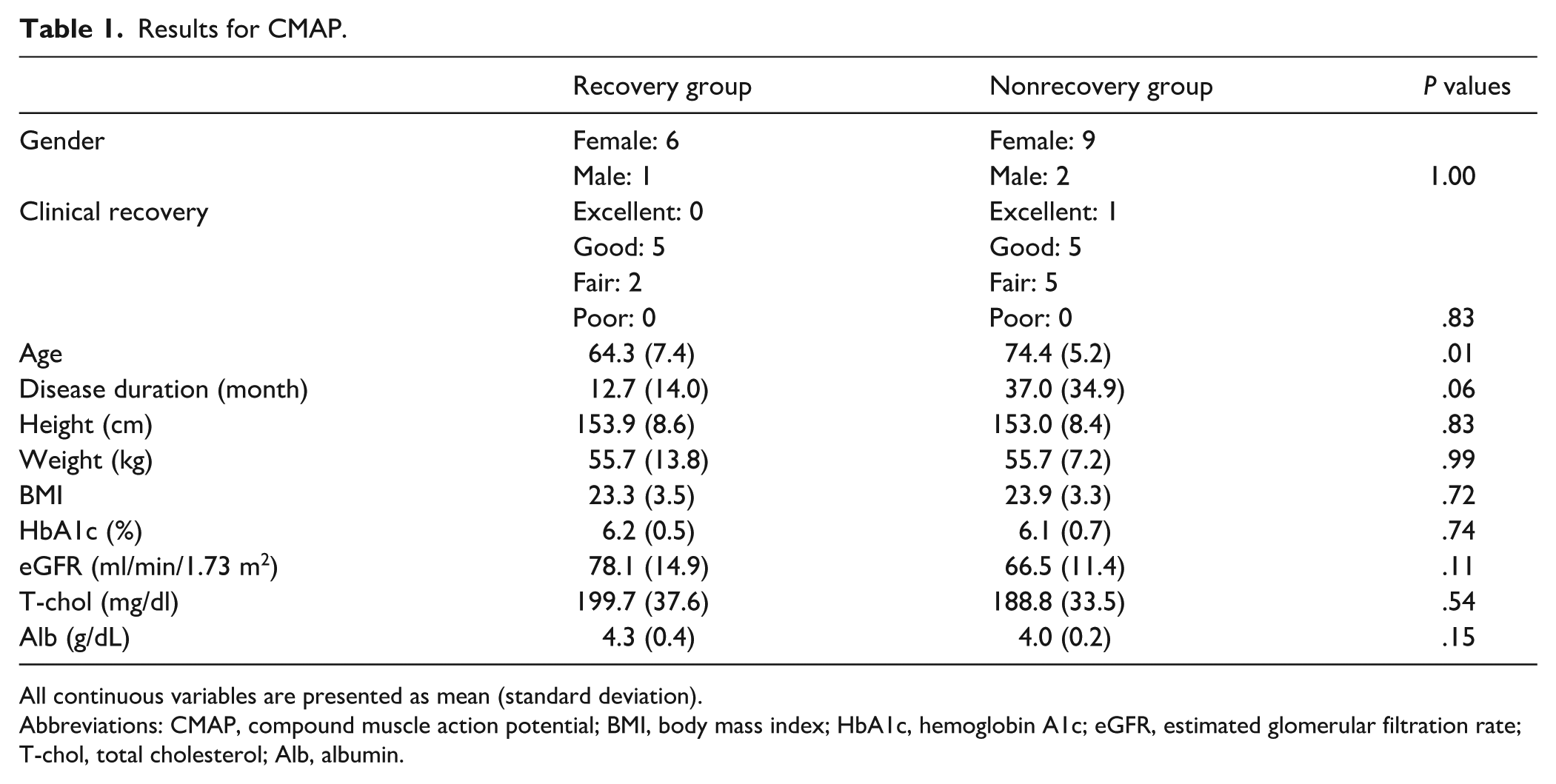
Table 1 shows the results for CMAP. Patients who demonstrated postoperative CMAP recovery were notably younger than those who did not recover. The mean age in the recovery group was 64.3 ± 7.4 years, compared with 74.4 ± 5.2 years in the nonrecovery group, a statistically significant difference (P = .01). Disease duration also tended to differ between groups: Patients who recovered had experienced symptoms for an average of 12.7 ± 14.0 months, whereas those without recovery had a substantially longer duration of 37.0 ± 34.8 months. Although this difference did not reach statistical significance (P = .06), the trend suggested that a shorter period of nerve compression may favor electrophysiological improvement.
Results for CMAP.
All continuous variables are presented as mean (standard deviation).
Abbreviations: CMAP, compound muscle action potential; BMI, body mass index; HbA1c, hemoglobin A1c; eGFR, estimated glomerular filtration rate; T-chol, total cholesterol; Alb, albumin.
No meaningful differences were observed in BMI, HbA1c, eGFR, or serum Alb between patients with and without CMAP recovery. These findings indicate that age and chronicity of symptoms, rather than metabolic or nutritional factors, were more closely associated with the likelihood of early motor nerve response recovery.
SNAP Recovery
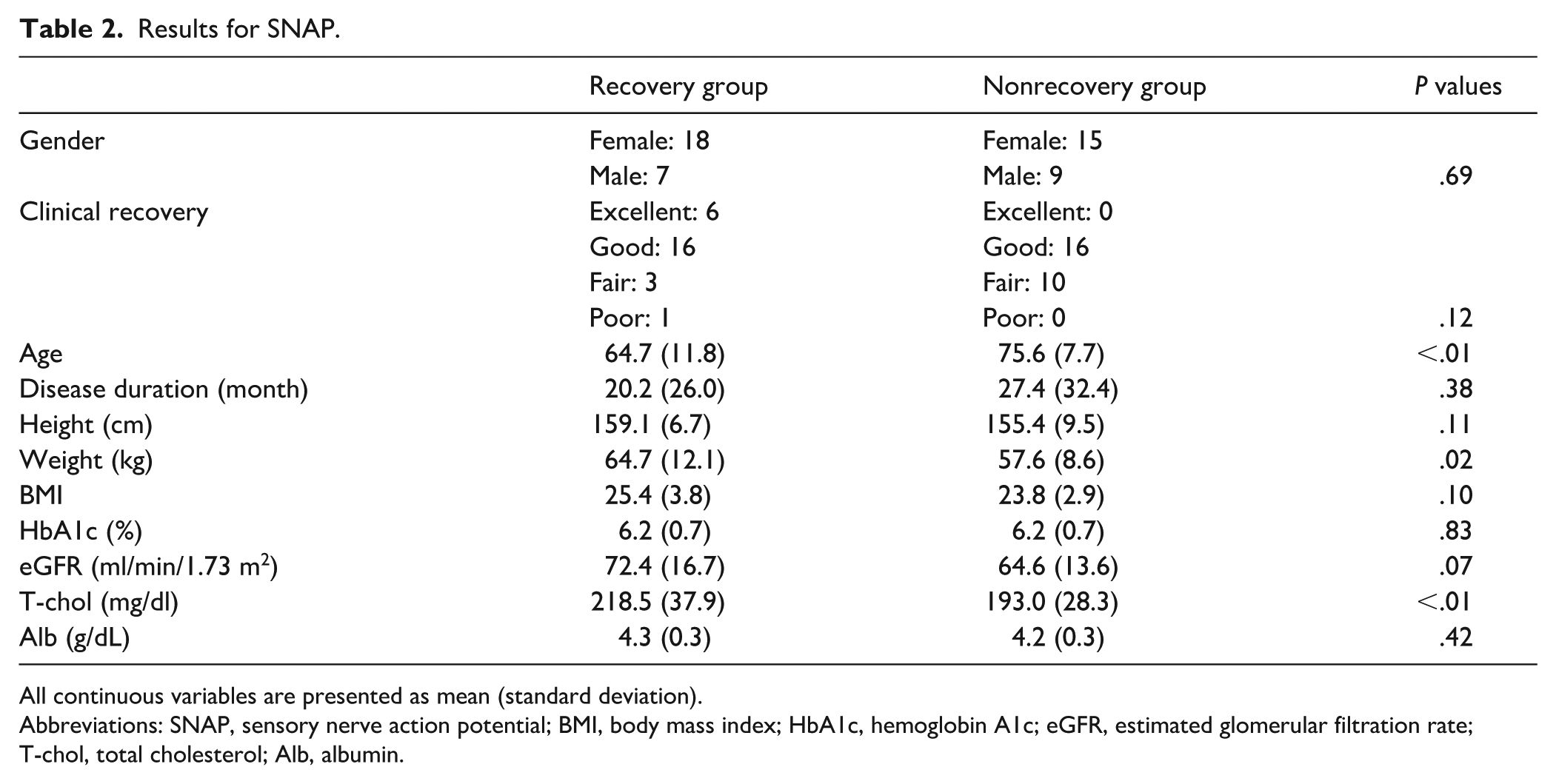
Table 2 shows the results for SNAP. A similar pattern was observed for sensory recovery. Patients who regained measurable SNAP responses were significantly younger than those who did not, with mean ages of 64.7 ± 11.8 years and 75.6 ± 5.7 years, respectively (P < .01). In contrast to the CMAP findings, body weight showed a significant association with SNAP recovery: Patients in the recovery group weighed an average of 64.7 ± 12.1 kg, compared with 57.6 ± 8.6 kg in the nonrecovery group (P = .02). Total cholesterol levels were also higher in the recovery group, although this difference did not reach statistical significance. As with CMAP, BMI, HbA1c, eGFR, and Alb did not differ substantially between groups.
Results for SNAP.
All continuous variables are presented as mean (standard deviation).
Abbreviations: SNAP, sensory nerve action potential; BMI, body mass index; HbA1c, hemoglobin A1c; eGFR, estimated glomerular filtration rate; T-chol, total cholesterol; Alb, albumin.
Summary of Predictive Patterns
Across both motor and sensory evaluations, age consistently emerged as the most influential predictor of electrophysiological recovery at 3 months after surgery. Although the electrophysiological recovery group showed a higher proportion of favorable clinical outcomes compared with the nonrecovery group, this difference was not statistically significant (P = .12). Younger patients were more likely to regain measurable nerve potentials. A shorter disease duration appeared to support CMAP recovery, strengthening the clinical notion that prolonged nerve compression may lead to irreversible axonal loss. Conversely, metabolic parameters showed little relationship to recovery, although the associations observed for body weight and cholesterol in SNAP recovery suggest possible systemic influences on sensory nerve regeneration.
A multivariable logistic regression analysis was performed to identify independent predictors of electrophysiological recovery. In the CMAP model, younger age showed the strongest association with recovery (OR 0.73 per year increase, P = .06), although this did not reach statistical significance, and symptom duration was not independently associated with recovery (P = .73). In contrast, the SNAP model demonstrated that younger age (OR 0.90 per year increase, P < .01) and higher body weight (OR 1.09 per kg increase, P = .04) were independently associated with recovery, whereas symptom duration was not significant (P = .52).
Discussion
The present study examined early electrophysiological recovery after carpal tunnel release in patients with severe CTS characterized by absent CMAP or SNAP responses preoperatively. Our findings indicate that measurable motor and sensory nerve potentials can reappear as early as 3 months after the surgery, even among patients with the most advanced electrophysiological deficits. Recent systematic reviews and cohort studies indicate that decompression can produce meaningful clinical and electrodiagnostic improvement in severe CTS, although postoperative recovery is heterogeneous and influenced by preoperative nerve severity.8,16 In this context, previous work has emphasized the prognostic value of a detailed preoperative neurophysiological assessment. It has been demonstrated that needle electromyography findings in the abductor pollicis brevis muscle correlate with postoperative muscle strength recovery in severe CTS, highlighting that even in advanced disease, residual neural integrity may predict postoperative functional restoration. 17
Across both CMAP and SNAP outcomes, younger age consistently predicted recovery, with patients in the recovery groups being nearly a decade younger than those without recovery. This aligns with recent clinical studies showing slower symptomatic and electrodiagnostic improvement in elderly patients following carpal tunnel release.18,19 These findings are further supported by contemporary peripheral nerve biology research demonstrating age-related declines in Schwann-cell repair capacity, axonal sprouting potential, and myelin remodeling efficiency. 20
For motor recovery, shorter disease duration showed a clear trend toward association with CMAP reappearance. Although not statistically significant in this cohort, the large difference in mean duration strongly suggests that prolonged compression leads to progressive axonal degeneration and intraneural fibrosis, limiting early recovery. This interpretation is consistent with prior reports showing that severe preoperative neurophysiological abnormalities, including denervation changes on needle electromyography, are associated with poorer postoperative motor recovery in advanced CTS.8,17,21 This supports the clinical recommendation that surgical intervention should not be delayed once motor deficits become evident.
In contrast, sensory recovery showed an unexpected association with higher body weight and elevated cholesterol. Contemporary epidemiological and genetic studies consistently show that obesity, dyslipidemia, and metabolic syndrome increase the risk of developing CTS, as well as recurrence after surgery.22-24 The present findings therefore diverge from classical risk-factor patterns. One hypothesis is that greater lipid availability may support sensory myelin repair, 25 though residual confounding—nutritional status, inflammatory pathways, or unmeasured comorbidities—cannot be excluded. Interestingly, canonical metabolic markers such as HbA1c, eGFR, and serum Alb—commonly associated with peripheral neuropathy—did not differ between recovery groups. Recent large clinical datasets show mixed effects of diabetes and systemic metabolic dysfunction on postoperative outcomes, suggesting that once CTS reaches an advanced stage, local mechanical factors and intrinsic nerve regenerative capacity may exert greater influence on early electrophysiological recovery.9,26,27
The multivariable analysis demonstrated that younger age was independently associated with SNAP recovery, whereas in the CMAP model, age showed the strongest association but did not reach statistical significance. These findings suggest that age plays an important role in early neural recovery following decompression. Higher body weight was also independently associated with SNAP recovery, while symptom duration was not independently significant after adjustment. Overall, age appears to be an important prognostic factor in severe CTS.
Differences observed between CMAP and SNAP recovery are consistent with physiological distinctions between motor and sensory fibers. Sensory fibers may recover earlier due to relatively preserved axonal pathways and shorter regeneration distances, whereas motor recovery requires successful neuromuscular junction reinnervation—typically a slower process. Recent electrodiagnostic studies confirm that sensory parameters often improve earlier than motor parameters after decompression.28,29
An important consideration is the relationship between electrophysiological and clinical recovery. In this study, the SNAP recovery group showed a higher proportion of favorable clinical outcomes, although the difference was not statistically significant at 3 months. This suggests that electrophysiological recovery may precede measurable clinical improvement. Because neural regeneration and functional recovery may occur at different rates, electrophysiological findings at this early time point should be interpreted as indicators of early neural recovery rather than definitive evidence of clinical recovery. Longer follow-up is needed to clarify the relationship between electrophysiological and functional outcomes.
This study has several limitations. Its retrospective design and modest sample size limit the ability to fully disentangle the effects of systemic metabolic factors, particularly in the context of advanced disease. The relatively small sample size, particularly in the CMAP subgroup, limits statistical power and increases the risk of type II error. Therefore, nonsignificant findings should be interpreted cautiously, as true associations may not have been detected. Larger prospective studies are required to confirm independent predictors of early electrophysiological recovery. In addition, 3 patients contributed bilateral wrists to the SNAP analysis. Although these procedures were performed at different time points, potential within-subject correlation cannot be fully excluded. Finally, the 3-month follow-up period captures only early postoperative changes and does not reflect longer-term recovery trajectories; prior studies suggest that electrophysiological and clinical improvement, especially in motor function, may continue for 6-12 months after decompression.
In summary, this study demonstrates that electrophysiological recovery is achievable in a notable proportion of patients with severe CTS presenting with absent CMAP or SNAP responses. Among all variables examined, younger age was the strongest predictor of recovery, while shorter disease duration favored CMAP restoration. The associations between sensory recovery and metabolic factors highlight potential systemic influences that merit further prospective research. These findings enhance our understanding of recovery processes following carpal tunnel release and have clinical relevance as prognostic information to be shared with patients when discussing treatment decisions and postoperative expectations.
Footnotes
Ethical Considerations
The study was performed in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Tokyo Medical University. Reporting followed the STROBE guidelines for observational research.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
Informed consent was obtained from all individual participants included in the study.
Author Contributions
YY: research design, acquisition and analysis of data, and wrote the manuscript. RA: acquisition and analysis of data and revise the manuscript. TI: acquisition and analysis of data and revise the manuscript. YT: acquisition and analysis of data and revise the manuscript. SI: acquisition and analysis of data and revise the manuscript. AI: acquisition and analysis of data and revise the manuscript. YH: acquisition and analysis of data and revise the manuscript. All authors were fully involved in the study and approved the final version of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Zimmer Biomet Holdings, Inc. These funds were not involved in data collection, data analysis, or the preparation or editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained when necessary.