
Abstract
Background:
Carpometacarpal (CMC) osteoarthritis can be associated with metacarpophalangeal (MCP) joint hyperextension. During CMC arthroplasty, surgeons may or may not choose to treat MCP hyperextension. This study aims to elucidate the preferences of surgeons regarding concurrent treatment of MCP hyperextension during CMC arthroplasty and identify factors that influence their decision-making.
Methods:
A survey inquiring about practice and training characteristics, CMC arthroplasty volume and type, concurrent MCP procedure and criteria for intervention, and perceived outcomes was formulated by the authors. It was distributed to orthopedic and plastic surgery fellowship-trained hand surgeons via REDCap.
Results:
Surveys were sent to 478 surgeons, and 73 responded (15.3% response rate). Academia accounted for 60.3% of the respondents, followed by 34.2% in hybrid private/academic practice. Length of practice ranged from <5 years (21.9%) to >30 years (19.2%). Most surgeons (69.0%) performed <30 CMC arthroplasties per year, and the most common procedure of choice was trapezium resection and suspensionplasty (63.9%). 61.6% of respondents reported performing an MCP procedure at the time of CMC arthroplasty. During residency and fellowship, 43.8% and 68.1% were taught to perform the technique, respectively. 56.9% continue to teach their trainees to perform it.
Conclusions:
Significant heterogeneity exists with regard to the practice, indications, and perceived outcomes of performing a concurrent MCP procedure during CMC arthroplasty. While a substantial proportion of training programs teach the technique, its use varies based on surgeon preference. Larger and comparative studies examining outcomes are necessary to standardize the treatment algorithm for CMC osteoarthritis with MCP hyperextension.
Keywords
Introduction
Although the prevalence of carpometacarpal (CMC) osteoarthritis is estimated to be 17.3% among elderly patients aged 50 to 89, the prevalence of this condition is expected to increase in light of the aging population.1,2 Given the essential role of the thumb in hand function, CMC osteoarthritis can be particularly debilitating.3,4 Conservative treatments include hand therapy, corticosteroid injections, and bracing. 5 Surgical intervention is typically considered when these modalities fail, with options such as trapeziectomy, arthroplasty, and arthrodesis.6,7
Carpometacarpal osteoarthritis can be accompanied by hyperextension of the metacarpophalangeal (MCP) joint. 8 The indications and approach to addressing MCP hyperextension remain controversial, and the decision is often guided by surgeon preference. Moineau et al 9 demonstrated that a postoperative hyperextension of the MCP joint of greater than or equal to 30° predicted poor grip strength and overall hand function, supporting concurrent intervention. Conversely, Poulter and Davis 10 observed that although arthrodesis or capsulodesis of the MCP joint improved deformity, functional outcomes were not necessarily enhanced.
Given the variability in clinical practice, this study aimed to characterize the specific preferences of fellowship-trained hand surgeons regarding concurrent management of MCP hyperextension during CMC arthroplasty and to identify clinical and surgeon-level factors influencing decision-making.11,12
Materials and Methods
Data Collection
Eligible fellowship-trained hand surgeons were identified through systematic Google searches of orthopedic and plastic surgery department websites and publicly available staff directories across the United States. Email addresses for fellowship-trained hand surgeons were compiled from these sources. The survey was administered electronically via REDCap. Before sending out the surveys to recipients, the authors conducted a pilot-test trial run to ensure the appropriate survey format, questions, and response documentation. The survey was then sent out to recipients, with reminder emails sent at 2 and 4 weeks following the initial invitation to optimize response rates.
A 12-question survey was developed by the authors to evaluate surgeon demographics, training background, clinical practice patterns, and specific clinical variables (Figure 1). Participants provided open-response information on institutional affiliation and were asked to categorize their practice type (private solo, private group, private/academic hybrid, or academic/health system employed). Training background included primary specialty (orthopedic, plastic, or general surgery) and residency/fellowship institutions. Respondents indicated years in practice (0-5, 6-10, 11-15, 16-20, 21-25, 26-30, >30).
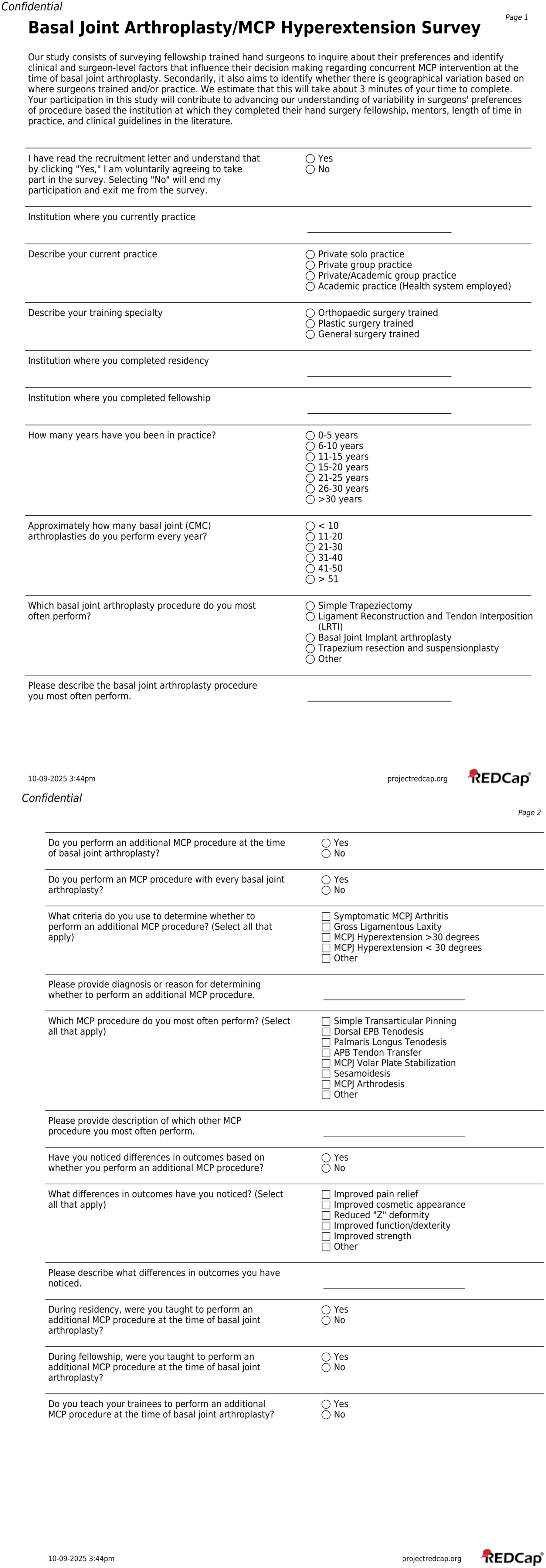
Carpometacarpal osteoarthritis/metacarpophalangeal hyperextension survey.
Questions addressed annual CMC arthroplasty volume (<10, 11-20, 21-30, 31-40, 41-50, >51), most common type of procedure (simple trapeziectomy, ligament reconstruction and tendon interposition [LRTI], CMC implant arthroplasty, trapezium resection and suspensionplasty, or other), and whether an MCP procedure was performed concurrently (yes/no). For those performing concurrent MCP procedures, additional items assessed frequency (routine vs selective), indications (symptomatic MCP joint osteoarthritis, gross ligamentous laxity, hyperextension >30°, hyperextension <30°, and/or other), procedural type (transarticular pinning, extensor pollicis brevis [EPB] or palmaris longus tenodesis, abductor pollicis brevis [APB] tendon transfer, volar plate stabilization, sesamoidesis, arthrodesis, and/or other), and perceived outcome differences (pain relief, improved cosmetic appearance, Z deformity correction, functional/dexterity improvement, improved strength, and/or other).
Respondents were also asked whether they were trained to perform a concurrent MCP procedure during residency/fellowship, and whether they currently teach the technique (yes/no).
Statistical Analysis
Descriptive statistics were used to summarize all variables. Practice locations, residency, and fellowship were categorized into U.S. Census Bureau regions (Northeast, Midwest, South, and West) and International. Surgeons were stratified by practice/residency/fellowship region (Northeast vs Other Regions), experience (≤10 vs >10 years), annual CMC arthroplasty volume (≤20 vs >20 cases), and use of concurrent MCP procedures. Intergroup comparisons were performed using chi-square or Fisher’s exact tests. Statistical analyses were performed using R Studio (Version 4.1.2. Vienna, Austria) with statistical significance set at P < .05.
Results
Respondent Demographics and Practice Patterns
The surveys were initially sent to 534 emails. Fifty-six of these surveys were rejected by the recipient’s email and returned. The surveys were successfully distributed to 478 fellowship-trained hand surgeons, of whom 73 responded (15.3% response rate). The majority practiced in academic (60.3%) or hybrid private/academic settings (34.2%), and most were located in the Northeast for practice (64.4%), residency (56.2%), and fellowship (56.2%). Respondents were largely orthopedic surgery-trained (84.9%). Experience distribution was bimodal, with 21.9% in practice for ≤5 years and 19.2% for >30 years.
Most surgeons (69.0%) performed ≤30 CMC arthroplasties annually, commonly performing trapezium resection with suspensionplasty (63.9%), followed by LRTI (29.2%). A majority (61.6%) reported performing a concurrent MCP procedure, though only 11.4% did so routinely. Training exposure varied; 43.8% were taught the technique during residency, and 68.1% were taught during fellowship; 56.9% reported teaching it to their own trainees (Table 1).
Surgeon Demographics.
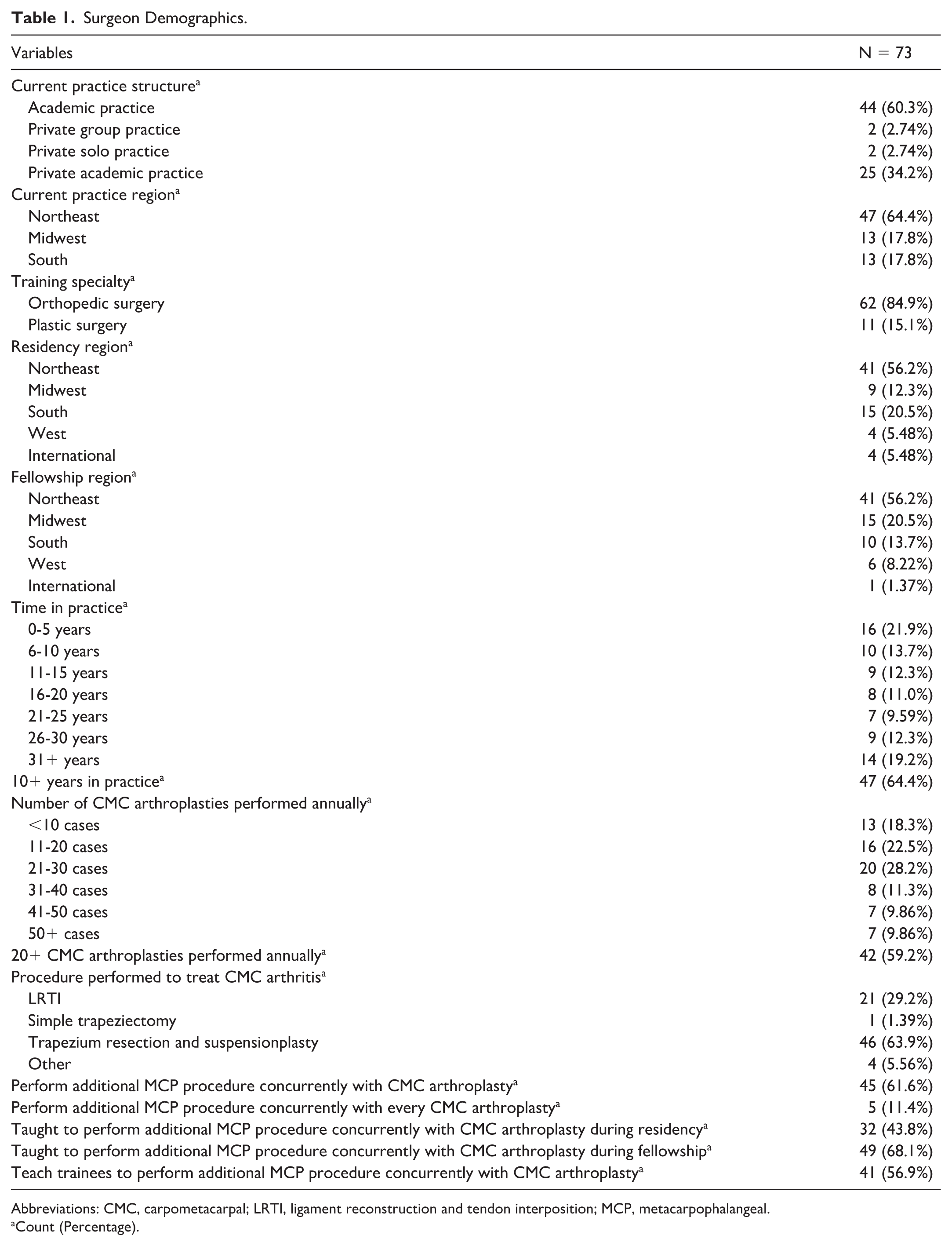
Abbreviations: CMC, carpometacarpal; LRTI, ligament reconstruction and tendon interposition; MCP, metacarpophalangeal.
Count (Percentage).
Practice Patterns Stratified by Region
Respondents primarily practiced (n = 47, 64.38%) and completed residency (n = 41, 56.16%) and fellowship (n = 41, 56.16%) training in the Northeast. As such, the remaining United States (Midwest, South, West) and International regions were combined into an “Other Regions” variable. All outcomes of interest were comparable between Northeast and Other Regions when analyzed based on practice, residency, and fellowship region.
Practice Patterns Stratified by Surgeon Experience
Among surgeons with ≤10 years in practice (n = 26) versus >10 years (n = 47), the former overwhelmingly preferred trapezium resection and suspensionplasty (92.0% vs 48.9%, P < .001), whereas the latter more frequently performed LRTI (42.6% vs 4.0%, P < .001). Experienced surgeons who performed concurrent MCP procedures were more likely to report perceiving outcome differences (86.2% vs 37.5%, P = .002), particularly in improved function/dexterity (31.9% vs 7.69%, P = .040). Other demographic and procedural variables were similar between groups (Table 2).
Surgeon Experience Comparison.
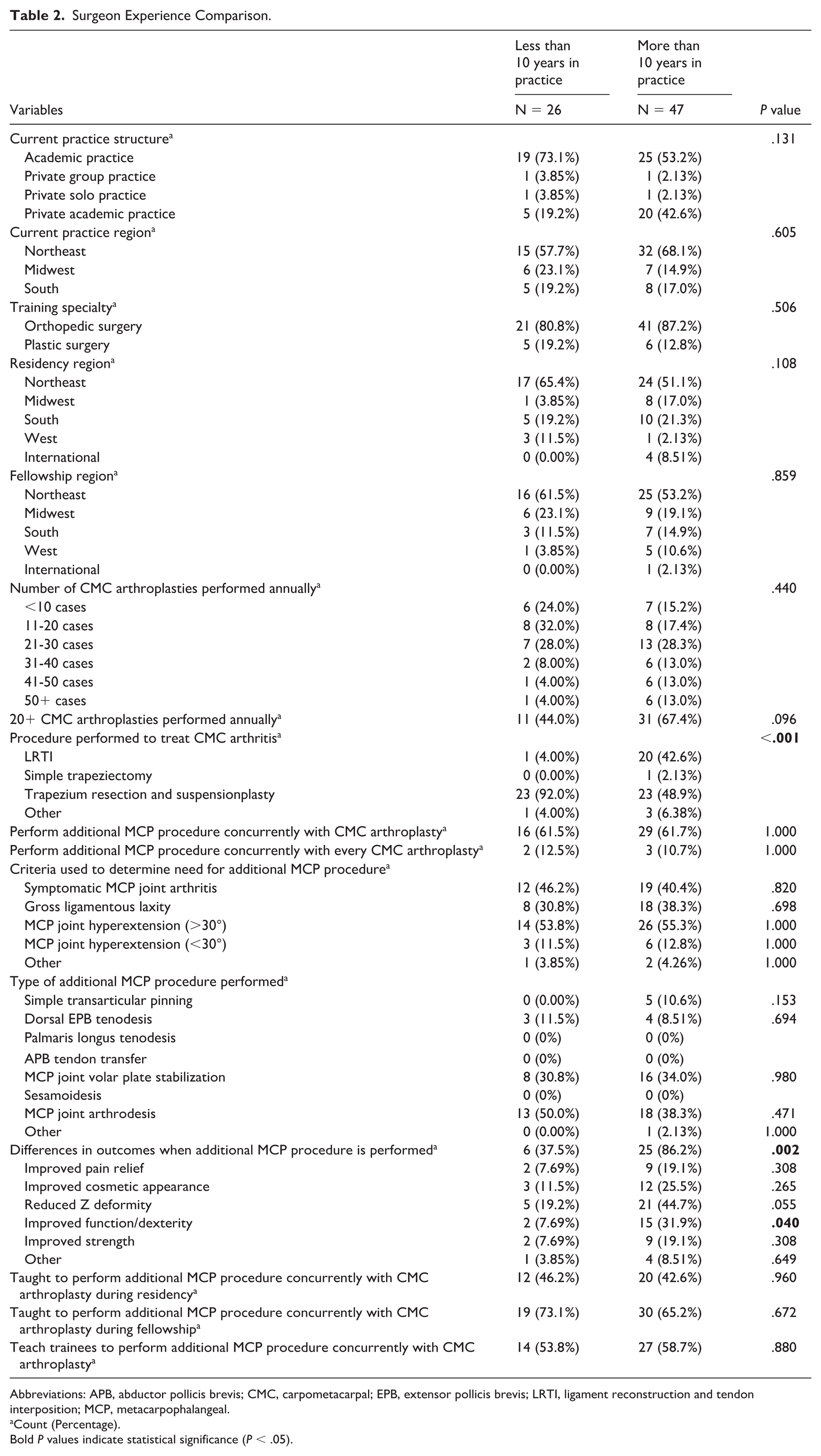
Abbreviations: APB, abductor pollicis brevis; CMC, carpometacarpal; EPB, extensor pollicis brevis; LRTI, ligament reconstruction and tendon interposition; MCP, metacarpophalangeal.
Count (Percentage).
Bold P values indicate statistical significance (P < .05).
Practice Patterns Stratified by Annual Case Volume
Surgeons performing ≤20 CMC arthroplasties per year (n = 29) were more likely to perform an MCP procedure routinely with every case than high-volume surgeons (>20 cases; n = 42) (27.8% vs 0%, P = .008). No other statistically significant differences were noted in surgeon demographics, CMC/MCP procedural choice, indications for MCP procedure, or perceived outcomes based on annual case volume (Table 3).
Annual CMC Arthroplasty Volume Comparison.
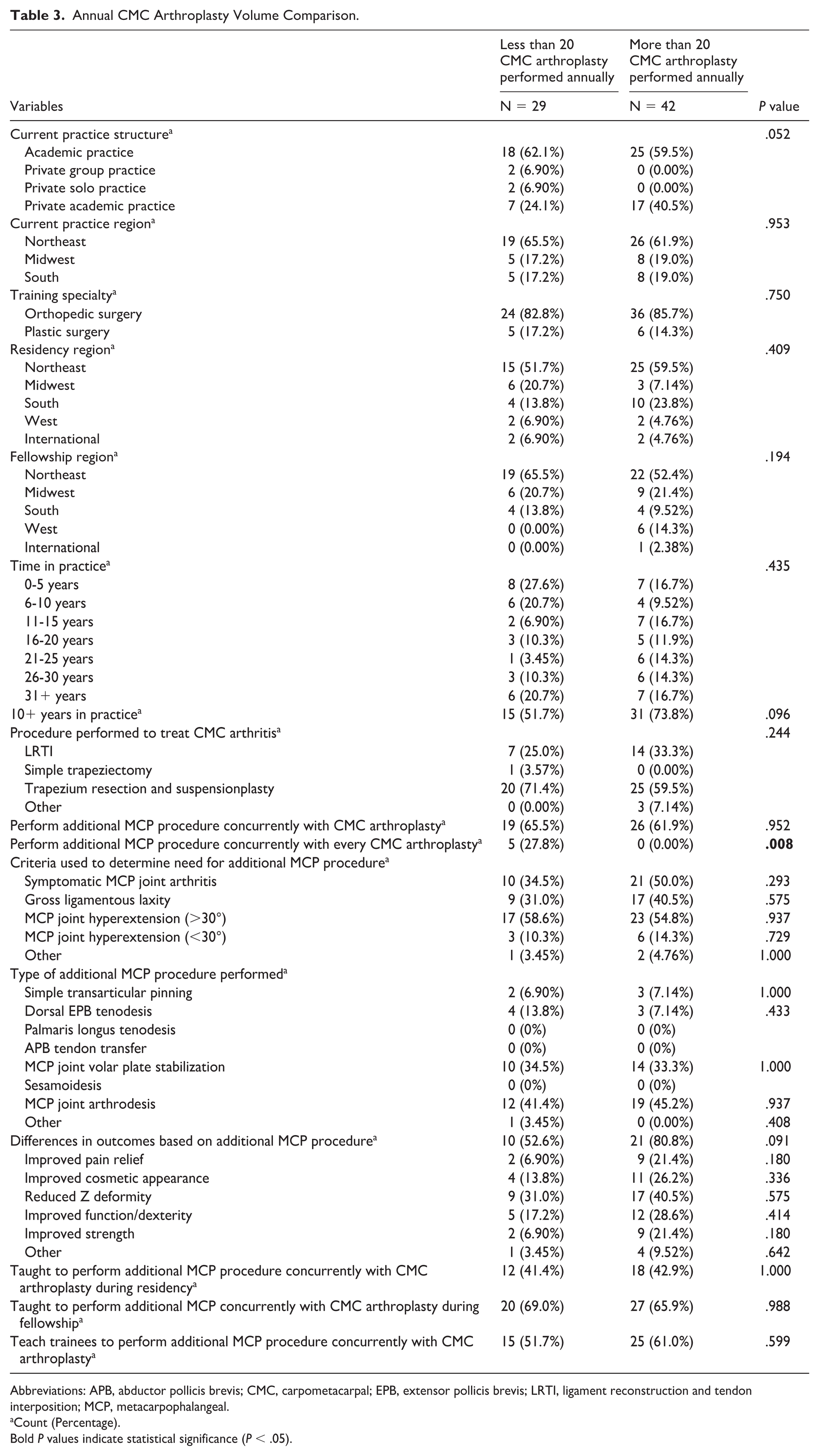
Abbreviations: APB, abductor pollicis brevis; CMC, carpometacarpal; EPB, extensor pollicis brevis; LRTI, ligament reconstruction and tendon interposition; MCP, metacarpophalangeal.
Count (Percentage).
Bold P values indicate statistical significance (P < .05).
Practice Patterns Stratified by Decision to Perform a Concurrent MCP Procedure
Practice patterns were compared between surgeons who perform a concurrent MCP procedure (n = 45) and those who do not (n = 28) during CMC arthroplasty. Surgeons who routinely perform concurrent MCP procedures were significantly more likely to have received fellowship training in the technique (81.8% vs 46.4%, P = .004) and in turn to teach it to their own trainees (88.9% vs 3.70%, P < .001). Distribution of practice duration between the 2 cohorts differed (P = .044), but other factors were comparable (Table 4).
Surgeons Performing versus Not Performing MCP Procedures.
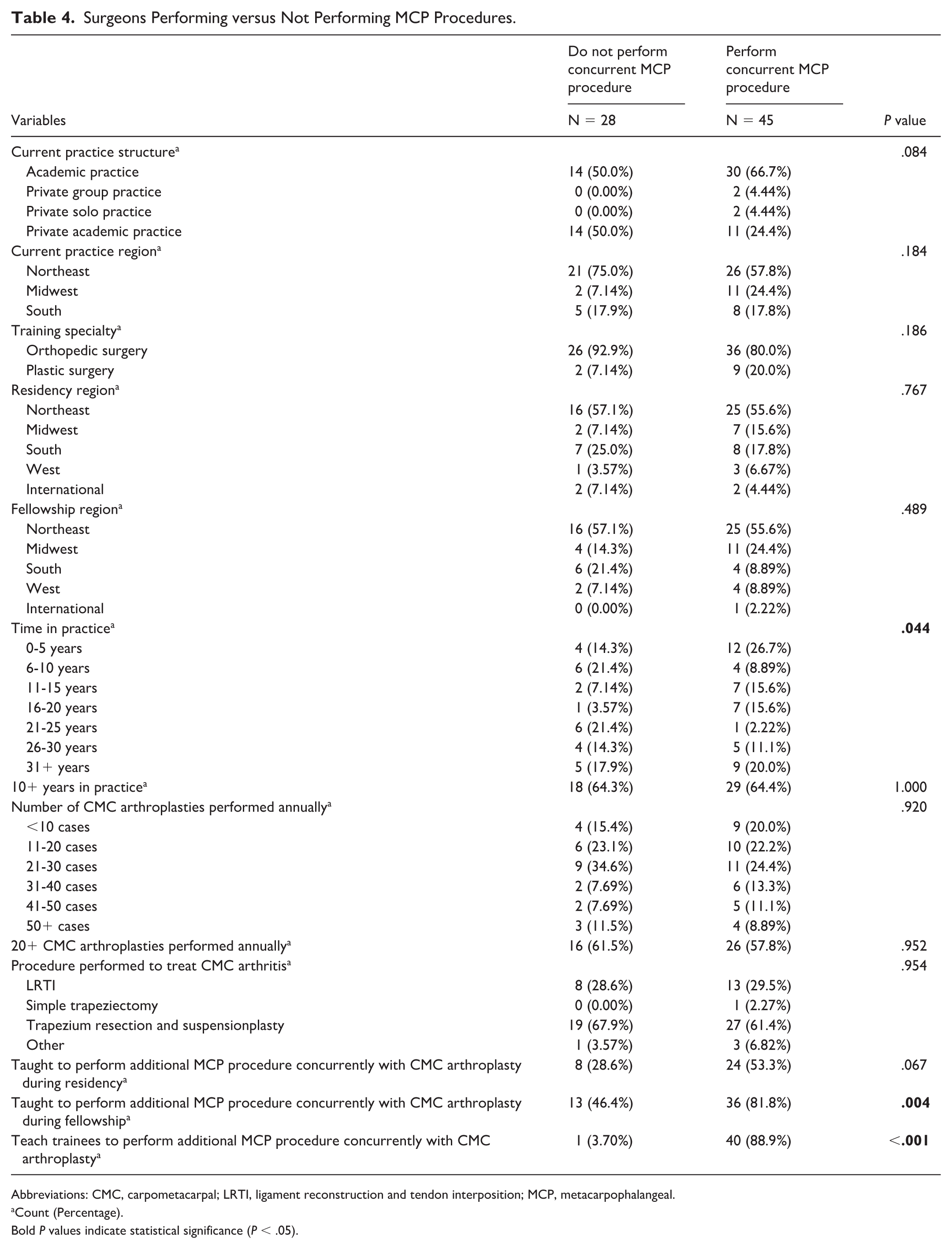
Abbreviations: CMC, carpometacarpal; LRTI, ligament reconstruction and tendon interposition; MCP, metacarpophalangeal.
Count (Percentage).
Bold P values indicate statistical significance (P < .05).
Practice Patterns of Surgeons Performing a Concurrent MCP Procedure
Among surgeons performing a concurrent MCP procedure (n = 45), the most common clinical indications were MCP joint hyperextension >30° (88.9%) and symptomatic MCP joint osteoarthritis (68.9%). The most frequently utilized techniques were MCP joint arthrodesis (68.9%) and volar plate stabilization (53.3%). The most frequently observed outcomes were reduced Z deformity (57.8%) and improved function/dexterity (37.8%) (Table 5).
MCP Intervention: Indications, Procedure, and Perceived Outcomes.
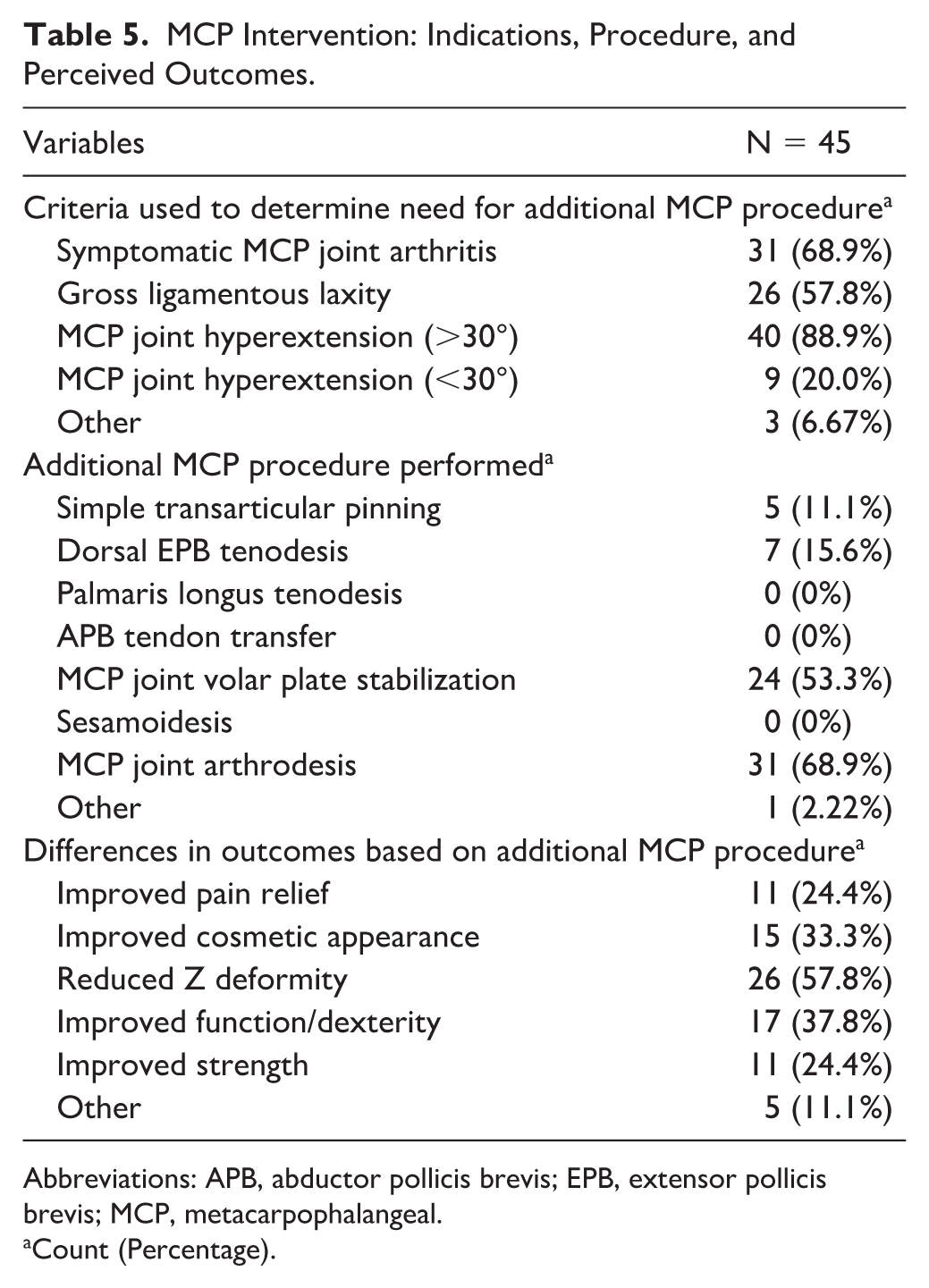
Abbreviations: APB, abductor pollicis brevis; EPB, extensor pollicis brevis; MCP, metacarpophalangeal.
Count (Percentage).
Discussion
Carpometacarpal osteoarthritis can be accompanied by MCP hyperextension due to ligamentous imbalance and capsular laxity.8,11,13 Attenuation of the volar beak and collateral ligaments promotes dorsoradial subluxation of the metacarpal.8,13 This phenomenon introduces an imbalance between the flexor and extensor mechanisms of the thumb, where the extensor pollicis brevis chronically pulls the MCP joint into hyperextension.8,11,14 Subsequently, a zig-zag (Z) deformity forms, which causes pain, decreased pinch strength, and an overall decrease in thumb function.11,15 Consequently, some surgeons advocate for concurrent correction of the MCP joint to restore alignment, optimize pinch strength, and improve cosmesis.13,16
However, clinical approaches vary widely. Despite a lack of clear guidelines, some studies have recommended using the severity of MCP hyperextension to guide management. In 1997, Blank and Feldon 17 proposed classifying MCP hypertension severity (0°-10°, 10°-20°, 20°-40°, >40°) as a guide for management. Armbruster and Tan 13 recommended observation for <10° deformity and arthrodesis for hyperextension >40°. Brogan et al 18 found no significant differences in clinical outcomes for MCP hyperextension <30° whether or not a concurrent procedure was performed. This suggests that surgical techniques that have traditionally been utilized to treat MCP hyperextension, including extensor pollicis longus/brevis tenodesis, sesamoidesis, volar plate advancement, arthrodesis, and capsulodesis, may not provide significant clinical benefit in moderate cases. Conversely, other studies support surgical intervention at thresholds ≥20°–30°.8,19,20 In the most recent review, Morrell et al proposed a stepwise treatment algorithm based on deformity severity, recommending arthrodesis for fixed deformity or arthrosis. In the absence of these severe findings, patients with functional deficits of the thumb are recommended to receive K-wire fixation or casting when the MCP deformity is <10°, spiral extensor pollicis brevis/longus tenodesis between 10° and 40°, and spiral extensor pollicis brevis/longus tenodesis with arthrodesis when >40°. 11
In the current study, surgeons earlier in their career (<10 years) more frequently performed trapezium resection and suspensionplasty, reflecting evolving practice trends and adoption of newer techniques associated with reduced rehabilitation time and improved subsidence resistance compared to LRTI.21-23 The tendency of less-experienced surgeons and surgeons who perform <20 CMC arthroplasties annually to perform concurrent MCP procedures more liberally may reflect both contemporary training emphasis and limited long-term outcome data guiding restraint. Even though surgeons who perform concurrent MCP procedures were trained in a fellowship and the majority of surgeons teach their trainees to perform MCP procedures, approximately half of the surgeons who were trained on the technique do not do so in practice, which may reflect personal preference or clinical equipoise. The limited sample size in this comparison renders it difficult to arrive at a definitive conclusion. Future studies are needed to contextualize these findings and to compare outcomes between patients who undergo CMC arthroplasty with or without a concurrent MCP procedure.
Severity of hyperextension (>30°) and symptomatic osteoarthritis were the predominant indications for MCP intervention. Arthrodesis and volar plate stabilization were the most common procedures, consistent with prior literature and algorithmic recommendations. 11 While this survey did not inquire about whether particular indications for an MCP procedure influenced the type of procedure performed, the high incidence of MCP joint arthrodesis points to symptomatic MCP joint osteoarthritis being a crucial indication for concurrent surgical treatment, which is in accordance with JAAOS guidelines. 11 Improved cosmesis (reduction of Z deformity) was the most frequently reported benefit, whereas functional improvements were less consistently observed, mirroring previous findings that correction of deformity may not always correlate with enhanced function/dexterity.10,19
Although this study is novel in its aims to examine and report on nationwide practice patterns, it has limitations. First, the authors did not have access to registries of fellowship-trained hand surgeons and therefore had to identify hand surgeons using online web searches. The response rate (15.3%) and reliance on publicly available email addresses likely introduced selection bias, favoring academic hand surgeons over private groups or solo practitioners who do not publicize their contact information. Similarly, a majority of respondents practice (64.4%) or completed residency (56.2%) or fellowship (56.2%) training in the Northeastern United States, which may have influenced practice patterns. The modest sample size of respondents also limits generalizability and precludes robust subgroup analysis. The survey design of the study makes it susceptible to potential recall and response biases, survey fatigue, and subjectivity as outcomes were self-reported rather than objectively measured. Thus, it is important to consider that perceived functional benefit can be influenced by recall bias and case selection. In addition, we were unable to account for more granular differences in techniques for specific surgeries. For example, the authors did not collect data regarding whether surgeons performed trapezium resection and suspensionplasty via a suture-button, tendon-based, or suture-only approach. We are also unable to account for specific techniques used for LRTI. Furthermore, for surgeons who answered “other” in response to the procedures that they perform to treat CMC osteoarthritis or MCP hyperextension, the authors were not able to obtain further granularity regarding practice patterns. Future multicenter studies with prospective data collection are warranted to validate these findings and correlate practice patterns with functional and patient-reported outcomes.
Conclusion
Substantial heterogeneity exists in the concurrent management of the MCP joint during CMC arthroplasty. Although many training programs teach the technique, usage varies widely and remains largely dependent on surgeon preference and perceived deformity severity. Larger, comparative studies are necessary to establish standardized, evidence-based guidelines for treating MCP pathology in the setting of CMC osteoarthritis.
Footnotes
Acknowledgements
None.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Thomas Jefferson University (no. iRISID-2024-1484) on February 18, 2025.
Consent to Participate
Informed consent to participate was provided by participants during the completion of the survey.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent to participate was provided by participants during the completion of the survey.