
Abstract
Background:
Distal radius fractures (DRFs) in older adults are frequently managed nonoperatively. However, treating “older adults” as a single group may obscure meaningful age-related differences in outcomes. We compared early and late sequelae after initial nonoperative management of DRFs in patients aged 50 to 69 versus 70 to 89 years.
Methods:
We performed a retrospective propensity-matched cohort study using the TriNetX electronic health record network. Patients with DRFs initially treated with closed management were stratified by age (50-69 vs 70-89 years) and matched 1:1 on demographics and comorbidities. We evaluated delayed operative intervention, healing complications, and neuropathic or soft-tissue sequelae up to 10 years. A 90-day landmark analysis assessed postacute events.
Results:
We identified 65 786 patients; propensity matching yielded up to 22 585 well-balanced pairs across intervals. Patients aged 50 to 69 years had higher rates of delayed surgery at all timepoints (eg, 5.03% vs 3.51% at 1 year; HR 1.49, P < .001). Nonunion, malunion, and posttraumatic arthritis were uncommon (<1%) and did not differ. Conversely, the 50 to 69 cohort demonstrated higher hazards of corrective repair, complex regional pain syndrome, and De Quervain tenosynovitis. In landmark analysis, the younger cohort remained at increased hazard of late-onset carpal tunnel syndrome and reconstructive procedures beyond 90 days.
Conclusion:
Despite similarly low rates of fracture healing complications across age strata, patients aged 50 to 69 years were more likely to undergo delayed operative intervention and experience neuropathic and soft-tissue sequelae than those aged 70 to 89 years. These findings support age-stratified counseling after initial nonoperative management.
Keywords
Introduction
Distal radius fractures (DRFs) are among the most common orthopedic injuries worldwide, with incidence increasing alongside population aging.1-3 Although operative fixation has become more prevalent, closed reduction and immobilization remain the predominant initial treatment for older adults, with nonoperative care used in roughly 70% to 80% of cases and increasing with advancing age.4,5 Accordingly, understanding downstream outcomes after initial nonoperative care remains clinically important.
However, the incidence of DRFs increases substantially beginning in the fifth and sixth decades of life.6-9 Grouping patients across broad age thresholds may obscure meaningful differences in physiologic reserve, bone quality, activity level, and functional expectations. Individuals in their sixth and seventh decades often differ clinically from those in their eighth and ninth decades with respect to comorbidity burden and baseline function.10-12 Such differences may influence tolerance of residual deformity, thresholds for surgical intervention, and patterns of postfracture sequelae.
Most prior studies evaluating DRFs in older adults have focused on radiographic alignment, short-term patient-reported outcomes, or binary comparisons of operative versus nonoperative treatment.13-15 Less is known regarding downstream clinical sequelae following initial conservative management, including delayed conversion to surgery, fracture healing complications, neuropathic or soft-tissue disorders, and motion-limiting reconstructive procedures.
The purpose of this study was to compare early and late sequelae following initial nonoperative management of DRFs in patients aged 50 to 69 years versus 70 to 89 years. We hypothesized that clinically meaningful differences would exist between age groups in rates of delayed operative intervention and postfracture sequelae, reflecting differences in functional demand and treatment thresholds, while rates of fracture healing complications would be similar.
Methods
Data Source
We conducted a retrospective, propensity-matched observational cohort study using the TriNetX Global Collaborative Network, a federated health research network aggregating de-identified electronic health records from approximately 180 million patients across over 170 health care organizations. 16 The platform provides access to diagnoses, procedures, medications, and demographic data across diverse health care systems. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 17 guidelines and the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) extension. 18
Study Population and Cohort Definition
We identified adult patients (≥18 years) with DRFs using International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes for fracture of the lower end of the radius (S52.5 series, including S52.50, S52.509A, S52.501, and S52.502). To ensure inclusion of fractures initially managed nonoperatively, patients were required to have both a qualifying distal radius fracture diagnosis and a corresponding closed treatment procedure within 14 days, defined by Current Procedural Terminology (CPT) 25600 (closed treatment without manipulation) or CPT 25605 (closed treatment with manipulation). This temporal constraint was selected to capture the initial management strategy and minimize misclassification of delayed fixation as primary operative treatment. Patients were excluded if they underwent operative fixation within 14 days on or after the qualifying fracture/closed-treatment episode, defined by CPT 25606 (percutaneous fixation) or CPT 25607/25608/25609 (open treatment with internal fixation).
Patients were stratified into 2 cohorts based on age at the index event: 50 to 69 years and 70 to 89 years, consistent with age thresholds used in prior studies.9,19 These age strata also capture the “second peak” found in the bimodal distribution of distal radius fracture incidence, occurring in patients aged 50 years or older and reflect clinically relevant differences in physiologic reserve and functional expectations across later decades of life. 14
Propensity Score Matching
To reduce confounding, 1:1 propensity score matching was performed using TriNetX’s greedy nearest-neighbor algorithm without replacement. Cohorts were matched on demographic characteristics and prespecified clinical covariates: diabetes mellitus, overweight/obesity, nicotine dependence, osteoporosis, rheumatoid arthritis, and glucocorticoid use. Covariate balance was assessed using standardized mean differences (SMDs), with SMD ≤ 0.10 considered acceptable for matched variables. Matching was repeated for each analysis window (90 days, 1 year, 5 years, and 10 years) to account for time-window–specific eligibility and censoring.
Outcome Measures
Outcomes were defined using prespecified ICD-10-CM and CPT code sets extracted from the TriNetX query export (Supplement 1). Delayed surgery was defined as operative fixation performed more than 14 days after the index event following initial nonoperative management. Additional outcomes included nonunion or malunion, corrective repair of malunion or nonunion, posttraumatic wrist arthritis, motion-limiting reconstructive procedures, tendon rupture, carpal tunnel syndrome (CTS), complex regional pain syndrome (CRPS), and De Quervain tenosynovitis. Patients with outcomes prior to the analysis window were excluded from all analyses.
Index Event and Follow-Up Windows
The index date was defined as the first occurrence of a qualifying distal radius fracture diagnosis with corresponding closed treatment. To minimize misclassification from peri-index coding and immediate postinjury encounters, outcomes were assessed beginning 15 days after the index date.
Analyses were performed within prespecified windows: days 15 to 90, days 15 to 365, day 15 to 5 years, and day 15 to 10 years following the index event. For longer horizons, follow-up was censored at the last recorded clinical activity within the TriNetX network, such that 5- and 10-year analyses represent time to event estimates within those windows rather than fixed duration follow-up. A minimum follow-up duration was not required; patients contributed time at risk from 15 days after the index event until occurrence of the outcome or censoring at their last recorded clinical encounter within the TriNetX network.
Statistical Analysis
All analyses were performed within the TriNetX platform. Time-to-event analyses were performed using Cox proportional hazards models, with patients censored at the time of the outcome or last recorded clinical activity. Hazard ratios (HRs) and 95% confidence intervals were reported alongside absolute event rates. Statistical significance was defined as a 2-sided P value < .05. A 90-day landmark sensitivity analysis was performed to evaluate whether long-term differences were driven by acute fracture healing and early conversion to surgery. A 90-day period was selected to account for the potentially slower time to fracture healing observed in older patients. 20 Patients were required to be event-free through day 90, and outcomes were subsequently evaluated from day 91 through 5 years postindex using the same time-to-event methods described above.
Ethical Considerations
This retrospective study was exempt from informed consent. The data reviewed represent a secondary analysis of existing data, do not involve intervention or interaction with human subjects, and are de-identified per the de-identification standard defined in Section §164.514(a) of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. 21 The de-identification process is attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule, most recently refreshed in December 2020.
Results
Study Population and Propensity Score Matching
A total of 65 786 patients with nonoperatively managed DRFs were identified, including 30 307 patients aged 50 to 69 years and 35 479 patients aged 70 to 89 years (Figure 1). Prior to matching, the 70 to 89 years cohort had higher proportions of female sex, osteoporosis, diabetes mellitus, and glucocorticoid use (all P < .001).
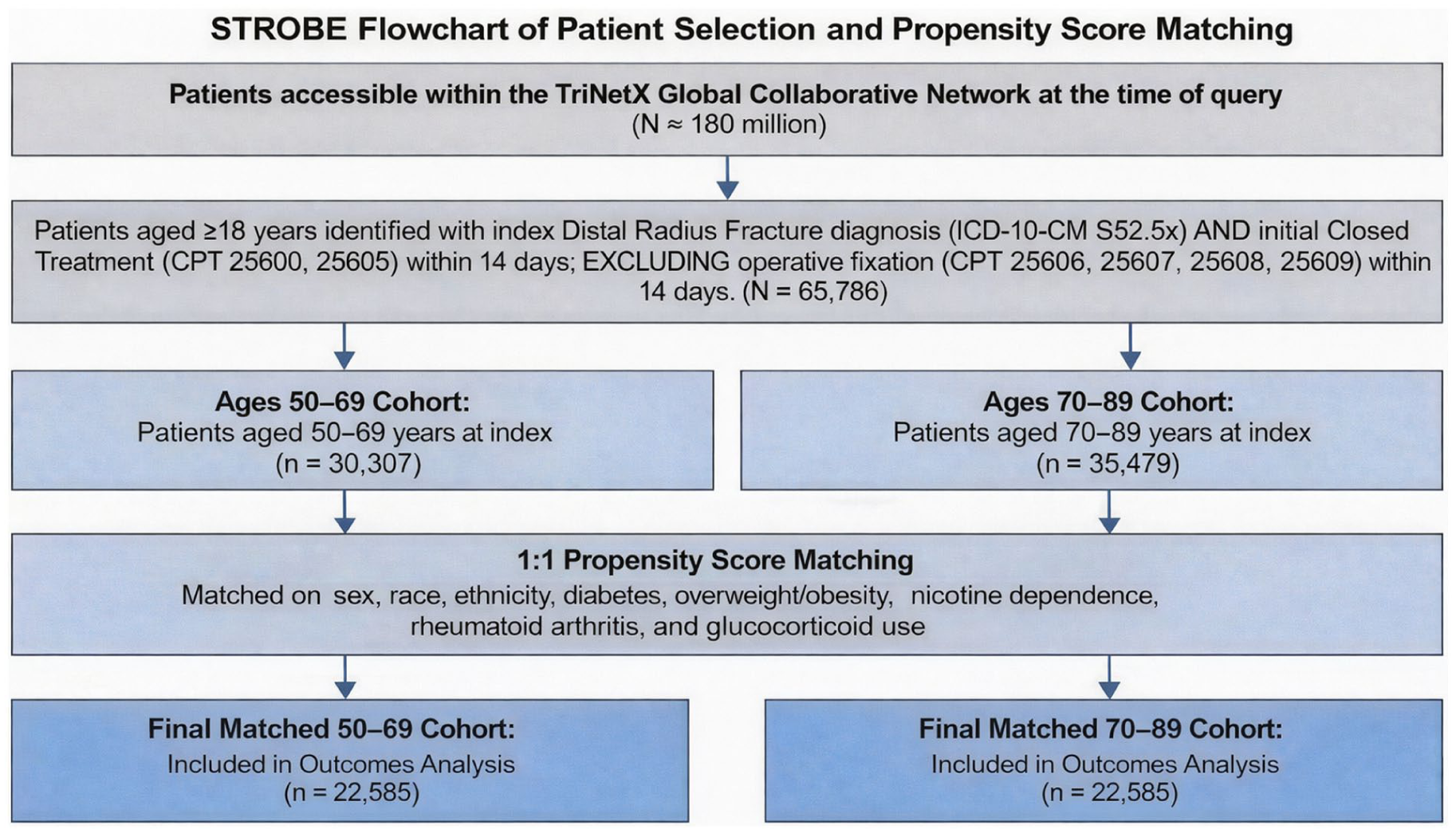
STROBE flow diagram of cohort identification and propensity score matching.
Acceptable covariate balance was achieved after propensity score matching across all follow-up intervals (all SMD ≤ 0.10). The 1-year matching cohort is presented as a representative example (Table 1). Matched sample sizes varied modestly across time horizons (eg, 22 585 pairs at 1 year vs 21 506 pairs at 5 years), reflecting time-window–specific eligibility and censoring based on available follow-up within the TriNetX network.
Baseline Characteristics of Propensity Score–Matched Cohorts.
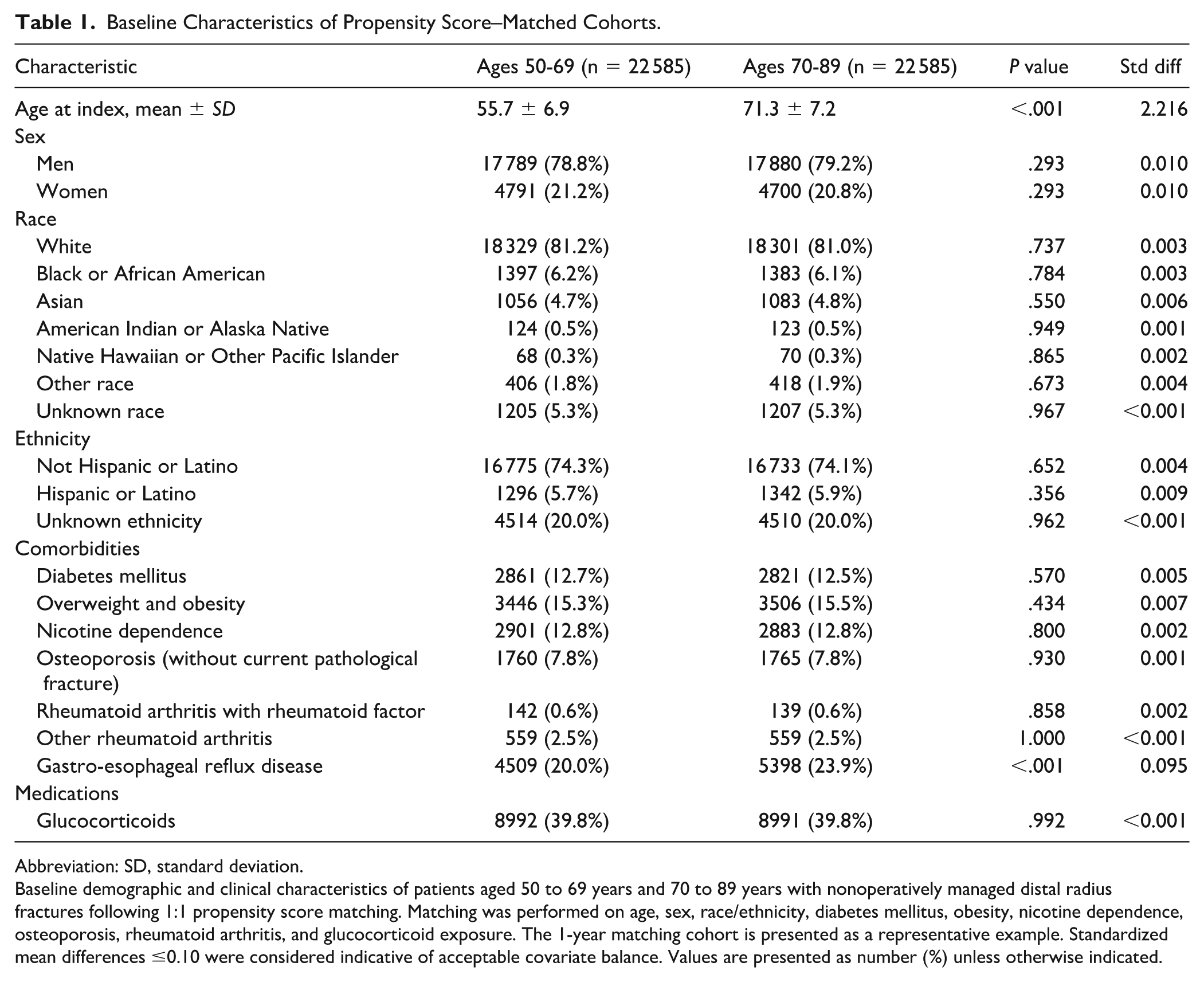
Abbreviation: SD, standard deviation.
Baseline demographic and clinical characteristics of patients aged 50 to 69 years and 70 to 89 years with nonoperatively managed distal radius fractures following 1:1 propensity score matching. Matching was performed on age, sex, race/ethnicity, diabetes mellitus, obesity, nicotine dependence, osteoporosis, rheumatoid arthritis, and glucocorticoid exposure. The 1-year matching cohort is presented as a representative example. Standardized mean differences ≤0.10 were considered indicative of acceptable covariate balance. Values are presented as number (%) unless otherwise indicated.
Early Outcomes (Days 15-90 After Index)
At a median follow-up of 90 days in both cohorts, delayed surgery occurred more often in patients aged 50 to 69 than 70 to 89 (4.97% vs 3.38%; HR 1.53, 95% CI 1.40-1.67; P < .001). Nonunion/malunion rates (0.349% vs 0.361%) and repair of malunion/nonunion did not differ between groups (0.418% vs 0.320%; both P = .073), though time-to-event analysis demonstrated a higher hazard for repair of malunion/nonunion in the 50 to 69 cohort (HR 1.36, 95% CI 1.01-1.83; P = .040). Posttraumatic arthritis was rare and not different between groups (0.078% vs 0.090%; P = .640).
Carpal tunnel syndrome did not differ by age (1.38% vs 1.57%; P = .087), but CRPS was more common in ages 50 to 69 (0.193% vs 0.115%; HR 1.76, 95% CI 1.10-2.80; P = .017). De Quervain tenosynovitis was also more common in the 50 to 69 cohort (0.386% vs 0.293%; HR 1.37, 95% CI 1.01-1.87; P = .043).
1-Year Outcomes (Days 15-365 After Index)
At 1 year, the median follow-up was 365 days in both cohorts. Delayed surgery remained more frequent in patients aged 50 to 69 compared with those aged 70 to 89 (5.03% vs 3.51%; HR 1.49, 95% CI 1.36-1.64; P < .001). Rates of nonunion or malunion were similar between cohorts (0.63% vs 0.62%; P = .587). In contrast, corrective repair of malunion or nonunion occurred more frequently in the younger cohort (0.84% vs 0.50%; HR 1.75, 95% CI 1.39-2.21; P < .001).
Posttraumatic wrist arthritis remained uncommon and did not differ between groups (0.22% vs 0.20%; P = .457). Similarly, rates of CTS were comparable (3.36% vs 3.46%; P = .695), and reconstructive procedures for advanced postfracture sequelae did not differ between cohorts (0.07% vs 0.05%; P = .364). However, patients aged 50 to 69 demonstrated higher rates of CRPS (0.38% vs 0.25%; HR 1.56, 95% CI 1.12-2.19; P = .008), as well as De Quervain tenosynovitis (1.25% vs 0.86%; HR 1.53, 95% CI 1.27-1.84; P < .001).
5-Year Analysis Window (Day 15-5 Years After Index)
Because follow-up is censored at last recorded clinical activity in TriNetX, the 5- and 10-year analyses represent time-to-event estimates within prespecified windows (up to 5 and 10 years), rather than fixed-duration follow-up. Within the 5-year analysis window, median follow-up was 966 days (interquartile range [IQR]: 1668) in patients aged 50 to 69 and 1101 days (IQR: 1596) in patients aged 70 to 89.
Within the 5-year window, delayed surgery remained more frequent in patients aged 50 to 69 compared with those aged 70 to 89 (5.45% vs 3.84%; HR 1.48, 95% CI 1.35-1.62; P < .001). Rates of nonunion or malunion were similar between cohorts (0.68% vs 0.69%; P = .814). In contrast, corrective repair of malunion or nonunion occurred more frequently in the younger cohort (0.91% vs 0.57%; HR 1.65, 95% CI 1.32-2.07; P < .001).
Posttraumatic wrist arthritis (0.36% vs 0.32%), CTS (4.73% vs 4.77%), motion-limiting reconstructive procedures (0.10% vs 0.07%), and tendon rupture (0.12% vs 0.07%) did not differ between groups (all P > .05). In contrast, patients aged 50 to 69 demonstrated higher hazard of CRPS (0.44% vs 0.25%; HR 1.86, 95% CI 1.33-2.60; P < .001) and De Quervain tenosynovitis (1.72% vs 1.14%; HR 1.59, 95% CI 1.36-1.88; P < .001).
Extended Analysis Window (Up to 10 Years After Index; Day 15-10 Years)
Within the extended window (up to 10 years), median follow-up was 941 days (IQR: 1996) in patients aged 50 to 69 and 1104 days (IQR: 2140) in patients aged 70-89. Delayed surgery remained more frequent in patients aged 50-69 compared with those aged 70-89 (5.34% vs 3.89%; HR 1.44, 95% CI 1.31-1.57; P < .001) (Figure 2). Rates of nonunion or malunion were identical between cohorts (0.72% vs 0.72%; P = .657). In contrast, corrective repair of malunion or nonunion occurred more frequently in the younger cohort (0.90% vs 0.57%; HR 1.64, 95% CI 1.31-2.05; P < .001).
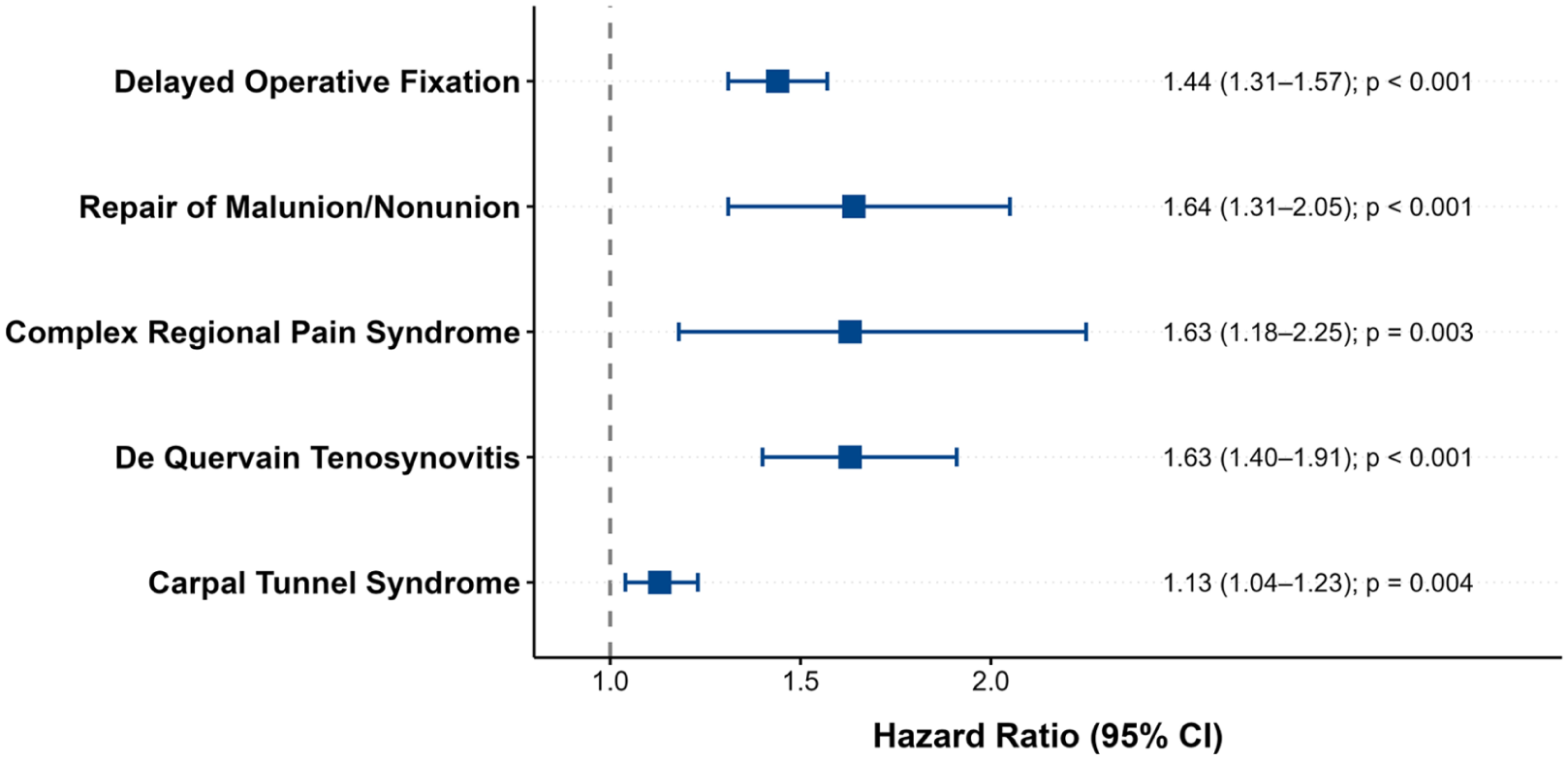
Age-stratified hazards of sequelae within the 10-year analysis window after nonoperative distal radius fracture management.
Posttraumatic wrist arthritis (0.41% vs 0.37%), motion-limiting reconstructive procedures (0.11% vs 0.06%), and rates of tendon rupture (0.11% vs 0.08%) remained uncommon and did not differ significantly between groups (all P > .05). Unlike earlier time intervals, CTS demonstrated increased hazard in the younger cohort (5.30% vs 5.01%; HR 1.13, 95% CI 1.04-1.23; P = .004). Furthermore, patients aged 50 to 69 continued to demonstrate higher rates of CRPS (0.43% vs 0.28%; HR 1.63, 95% CI 1.18-2.25; P = .003) and De Quervain tenosynovitis (1.81% vs 1.19%; HR 1.63, 95% CI 1.40-1.91; P < .001).
Sensitivity Analysis
To evaluate whether long-term differences were driven primarily by acute fracture healing, we performed a 90-day landmark sensitivity analysis isolating events occurring strictly between 90 days and 5 years postindex. Median follow-up in this matched cohort was 957 days (IQR: 1670) for patients aged 50 to 69 and 1112 days (IQR: 1581) for patients aged 70 to 89.
When excluding the initial 90-day acute phase, delayed operative fixation of the index fracture remained rare (0.39% vs 0.38%; P = .518), as did diagnoses of nonunion or malunion (0.33% vs 0.33%; P = .791), with no differences between cohorts. However, the younger cohort demonstrated significantly higher hazards for requiring delayed operative interventions, including late corrective repair of malunion/nonunion (0.42% vs 0.23%; HR 1.91, 95% CI 1.38-2.65; P < .001) and motion-limiting reconstructive procedures (0.11% vs 0.06%; HR 1.98, 95% CI 1.03-3.78; P = .036).
Patients aged 50 to 69 remained at a higher risk for developing late-onset neuropathic and soft-tissue sequelae. Time-to-event analysis demonstrated increased hazards in the younger cohort for late CTS (3.40% vs 3.16%; HR 1.15, 95% CI 1.04-1.27; P = .008), CRPS (0.25% vs 0.15%; HR 1.77, 95% CI 1.17-2.68; P = .006), and De Quervain tenosynovitis (1.20% vs 0.77%; HR 1.67, 95% CI 1.39-2.01; P < .001). Posttraumatic arthritis remained uncommon and did not differ between groups in this window (0.31% vs 0.27%; P = .289).
Discussion
In this large propensity-matched cohort study of patients initially managed nonoperatively for DRFs, we observed clinically meaningful age-related differences in downstream sequelae. Patients aged 50 to 69 years consistently demonstrated higher rates of delayed operative intervention, corrective procedures for malunion or nonunion, and neuropathic or soft-tissue complications compared with patients aged 70 to 89 years. In contrast, fracture healing complications, including nonunion and malunion, occurred at similarly low rates across age groups at all time points. These findings support our hypothesis that functional demand and treatment thresholds differ across age strata, while biologic fracture healing appears largely comparable.
Delayed conversion to surgery was significantly more common in the younger cohort across all follow-up windows, with approximately 40% to 50% higher hazards persisting through 10 years. Importantly, this pattern remained evident even after a 90-day landmark analysis excluding early failures, suggesting these differences are not driven solely by acute fracture displacement or early reassessment of alignment. Rather, younger patients continued to demonstrate higher hazards for late corrective procedures and reconstructive interventions well beyond the initial healing phase. These findings align with prior work demonstrating that younger age within older adult populations independently predicts operative management, even after accounting for fracture severity and radiographic parameters.12,22 One potential explanation is that patients aged 50 to 69 years may be more likely to sustain higher-energy injuries or fracture patterns that are less impacted and therefore less tolerant of residual deformity. In addition, greater baseline activity level and functional demand in this cohort may further lower the threshold for pursuing delayed surgical intervention. Because injury mechanism and fracture morphology are not captured in the TriNetX dataset, these factors cannot be directly assessed but likely contribute to the observed differences. Collectively, this suggests that patients in their sixth and seventh decades may have lower tolerance for residual deformity and greater expectations for functional restoration, contributing to higher rates of delayed surgical intervention despite similar healing profiles.
Notably, rates of nonunion or malunion remained uniformly low (<1%) and did not differ between age groups at any interval. This observation reinforces prior studies demonstrating that radiographic alignment and surgical fixation do not necessarily translate into superior functional outcomes in older adults.8,14,15,23 Our findings extend this by showing that while fracture union is comparable across age strata, younger patients are more likely to pursue secondary corrective procedures. This likely reflects differences in activity level, occupational demands, and perceived disability rather than intrinsic biologic healing capacity.
Beyond surgical outcomes, we identified consistent age-related differences in neuropathic and soft-tissue sequelae. Patients aged 50 to 69 years demonstrated higher cumulative incidence and hazard of CRPS and De Quervain tenosynovitis across all time horizons, with these disparities persisting even after exclusion of the acute postinjury period. Prior studies of postfracture CRPS have focused on overall incidence and general risk factors rather than age-stratified analyses, limiting direct comparison.24-27 However, the higher rate of De Quervain tenosynovitis in the younger cohort aligns with prior work demonstrating strong associations between this condition and strenuous overuse activities following DRFs. 28 Similarly, while early rates of CTS were comparable, the modestly increased hazard for late-onset CTS in the younger cohort is noteworthy and mirrors recent analyses identifying patients aged 50 to 69 years as having the highest likelihood of progression to carpal tunnel release following distal radius fracture. 29 Delayed median neuropathy following conservative management has been linked to anatomical alterations and residual carpal malalignment, including changes in volar tilt and carpal alignment parameters, 30 and the divergence in late-onset symptoms observed in our cohort suggests that these altered mechanics may be further exacerbated by prolonged, repetitive extremity use. These findings suggest that younger patients may be more susceptible to, or more likely to seek care for, postfracture pain syndromes and tendon disorders, reflecting higher functional demands, greater extremity use, and heightened symptom awareness.
In contrast, posttraumatic arthritis was uncommon and largely similar between groups, suggesting that progressive joint degeneration alone does not account for the observed age-dependent differences in downstream care. Radiographic posttraumatic arthritis after distal radius fracture has been reported to occur frequently in younger, non-osteoporotic populations with long-term follow-up, with prevalence estimates exceeding 50% in some series, although its association with clinical symptoms and functional outcomes remains unclear. 31 However, in older adults, recent prospective data demonstrate that radiographic arthritis and malunion after nonoperative management often do not translate into persistent pain or functional decline. 32 In a cohort of patients aged ≥ 65 years treated conservatively, Thorninger et al 32 reported radiographic arthritis in approximately one-third of patients at more than 3 years, yet only a small subset experienced pain and patient-reported outcomes remained stable over time. Similarly, Wæver et al 33 reported no significant differences in posttraumatic osteoarthritis or functional outcomes between volar plating and casting at minimum 2-year follow-up in patients aged ≥65 years, reinforcing nonoperative management as a durable first-line strategy in older adults.
Despite similar rates of posttraumatic arthritis, younger patients were significantly more likely to undergo late reconstructive procedures. Motion-limiting reconstructive procedures, including wrist arthrodesis and proximal row carpectomy, were rare overall but occurred more frequently in the younger cohort following landmark analysis. These salvage operations are typically reserved for end-stage symptomatic deformity or intractable pain.34,35 The higher hazard observed in the 50 to 69 age group underscores that patients in this younger age stratum, who face longer periods of continued occupational or recreational wrist loading, are more likely to pursue definitive surgical solutions for persistent dysfunction. This pattern suggests that downstream health care use is likely influenced more by functional demands than by differences in fracture healing. These findings have direct implications for shared decision-making. Patients in their sixth and seventh decades should be counseled about the modestly higher likelihood of delayed intervention and late reconstructive procedures, whereas those in their eighth and ninth decades can be reassured that nonoperative management is unlikely to culminate in major salvage surgery.
Our results highlight the limitations of broad age-based categorization when evaluating distal radius fracture outcomes in older adults. Prior studies frequently rely on coarse decade-based stratification or aggregate patients into a single “older adult” group, often defined as ≥65 years, potentially obscuring important differences in postfracture trajectories across later decades. In contrast, our data demonstrate substantial heterogeneity within this population: patients aged 50 to 69 years were more likely to undergo delayed surgery and experience symptomatic sequelae despite similar fracture healing, whereas those aged 70 to 89 years demonstrated lower rates of late intervention and appear more tolerant of residual deformity. These differences suggest that downstream care is driven less by biologic union and more by functional expectations and symptom burden. Clinically, this distinction supports more individualized counseling. Patients in their sixth and seventh decades should be informed of the modestly higher likelihood of delayed intervention, while patients in their eighth and ninth decades can be reassured that nonoperative management is unlikely to culminate in major reconstructive procedures. Collectively, these results underscore the importance of nuanced age stratification when guiding conservative fracture care and designing future outcomes research.
Limitations
This study has limitations inherent to retrospective analyses of de-identified electronic health record data. Outcomes were ascertained using ICD-10 and CPT codes rather than adjudicated clinical assessments, which may introduce misclassification and under-capture of events, particularly for diagnoses that are variably coded or managed outside orthopedic settings. This limitation is especially relevant for outcomes such as nonunion and malunion, which may be variably coded and therefore underrepresented in administrative datasets. TriNetX also lacks fracture morphology, radiographic alignment, immobilization details, rehabilitation data, hand dominance, and patient-reported outcomes, limiting assessment of how anatomic parameters and functional status relate to downstream use. Although propensity matching achieved balance across measured comorbidities and medication exposures, residual confounding from unmeasured factors including frailty, socioeconomic variables, access to specialty care, baseline activity, and occupational demands remains possible. Long-term estimates may also be influenced by incomplete capture of care outside participating health systems and by censoring at the last recorded encounter, such that extended-window analyses reflect time-to-event within the network rather than guaranteed fixed-duration follow-up. In addition, the analysis does not explicitly account for competing risks such as mortality, and older patients may have a higher likelihood of death prior to experiencing downstream sequelae, which could partially attenuate observed event rates in this cohort. Finally, while the overall cohort was large, several outcomes were rare, yielding wider uncertainty for less frequent events. Despite these constraints, the consistency of findings across multiple time horizons and the landmark sensitivity analysis strengthens the inference that clinically meaningful age-stratified differences exist after initial nonoperative distal radius fracture management.
Conclusion
Among patients initially managed nonoperatively for DRFs, those aged 50 to 69 years experienced higher rates of delayed surgical intervention, corrective procedures, and neuropathic or soft-tissue sequelae compared with patients aged 70 to 89 years, despite similar low rates of fracture healing complications. These findings highlight meaningful clinical heterogeneity within older adult populations and suggest that functional expectations and treatment thresholds, rather than biologic healing alone, influence downstream care following conservative fracture management. Incorporating age-specific counseling and follow-up strategies may help better align treatment decisions with patient goals and anticipate long-term sequelae in this growing patient population.
Supplemental Material
sj-docx-1-han-10.1177_15589447261453552 – Supplemental material for Age-Stratified Sequelae After Nonoperative Distal Radius Fractures: A Propensity-Matched Cohort Study
Supplemental material, sj-docx-1-han-10.1177_15589447261453552 for Age-Stratified Sequelae After Nonoperative Distal Radius Fractures: A Propensity-Matched Cohort Study by Nicholas Frappa, Morgan R. Dillon, Aidan G. Papalia, Matthew G. Alben, Tripp Leavitt and Lindsay Kosinski in HAND
Footnotes
Acknowledgements
None.
Ethical Considerations
This study utilized de-identified data from the TriNetX Global Collaborative Network. In accordance with the Common Rule (45 CFR 46.102), this research does not constitute human subjects research. Therefore, Institutional Review Board approval and informed consent were not required. All data were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule (§164.514[a]).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The data that support the findings of this study are available from TriNetX, Inc., but restrictions apply to the availability of these data, which were used under license for the current study and are not publicly available. Data are available from the authors upon reasonable request and with permission of TriNetX.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained when necessary.
Supplemental Material
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.