
Abstract
Background:
The purpose of this study was to define radiographic morphologic variations of the proximal and middle phalanges of all digits to compare these anatomic parameters with the dimensions of currently available intramedullary (IM) headless screws.
Methods:
Standardised posteroanterior (PA) and lateral (LAT) radiographs of 250 digits (125 males and 125 females) were analysed. Measurements were performed for the proximal phalanx of the thumb through little finger and for the middle phalanx of the index through little finger. Measurements included IM isthmus and cortical diameters, head and base dimensions, total bone length, and anterograde and retrograde distances from the isthmus. All dimensions were compared with specifications from commercially available headless screws.
Results:
On PA views, the mean IM isthmus diameter of the proximal phalanx was greatest in the thumb (4.8 mm) and smallest in the little finger (2.9 mm). On PA views the middle phalanx demonstrated isthmus diameters of 3.4 mm (middle finger) to 2.5 mm (ring finger). On LAT views, IM diameters were narrower (1.5-2.4 mm). Male participants demonstrated significantly larger osseous dimensions across most parameters. Comparative analysis with available implants demonstrated that smaller-calibre screws (≤3.0 mm) appropriately matched the IM canal of most middle and ring phalanges. In contrast, larger devices (≥3.0 mm) may be suitable for the proximal phalanges of the thumb and middle finger.
Conclusion:
Intramedullary canal diameter and phalangeal morphology vary by digit and gender. For most digits, 2.0- to 3.0-mm IM headless screws best approximate the native canal dimensions. Awareness of these anatomic constraints is essential for preoperative planning and selecting the correct implants therby minimising the risk of iatrogenic fracture and screw jamming while optimisng intramedullary phalangeal fracture fixation.
Keywords
Introduction
Phalangeal fractures account for a substantial proportion of all upper-extremity fractures and are the most common fractures of the hand.1,2 Among these, injuries to the proximal (P1) and distal (P3) phalanges occur most frequently, particularly involving the middle and ring fingers.3,4 Phalangeal fractures can significantly compromise digital motion, grip strength, and overall hand function, especially when affecting the dominant hand or multiple digits.4,5
The principal goal of treatment is to achieve solid union and a stable, pain-free digit with functional range of motion (ROM). Stable, minimally displaced fractures may be managed conservatively with splinting or buddy strapping, allowing controlled early motion once sufficient stability is achieved. However, operative fixation is indicated when fractures demonstrate instability, displacement, malrotation, or intra-articular involvement, or when deformity recurs after closed reduction.
A variety of fixation techniques have been developed, each with distinct biomechanical advantages and limitations. Percutaneous pinning with Kirschner wires (K-wires) remains a widely used method because of its technical simplicity and cost-effectiveness. 6 However, external immobilisation may still be required depending on the fracture pattern, which can predispose to stiffness and pin-site complications such as infection, migration, or breakage. Open reduction and internal fixation with plates and screws provides rigid fixation and permits early mobilisation but necessitates greater surgical exposure and soft-tissue dissection, increasing the risk of tendon adhesions, hardware irritation, and secondary implant removal.7,8 Lag screws are effective for long oblique or spiral fractures, providing interfragmentary compression and primary bone healing. 9
Recently, intramedullary headless cannulated screws (IM HCS) have emerged as a minimally invasive, load-sharing alternative that preserves the soft-tissue envelope. This technique allows stable fixation entirely within the medullary canal and has shown favourable clinical outcomes with reduced complication rates in both metacarpal and phalangeal fractures. 10 However, due to the small and variable canal morphology of the phalanges, implant selection requires a detailed understanding of intramedullary (IM) dimensions and cortical anatomy to minimise the risk of cortical iatrogenic fracture, screw jamming, or hardware prominence. 11 Detailed digit- and gender-specific IM morphometric data for the phalanges remain limited.
The purpose of this study was to quantify radiographic morphologic parameters of the proximal and middle phalanges across all digits as they relate to IM fixation and to compare these anatomic findings with the dimensions of currently available headless screws and IM devices.
Methods
Standardised posteroanterior (PA) and lateral (LAT) radiographs of 450 phalanges were analysed. Radiographs demonstrating phalangeal fractures and those with rotation of the finger were excluded. All dimensions were referenced through the central longitudinal axis of each phalanx, as illustrated in Figures 1 and 2. All measurements were performed on the Sectra IDS7 diagnostic imaging platform (Linköping, Sweden) and reviewed by a fellowship-trained orthopaedic hand surgeon (KRV). Measurement calibration within the imaging system was standardised for magnification. All data were anonymised prior to analysis.
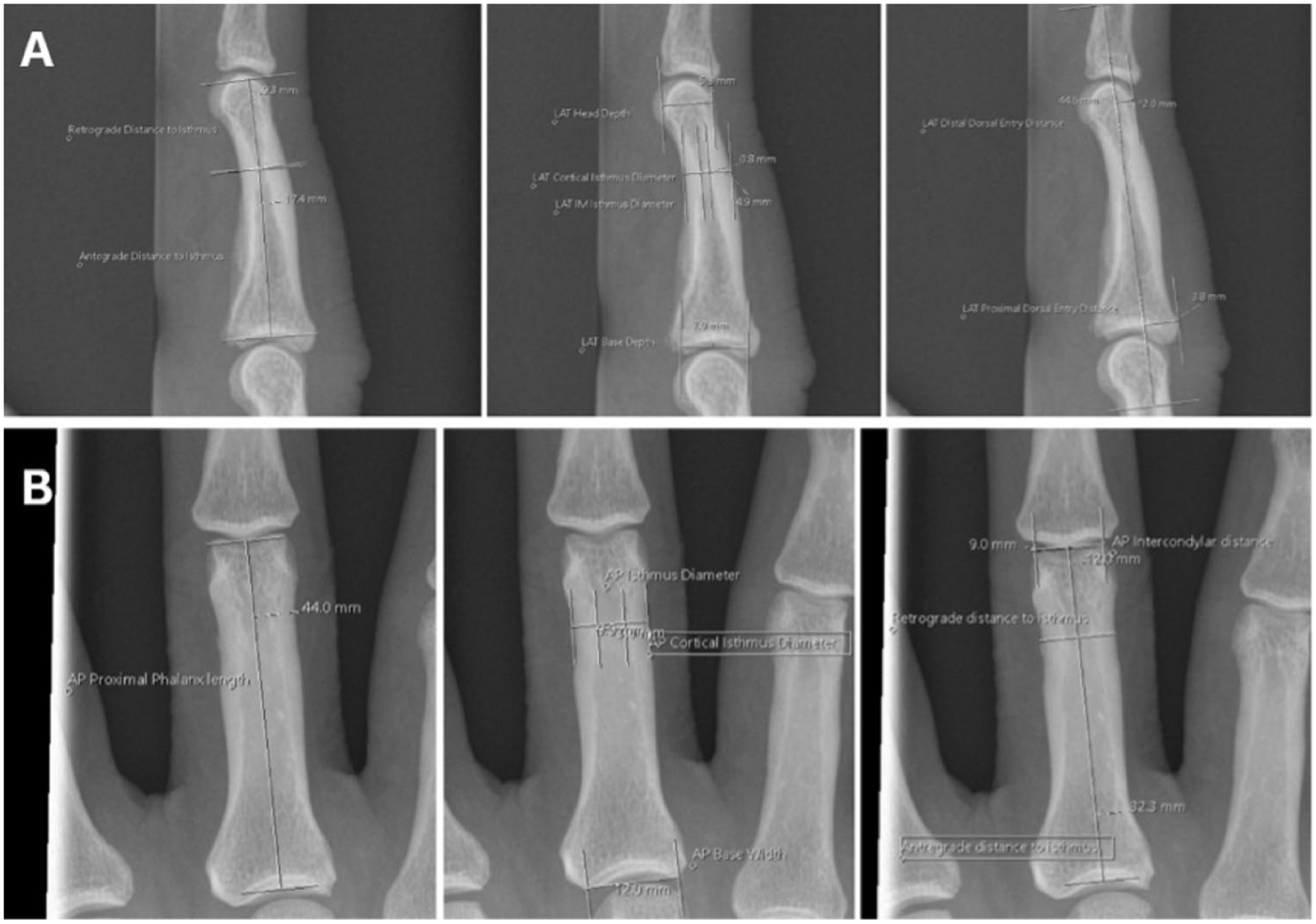
Lateral and posteroanterior radiographic measurements of the proximal and middle phalanges. (A) Lateral radiographic measurements of the proximal and middle phalanges. (B) Posteroanterior radiographic measurements of the proximal and middle phalanges.
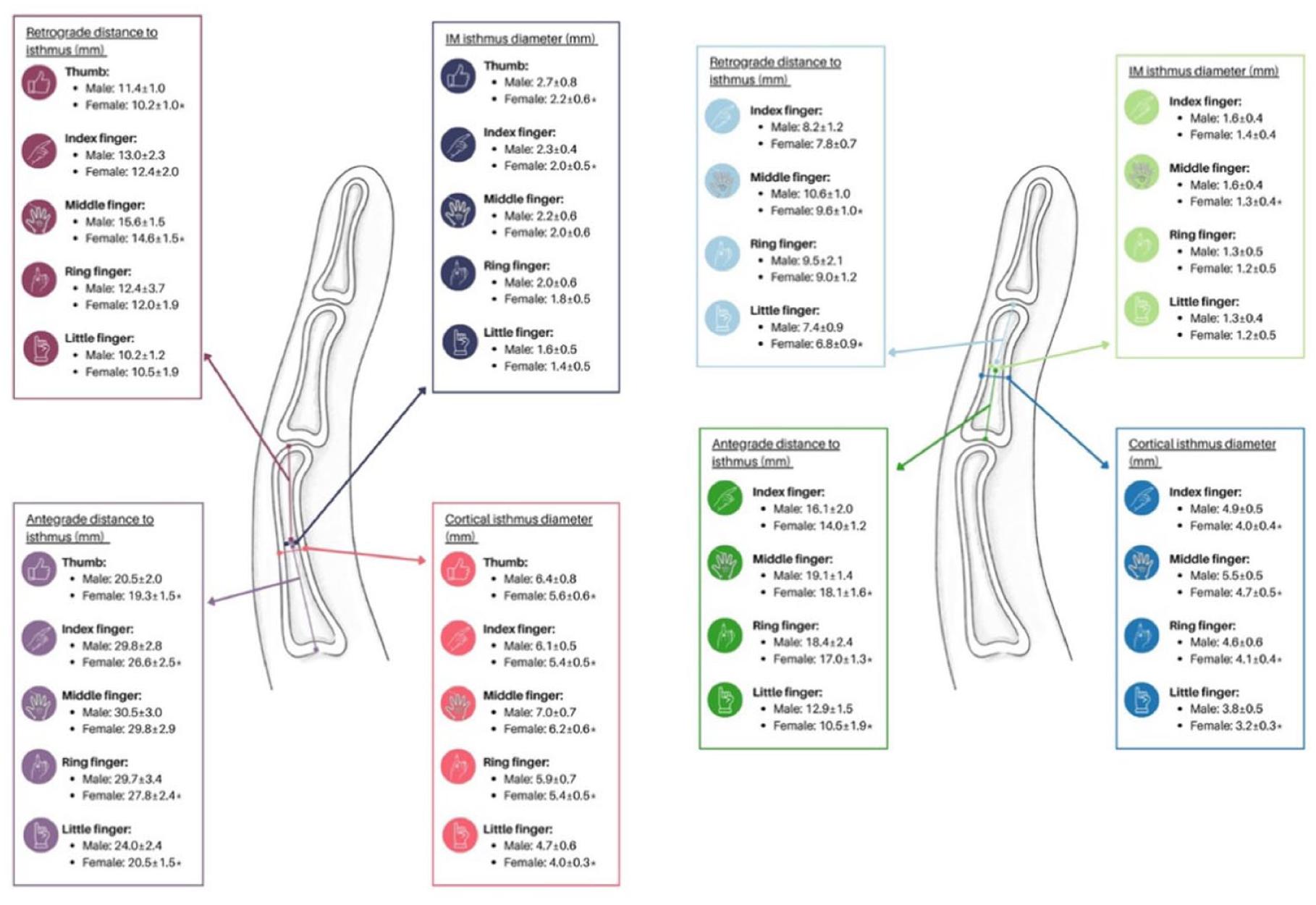
Schematic summary of the main measurements from the lateral view of the proximal and middle phalanges. Values are presented as mean ± SD.
Continuous variables were reported as mean (± standard deviation) with ranges. Normality was assessed using the Shapiro-Wilk test. Gender-based comparisons were performed using independent-samples t tests for normally distributed data and Mann-Whitney U tests for nonparametric data. A 2-tailed P-value <.05 was considered statistically significant.
Radiographic parameters were selected to reflect key anatomical constraints relevant to IM implant design and placement, including canal diameter, cortical thickness, implant length, and entry trajectory. Isthmus diameters assessed compatibility with implant core and trailing thread dimensions, whereas cortical measurements informed the risk of cortical breach with larger implants or reaming. Phalangeal lengths and anterograde/retrograde distances guided implant length selection and isthmus purchase. Head and base dimensions, along with intra-/trans-articular entry distances, characterised safe starting points and trajectories for anterograde and retrograde insertion.
Lateral parameters included: IM isthmus diameter, cortical isthmus diameter, head depth, base depth, proximal and middle phalanx length, anterograde and retrograde distances to the isthmus, retrograde intra-articular approach distance (distal dorsal entry distance – dorsal head to IM canal line), and anterograde intra-/trans-articular approach distance (proximal dorsal entry distance – dorsal base to IM canal line) (Figure 1).
Posteroanterior parameters included: IM isthmus diameter, cortical isthmus diameter, intercondylar (head) width, base width, proximal and middle phalanx length, anterograde distance to the isthmus (base to isthmus), and retrograde distance to the isthmus (head to isthmus) (Figure 1b).
For LAT views, absolute cortical width was calculated as: cortical isthmus diameter – IM isthmus diameter. Gender-based comparisons were performed, and all measurements were compared with specifications from 70 commercially available headless screws and IM nails.
This analysis included 70 distinct IM device specifications from 9 manufacturers, categorised into 47 headless compression screws, 13 headed or fully threaded screws, 6 IM nails, and 4 “twist-off” designs. Leading thread diameters ranged from 1.5 to 4.0 mm, with 11 specifications featuring diameters ≤2.0 mm, 33 between 2.1 and 3.0 mm, and 26 ≥3.1 mm. Trailing thread diameters reached up to 4.5 mm. While overall lengths spanned 8 to 80 mm, smaller-diameter systems (≤2.5 mm) were frequently limited to maximum lengths of 30 to 40 mm and offered in 1-mm to 2-mm increments. Conversely, larger-diameter systems (≥3.0 mm) reached up to 80 mm, typically utilising 2-mm to 5-mm increments (Table 3).
Results
Radiographs of 250 digits from 250 individuals (125 males, 125 females), comprising 50 digits from 50 individuals per ray (25 males, 25 females). Proximal phalanx measurements were obtained from the thumb through little finger, and middle phalanx measurements were obtained from the index through little finger. No contralateral digits were used. The mean age across all groups was 39.9 years (range, 16-89 years), with no significant difference in age between males and females for any digit (Table 1).
Radiographic Morphometric Measurements of the Proximal Phalanx by Digit and Gender.
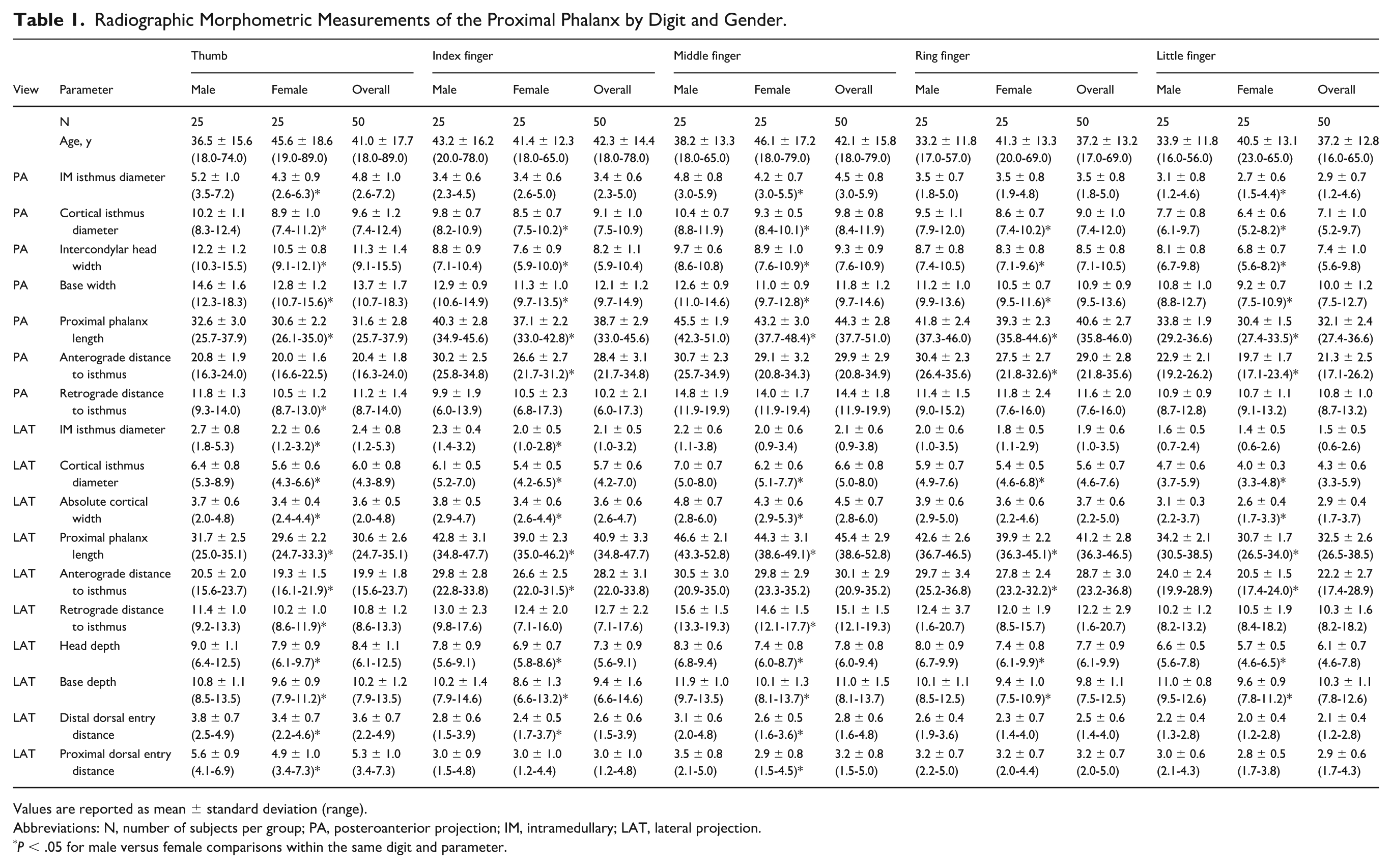
Values are reported as mean ± standard deviation (range).
Abbreviations: N, number of subjects per group; PA, posteroanterior projection; IM, intramedullary; LAT, lateral projection.
P < .05 for male versus female comparisons within the same digit and parameter.
Proximal Phalanx
On PA projection, the IM isthmus canal diameter was greatest in the thumb (4.8 mm) and smallest in the little finger (2.9 mm) (Table 1). Cortical isthmus diameter ranged from 9.8 mm (middle finger) to 7.1 mm (little finger). Total phalanx length ranged from 31.6 mm (thumb) to 44.3 mm (middle finger). The anterograde distance from the head to the isthmus varied from 20.4 mm (thumb) to 29.9 mm (middle finger), whereas the retrograde distance from the base to the isthmus ranged from 10.2 mm (index finger) to 14.4 mm (middle finger) (Table 1).
On LAT projection, the IM isthmus diameter ranged from 2.4 mm (thumb) to 1.5 mm (little finger). Cortical isthmus diameter measured 4.3 mm (little finger) to 6.6 mm (middle finger), and absolute cortical width averaged 2.9 mm (little finger) to 4.5 mm (middle finger). Proximal phalanx length ranged from 30.6 mm (thumb) to 45.4 mm (middle finger) (Table 1).
When stratified by gender (Table 1), males demonstrated larger osseous dimensions in most parameters on both projections. On PA views, cortical isthmus diameter was greater in males in every digit (eg, thumb 10.2 vs 8.9 mm; index 9.8 vs 8.5 mm; all digits P ≤ .0008), and base width and total length were similarly larger (eg, thumb base width 14.6 vs 12.8 mm; thumb length 32.6 vs 30.6 mm; P < .01). On LAT views, males also had larger cortical isthmus diameters (eg, thumb 6.4 vs 5.6 mm; middle 7.0 vs 6.2 mm; all digits P ≤ .0059), greater absolute cortical widths (eg, middle 4.8 vs 4.3 mm; P = .004), and increased head and base depths (eg, thumb head depth 9.0 vs 7.9 mm; base depth 10.8 vs 9.6 mm; P < .001). Phalangeal length was significantly greater in males across all digits on both projections (P < .01) (Table 1).
Middle Phalanx
On PA projection, the IM isthmus diameter ranged from 2.5 mm (ring finger) to 3.4 mm (middle finger) (Table 2). Cortical isthmus diameter was largest in the middle finger (7.9 mm) and smallest in the little finger (5.9 mm). Total bone length ranged from 18.4 mm (little finger) to 28.1 mm (middle finger). The anterograde distance from the head to the isthmus varied from 11.2 mm (little finger) to 18.3 mm (middle finger), whereas the retrograde distance from the base to the isthmus ranged from 7.0 mm (index finger) to 9.7 mm (middle finger) (Table 2).
Radiographic Morphometric Measurements of the Middle Phalanx by Digit and Gender.
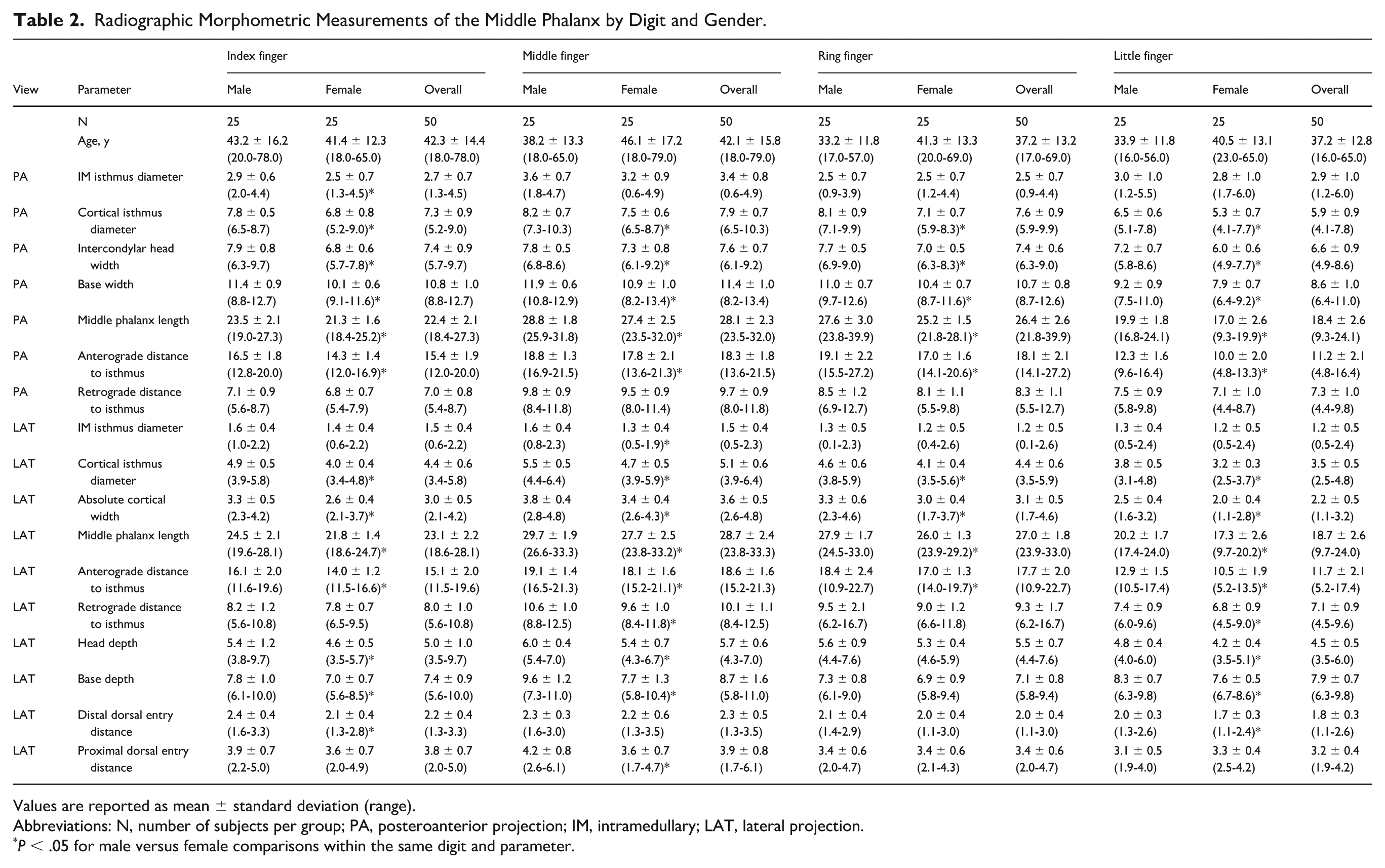
Values are reported as mean ± standard deviation (range).
Abbreviations: N, number of subjects per group; PA, posteroanterior projection; IM, intramedullary; LAT, lateral projection.
P < .05 for male versus female comparisons within the same digit and parameter.
On LAT projection, IM isthmus diameter ranged from 1.2 mm (ring and little fingers) to 1.5 mm (index and middle fingers), and cortical isthmus diameter ranged from 3.5 mm (little finger) to 5.1 mm (middle finger). Absolute cortical width averaged 2.2 mm (little finger) to 3.6 mm (middle finger), and phalangeal length ranged from 18.7 mm (little finger) to 28.7 mm (middle finger) (Table 2).
Gender-based analysis (Table 2) demonstrated larger cortical and overall structural dimensions in males. On PA views, cortical isthmus diameter was greater in men than females in every digit (index 7.8 vs 6.8 mm; middle 8.2 vs 7.5 mm; ring 8.1 vs 7.1 mm; little 6.5 vs 5.3 mm; all digits P ≤ .0002), with corresponding increases in base width and total length (P < .01). On LAT views, males again exhibited larger cortical isthmus diameters (eg, index 4.9 vs 4.0 mm; middle 5.5 vs 4.7 mm; all digits P ≤ .0018), greater absolute cortical widths, and increased head and base depths (eg, middle finger base depth 9.6 vs 7.7 mm; P < .001). Phalanx length on LAT projection was longer in men across all digits (P < .01) (Table 2).
Intramedullary Isthmus Diameter
On LAT radiographs, IM isthmus diameter varied by digit and phalanx level and was greater in males than females (Figures 3 and 4). In the middle phalanx, mean IM diameters ranged from 1.2 to 1.5 mm overall (Table 2), with gender-stratified means of 1.3 to 1.6 mm in males and 1.2 to 1.4 mm in females (Table 2). Proximal phalanges demonstrated larger canals, with overall means of 1.5 to 2.4 mm (Table 1) and gender-stratified means of 1.4 to 2.7 mm in males and 1.4 to 2.2 mm in females (Table 1), with the thumb exhibiting the greatest dimensions. Mean values closely approximated the medians (Tables 1 and 2).
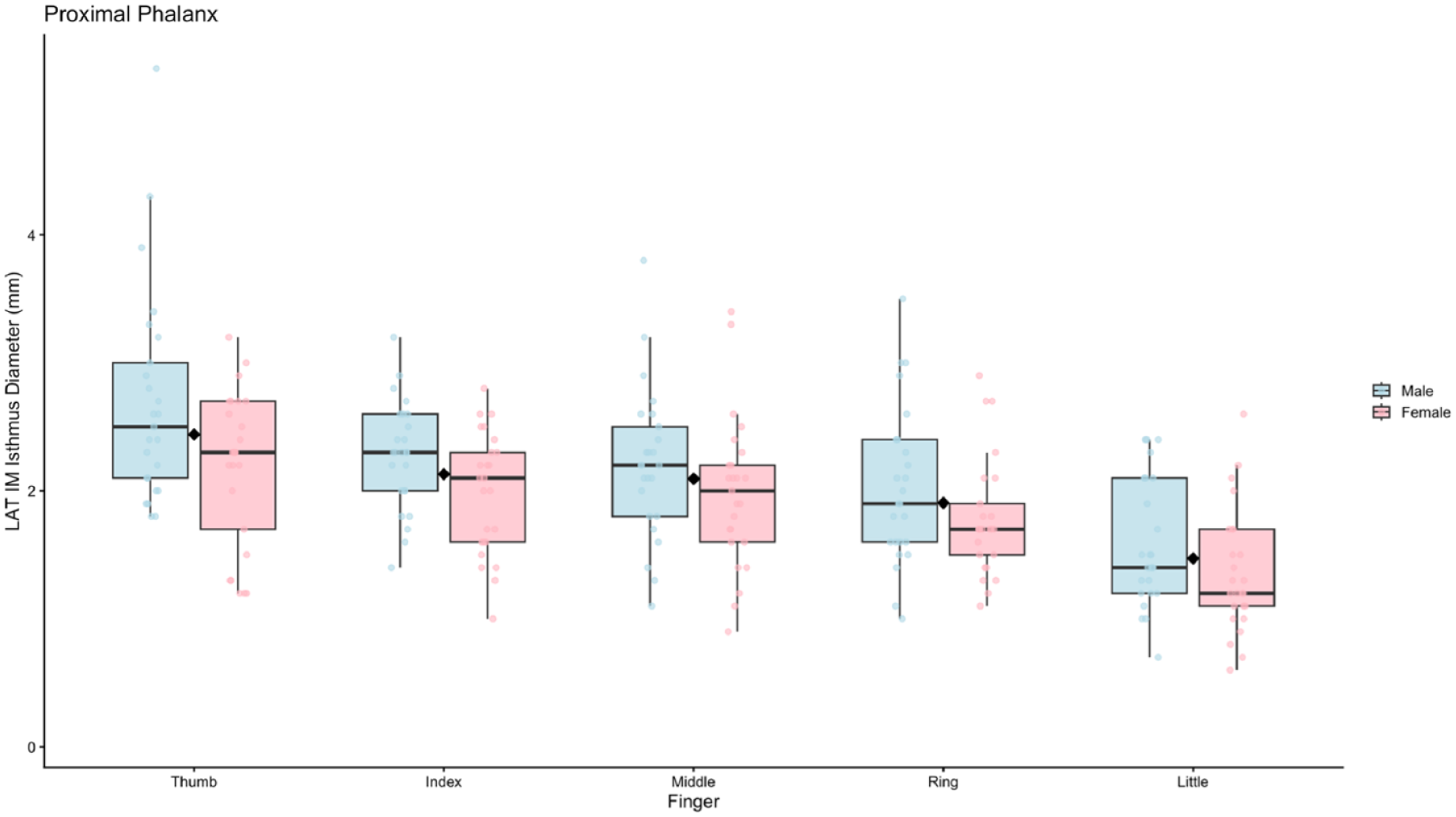
Gender-based differences in LAT IM isthmus diameter of the proximal phalanx by digit.
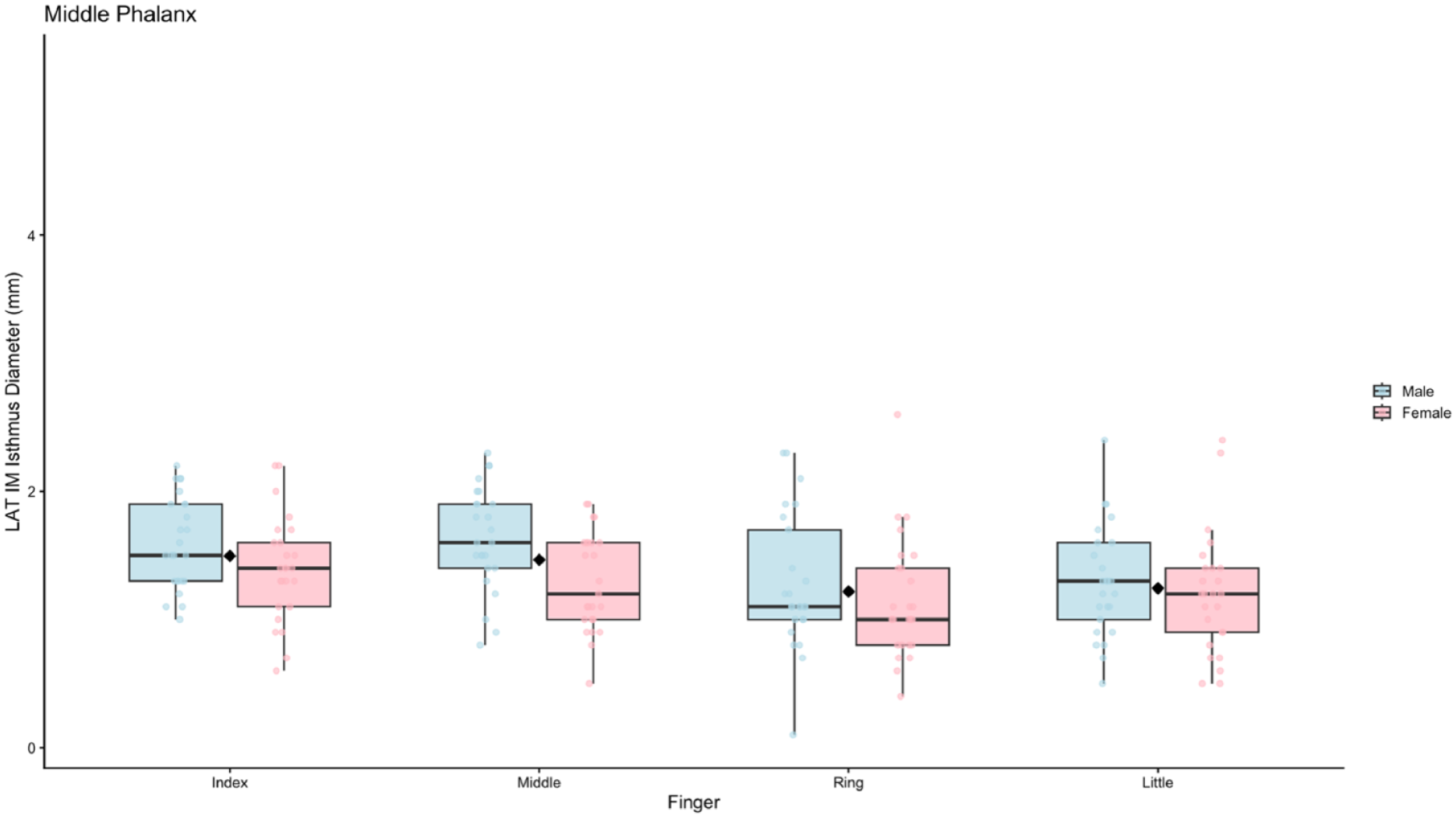
Gender-based differences in LAT IM isthmus diameter of the middle phalanx by digit.
IM Screws
Dimensions of commercially available headless compression screws and IM fixation devices used for phalangeal fracture fixation were tabulated across multiple manufacturers (Table 3). Leading thread diameters ranged from 1.5 to 4.0 mm. Where reported, trailing thread diameters ranged from 2.0 to 4.5 mm, consistent with the compressive design of headless compression screw systems. Cross-sectional area of the trailing head, available for a subset of implants, ranged from 3.1 to 15.9 mm². For several systems—including twist-off screws, IM nails, and partially threaded designs—trailing thread dimensions and/or trailing head cross-sectional areas were not publicly available (Table 3).
Dimensions of Commercially Available Headless Compression Screws and Intramedullary Fixation Devices Used for Phalangeal Fracture Fixation.
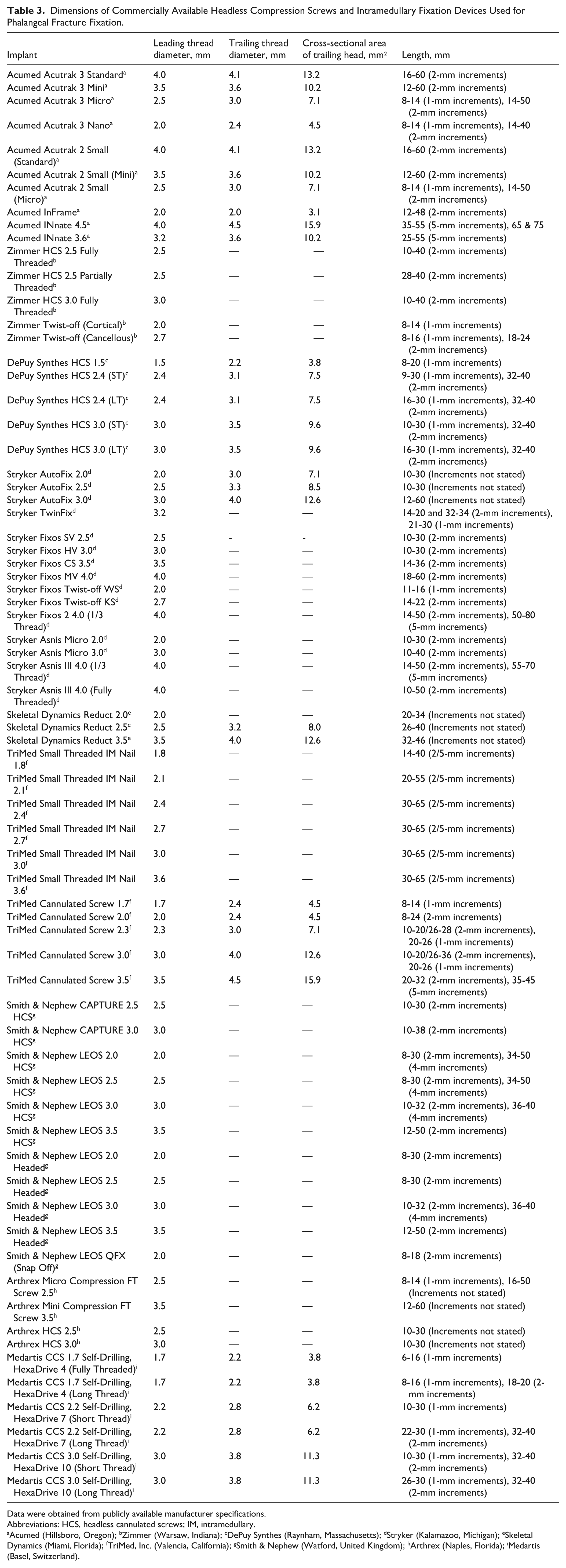
Data were obtained from publicly available manufacturer specifications.
Abbreviations: HCS, headless cannulated screws; IM, intramedullary.
Acumed (Hillsboro, Oregon); bZimmer (Warsaw, Indiana); cDePuy Synthes (Raynham, Massachusetts); dStryker (Kalamazoo, Michigan); eSkeletal Dynamics (Miami, Florida); fTriMed, Inc. (Valencia, California); gSmith & Nephew (Watford, United Kingdom); hArthrex (Naples, Florida); iMedartis (Basel, Switzerland).
A wide range of screw lengths was available across systems. Lower-diameter implants were commonly offered in shorter lengths (often 8-30 mm), whereas larger-diameter systems extended to maximum lengths of approximately 50 to 80 mm depending on manufacturer and design. Length increments varied by system, with 1-mm steps more frequently available in smaller screws and 2-mm to 5-mm increments more typical of larger implants. Several lower-diameter systems had upper length limits of 20 to 30 mm (and in some cases 40 mm), which may constrain optimal length matching in longer proximal phalanges, particularly in the index and middle digits (Table 3).
Discussion
A range of operative techniques exist for fixation of proximal and middle phalanx fractures, including percutaneous K-wire fixation, lag screws, plate-and-screw constructs, and IM HCS fixation.12-14 Each method offers distinct biomechanical advantages and limitations, and the choice of fixation is dependent on the fracture pattern and condition of the soft-tissue envelope. The optimal fixation method provides rigid fracture stability with preservation of the soft-tissue gliding layers and the ability to permit early motion to prevent joint stiffness. 15
Kirschner wire fixation is commonly used in the fixation of phalangeal fractures typically in a crossed configuration. They are a versatile option, with ease of use and ability to treat several fracture configurations.16,17 However, K-wires are frequently left protruding through the skin, exposing patients to risks of pin-site infection, wire migration, and irritation. 18 In addition, K-wire constructs may tether surrounding soft tissues and often necessitate a period of immobilisation, which can compromise early ROM and predispose to stiffness—particularly in the small joints of the hand.18,19
Plate-and-screw fixation provides rigid stabilisation, allows early mobilisation, but requires greater surgical exposure. The soft-tissue dissection necessary for plate application increases the risk of tendon adhesions, joint stiffness, and hardware irritation, and implant removal is not uncommon.20,21 These concerns are amplified in the phalanges, where the extensor mechanism is closely applied, and the tolerance for additional bulk is limited.22,23 Lag screw fixation is effective for long oblique or spiral fractures. However, it is not applicable to all fracture patterns and still requires precise implant sizing and trajectory to avoid cortical breach and irritation of tendons.14,24
Intramedullary headless cannulated screw fixation has emerged as a minimally invasive alternative that combines stable fixation with preservation of the soft-tissue envelope.25-27 By burying the implant entirely within the medullary canal, this technique minimises tendon irritation and allows for early mobilisation. 28 Intramedullary screws are available in both compressive and noncompressive options. The compressive screws are indicated in transverse and short oblique fractures where interfragmentary compression and absolute stability are achieved, whereas noncompressive or threaded nails are indicated in comminuted or length unstable fractures providing relative stability. 29 The IM canal of the phalanges can be approached through a retrograde or anterograde approach resulting in small extensor tendon and cartilage defects.30,31 Clinical studies have reported favourable outcomes with low complication rates in both metacarpal and phalangeal fractures.32-34 Nevertheless, the successful application of IM HCS fixation in the phalanges is highly dependent on accurate implant sizing, given the narrow and variable morphology of the IM canal. 25 Meticulous preoperative planning and operative technique is therefore essential when using IM HCS for the treatment of phalangeal fractures. This includes fracture reduction, accurate guidewire placement, and reaming. Inappropriately sized screws can result in jamming within the IM canal leading to iatrogenic fracture, screw breakage, or stripping of the head.
The present study provides a comprehensive radiographic assessment of proximal and middle phalanx morphology across all digits, with particular emphasis on IM isthmus dimensions as they relate to IM fixation. Our results demonstrate substantial variation in IM canal diameter by digit, phalanx level, and gender. On lateral radiographs—most relevant to screw diameter selection—the IM isthmus was consistently narrower than on PA views, with mean diameters ranging from approximately 1.2 to 2.4 mm. These findings underscore the importance of relying on lateral measurements when planning IM fixation, as PA views may overestimate canal capacity.
Across both proximal and middle phalanges, males demonstrated larger IM isthmus diameters and greater cortical dimensions than females. These differences were consistent across digits and projections and were most pronounced in the proximal phalanx. Such gender-based differences have direct implications for implant selection, as a screw diameter that may be appropriate in a male patient could pose a higher risk of iatrogenic fracture or cortical breach in a female patient, particularly in the ring and small fingers, where canals are narrowest. Furthermore, canal diameter alone does not define the safety margin for IM fixation; the cortical envelope at the isthmus governs how much reaming can be tolerated before risking cortical breach or iatrogenic fracture. In both the proximal and middle phalanges, males demonstrated significantly larger cortical isthmus diameters than females across all digits on PA and lateral projections (proximal phalanx: all digits P ≤ .0059 on LAT and P ≤ .0008 on PA; middle phalanx: all digits P ≤ .0018 on LAT and P ≤ .0002 on PA). This gender effect was mirrored by lateral absolute cortical width, which was generally smaller in females. The absolute cortical width represents both the dorsal and volar cortical thicknesses.
Digit-specific trends were also consistent: the ring and small fingers exhibited the smallest cortical dimensions, indicating the least “cortical reserve” for reaming. Notably, in the proximal phalanx, the small finger demonstrated the lowest lateral cortical metrics (female cortical isthmus diameter 4.0 ± 0.3 mm; absolute cortical width 2.6 ± 0.4 mm), and in the middle phalanx, the small finger again had the smallest lateral cortical envelope (female cortical isthmus diameter 3.2 ± 0.3 mm; absolute cortical width 2.0 ± 0.4 mm). Collectively, these findings suggest that the ulnar digits—particularly in female patients and at the middle phalanx level—are likely to be less tolerant of overreaming and therefore warrant heightened caution with reamer/screw upsizing even when the nominal canal diameter appears acceptable.
When our morphometric data were compared with the dimensions of currently available IM screws and nails, important mismatches became evident. Although a wide range of implants is commercially available, many systems offer leading thread diameters that exceed the mean lateral IM isthmus diameter of the middle and ring phalanges. Our findings suggest that screws with leading diameters of 2.0 to 3.0 mm most closely approximate native canal dimensions for most proximal and middle phalanges, particularly in females and in the ulnar digits. Larger-diameter devices (≥3.0 mm) appear most suitable for the thumb and, in select cases, the proximal phalanx of the middle finger, where canal dimensions are more capacious.
In addition to diameter, screw length must be considered in relation to isthmus location. Although a variety of screw lengths is available, shorter maximum lengths may limit the ability to achieve optimal purchase across the isthmus in longer phalanges, particularly in the index and middle fingers. Furthermore, trailing thread diameter and cross-sectional area—where reported—often substantially exceed the measured IM canal dimensions, raising concern for metaphyseal or articular violation if not carefully positioned. While the metaphysis is wider than the isthmus, the IM canal is irregular and often eccentric with thin cortices, so an oversized implant or slight malalignment can lead to cortical perforation. Although articular entry is intentional, an imprecise start point, off-axis trajectory, or excessive length may result in unintended joint penetration or subchondral disruption. These considerations reinforce the need for meticulous preoperative planning and familiarity with implant-specific dimensions.
The morphometric data in this study also have important clinical utility for the selection of IM arthrodesis devices for the metacarpophalangeal and proximal interphalangeal joints. Linked IM fusion systems offer several advantages, including rigid fixation, the ability to select predetermined arthrodesis angles, and a low-profile implant that minimises soft-tissue irritation.35,36 However, because these devices rely on IM fixation within the phalanges, their safe application is similarly constrained by the narrow and highly variable canal and cortical dimensions demonstrated in this study.
In particular, the anterograde and retrograde distances from the articular surface to the isthmus provide practical guidance for selecting appropriate implant length, whereas the IM isthmus diameter informs safe screw or nail sizing. Given the reduced canal dimensions and thinner cortices observed in the ring and small fingers—especially in female patients—these digits may be less tolerant of reaming and implant upsizing when performing IM, metacarpophalngeal joint or proximal interphalngeal joint arthrodesis. Accordingly, preoperative templating using digit-specific and gender-specific morphometric data should be considered essential when selecting IM fusion devices; this may be performed using radiographs of the involved digit or the contralateral digit.
Several limitations of this study merit consideration. First, measurements were derived from 2-dimensional radiographs and therefore cannot fully account for the 3-dimensional geometry of the phalanges. Although all images were obtained using standardised techniques and calibrated software, some degree of projectional variation is unavoidable. Computed tomography would provide 3-dimensional data with greater accuracy but with increased radiation dose. Despite this limitation, the radiographic measurements described in this study are applicable in clinical practice as they are derived from standard phalangeal views and are therefore useful for preoperative planning. Second, the study population consisted of individuals with normal bony anatomy; results may not be directly applicable to patients with deformity, malunion, or degenerative changes. Moreover, while bone density was not directly measured, the study population spanned a broad age range (16-89 years) to capture a representative spectrum of adult phalangeal anatomy. Third, while this study assumes that optimal screw fit occurs at the isthmus, there is limited clinical evidence directly linking isthmus engagement to superior outcomes in phalangeal fractures. Finally, the implant comparison was limited to devices with publicly available specifications and did not account for differences in thread design, pitch, material, or cannulation, all of which may influence fixation strength.
In conclusion, this study provides clinically relevant morphometric data that clarify the anatomic constraints governing IM fixation of the proximal and middle phalanges. Surgeons should be cognizant of the substantial variability in IM canal dimensions by digit and gender, particularly the narrow canals of the ring and small fingers and the consistently smaller dimensions observed in females. Careful implant selection—favouring smaller-diameter screws in most cases—and attention to lateral radiographic measurements may help reduce the risk of iatrogenic fractures, head stripping, screw jamming, and implant-related complications. Future advances in implant design that better reflect the native anatomy of the phalanges may further expand the safe application of IM fixation in hand fracture management. These data provide a radiographic framework for implant selection in phalangeal IM fixation and highlight the need for smaller-diameter devices tailored to digit-specific and gender-specific anatomy.
Footnotes
Ethical Considerations
This study was conducted in accordance with the ethical standards of the responsible institutional and national research committees and with the Declaration of Helsinki (1975, revised 2008).
Consent to Participate
This work was undertaken as a service evaluation (2026-0883-R) using retrospective radiographs acquired as part of routine clinical care. Radiographs were randomly selected and all data were anonymised prior to analysis. As this was a service evaluation using anonymised retrospective data, individual patient consent to participate was not required.
Consent for Publication
This study involved the retrospective analysis of anonymised human radiographic data only. No identifiable patient information, clinical images, or personal details are included in the manuscript. Therefore, individual patient consent for publication was not required. This study did not involve animal subjects.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The datasets generated and/or analysed during the current study are not publicly available due to institutional data governance and patient confidentiality restrictions but are available from the corresponding author on reasonable request, subject to appropriate ethical and legal approvals.