
Abstract
Background:
Perilunate dislocations and fracture-dislocations are high-energy wrist injuries. Standard treatment involves urgent closed reduction followed by open reduction and fixation of both radial (scapholunate) and ulnar (lunotriquetral) intervals. In our experience, fixation of the radial-sided injury alone (scaphoid fracture or scapholunate ligament tear) restores carpal alignment without separate lunotriquetral stabilization. We present the largest series to date using this approach.
Methods:
Between 2004 and 2025, 36 patients with acute perilunate injuries were treated by a single surgeon with a radial-sided only fixation protocol. All underwent urgent closed reduction, followed by Kirschner wire fixation for ligamentous injuries or headless compression screw fixation for scaphoid waist fractures. Patients were immobilized in a short arm cast for 8 weeks, with wires removed at that time. Radiographs obtained postoperatively and at final follow-up were assessed for scapholunate angle, scapholunate and lunotriquetral intervals, and presence of volar intercalated segment instability (VISI) or dorsal intercalated segment instability (DISI) deformity.
Results:
All patients achieved stable carpal alignment with radial-sided only fixation. At final follow-up, mean scapholunate angle was 55° (range 34°–84°), mean scapholunate interval 1.8 mm, and mean lunotriquetral interval 1.7 mm. No patients developed VISI deformity.
Conclusions:
Perilunate injuries can be effectively managed with fixation limited to the radial side, eliminating the need for lunotriquetral pinning. This series—the largest reported with this technique—challenges traditional dogma derived from Mayfield’s description and demonstrates excellent radiographic outcomes with a simplified surgical approach.
Introduction
Perilunate injuries are uncommon, usually occurring in young, male patients from high energy trauma.1-4 These injuries include perilunate dislocation, lunate dislocation, and perilunate fracture dislocation. The predictable sequence of injury propagates counterclockwise about the lunate—first disrupting the scapholunate (SL), followed by the capitolunate, and lunotriquetral (LT) articulations. Perilunate dislocation may be associated with fractures of the carpal bones, most commonly scaphoid waist fracture.2,5,6 Dislocation is best appreciated on the lateral radiograph, and as these are uncommon injuries, diagnosis may be missed on initial presentation. Perilunate injuries may be associated with other injuries about the wrist, including fractures and fracture-dislocations of the metacarpals, and distal radius. 5
Early treatment with open reduction and internal fixation is recommended. 2 Non-operative treatment has been described with unsatisfactory results. 7 - 9 The hallmark of treatment is percutaneous or open intercarpal pinning of the SL, LT, and midcarpal joints for lesser arc injuries with bony fixation for greater arc injuries. 1 While controversy exists regarding surgical approach and the need for direct soft tissue repair,10-14 intercarpal pinning across the LT interval is classically suggested to avoid late complications associated with carpal instability.4,6,15-17 Volar intercalated segment instability has been reported after perilunate injuries, with lunate hyperextension caused by an incompetent LT ligament.18-20
In contrast to this, in the cases we present in this series, we have found the LT interval to be anatomic following open reduction of the lunate and pinning of the SL articulation, or open reduction and fixation of associated scaphoid fracture. Fluoroscopy is used to confirm congruence of the SL and LT intervals after radial sided fixation. Postoperatively, patients are immobilized for 8 weeks in a short arm cast, with SL pins removed 8 weeks postoperatively. At each post-operative visit, patients were assessed for maintained reduction of the LT and SL intervals, as well as development of VISI deformity. This approach avoids the additional risks of introducing an ulnar-sided pin, including infection, nerve injury, or iatrogenic malreduction of the LT interval. Prior literature has reported pin tract infection in 4.5% of patients and ulnar nerve complications associated with 9% of LT pins in a cadaveric model.21,22 Prior series of perilunate injuries have not addressed the rates of LT malreduction.
The aim of this study was to evaluate radiographic outcomes in patients with radial-only fixation of perilunate injuries. Radiographic outcomes included development of VISI postoperatively, as well as SL angle, LT interval, SL interval, and the difference between SL and LT intervals. We hypothesized that patients with perilunate injuries that do not undergo ulnar sided fixation would have concentric reduction of the SL and LT intervals at final follow-up, without development of VISI deformity.
Methods
Patient Population
Our orthopedic billing database at a single academic level 1 trauma center was queried for patients with treatment of perilunate injury (Current Procedural Terminology [CPT] Codes 25685, 25670, 25695). Patients with surgery performed between January 1, 2004, and May 1, 2025, and age greater than 18 at time of surgery were included.
Surgical Technique
Surgeries were performed by a single hand-fellowship trained surgeon. All patients received an attempt of immediate closed reduction and casting in the emergency department prior to surgery.
For surgical exposure, we routinely used a longitudinal dorsal incision made over the dorsum of the wrist just ulnar to Lister’s tubercle. The extensor pollicis longus (EPL) is released and retracted radially with the extensor carpi radialis longus (ECRL). A longitudinal capsular incision is made to expose the scaphoid. In the setting of a volar dislocation, a volar approach was used for reduction as needed.
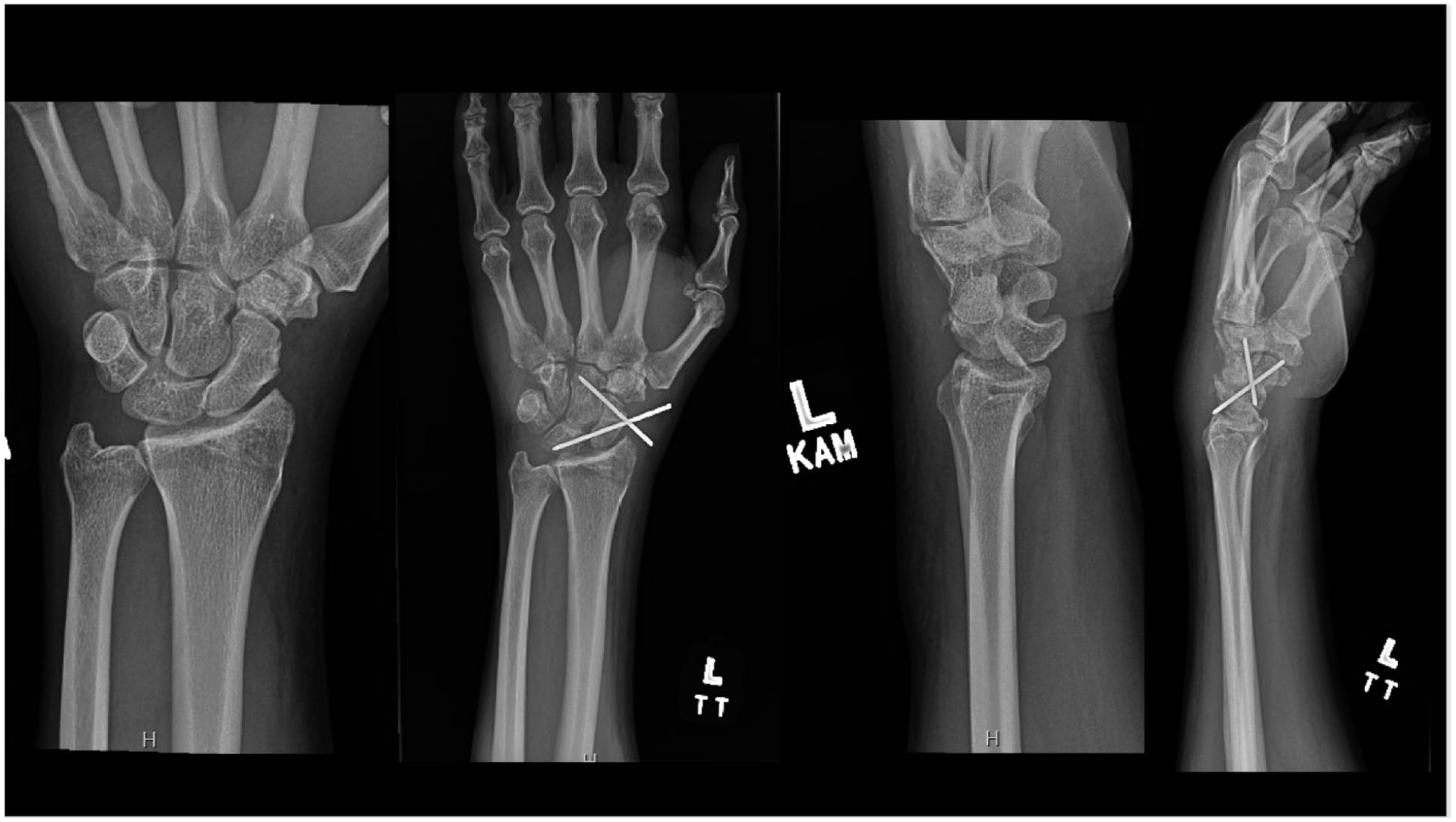
For trans-scaphoid injuries, the scaphoid was reduced and held with a Kirschner wire parallel to the path of the screw. Occasionally, Kirschner wires were used to help in fracture reduction. In this series, all trans-scaphoid injuries were treated with headless compression screws (Figure 1). For perilunate dislocations, the lunate was held in a neutral position, then the normal SL relationship was restored and held with introduction of 2 Kirschner wires, 1 across the SL articulation and 1 across the scaphocapitate articulation (Figure 2). Fluoroscopy was used to confirm anatomic carpal reduction. As the LT interval was anatomic for all patients after SL fixation, LT fixation was not performed for any patient. Intercarpal pins were removed at the 8-week postoperative visit.

Scaphoid fracture and volar lunate dislocation treated with radial-sided only fixation.
Perilunate dislocation treated with radial-sided only fixation.
Postoperative Management
Kirschner wires were buried beneath the skin. Postoperatively, all patients were immobilized in a short arm cast for 8 weeks, with subsequent removal of intercarpal pins.
Radiographic Review
Preoperative radiographs were examined to characterize the injuries according to the Herzberg classification, 23 as well as the presence of any associated fractures indicating greater arc injury. Postoperative radiographs were reviewed for SL angle, widening of the SL interval, or widening of the LT interval. Radiographs were obtained at each postoperative visit, which were planned for 2 weeks, 8 weeks, 3 months, 6 months, and 1 year postoperatively.
Results
Patient Cohort
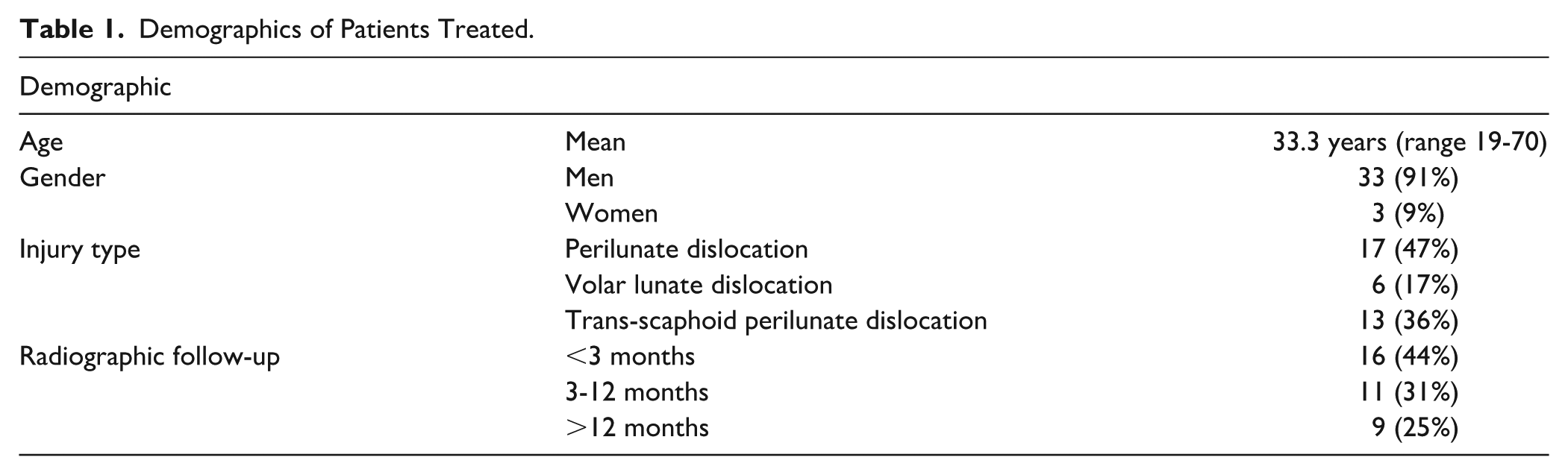
Thirty-six patients meeting inclusion criteria were identified (Table 1). 91% were men and 9% were women. Mean age of the sample was 33 years. 64% were purely ligamentous injuries (17 perilunate dislocations and 6 volar lunate dislocations), and 36% were greater arc trans-scaphoid fracture-dislocations. Mean time to final radiographs was 17 months (range 1-128 months).
Demographics of Patients Treated.
Radiographic Outcomes
Scapholunate angle was evaluated on postoperative radiographs and at final follow-up (Table 2). On postoperative imaging, mean SL angle was 51° (range 38-72). At final follow-up mean SL angle was 56° range (34-84). No patients had evidence of volar intercalated segment instability (VISI), defined as SL angle less than 30°.
Radiographic Results of Operative Treatment.
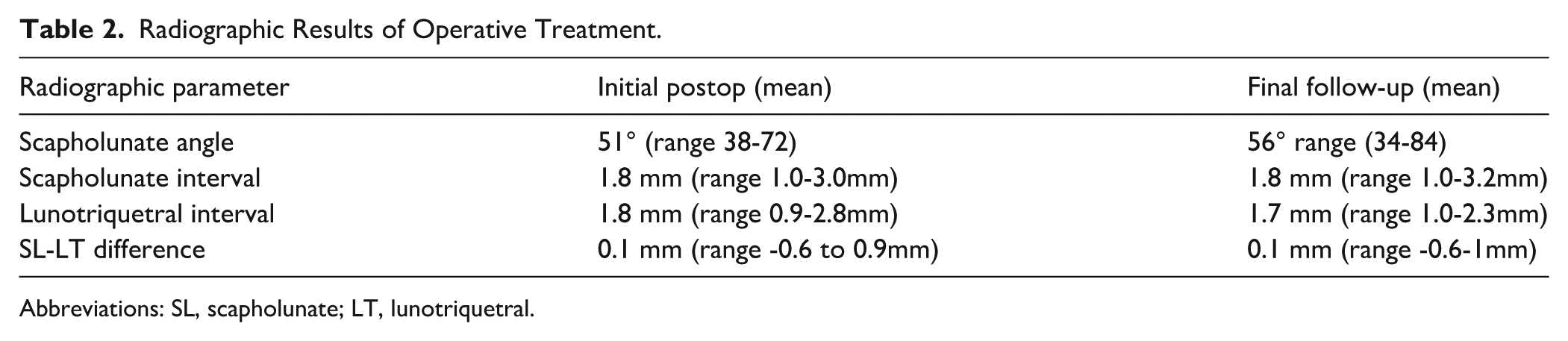
Abbreviations: SL, scapholunate; LT, lunotriquetral.
Scapholunate interval and LT interval were also evaluated on postoperative and final follow-up radiographs. To confirm concentric reduction of the carpus, the difference between SL and LT interval was calculated for each patient.
On postoperative radiographs, mean SL interval was 1.8 mm (range 1.0-3.0 mm), and mean LT interval was 1.8 mm (range 0.9 mm-2.8 mm). The mean difference between SL and LT interval was 0.1 mm (range -0.6 to 0.9mm).
At final follow-up, mean SL interval was 1.8 mm (range 1.0-3.2 mm), and mean LT interval was 1.7 mm (range 1.0-2.3 mm). The mean difference between SL and LT interval was 0.1 mm (range -0.6 to 1 mm). No patients had difference of SL and LT interval of more than 1 mm after fixation of the radial side, confirming concentric reduction of the radial and ulnar side.
Discussion
This study presents the largest cohort of patients with perilunate injuries treated without LT pinning. Only one previous study described treatment of 24 patients using only radial sided percutaneous fixation, with good results (mean Mayo score 84). However, this included only a subset of perilunate dislocations amenable to percutaneous fixation. 24 Our series includes patients with lunate dislocation and trans-scaphoid fracture dislocation, important considering the assumed rupture of the dorsal radiocarpal ligament with that severity of injury.
In our cohort, patients with perilunate injuries that do not undergo ulnar sided fixation achieved excellent radiographic outcomes. Our findings suggest that omission of the LT and lunocapitate pins is safe and avoids potential complications including pin site irritation or infection, nerve or vessel injury, malreduction of the LT interval, as well as additional time in the operating room.12,25 Radiographically, patients maintained congruence of the SL and LT intervals on initial postoperative radiographs and at final follow-up. Furthermore, no patients developed VISI deformity, or any radiographic evidence of LT or radiocarpal ligament instability.
This study is limited by the inconsistent follow-up within this cohort, as approximately half of patients did not return for follow-up after 3 months, and 25% were followed for over 1 year. This presents the possibility of a late presenting VISI deformity or development of post-traumatic arthritis that was not captured in this cohort. In the setting of trauma, VISI deformity has been described as early as the time of injury.26,27 However, dynamic instability is also described chronically after injury as secondary stabilizers fail, resulting in the development of visible deformity (VISI or DISI) 3 to 12 months after injury.28,29 For the patients followed greater than 1 year, this is likely sufficient time to detect VISI deformity. For patients followed less than 3 months, this interval offers the ability to evaluate SL and LT reduction. However, later deformity or arthritic changes are still possible. For patients followed between 3 and 12 months, based on prior literature it may be possible to observe VISI deformity in some patients, though the deformity may also develop later as secondary stabilizers degenerate.
Furthermore, in prior series of perilunate injuries, radiographic outcomes have not shown strong correlation with functional outcomes. 23 Despite the high percentage of patients who develop radiographic arthritis after perilunate injury, prior studies were unable to show a difference in functional outcomes for patients who developed radiographic arthritis after perilunate dislocation.23,30
These results are in contrast to existing case reports suggesting that ulnar-sided carpal instability can occur.18,31,32 Multiple cases of VISI have been reported even in the presence of LT pinning. Viegas reported patients without LT pin that went onto VISI in a clinical outcomes study, and a VISI case even with pinning. 33 Authors have also advocated for LTIL repair in addition to pinning. 32
Our hypothesis is that, even though our patients sustain injury to the structures known to be involved in development of VISI (Lunotriquetral interosseous ligament [LTIL], palmar LT ligament, dorsal radiocarpal ligament)—the LT interval is typically reduced after radial sided fixation and can be adequately held in this position with short arm cast immobilization, the standard postoperative care regimen with or without ulnar sided fixation. To this point, even for patients with isolated LT ligament injuries, good outcomes have been reported after nonoperative treatment with immobilization alone. 34 Compared with isolated inter-carpal ligament tears, we hypothesize that perilunate injuries result in a more robust scar reaction, which explains the more predictable healing of the injured structures including the LTIL in patients with perilunate injury.
It is possible that for patients who did develop VISI after treatment of perilunate injury, the patients were not immobilized adequately. We find this component key—as in biomechanical studies of VISI, the patients underwent sectioning of the essential structures, followed by repeated axial loading in the lab to develop the VISI pattern. 16 Based on this, it is reasonable to suggest that even if our patients sustained traumatic injury to all of these essential structures to develop VISI, they will avoid carpal instability if held reduced while the normal cascade of biological changes is allowed to restore these structures.
This study does have limitations to note when interpreting the results. Due to the retrospective nature of the study, our postoperative data also did not include functional measures such as range of motion or a clinical examination of LT instability.
Additionally, as the rate of VISI after operative treatment of perilunate injury has not been reported, it is not clear whether our study was powered to detect these rare complications. It is also likely that each patient sustains a unique degree of soft tissue injury and many patients do not have the commensurate ligamentous injury required to develop VISI—in fact, Mayfield noted that the Dorsal radiocarpal ligament (DRCL) injury occurs with stage 4 injuries with complete dislocation of the lunate. Finally, the postoperative radiographs used for this study would only identify static VISI. It is possible that we are missing dynamic VISI which correspond with LTIL and palmar LT ligament injury.
Another possible source of bias is the percentage of lost to follow-up. Of the 36 patients treated using this protocol, 18 did not return for radiographs after 3 months. It is possible that some of these patients developed complications after the study period and did not return for follow-up.
The results of this cohort demonstrate that perilunate injuries can safely be treated without LT pinning. This strategy produces excellent radiographic outcomes, concentric reduction of the carpus without radiographic evidence of carpal instability, and challenges the dogma based on Mayfield’s original anatomic description.
Footnotes
Ethical Considerations
This study was approved by our institutional review board.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.