
Abstract
Background:
Soft tissue reconstruction using a pronator quadratus pedicled rotational flap (PQPRF) has not been described in detail previously. This cadaveric study assesses surface-area mapping for PQPRF reconstruction and technical considerations for surgical use.
Methods:
Fresh-frozen trans-humeral cadaveric amputation specimens were used. The PQPRF and its anterior interosseous artery (AIA) pedicle were isolated to assess muscle perfusion and to map the anatomic feasibility of rotational flap coverage. The AIA pedicle was created by its distal to proximal dissection, preserving the distal most flexor pollicis longus neurovascular pedicle to facilitate flap mobilization and simulate flap elevation. Following India ink injection of the brachial artery, muscular perfusion was confirmed. Pronator quadratus pedicled rotational flap dimensions and its rotational arc relative to local anatomy references were measured. Descriptive statistical analyses were reported.
Results:
Seven cadaveric specimens were evaluated. Mean PQPRF dimensions were 54 × 37 mm ± 5.8 × 3.5 mm. Anterior interosseous artery pedicle length was 84 ± 17 mm. Pronator quadratus pedicled rotational flap rotational arc observed was: distal: 8 ± 6.9 mm proximal to the radial styloid and 20 ± 13.2 mm proximal to the ulnar styloid; the flap covered dorsal and radial to the mid-sagittal line of the radial forearm 38.6 ± 24.7 mm. In a proximal direction, the flap covered up to 44.3 ± 31.6 mm distal to the medial epicondyle. Dorsal forearm and wrist coverage using the PQPRF via an interosseous membrane window was measured to 9.2 ± 7.1 mm distal to Lister’s tubercle.
Conclusion:
The PQPRF is reliably perfused based on an anterograde AIA vascular supply and is a variable but useful option for wrist and forearm soft tissue reconstruction.
Keywords
Introduction
The pronator quadratus (PQ) muscle has been described previously as a reconstructive option as a pedicled flap, a free flap, or as part of a composite vascularized bone graft. Along with the pronator teres, the PQ pronates the forearm, and this redundant function permits sacrifice of the PQ without substantial strength or range of motion deficit.1-3
Numerous soft tissue reconstructive options have been described for full-thickness defects of the forearm and wrist. 4 When muscular flap reconstruction is considered, regional rather than distant (free) flap reconstruction is favored where possible, although regional donor options in the forearm and wrist are limited, often due to the zone of injury and anatomical constraints of the donor flap. Sacrifice of major vessels can be associated with moderate risks. 5 The reverse radial forearm flap (RRFF) sacrifices the radial artery as a pedicle for distal coverage which creates a low, but not insignificant, risk of thumb devascularization when normal radial and ulnar artery connections are absent or compromised. 5 The posterior interosseous artery flap (PIAF) is another forearm-based flap, which involves donor site morbidity and elevated risks of venous congestion. 4
The PQ muscle is supplied by the anterior interosseous artery (AIA), which terminates approximately 1 cm distal to the proximal edge of the muscle belly.6-8 Distal radius perfusion is highly redundant with contributions from AIA, radial artery, ulnar artery, posterior interosseous artery, and supra-retinacular arteries. This redundant vascular supply permits sacrifice of the AIA distal to the flexor pollicis longus (FPL) perforators, maintaining perfusion of the isolated pronator quadratus pedicled rotational flap (PQPRF). 9 Therefore, the PQPRF is an attractive option for potential regional soft tissue reconstruction due to its availability via the flexor carpi radialis (FCR) approach to the wrist and the lack of need for microvascular anastomosis such as with a distant/free flap method.
Although previous reports have described using the PQPRF for reconstruction of upper extremity soft-tissue defects,10-13 the surgically relevant coverage area of the PQPRF has not been determined. This cadaveric study assesses the anatomical extent of PQPRF reconstruction of soft tissue deficits, confirms flap perfusion based on the AIA, and describes technical considerations for surgical flap use.
Methods
Seven trans-humeral, fresh-frozen cadaveric specimens were obtained following institutional review board exemption by the Colorado Multiple Institutional Review Board as a cadaveric study with deidentified, previously collected specimens. All specimens were determined to be without evidence of prior trauma or surgical intervention. For each specimen, exposure of the PQPRF was done via an approximately 15-cm incision overlying the FCR tendon beginning just proximal to the volar wrist crease, extending proximally. Through the floor of the FCR sheath, the PQ was exposed on the volar surface of the distal radius and ulna. Dissection was carried proximally between flexor digitorum profundus ulnarly and FCR radially. The distal FPL origin was elevated off the radius to facilitate exposure of the PQ and the anterior interosseous neurovascular bundle. The PQ muscle belly was elevated from its osseous attachments from distal to proximal, preserving the AIA and accompanying veins. Perforating vessels from the AIA distal to FPL were isolated and ligated with 2-0 silk ties (Perma-Hand Silk, Ethicon, Bridgewater, New Jersey). The distal most arterial perforator from AIA and accompanying anterior interosseous nerve (AIN) branch to FPL were identified and preserved, thus defining the proximal extent of the PQ pedicle.
Following PQPRF mobilization, flap dimensions (length and width) specific to the muscle were measured. Flap length was defined as the greatest proximal to distal measurement, and flap width was defined as the greatest muscle measurement from radial to ulnar with accompanying PQ muscle fascia. The AIA pedicle length was measured from the distal AIA/AIN perforator to the FPL to the AIA at the proximal PQ muscle belly. The presence of venae comitantes was recorded. The arc of rotation of the PQPRF was measured to determine the extent of anatomical coverage in the forearm and wrist. Flap placement was done avoiding excessive tension across the arterial pedicle to replicate the clinical scenario for reconstruction of a soft tissue defect. Standardized measurements of the position of the distal PQ muscle margin were obtained relative to the following anatomical landmarks: medial epicondyle (proximal), mid-sagittal line (radial), radial and ulnar styloid (distal, volar), and Lister’s tubercle via trans-osseous membrane dorsal and distal (distal, dorsal).
Before vascular injection and following PQPRF isolation, AIA perforators and proximal arm veins were ligated to minimize unnecessary India ink extravasation. The brachial artery was cannulated with a 14 g angiocatheter (Becton, Dickinson and Company, Franklin Lakes, New Jersey), which was secured with a circumferential 0 silk suture (Perma-Hand Silk, Ethicon, Bridgewater, New Jersey). The artery was irrigated with a 1:50 mixture of soap (Dawn; Procter and Gamble, Kansas City, Kansas) and tap water before injection with India ink (Higgins, Chartpak, Leeds, Massachusetts) pressurized through a 10-mL syringe for 10 minutes. The AIA pedicle was transected, and the PQ muscle belly was sectioned in 2-mm transverse sections to assess distal capillary perfusion of India ink using optical loupe magnification.
Descriptive statistical analyses were performed with SPSS statistical software (IBM Inc., Chicago, Illinois) for each specimen and categorized based on the sex of the specimen.
Results
Seven trans-humeral cadaveric specimens, 3 left and 4 right, from 6 men and 1 woman (ages 52-69 years; average: 65 years) were used. The mean flap dimension was 54 × 37 mm ± 5.8 × 3.5 mm, with an average forearm possible coverage area of 20.2 cm2 ± 3.8 cm2. The AIA pedicle length was 84.3 ± 17.2 mm. A single vein was noted traveling within the pedicle in all specimens (Table 1, Figure 1). Distal reach of the flap margin was measured; the PQ flap reached 8 ± 6.9 mm proximal to the radial styloid and 20 ± 13.2 mm proximal to the ulnar styloid. The flap was able to be rotated radially and dorsally to extend beyond the mid-sagittal line by 38.6 ± 24.7 mm. Proximally, the flap could be placed up to 44.3 ± 31.6 mm distal to the medial epicondyle (Figure 2). The PQPRF could be transferred dorsally via an interosseous membrane window to facilitate coverage up to 9.2 ± 7.1 mm distal to Lister’s tubercle (Figure 3). Vascular injection with India ink revealed full flap perfusion after muscle sectioning.
Specimen Characteristics, Pedicle and Flap Characteristics, Excursion of Pedicled PQ Flap to Relevant Anatomic Landmarks.
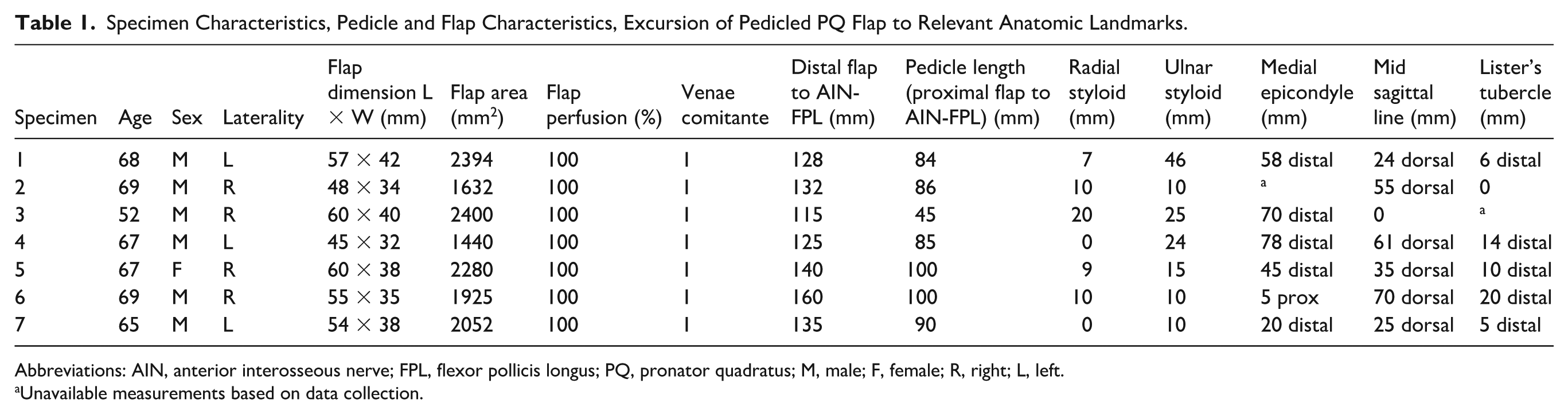
Abbreviations: AIN, anterior interosseous nerve; FPL, flexor pollicis longus; PQ, pronator quadratus; M, male; F, female; R, right; L, left.
Unavailable measurements based on data collection.

Surgical application of pronator quadratus pedicled rotational flap: (A) dorsal forearm, (B) dorsal radial styloid, (C/D) medial elbow, (E) dorsal wrist, (F) dorsal ulnar styloid, (G) volar ulnar styloid, and (H) volar radial styloid.
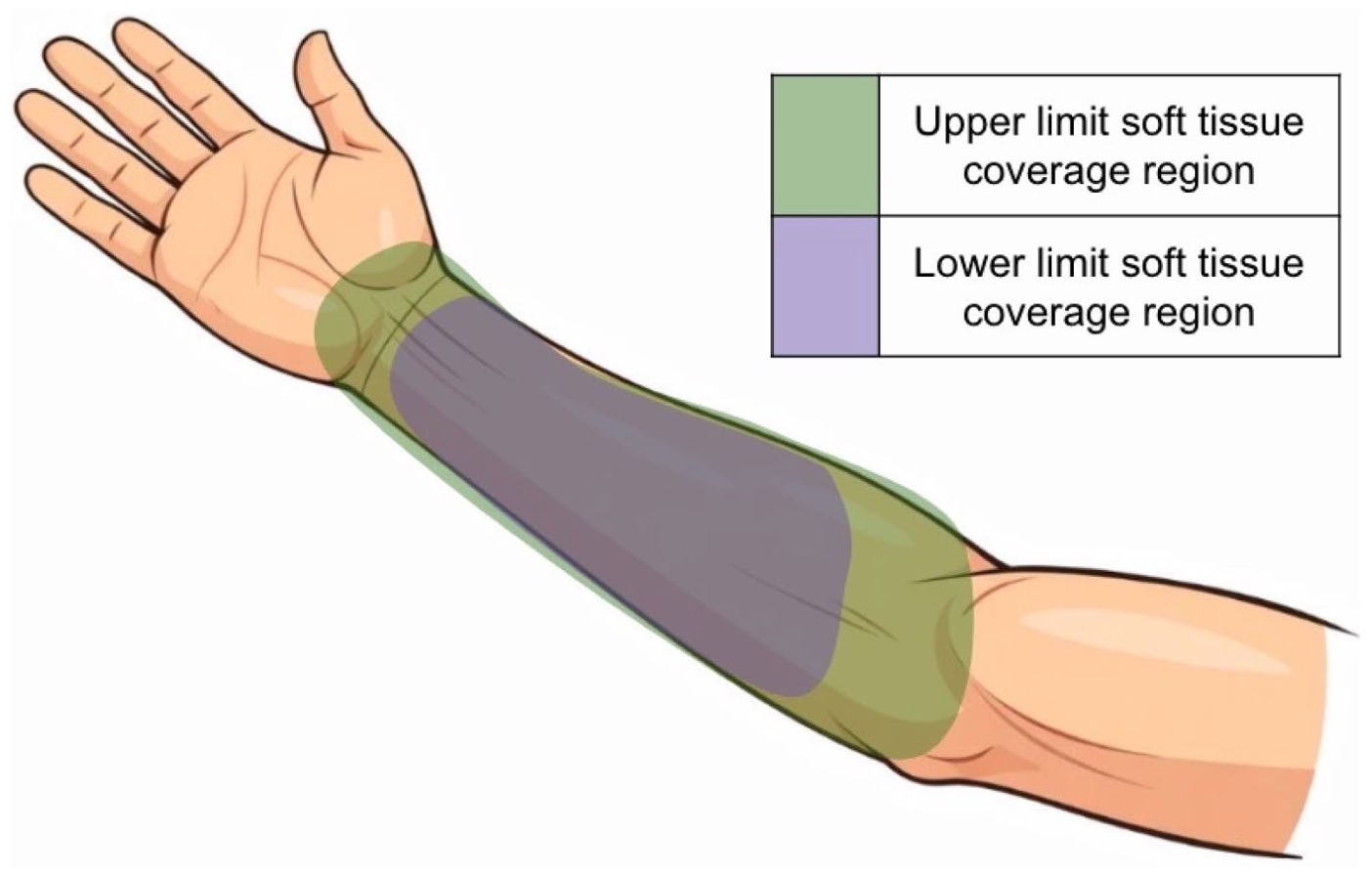
Volar forearm pronator quadratus pedicled rotational flap regional coverage heat map.
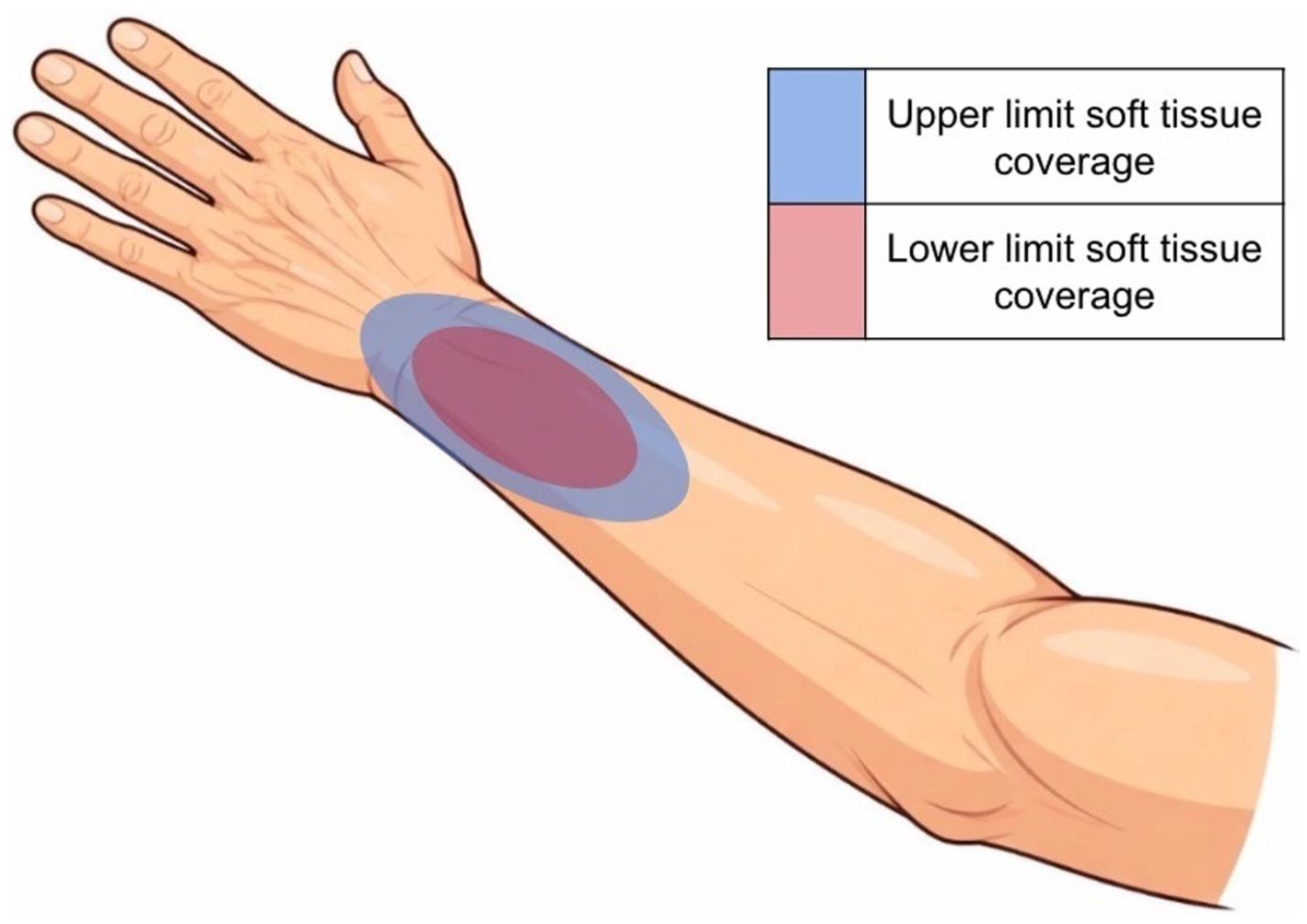
Dorsal forearm pronator quadratus pedicled rotational flap regional coverage heat map.
Discussion
Clinical utility of the PQ muscle as a source of vascularized soft tissue for wrist or forearm reconstruction should consider anatomic constraints, donor site morbidity including functional deficits, and technical consistency. The PQ contributes to forearm pronation in conjunction with the pronator teres. McConkey et al 3 demonstrated an average 21% decrease of pronation torque from supination to 45° of pronation with temporary PQ muscle paralysis. However, repair of PQ following volar plate fixation for distal radius fractures or PQ harvest as a free flap has not been shown to affect pronation strength or functional outcome scores.14,15 Electrodiagnostic studies by Gordon et al 16 and Stuart 6 demonstrate superficial head PQ activity with pronation as well as activity of the deep head with grip and supination, contributing to notion that the deep head of PQ is involved in stabilization of the distal radioulnar joint (DRUJ). 17 Despite these electrodiagnostic findings, DRUJ instability and palmar carpus instability are not observed in volar distal radius plating without PQ repair, likely because of the restraints provided by the palmar capsuloligamentous structures.14,18 The redundant nature of PQ’s functions and reassuring outcomes in PQ-deficient patients make PQ a reasonably expendable muscle for flap harvest. 10
Stuart 6 described the PQ gross morphology as a trapezoidal muscle with distinct superficial and deep heads, originating from the volar border of the radius and inserting into the dorsal-medial border of the ulna. Previously reported dimensions of the PQ muscle have ranged from 4.6 to 5.5 cm in length and 3.8 to 5 cm in width, which are similar to those dimensions identified in this current study (5.4 ± 0.37 cm and 3.7 ± 0.35 cm, respectively).7,8,10,13 A consistent PQ neurovascular supply involves the AIA and innervation from the AIN, both of which course along the anterior surface of the interosseous membrane before penetrating the deep head and into the superficial head of PQ 1 to 2 cm distal to the proximal edge of the muscle.6,7,10,13 Typically, the AIA and AIN to PQ are accompanied by a single anterior interosseous vein (AIV), which was observed in this study; however, 2 venae comitantes have been reported accompanying the neurovascular bundle to the distal extent of the pedicle. 13 The presence of an AIV with a raised PQ flap improves venous drainage. 8 Additional sub-millimeter-diameter minor pedicles to PQ from the radial and ulnar arteries are reliably present, creating anastomoses with redundant muscular perfusion that can be safely sacrificed without substantial risk to muscle viability. 13 Maintained muscle perfusion after PQPRF isolation on its pedicle was confirmed across all specimens with the use of India ink injection in our study and is consistent with previous vascular studies of the PQ muscle. Lee et al 19 injected 25 cadaveric specimens with colored latex and Thomas et al 13 injected 7 fresh-frozen cadavers (4 men and 3 women) with lead oxide-gelatin, revealing AIA as the primary pedicle to the PQ.
During distal to proximal dissection of the anterior interosseous neurovascular bundle from the PQ to the FPL, several small perforating vessels were encountered and required ligation to mobilize the PQPRF. For our study, 0-Silk ties were used to tie off vessels; however, the use of ligature clips could enhance the operative efficiency given the number of small perforators present. One constant named perforator that requires attention in this approach is the dorsal cutaneous perforating branch (DPB) of the AIA. Thomas et al 13 reported the DPB is an approximately 1.2-mm-diameter artery which arises 4 cm proximal to Lister’s tubercle and contributes arterial flow to the skin over the distal third of the forearm and wrist as well as the 1,2 intercompartmental supra-retinacular artery. In planning complex upper extremity reconstruction, consideration should be given to sacrificing DPB given these potentially important contributions to dorsal forearm and wrist structures. 20
A clinically relevant rotation arc for tissue transfer for regional pedicled flaps is limited by the pedicle length and potential constraints of local anatomy. Flap isolation and mobilization should not compromise adjacent functional structures. 20 In the PQPRF, flap mobilization is limited by the distal most AIN perforator to FPL. In our study, the average pedicle length from the distal most FPL perforator to the proximal muscle belly measured 8.4 ± 1.7 cm. Previously reported pedicle lengths have varied significantly, ranging from 5 to 13 cm.7,8,10,12,13,21 Discrepancy in these measurements is multifactorial, relating to ethnic and gender dimorphism of the PQ and AIN as well as limitations inherent to cadaveric models. The arc of rotation of a PQ pedicle flap on the volar forearm is approximately 6 cm as reported by Dellon and Mackinnon 10 and Thomas et al. 13
Dellon and Mackinnon 10 reported favorable clinical outcomes in a case series consisting of 9 patients who underwent pedicled PQ flap combined with various nerve reconstruction procedures to minimize neuroma formation. The authors concluded that their pedicled PQ flap was technically difficult to use for regional soft tissue reconstruction alone and was best suited in conjunction with neurolysis and/or tenolysis procedures. 10 Thomas et al 13 reported successful outcomes in 2 patients who underwent pedicled PQ flap reconstruction followed by split tissue skin graft for local soft tissue coverage of the volar forearm and flexor surface of the wrist. Husain et al 22 performed a retrospective review comparing PQ flap transposition following volar plate fixation of distal radius fractures which revealed a relative risk reduction of 86.4% in flexor tendon irritation or rupture compared with conventional techniques.
Reported indications for PQPRF reconstruction have been limited to local/regional applications in the volar distal forearm and wrist; no studies have defined the potential soft tissue coverage areas beyond general remarks about arc of motion.10,13 For example, in a review of flap coverage of the upper extremity, Benanti et al 4 describe only the RRFF and PIAFs as regional pedicled soft tissue reconstruction options for coverage of distal wrist and hand defects.
We found the greatest variability in PQPRF coverage when it was reflected proximally, with flap rotation ranging from 5 mm proximal to 70 mm distal to the medial epicondyle. Reliable flap coverage extended at least to and often past the mid-sagittal line both radially and ulnarly along the course of the forearm to the distal wrist crease. Robust dorsal coverage was facilitated by dorsal transfer of the PQPRF through a window in the interosseous membrane; a dorsal 4 to 6 cm longitudinal skin incision facilitated flap retrieval. Flap coverage included the extensor compartments, Lister’s tubercle, radial styloid, or ulnar styloid with no tension on or compression of the pedicle. The lower limit of soft tissue coverage shown in Figures 2 and 3 reflects the minimum expected excursion of the PQPRF around its pedicle for coverage planning purposes. It is important to note that these heat maps were overlaid on AI-generated images of the upper extremity and demonstrate the potential extents of regional coverage, not a total expected area of soft tissue coverage from a PQPRF.
Limitations
There are inherent limitations in our study design. Variations in absolute measurements (ie, flap width, length, depth) between specimens are expected based on factors other than sex and age. Anatomic variations exist and may not be considered in this small number of specimens. There may be differences in tissue mobility comparing surgery in cadaveric specimens versus the in vivo setting, potentially underestimating PQPRF coverage. Similarly, tissue viability following flap mobilization cannot be assessed in a cadaveric model. This study may provide predictive power for assessment of flap coverage relative to identifiable anatomic markers (ie, radial styloid or medial epicondyle), but our model does not account for physiologic influences on flap viability and wound healing such as patient comorbidities or the local zone of injury. Despite these inherent limitations, the outcomes of this study provide a reasonable guide for PQPRF use during regional soft tissue reconstruction.
Conclusions
The PQPRF is a relatively thin, pliable, and expendable muscle with a robust and consistent neurovascular pedicle. Technically, PQPRF harvest is straightforward, does not require specialized microsurgical technique, and does not require sacrifice of major neurovascular structures to the wrist or hand. A PQPRF facilitates consistent muscular soft tissue coverage for defects ranging from the proximal forearm to the volar wrist crease and provides reliable coverage of the dorsal extensor compartments, Lister’s tubercle, and radial styloid or ulnar styloid when transferred through an interosseous window.
Footnotes
Acknowledgements
The authors would like to recognize Todd Baldini for specimen storage and laboratory space for this study.
Ethical Considerations
This cadaveric study followed appropriate ethical and institutional guidelines.
Author Contributions
The authors certify that each author has participated in and has contributed sufficiently to the work to take public responsibility for the appropriateness of the experimental design and method, and the collection, analysis, and interpretation of the data and that this final version has been reviewed and approved for submission and/or publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
All institutional and national guidelines for the care and use of human cadaveric specimens were followed.
Statement of Informed Consent
This was not needed as this is a cadaveric study.
Disclosure of AI Use
AI was used to generate the arm images depicted in Figures 2 and ![]() . AI was not used for the creation of the heat map images as a whole. AI was not used in any capacity for the writing or editing of this manuscript or statistical analysis.
. AI was not used for the creation of the heat map images as a whole. AI was not used in any capacity for the writing or editing of this manuscript or statistical analysis.