
Abstract
Stress is ubiquitous in our modern society and contributes to many disease states. This narrative review describes the effect of stress/distress on cancer development and progression. Seminal randomized controlled trials, systematic reviews/meta-analyses, and distress management guidelines from the National Comprehensive Cancer Network (NCCN), the American Society of Clinical Oncology (ASCO), and the Society for Integrative LinearOncology (SIO) are highlighted. We describe the physiological effects of distress, distress assessment, and management. Psychological treatments are summarized. Evidence-based lifestyle modifications and integrative therapies are reviewed in detail, including mindfulness-based techniques, yoga, guided imagery, breathing techniques, hypnosis, exercise, music therapy, qigong/Tai Chi, eye movement desensitization and reprocessing, and improving sleep and heart rate variability. Recognition and treatment of distress can improve quality of life. More research is needed to determine the effects of managing distress on cancer outcomes, as well as the best type and duration of intervention, noting that the benefits of interventions may be specific for patients with different cancer types.
“Distress interventions have been shown to improve quality of life, physical symptoms, and cancer outcomes.”
Introduction
In 2024, over 2 million people will be diagnosed with cancer, and over 600 000 will die of cancer in the United States. 1 All patients with a cancer diagnosis, regardless of stage, are likely to experience stress or distress due to the nature of the diagnosis and the adverse effects of the disease and its treatment. Stress can be considered a normal reaction to life events, but when the stress is chronic, severe, or one cannot cope with these events, distress ensues. Distress can have adverse effects on quality of life and cancer outcomes. This narrative review describes the impact of distress on cancer development and outcomes and describes interventions designed to mitigate distress. National guidelines, systematic reviews/meta-analyses, and randomized controlled clinical trials (RCTs) are highlighted. Psychological interventions and lifestyle/integrative therapies are reviewed.
Definition of Stress/Distress
In the context of cancer, Antoni et al define stress as “a constellation of events that involves a stimulus (stressor), which precipitates a reaction in the brain (stress perception) and, in turn, activates physiologic fight-or-flight responses in the body (stress response).”
2
This understanding of stress is crucial in the context of cancer, as it helps us comprehend the distress experienced by cancer patients, which can range from mild (i.e., common feelings of vulnerability) to disabling.
3
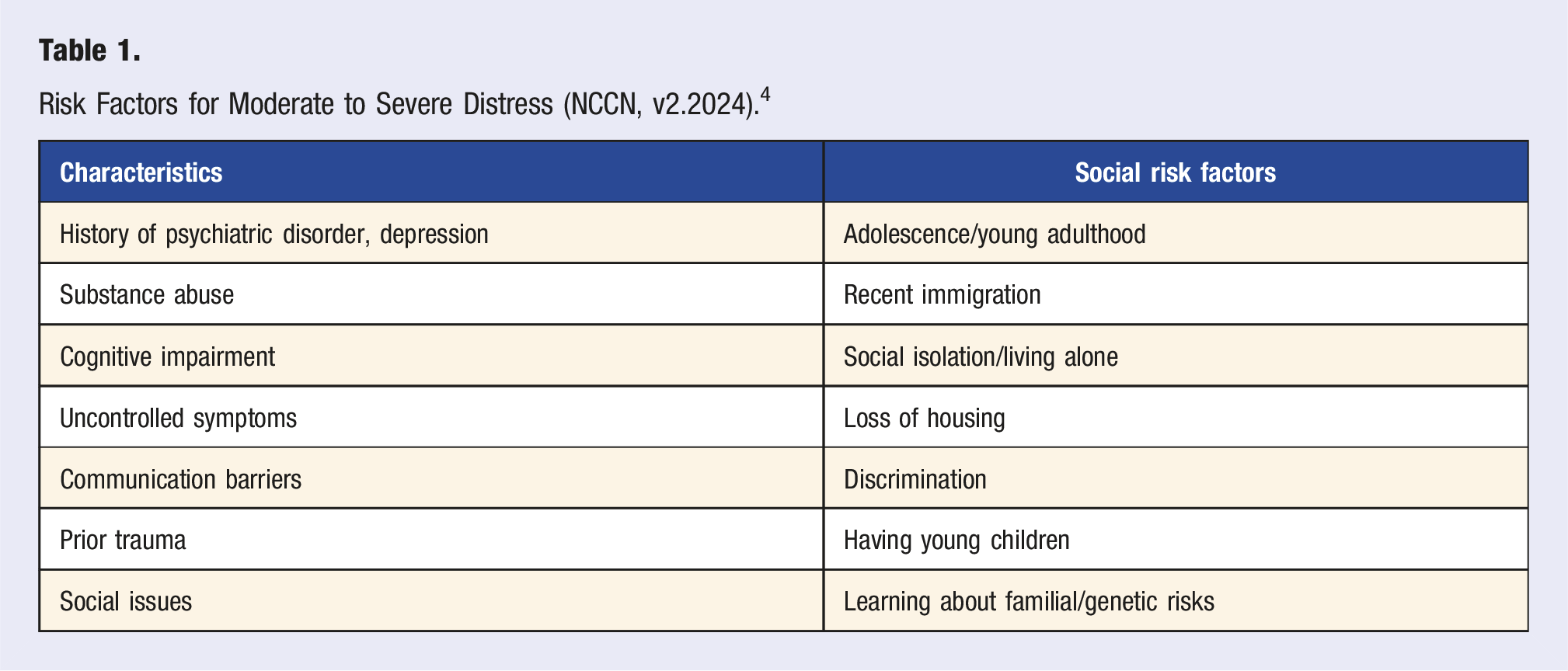
The assessment of distress will be covered below. The National Comprehensive Cancer Network (NCCN) defines distress as:
Risk Factors for Moderate to Severe Distress (NCCN, v2.2024). 4
Effects of Stress on the Body
The physiological components of the stress response, commonly termed “flight, fight, or freeze,” are predominant in two systems: a fast response mediated by the sympathetic-adrenal-medullary (SAM) axis and a slow response mediated by the hypothalamus-pituitary-adrenal (HPA) axis. 11 This response is a combination of physiological changes that helps an individual appropriately respond to a threat, ensuring survival. When the SAM axis is triggered, it increases secretion of the catecholamines epinephrine and norepinephrine. Circulating epinephrine and norepinephrine interact with α-adrenergic and β-adrenergic receptors, driving the flight or fight response. 11 The slow stress response, the HPA axis, is activated when the amygdala sends a distress signal to the hypothalamus, leading it to release corticotropin-releasing factor (CRF). CRF then triggers the anterior pituitary gland to release adrenocorticotropic hormone (ACTH). ACTH, in turn, stimulates the release of glucocorticoids, such as cortisol, from the adrenal glands. Cortisol is a steroid hormone that regulates behavioral, cardiovascular, and immune responses. 12 Activation of the SAM axis and the HPA axis affects all body organ systems, including the nervous system, the cardiovascular system, the endocrine system, the respiratory system, the gastrointestinal system, the musculoskeletal system, and the reproductive system. The physiological changes due to the impacts on these organ systems are as follows: increased heart rate and redirection of blood to large muscles, increased respiratory rate allowing for improved oxygenation of cells and reduction in carbon dioxide waste, increased production of stress hormones, glycogenolysis and gluconeogenesis allowing cells to receive adequate nutrition, increased muscle contraction and decreased sexual desire and function in the face of chronic stress. 11 While acute stress is essential to human survival, chronic stress (or distress) is associated with several chronic diseases, including cardiovascular disease, diabetes, gastrointestinal disease, and psychiatric diseases. Systemic low-grade chronic inflammation, measured by elevated plasma pro-inflammatory biomarkers such as interleukin 6 (IL-6), tumor necrosis factor-alpha (TNF-alpha), and C-reactive protein (CRP), have been hypothesized to be the mechanism of action driving these disease states. 13
How Do We Measure the Stress Response/Distress?
Patient Self-Report
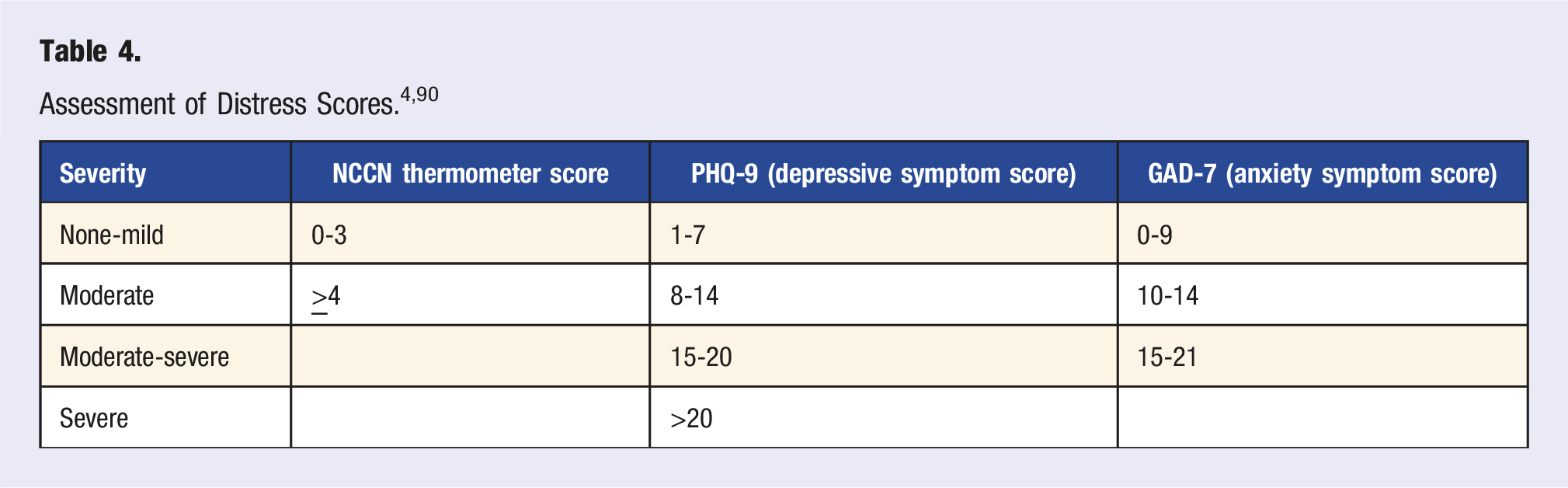
Patient self-report measures include ultrashort (e.g., NCCN Distress Thermometer, Patient Health Questionnaire 2), short (e.g., Generalized Anxiety Disorder 7 (GAD-7), Patient Health Questionnauire-9 (PHQ-9)), and long (e.g., Beck Depression Inventory-II, Profile of Mood State) questionnaires. Although many questionnaires that assess distress are psychometrically valid, sensitivity and specificity can vary widely by measure. Sensitivity, specificity, and content validity are higher in longer, psychometrically well-constructed questionnaires, 14 while brief questionnaires (1-4 questions) can be adequate for ruling out distress. 15 Therefore, it is important to consider the pros and cons of each questionnaire to optimize tool selection, including downstream burdens on patients and clinical systems (e.g., false negative screens send distressed patients through cancer treatment with untreated distress and its associated symptom burden). Furthermore, measures of distress extend beyond those commonly used in the clinical setting (e.g., measures of depression and anxiety) to include more basic, transdiagnostic, dimensional constructs within the National Institute of Mental Health Research Domain Criteria Framework (RDoC) that are intended to advance scientific understanding and theories of distress. 16
Biomarkers of Distress
Inflammatory biomarkers (e.g., pro-inflammatory cytokines and gene expression) are commonly linked to stressful life events such as cancer and associated measures of psychological response (i.e., distress). 2 Distress can trigger chronic inflammation (a shift from predominantly antiviral to pro-inflammatory immune orientation), moderated by psychological factors. 17 Animal models of chronic stress document activation of microglia, neuroinflammation, blood-brain barrier (BBB) permeability, allowing pro-inflammatory cytokines into the CNS (mediating depression), transport of peripheral monocytes to stress-sensitive neural regions, and increased metastasis associated with distress. 18 Meta-analyses of patients with post-traumatic stress disorder (PTSD) or depression have examined over 20 soluble/peripheral blood-derived inflammatory mediators, documenting elevations in serum levels of IL-6, TNFa, CRP, IL-3, IL-12, IL-18, sIL-2R (possibly IL-1B) and reduced IL-4 when compared to control groups.19,20
Salivary cortisol has been used to detect abnormal HPA axis signaling. Cortisol has a diurnal pattern, with the highest level occurring about 30 min after awakening and declining throughout the day. Various abnormalities include a flattened slope (low awakening spike), abnormal cortisol awakening response (CAR), abnormal total cortisol (AUC), and high evening cortisol levels.21-25 Salivary cortisol testing has mainly been used as a research tool.
Heart rate variability (HRV) is a valuable surrogate for distress/autonomic dysfunction in the research setting. 26 It predicts morbidity and mortality for various health conditions, including cardiovascular disease27-29 and cancer30-32 in many but not all studies. 33 HRV is defined as the fluctuation in the interval between heartbeats 34 and is a non-invasive method to determine sympathetic/parasympathetic tone as a biomarker for well-being, resiliency, and adaptability.35-37 The beat-to-beat variability is calculated, with higher HRV corresponding to more “coherence” or an optimal balance between parasympathetic/sympathetic tone or more resiliency. Many complex metrics are used to measure HRV, which are time-dependent and provide different information. ECG is the gold-standard measurement of HRV, but various monitors (i.e., watches, chest bands, rings, heart math) are also available for consumers and research.38,39 HRV can be affected by heart rate, medications, physical activity, breathing, age, sex, overall health, and emotions, thus making interpretation of many widely available/over-the-counter devices difficult.39,40
Does Distress Cause or Contribute to the Development of Cancer?
Though it is challenging to study the impact of distress on cancer development or incidence,41–45 seminal and analytic studies largely conclude that while distress does not cause cancer, it does contribute to cancer progression.2,46,47 Existing studies have been marked by methodologic limitations, including difficulty in controlling for confounders, non-prospective designs, and heterogeneity in measuring anxiety/depression. An older meta-analysis did show that depression was associated with a small increased risk of developing cancer (RR 1.15). However, the studies were extremely heterogeneous, as well as variable in controlling for confounders (such as smoking and alcohol use). 48 Another large meta-analysis of 51 cohort studies also showed that depression and anxiety were associated with a small increased risk of cancer incidence (RR 1.13); the authors state that results should be interpreted with caution due to significant heterogeneity in the included studies. 47 A recent meta-analysis from the Netherlands using individual patient data and validated measures for anxiety and depression did not find any evidence that baseline anxiety or depression was associated with cancer incidence. 49 The study controlled for age, sex, smoking history, alcohol use, exercise frequency, and cancer-specific risk factors. When looking at specific cancer types, depression and anxiety were associated with an increased risk of lung cancer in the minimally adjusted models (Hazard ratios (HR) 1.12-1.60). However, this is likely due to increased smoking in patients with depression. This study did not include patients with chronic anxiety or depression or a history of anxiety and depression; other studies have shown that chronic depression may be a risk factor for cancer development.50,51
Another recent meta-analysis of 22 cohorts and over 400 000 patients examined whether psychosocial factors (depression diagnosis, depression symptoms, anxiety diagnosis, anxiety symptoms, perceived social support, loss events, general distress, neuroticism, and relationship status) interacted with or modified the effects of health behaviors (smoking, alcohol use, physical activity, body mass index, sedentary behavior, sleep quality, sleep duration) that are known to affect cancer risk. They found that the “behavioral risk profile for cancer incidence was similar with and without psychosocial stress,” meaning that stress does not independently worsen the negative effects of unhealthy behaviors. This study, however, only looked at stress and behavioral factors at one point in time; further studies should examine longer-term stress and its relationship with behaviors and cancer risk. 52
Adverse childhood events (ACEs) such as neglect, physical or sexual abuse, household challenges, and other traumatic experiences have been associated with chronic health problems, including cancer, mental health issues, and behavioral risk factors (smoking, obesity, drug use).53-55 Patients exposed to more ACEs have more fatigue and experience greater mental health issues during cancer treatment. 56 A systematic review of 12 publications showed that higher ACE scores were significantly associated with the risk of any cancer development. 57 Notably, in this and similar studies, high ACE scores were also associated with adverse health behaviors (smoking, alcohol use, etc) that are known risk factors for cancer development, which are difficult to control in study design. 58 The mechanisms of how ACEs may contribute to cancer or other disease development may be related to these adverse health behaviors, as well as increased inflammation,59,60 shortened telomeres, 61 or altered/maladapted stress responses. 62 More research must be conducted to determine the mechanisms of such associations and if interventions can lead to prevention and/or improved outcomes.
Effects of Distress on Cancer Outcomes
Preclinical Models
Preclinical models have shown that stress can impact multiple pathways that can lead to cancer growth and metastasis. Distress can increase cortisol and norepinephrine, which may enhance tumor growth and metastasis, enhance angiogenesis, increase resistance to chemotherapy, and negatively affect the immune system.63,64 He et al 64 showed that chronic stress alters the tumor microenvironment in mice in several ways, including reduced T-cell infiltration, increased neutrophil infiltration, and fibronectin accumulation. They also found that glucocorticoid release with chronic stress causes increased neutrophil extracellular trap formation and promotes metastasis. Effects on natural killer cells (NKC) have also been demonstrated—in patients with breast cancer who had abnormal cortisol patterns, the number and activity of NKC decreased. 21
Effect of Stress on Cancer Recurrence and Mortality
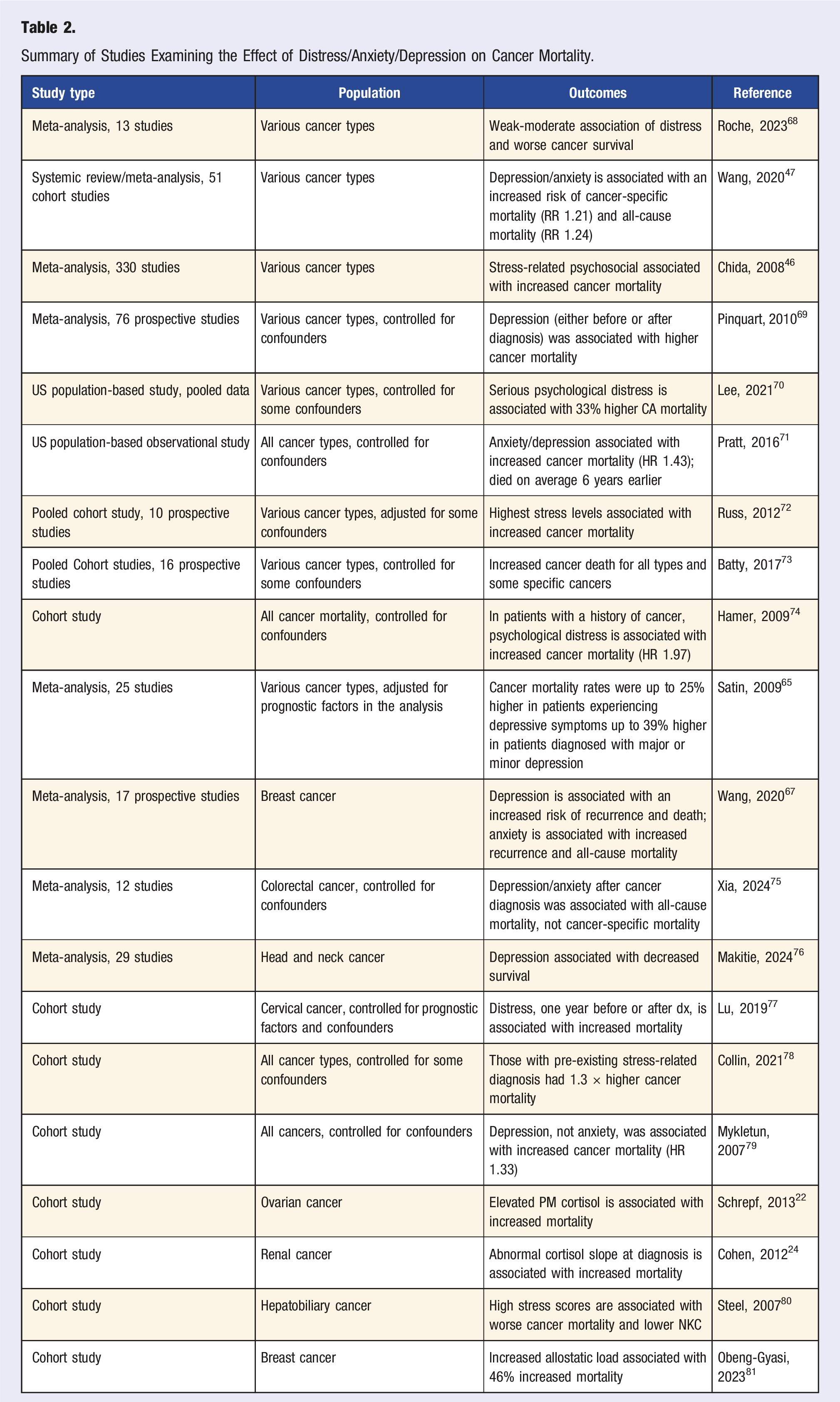
Evaluating the effect of distress on cancer outcomes is difficult. There are many different methods of assessing distress, as well as multiple diagnoses associated with distress, such as depression/anxiety/PTSD, that are used in many studies. Also, many risk factors need to be controlled, including cancer-specific prognostic features and behavioral and physiologic factors. Studies are subject to publication bias and are extremely heterogeneous, making interpretation of the literature difficult. There are limited studies examining the relationship between distress and cancer recurrence, and these show mixed findings. Older reviews/small meta-analyses65,66 showed no association between distress and cancer recurrence, but a newer meta-analysis of 17 studies involving patients with breast cancer did show that anxiety and depression were associated with increased cancer recurrence. 67
Summary of Studies Examining the Effect of Distress/Anxiety/Depression on Cancer Mortality.
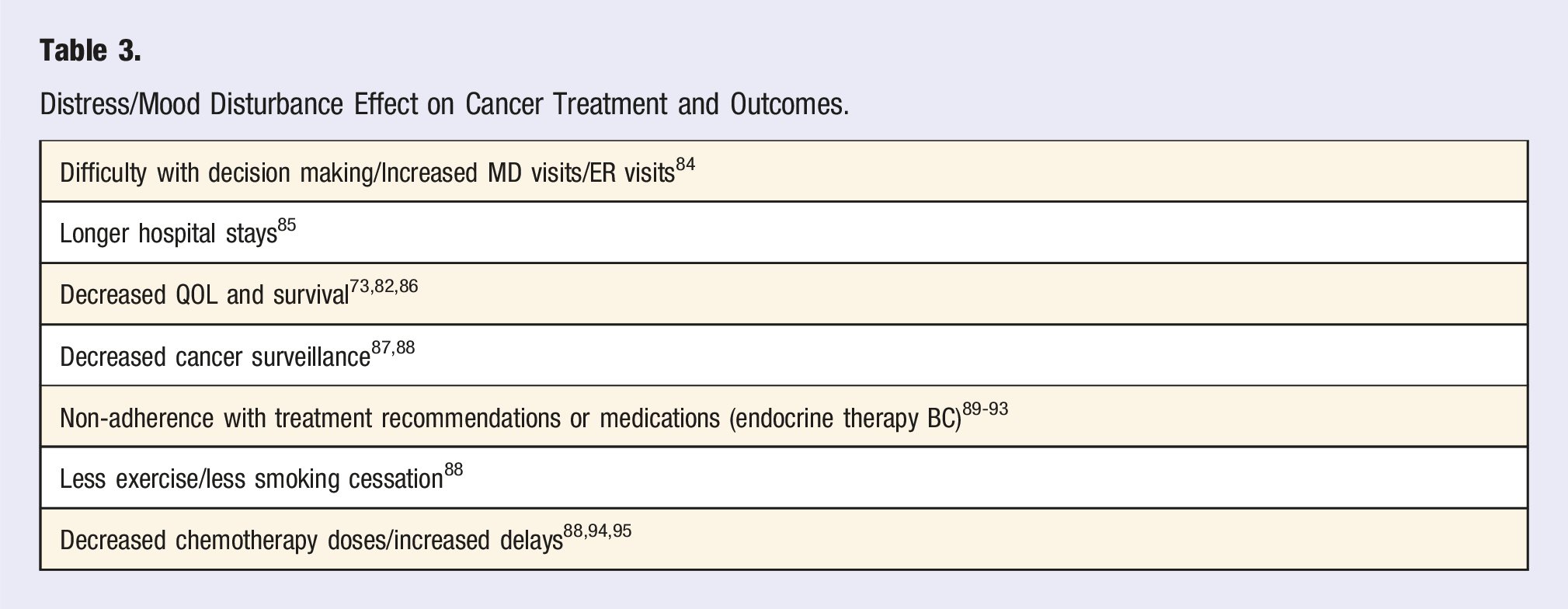
Effects of Stress on Treatment Adherence
Distress/Mood Disturbance Effect on Cancer Treatment and Outcomes.
Effects of Stress on QOL/Symptoms
Stress or distress also affects how patients experience cancer treatment. According to NCI PDQ, “For patients undergoing cancer treatment, anxiety can also heighten the expectancy of pain, other symptoms of distress, and sleep disturbances, and it can be a major factor in anticipatory nausea and vomiting. Regardless of its severity, anxiety can substantially interfere with the quality of life of cancer patients and their families and should be evaluated and treated.” 96 Fortin and colleagues 3 also found that patients with severe anxiety experienced more physical symptoms, such as nausea and vomiting, which can compound cancer-related somatic symptoms. In a secondary analysis of data from an RCT evaluating guided imagery and progressive muscle relaxation (PMR) on pain, fatigue, anxiety, and depression, Charalambous et al showed evidence of co-occurrence and inter-relation between pain, anxiety, depression, and fatigue in 208 patients with breast and prostate cancer. The analysis concluded that targeting fatigue, anxiety, and depression may positively affect pain and health-related QOL in this population. 97 Another RCT showed that in a cohort of 169 patients with BC, self-reported depression burden significantly influenced the severity of side effects, number of side effects, and the burdens of fatigue, difficulty concentrating, and anxiety. 98
Interventions
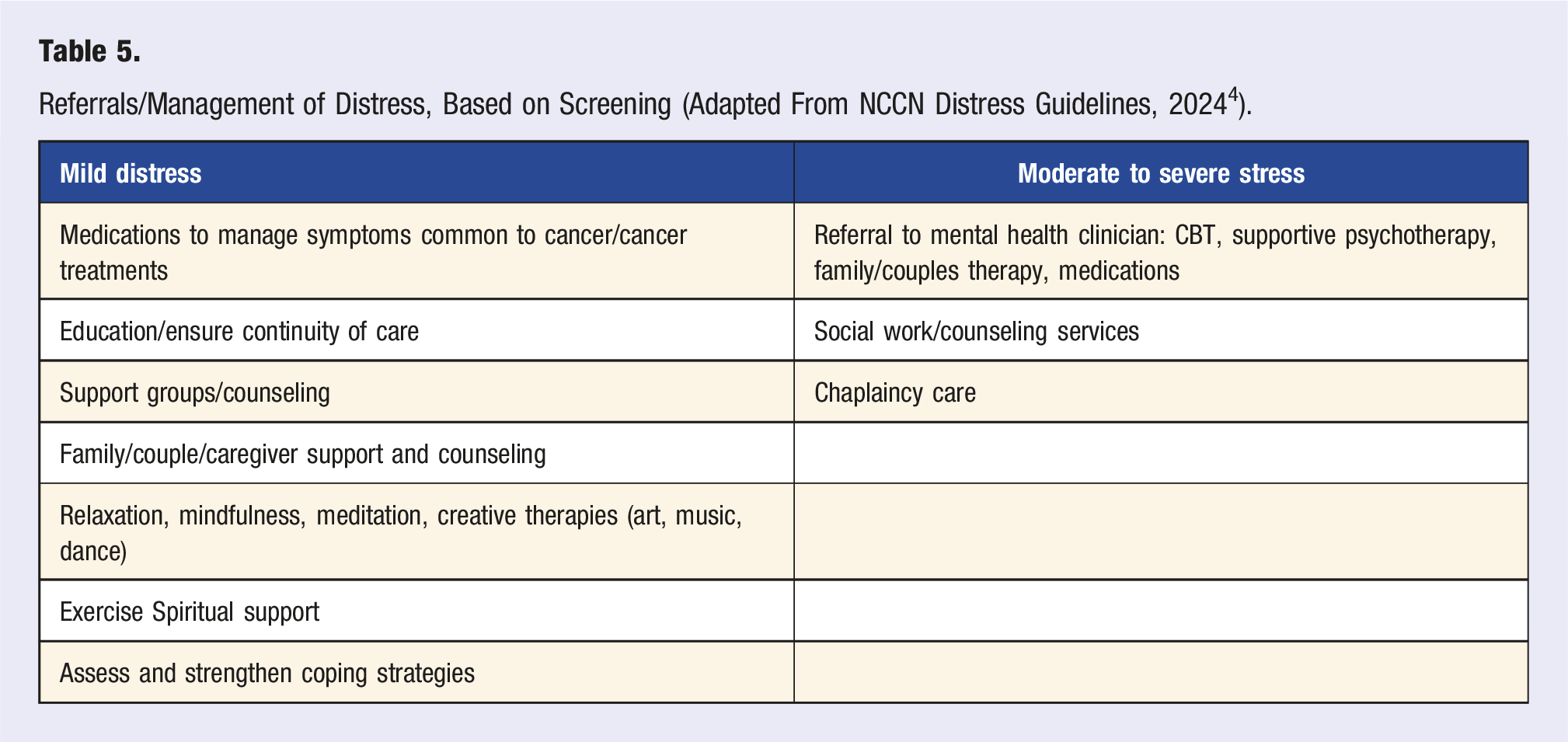
NCCN/ASCO Guidelines for Distress Management
Referrals/Management of Distress, Based on Screening (Adapted From NCCN Distress Guidelines, 2024 4 ).
ASCO Distress Guidelines (Adapted From Andersen, B et al, 2023). 90
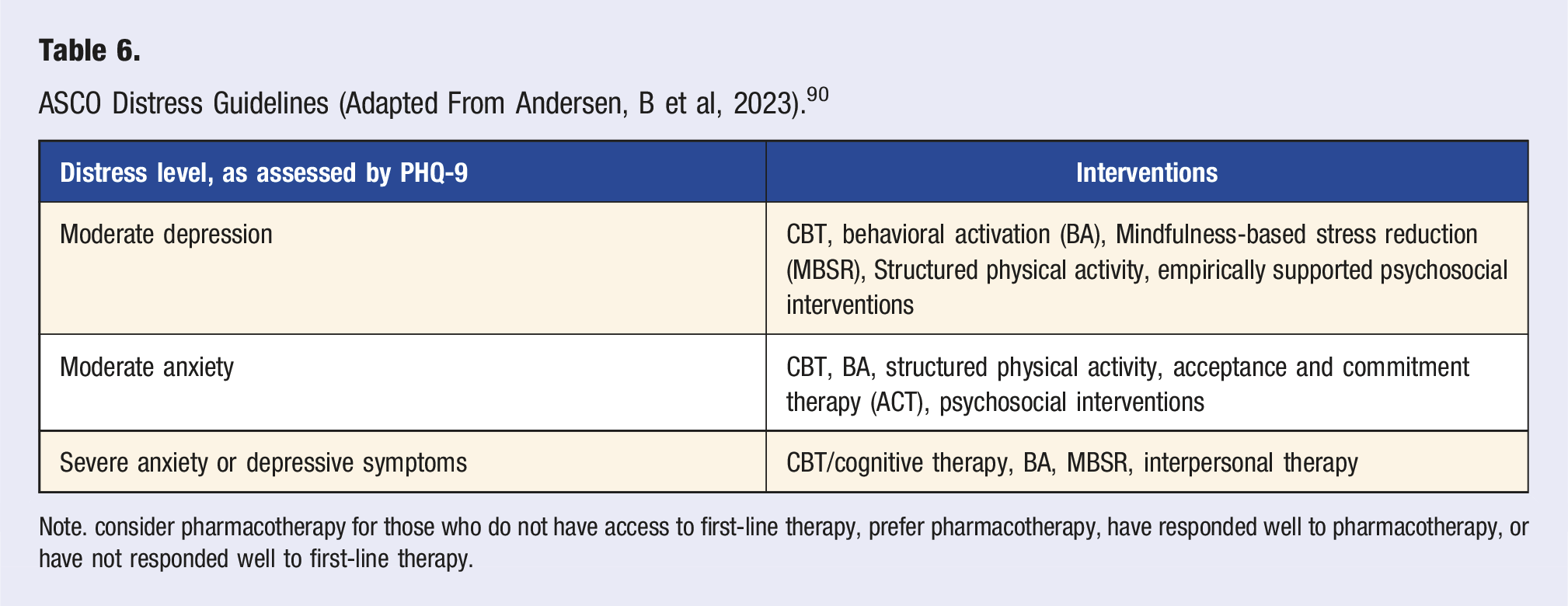
Note. consider pharmacotherapy for those who do not have access to first-line therapy, prefer pharmacotherapy, have responded well to pharmacotherapy, or have not responded well to first-line therapy.
It should be noted that while distress screening is recommended, there is some evidence that this practice does not improve outcomes.100,101 A recent Cochrane review did not support the effectiveness of routine screening, highlighting the heterogeneity and methodological issues with the studies. 102 Many patients who screen positive for distress do not utilize available resources. 103 Cancer distress guidelines define distress as a complex, multi-component construct best treated by teams that include multiple specialists with expertise in each component of distress (e.g., depression, pain, spiritual concerns). Unfortunately, the scientific literature on distress screening trials tends to focus on brief distress screening measures that do not adequately capture the complexity of distress and thus do not adequately test distress screening as recommended within current guidelines. Distress treatment within the scientific literature also tends to be less specialized than recommended within guidelines and thus inadequately tested. Furthermore, there is a lack of investigation between distress screening measure selection, construct validity, and downstream impacts such as burdens on patients and staff. In sum, guideline congruent care is not well tested. There is a significant need to test comprehensive care models that align with guidelines. 104
Psychological Therapies and Cancer Outcomes
Psychological therapies, such as CBT, Acceptance and Commitment Therapy (ACT), and supportive psychotherapy, can be beneficial for patients with distress. These psychosocial interventions may also have a small to moderate effect on survival. 105 CBT interventions are the most studied psychological intervention for cancer distress and are considered the gold-standard psychological intervention. CBT is an evidence-based psychological intervention that challenges maladaptive thought patterns to improve psychological, emotional, and behavioral responses to stress. As a skills-based intervention, individuals learn various coping skills through practice with a mental health provider and integrate skills into their home lives. Numerous studies have used CBT to improve psychological and physical outcomes for patients with cancer in survivorship and with advanced disease.106-110 ACT, a promising intervention for cancer distress, is considered a third-wave behavioral intervention stemming from the CBT tradition. ACT aims to promote psychological flexibility by fostering awareness of and willingness to experience distressing internal experiences while encouraging engagement in value-driven behaviors. 111 Unlike CBT, ACT focuses on changing the relationship to thoughts instead of altering the content of thoughts. ACT consists of six core processes (i.e., mindfulness, acceptance, self-as-context, cognitive defusion, values, and committed action) which promote psychological flexibility. 112 A recent meta-analysis of 110 articles examining the association between ACT processes and cancer-related distress indicated that higher self-reported scores related to psychological flexibility (present-moment awareness and acceptance) were associated with lower levels of cancer distress. 113 ACT has been shown in a systemic review of 8 studies of advanced cancer patients to improve anxiety, depression, psychological distress, and fatigue, but not pain or psychological flexibility. 114 Similarly, in cancer survivors, ACT reduced anxiety, depression, and fear of recurrence, as well as improved QOL and psychological flexibility. 115
Physiologic Basis of Psychological Therapies
Though there is a paucity of rigorous psychological intervention trials for cancer distress that include the measurement of inflammatory biomarkers, psychological treatment is associated with improvements in both distress constructs and associated inflammatory markers. 116 In more controllable animal models, protocols have demonstrated similar effects and reversibility of these effects via blocking the psychoneuroimmunological cascade of stress.117-119 Meta-analysis of 56 human psychological treatment RCTs also revealed reversibility of chronic inflammation (e.g., pro-inflammatory cytokine levels, immune cell counts, NKC activity, in vitro T-cell mitogen-driven blastogenesis, infection). 120 CBT, mindfulness, and meaning-based therapies share common mechanisms and thus are commonly grouped as “psychological treatments.” 121 Shields et al 120 documented effects for both CBT and combined psychological interventions within cancer and other defined populations (HIV, autoimmune, insomnia), with durability of at least six months. CBT was associated with a 33% decrease in parameters of chronic inflammation, while psychological treatments, in general, were associated with an 18% decrease.`123 Beyond pro-inflammatory cytokines and immune cell counts, CBT was also associated with improved NKC activity, in vitro T-cell mitogen-driven blastogenesis, and decreased incidence of postoperative infections. Interestingly, age and sex did not moderate effects.
Across RCTs of psychological treatment in cancer populations, psychological therapies are associated with reduced peripheral blood mediators of chronic inflammation and improved parameters of normal/healthy immune homeostasis (see Figure 1). The effect of CBT on inflammation in cancer patients has been studied to a greater extent than other psychological interventions. In a study of CBT for cancer interventions compared to controls, individuals randomized to CBT had lower levels of inflammation (e.g., s100A8/A9),
121
lower serum cortisol,
122
and greater NKC cytotoxicity, T-cell blastogenesis, and proliferation.105,123 Notably, the relationship between CBT and inflammation is important for short-term improvements in the tumor macroenvironment and long-term impacts. Andersen and colleagues
123
randomized newly diagnosed BC patients into a CBT intervention or control arm. Following the completion of the intervention, participants were asked to complete follow-up assessments at regular intervals. Participants who experienced a recurrence (median = 11 years after initial diagnosis) and received the CBT intervention had significantly higher NKC in the 12 months following recurrence diagnosis than those in the control group. Although these studies suggest that non-pharmacological interventions can decrease psychological distress and lower inflammation and stress response, it is important to note that measurements of immune function vary greatly. Given the improved understanding of the role of immunity in cancer and the use of immunotherapy to treat cancer, there is a pressing need for more sophisticated measures. Psychological therapies and immune markers.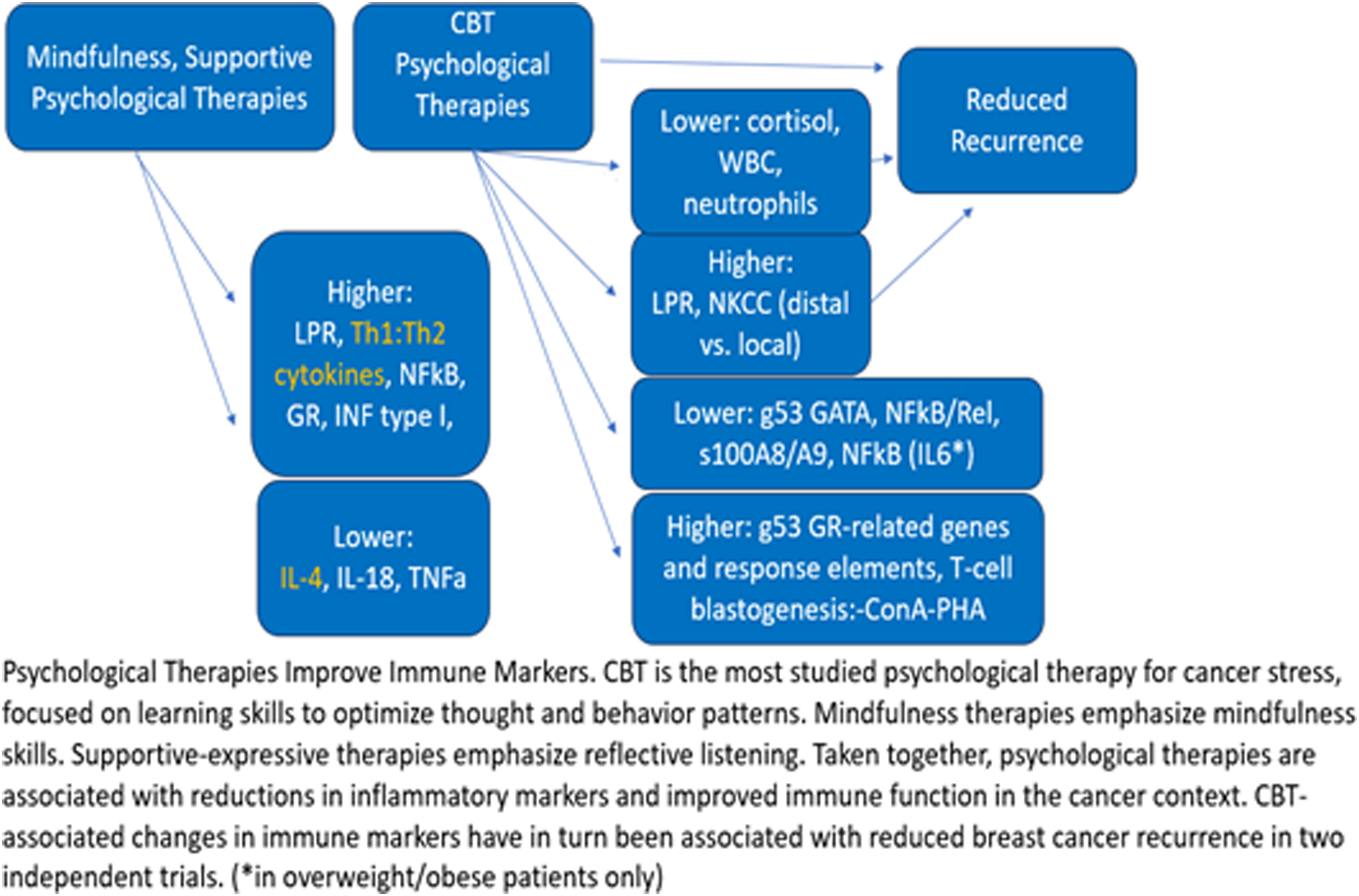
Trauma Therapy: Eye Movement Desensitization and Reprocessing (EDMR)
Oncology patients can experience cancer-related PTSD symptoms as a result of their treatment, and more traumatic stress symptoms may occur for patients with a recurrent cancer diagnosis. 124 These patients should be referred to a mental health professional for evaluation and treatment. EDMR is an adjunctive therapy that involves focusing patients’ attention on their trauma memory while also incorporating eye movements, tones, or tapping to decrease the intensity and emotion surrounding the memory (APA). 125 EMDR may be recommended as an intervention for post-traumatic stress disorder (PTSD) and is performed by a trained therapist. EDMR is an emerging therapy for additional emotional health support and enhancement of QOL in the oncology patient population.124,126,127
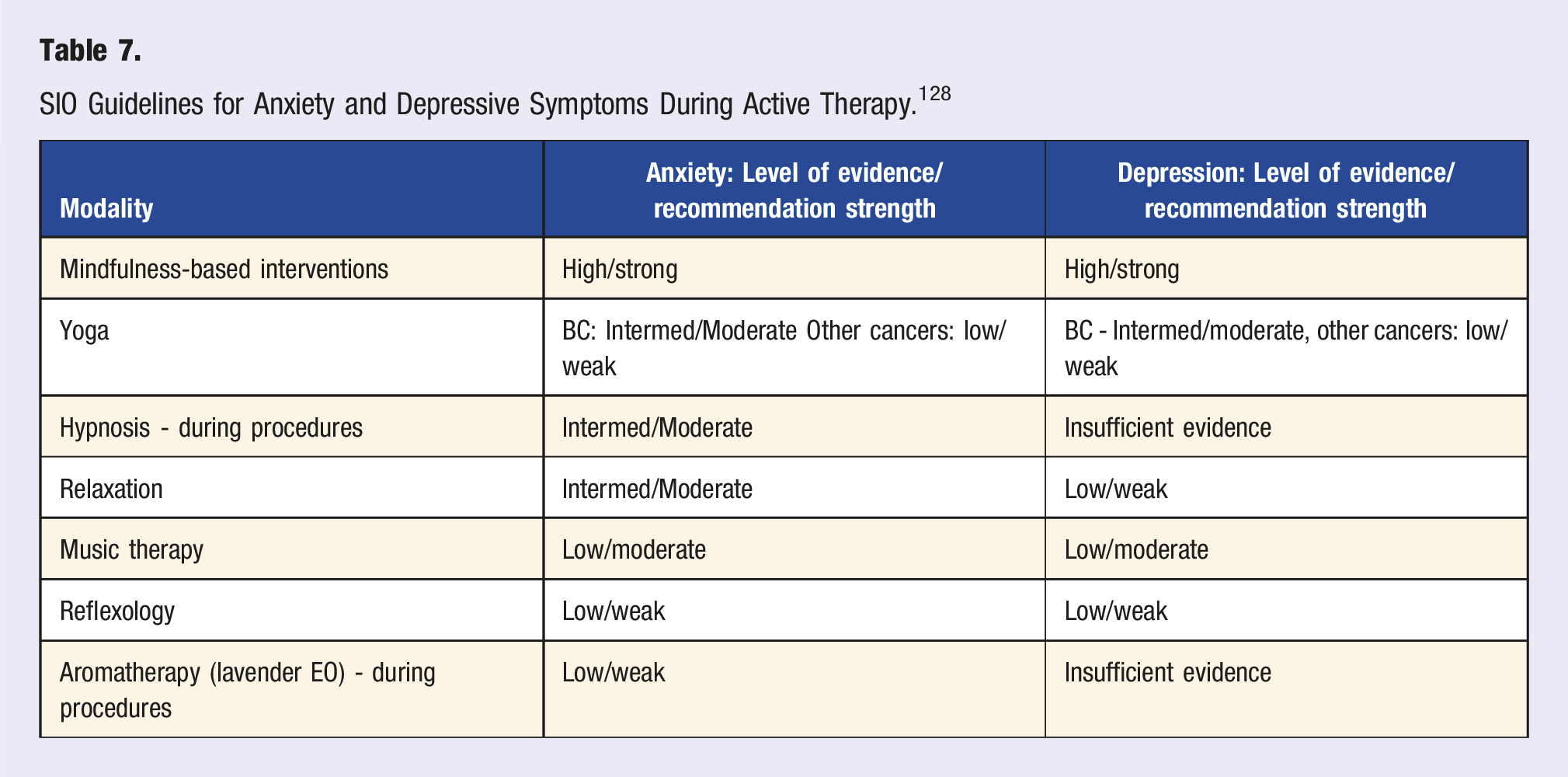
Integrative Therapies for Distress
SIO Guidelines for Anxiety and Depressive Symptoms During Active Therapy. 128
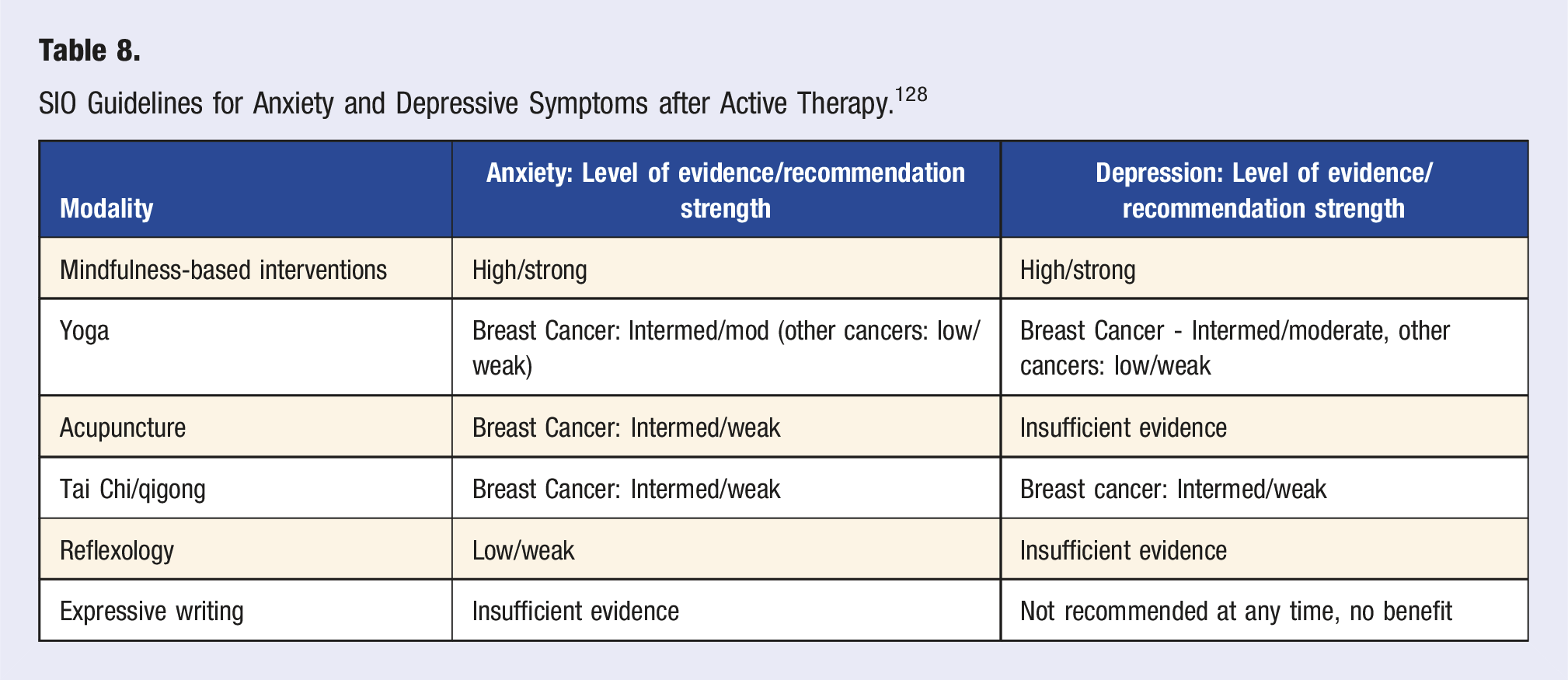
SIO Guidelines for Anxiety and Depressive Symptoms after Active Therapy. 128
Mindfulness-Based Interventions (MBI)
Mindfulness-based interventions teach patients to be aware of the present moment and nonjudgmentally address thoughts, feelings, and sensations. Patients may practice mindfulness in different ways, including meditation, yoga, Tai Chi, breathing techniques, guided imagery, and body scans. 129 Guided imagery (GI) can help individuals visualize images, objects, sounds, and smells that may assist with relaxation and support healing. 130 Performing a body scan is a technique in which the patient focuses attention on different body parts, noting temperature, muscle tightness, and other sensations, intending to reconnect patients to their bodies. 131
One common MBI is an intervention called Mindfulness-Based Stress Reduction (MBSR). In this group-based intervention, participants learn about mindfulness-based practices such as meditation, body scans, and yoga under the guidance of trained instructors for two to two and a half hours weekly over eight weeks. This includes one full-day retreat and approximately 45 minutes/day of home practice between weekly sessions. 132 The benefits of MBI have been shown in multiple meta-analyses, confirming improvement in anxiety and depressive symptoms and improvements in QOL.133-135 It is possible that longer-term benefits may require repeating the course or that follow-up sessions may be needed, but more studies are needed.136,137 MBI may also be effective when done virtually, which improves access for those who cannot travel or attend in-person sessions. Compen et al 138 showed that an internet-based mindfulness program decreased distress, reduced fear of recurrence, and improved overall mental health compared to usual care (and equivalent to in-person). Another mindfulness intervention called Mindfulness-Based Cancer Recovery (MBCR) has been developed at the University of Calgary and is more specific for patients with cancer. 139 MBCR programs consist of body awareness, exercises/gentle yoga, meditation, inquiry, and daily home practices. The in-person class is nine weeks, with one week being an in-person retreat. MBCR has been shown in clinical trials to improve psychological and sleep outcomes in patients with cancer.139-141 MBIs are strongly recommended by the SIO for the treatment of anxiety and depression during and after therapy (Tables 7 and 8). 128
Yoga
Yoga, an ancient practice rooted in Indian philosophy, combines breathing techniques (pranayama), physical postures (asanas), and meditation (dyana) to promote relaxation through reduced activity in the sympathetic nervous system. As with psychological therapies, yoga also decreases inflammatory cytokines and oxidative stress in patients with breast cancer. 142 Much like MBSR, many of the RCTs in this space have looked at the use of yoga amongst patients with BC.142,143 Given the limited evidence in malignancies outside of BC, a wide variety of forms and styles of yoga, and variable designs in yoga protocols amongst current studies, further research would prove beneficial. SIO recommends yoga for anxiety and depression in patients with BC, both during and after therapy (Tables 7 and 8). 128
Tai Chi/Qigong (TCQ)
Qigong and Tai chi originated thousands of years ago in China and involve slow-flowing movements, breathing techniques, and focused attention. Tai Chi is a form of Qigong, but these are considered equivalent practices for most purposes and will be referred to as TCQ. These forms of mindful movement have shown many health benefits. 144 These exercises can be practiced anywhere- at home or outside, without requiring special equipment. With practice, TCQ can influence stress centers (activating the parasympathetic nervous system) to reduce stress hormones and lower blood pressure and heart rate. 145 Multiple clinical trials have shown the benefits of TCQ. In patients with cancer, TCQ has been shown to improve quality of life, decrease fatigue, improve cognition, and improve immune functioning.146-151 SIO recommends TCQ to help treat anxiety/depressive symptoms for patients with BC after they have completed therapy (Table 8). 128
Hypnosis/Guided Imagery
Hypnosis is “a waking state of awareness, (or consciousness), in which a person’s attention is detached from his or her immediate environment and is absorbed by inner experiences such as feelings, cognition, and imagery.” 152 This can be therapeutic because suggestions alter perceptions, thoughts, emotions, and behaviors. This can be done in various formats, including in person, group, or self-directed. 153 Hypnosis does appear to improve mental health in patients with cancer; more studies are needed on the effects on cancer-specific outcomes.154-157 SIO recommends hypnosis for anxiety for patients with cancer undergoing diagnostic or treatment procedures (Table 7). 128 Guided imagery (GI) can help individuals visualize images, objects, sounds, and smells that may assist with relaxation and support healing. 130 Studies focusing on GI for individuals with cancer often combine this technique with other mind-body practices such as PMR, deep breathing, and music.
Music Therapy
A trained music therapist typically supports music therapy; patients generally listen to pre-recorded selections. These music selections are often culturally appropriate or tailored to patients’ preferences. Music therapy may help with mood disorders during active treatment and may be recommended. 128 In an updated Cochrane review, Brandt et al found that music therapy improved anxiety symptoms and, to a lesser extent, depressive symptoms; the evidence for this, however, was low. 158
Other Lifestyle Interventions for Distress
Exercise
Exercise has been shown to improve QOL, cognition, fatigue, and cancer-related outcomes and is recommended for patients in active treatment and survivorship.99,159-166 In general, 150-300 min of moderate aerobic activity per week and twice-weekly strength training sessions are recommended. 167 In large meta-analyses, exercise has also been shown to improve depressive symptoms in patients with various cancers, although the effect size may be smaller than for other outcomes.165,166,168-171 The effects of exercise on improving anxiety are mixed.166,172,173 A large meta-analysis showed benefits in QOL domains, including emotional well-being, sexuality, sleep disturbance, social functioning, anxiety, fatigue, and pain at varying follow-up periods. The authors called for more research to determine exercise prescriptions for different types of cancer and how to sustain effects for more extended periods. 171 For example, in patients with lung cancer, prostate cancer, and multiple myeloma, exercise has not been shown to improve mood symptoms.174-176 However, given the multitude of benefits of exercise, it is recommended for all patients during treatment (as tolerated) and survivorship.
Importance of Sleep
Sleep Hygiene Techniques.
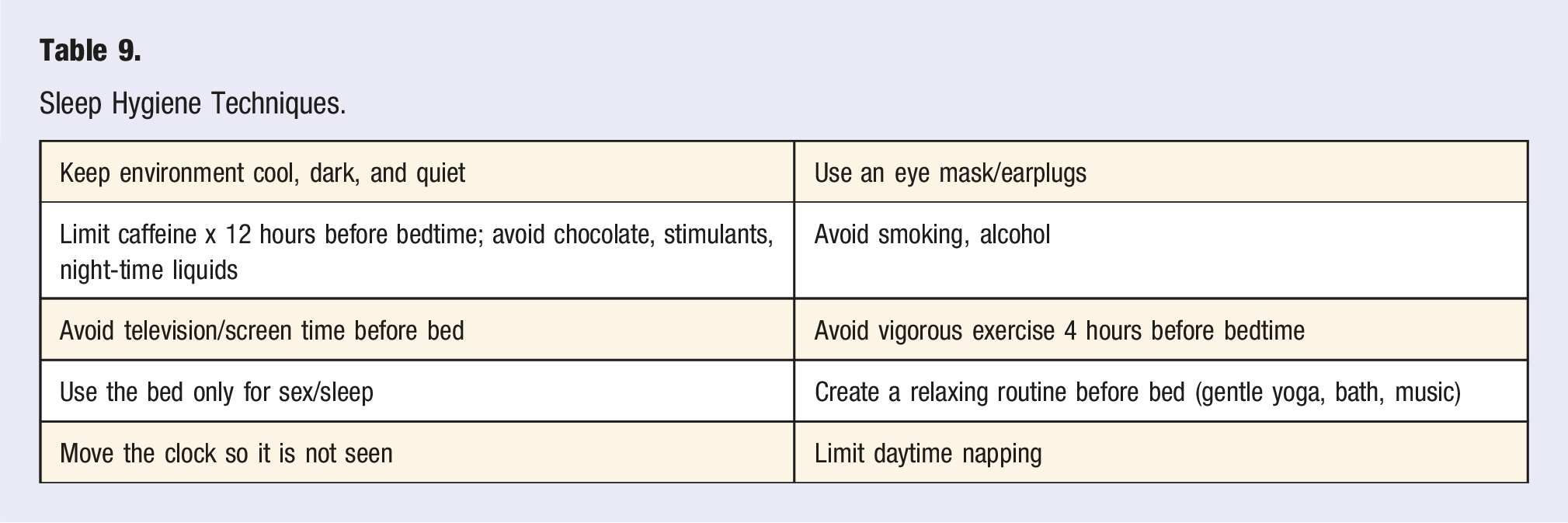
Stimulus control involves changing the relationship between the bed and other activities. After winding down, patients should only go to bed when feeling sleepy. If they are not asleep in 15-20 min, they are instructed to get up and go to another room. Engagement in mundane activities, such as reading, coloring, or listening to music, is acceptable, while avoidance of stimulating activities or those with bright lights is discouraged. Patients are then instructed to go to bed again, but only when feeling sleepy; this process is repeated until sleep initiation is obtained. Stimulus control thus associates sleep with the bed/bedroom environment. Sleep restriction involves setting consistent sleep and wake times based on sleep diary data to set an optimal sleep window, creating a sleep deficit and promoting healthy sleep patterns. Relaxation and worry management are also taught to help reshape negative thoughts about insomnia. Many of the techniques described above, including mindfulness-based interventions, breathing exercises, PMR, and Qigong or gentle yoga, may be helpful for relaxation and quieting the mind. Patients with seizures or bipolar disorders should only attempt CBT-I with the guidance of trained professionals.185-187
Lifestyle/Integrative Approaches to Improve Heart Rate Variability (HRV)
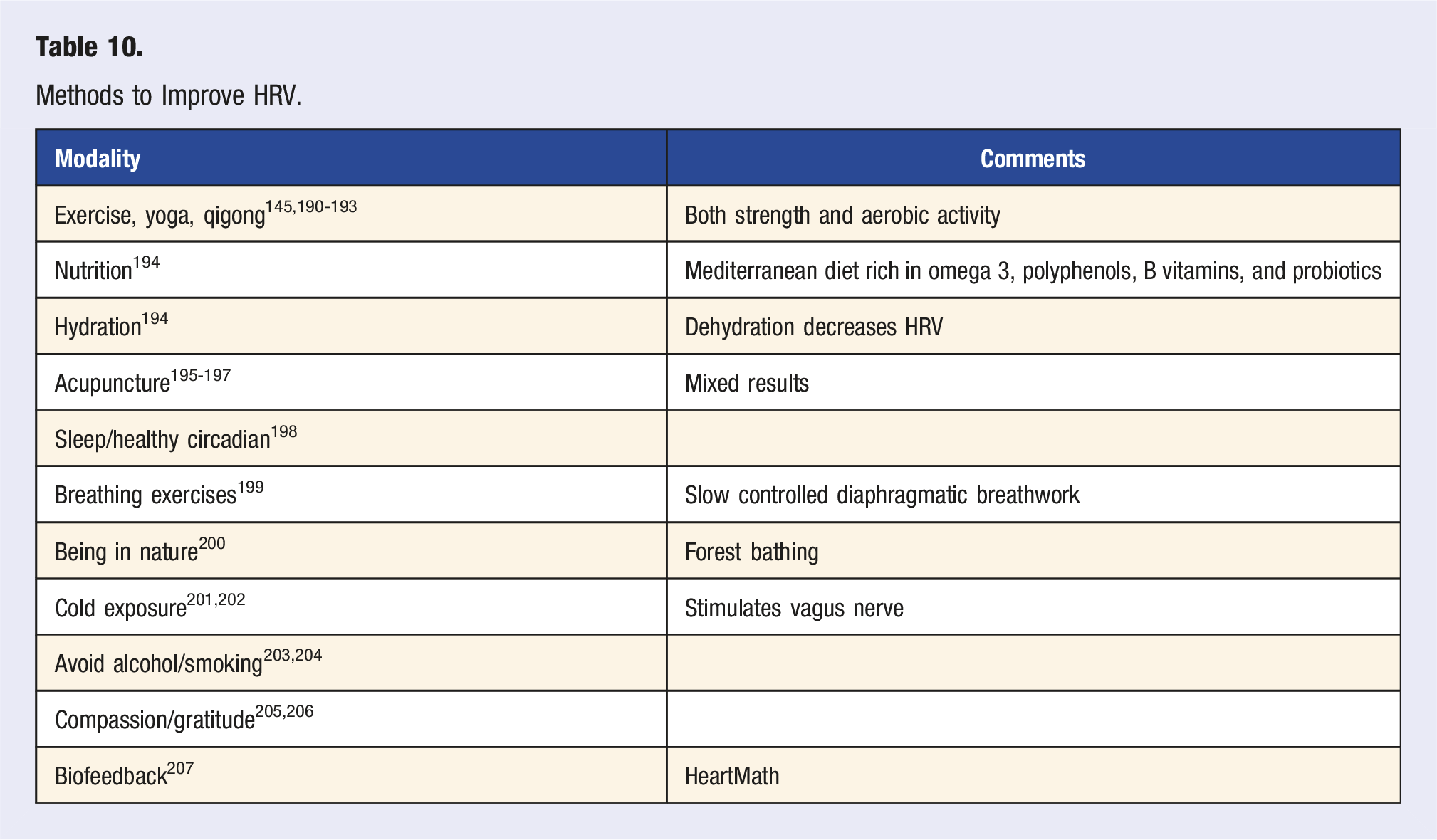
Methods to Improve HRV.
Importance of Social Support
NCI defines social support for patients with cancer as “a network of family, friends, neighbors, and community members that is available in times of need to give psychological, physical, and financial help.” 208 Higher levels of social support have been shown to positively impact QOL, increase resilience and coping, improve emotional health, and increase survival.209-214 Social constraint (refraining from or modifying patients’ disclosure of stress- and trauma-related thoughts, feelings, or concerns) may also impact patients’ well-being. 214 Patients with higher levels of social support also have lower inflammatory markers such as CRP, IL-6 and TNF-a. 215 It is important to refer patients who lack social support to resources through social workers or cancer resource/education centers. 216
Summary
Stress/distress are ubiquitous in society and play a significant role in human disease. The literature does not support stress as a factor in the development of cancer, but it may lead to behaviors that increase cancer risk. Conversely, more robust data shows that distress in patients with a cancer diagnosis can contribute to cancer progression and lead to worse outcomes. Distress interventions have been shown to improve quality of life, physical symptoms, and cancer outcomes. NCCN/ASCO guidelines are available to help clinicians assess and refer patients. Many integrative and lifestyle interventions are available for patients, including mindfulness interventions, meditative movements, exercise/yoga, music therapy, breathing exercises, guided relaxation, and activities that improve sleep and HRV. Lifestyle/integrative clinicians can play a much-needed role in many of these interventions.
Recommendations and Important Points for Practice
1. Recognize that distress is common among patients with cancer 2. Reassure patients that stress itself did not cause their cancer 3. Screen per institutional guidelines for distress at multiple time points and ensure that patients have access to support 4. Recognize that treating distress likely improves QOL and cancer outcomes 5. Utilize NCCN/ASCO guidelines as needed to guide referrals 6. SIO guidelines are available to guide referrals for integrative practices, with mindfulness-based interventions having the strongest recommendations for depressive/anxiety symptoms 7. Optimize lifestyle factors, such as exercise, sleep, and social support, which play an important role in mitigating distress
Footnotes
Acknowledgments
The authors want to acknowledge Dawn M. Mussallem, DO, for reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Markovic has research support from Bristol-Myers Squibb.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.