
Abstract
Lifestyle medicine interventions are well established for the prevention and treatment of cardiovascular disease (CVD) and are increasingly applied to people with cancer, who face elevated cardiovascular risk from both the disease and its treatments. Cardio-oncology, an emerging subspecialty, focuses on prevention, management, and treatment of CVD in patients with cancer and survivors. Incorporating lifestyle medicine principles—such as physical activity, healthy diet, stress management, and social connections—can help mitigate CVD risk in this population. This article reviews the impact of cancer and its therapies on cardiovascular health, current guideline recommendations, and the importance of an interprofessional, holistic approach to individualized care.
“Exercise has an anti-inflammatory and anabolic effect on the body, which can counteract the catabolic and systemic inflammation caused by cancer.”
Introduction
Lifestyle medicine interventions have been well characterized for the prevention and treatment of cardiovascular disease (CVD). 1 These interventions are being used to inform how we manage CVD risk in people with co-morbidities such as cancer. An emerging subspecialty in cardiology, aptly named cardio-oncology, is centered on the prevention, management and treatment of CVD in people with cancer and survivors. 2 People with cancer are at an elevated risk of developing CVD due the effects the cancer itself can have on the heart in addition to the effects of cancer treatment on the heart. 3 Lifestyle medicine principles, such as physical activity, healthy diet, and avoidance of risky substances, are important for clinicians to incorporate to mitigate the risk of developing CVD. 4 The other pillars such as social connections and stress management also play a vital role. In this article, we discuss how cancer itself, cancer treatments, and other lifestyle factors impact cardiovascular risk and disease. Additionally, the current guidelines for managing heart health and practical ways clinicians can address cardiovascular health with lifestyle medicine in people with cancer and history of cancer will be discussed.
Potential Pathophysiological Explanations for CVD in People with Cancer
Cancer itself can contribute to deterioration in CV function. 3 Several mechanisms for this have been proposed including systemic inflammation in response to the tumor and inflammatory factors secreted by the tumor contributing to catabolic breakdown of tissues including cardiac tissue. 3 Second, cancer influences increased sympathetic nervous system and renin-angiotensin-aldosterone-system activity leading to cardiac damage. 3 Third, in advanced cancers, weight loss and physical inactivity are associated with cardiac atrophy due to wasting and disuse. 3 There are several other proposed pathways in which cancer contributes to the deterioration of cardiac function including alterations in cardiac gene expression to a phenotype more similar to heart failure and mitochondrial dysfunction causing alterations in substrate metabolism and subsequently impairing cardiac myocyte contractility. 3
Cancer and CVD Risk
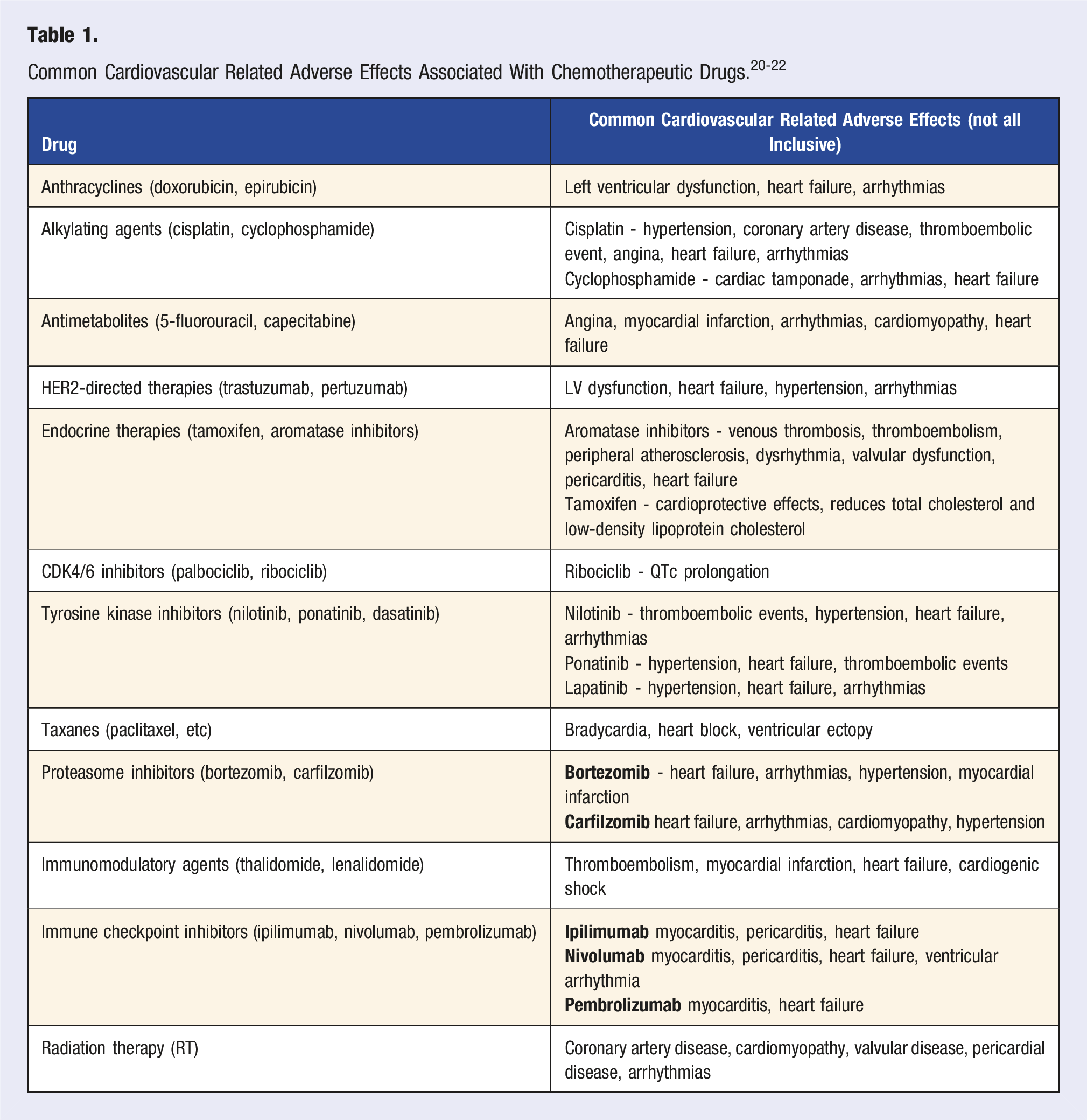
Certain types of cancer are more strongly associated with CVD risk, including breast, lung, colorectal, hematologic, kidney, ovarian, pancreatic, prostate, bladder, endometrial and melanoma. 5 This association is believed to arise to 3 main factors—shared risk factors of CVD and cancer, such as smoking, which increases risk for lung cancer and CVD, disease specific mechanisms including systemic inflammation, paraneoplastic syndromes and hypercoagulability which promote thrombotic states and vascular injury seen in hematologic cancers and liver cancer and the cardiotoxic effects of some cancer treatment regimens such as anthracyclines used in breast cancer treatment. 6
Chemotherapy and CVD Risk
Cancer and CVD: Shared Risk Factors
Cancer and CVD share many of the same risk factors including hypertension, hyperlipidemia, diabetes mellitus, obesity, smoking, diet, physical activity and the social determinants of health. 7 Understanding the overlap is essential to prevention and management of people with cancer or CVD disease. Additionally, by implementing lifestyle medicine interventions such as smoking cessation, we are able to have a greater impact on the health of our people.
General Approach to Cardio-Oncology Management
The current approach to cardio-oncology management involves screening cardiovascular function prior to initiating cancer treatment and monitoring cardiac function throughout the course of their treatment. 8 The American Heart Association (AHA) and American Cancer Society (ACS) recommend baseliness assessment of heart function through transthoracic echocardiogram (TTE) to all people who are starting potentially cardiotoxic chemotherapies. 8 Additionally, monitoring cardiac biomarkers such as cardiac troponin, atrial natriuretic peptide (ANP), and brain natriuretic peptide (BNP) may be recommended, depending on the person’s risk factors and treatment regimen. 8
Lifestyle Medicine Interventions in Cardio-Oncology
Beyond addressing shared risk factors, the pillars of lifestyle medicine impact heart health and overall wellbeing in people with cancer. Interventions addressing nutrition, physical activity, substance use, sleep, stress, and social connection can help reduce treatment-related complications, improve quality of life, and promote long-term survivorship. The following sections highlight how each of these pillars can be adapted to meet the unique needs of people with cancer.
Nutrition Counseling
Adverse effects of cancer treatment, such as nausea, loss of appetite, mouth sores, dry mouth, and changes to bowel movements may impact people’s eating patterns. 9 While eating a heart healthy diet remains to be important, it may be challenging for people who are experiencing these adverse effects. Recognizing the impact this may have on a person’s nutrition is especially important to provide individualized nutrition counseling. By providing specific nutritional guidance as well as referring people to dietitians for more personalized interventions is essential to maintaining general health and heart health throughout cancer treatment. 9 In general, emphasis on high protein, nutrient dense foods to avoid cachexia and cardiac atrophy caused by muscle wasting is part of the plan. 9
Physical Activity
Exercise has an anti-inflammatory and anabolic effect on the body, which can counteract the catabolic and systemic inflammation caused by cancer. 10 While it is important to consider the level of fatigue, age and mobility constraints of people with cancer, exercise is a safe and effective way to maintain heart health, improve quality of life, counteract fatigue, prevent muscle loss and preserve strength during cancer treatment. 10 The current ACS recommendation for exercise during cancer treatment is working up to 150-300 minutes of moderate (or 75-150 minutes of vigorous intensity) aerobic exercise, at least 2 days of strength training, and 2 days of stretching. 11 While the recommendations provide appropriate guidance, it is important to recognize that cancer treatments may affect a person’s ability or motivation to engage in physical activity. Individualized recommendations are necessary to ensure that a patient can safely engage in physical activity and adjust it as needed throughout different stages of their treatment.
Avoidance of Risky Substance
Smoking has detrimental impacts to both CVD health and cancer treatment. 12 People who continued smoking during treatment with cardiotoxic chemotherapies were associated with the highest risk of developing heart failure compared to people who never smoked and people who stopped smoking. 13 Effective strategies to encourage smoking cessation in people with cancer include long-term behavioral counseling as well as pharmacotherapies such as varenicline, bupropion sustained release, single or combination nicotine replacement therapy patch and/or lozenges. 14
Social Connection, Stress Management and Sleep
While the research on the impact on cardio-oncology of the other 3 pillars of Lifestyle Medicine: connectedness, stress management, and restorative sleep, is not as extensive, there is evidence that these pillars play an important role in the health and wellbeing of people with cancer. For instance, sleep disorders are associated with an increased risk of cancer and CVD mortality as well as an increased long-term mortality in cancer survivors. 15 While more research is needed in this area, screening for sleep disorders and educating people with cancer on the importance of sleep for their health is essential. In regards to social isolation, a 2018 study by Boel et al found that people with cancer who had feelings of higher social support were more likely to have a lower cancer mortality risk than people who felt like they had lower social support. 16 In another research study examining inflammatory markers in people experiencing social isolation, the authors concluded that the negative impact of social isolation is linked to elevated inflammatory markers in those who are less satisfied with the amount of social support they receive. 16 Additionally, there has been some evidence to show that CVD risk is elevated by social isolation and loneliness. 17 Lastly, stress has been shown to activate hypothalamic-pituitary-adrenal axis as well as the sympathetic nervous system causing suppression of the immune system and a pro-inflammatory state ultimately elevating risk of cancer. 18 All together, lack of sleep, social isolation and increased stress levels are all associated with higher inflammation in the body which has been associated with higher cancer risk and progression of cancer.16,18,19 Therefore, it is essential to include education and support for health behavior changes about sleep, social support, and reducing stress levels during and after treatment.
Treating Co-morbidities
As stated previously, CVD and cancer share many of the same risk factors. Continued treatment and monitoring of these risk factors, based on guidelines that focus on cardiovascular health through collaboration and a multidisciplinary approach is essential to preserving heart health and general health during cancer treatment.
Conclusion
Health care professionals are able to work interprofessional to provide holistic care to people with cancers. To provide individualized care—an interprofessional team approaching the patient from a holistic approach is essential.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.