
Abstract
Pharmacists are central in providing individual, patient-centered care that embraces education about medications and healthy lifestyles to optimize health. Nutrition is a part of the patient education provided, and it includes evidence-based recommendations for patients. However, oftentimes it may overlook the cultural, emotional, and social significance food plays in people’s lives. Considering culinary medicine into pharmacy education and practice can lead to more patient engagement and support healthier behaviors.
“Food Is Medicine refers to a spectrum of interventions that integrate food and nutrition into health care delivery to treat, manage, or prevent diet-related diseases.”
Introduction
This is a familiar patient encounter: A 58-year-old patient presents with hypertension and type 2 diabetes to pick up refills for lisinopril and metformin. The pharmacist counsels the patient about the medications and also discusses dietary changes, including salt intake, impact of different foods on glucose levels, and increasing vegetables and fiber. In this scenario, the pharmacist is providing holistic care, touching upon pharmacologic and nonpharmacologic recommendations, with a patient-centered approach. This is a typical conversation about nutrition a patient may often hear—centered around “do’s and don’ts.” This conversation is based on evidence-based medicine—that is, DASH diet or Mediterranean diet, or whole food plant-based diet and oftentimes the emphasis is about the “healthiness” of food, the impact on patient outcomes and objective parameters like glucose levels or blood pressure.1,2 However, while these recommendations lead to the prevention, mitigation, and reversal of diseases—it may overlook the role food provides in people lives—how memories are ignited by certain recipes, flavors, and scent. While the idea of “you eat to live” is fine for some, many live to eat—and food is tied to cultural identity, social connection, historical memories, and personal well-being. This is where culinary medicine comes in—it further blends the evidence-based dietary approach of food choices that prevent and manage disease, promote wellness, and improve clinical outcomes, combining it with the art of food preparation and cooking. 3
Culinary medicine represents an emerging, team-based approach that blends the science of nutrition with the practical skills of preparing and choosing food for health. While optimal implementation involves collaboration with experts trained in culinary medicine, the principles are relevant for all pharmacists. Pharmacists routinely engage in patient care conversations about food, nutrition, and chronic disease management. Expanding their understanding of culinary medicine—beyond the evidence-based nutrition education currently emphasized in pharmacy curricula—can enhance the quality and confidence of those discussions. At a minimum, such exposure strengthens pharmacists’ ability to connect clinical recommendations with real-world application; for those with greater interest, it can also provide a pathway toward advanced training and specialization in culinary or lifestyle medicine.
Brief Review of the Literature
A brief search, specifically about pharmacists and culinary medicine—resulted in a few findings—a couple of which are shared below to bring to light what is happening, conversations to get started, and hopefully ignite more to do and share. A poster presentation about the Clinic to Kitchen elective, a 2-credit course that brings together pharmaceutical science, pharmacy practice, and culinary medicine to help pharmacy students develop practical nutrition and culinary skills they can apply in patient care. Through a mix of classroom learning, hands-on kitchen experiences, and community engagement, the course aims to prepare future pharmacists to confidently provide nutrition-focused education and promote healthier lifestyles among their patients. 4 Additionally, food pharmacy programs are also being explored as ways to integrate pharmacists into nutrition-focused care. For example, there are programs where pharmacists provide education, medication adjustments, and blood pressure monitoring during weekly one-on-one visits to community-based events. Evidence suggests these programs can improve outcomes such as blood pressure and reduce health care utilization, while also fostering patient empowerment, relationship building, and advancing health equity. More research is needed to determine the most effective pharmacist involvement model. 5
Another aspect of heath via food is the concept that food is medicine (FIM). Food Is Medicine refers to a spectrum of interventions that integrate food and nutrition into health care delivery to treat, manage, or prevent diet-related diseases. These include medically tailored meals, produce prescriptions, and food pharmacies which are designed to improve health outcomes and reduce health care costs, particularly among populations with limited food access. 6
The Milken Institute report outlines a national framework to integrate Food is Medicine (FIM) services into pharmacy practice by positioning pharmacists as accessible providers of nutrition-related care. It includes 12 recommendations and 34 actions across payment policy, pharmacy workflow, and technology infrastructure. Core goals include establishing reimbursement pathways through Medicare, Medicaid, and employer-sponsored health plans; embedding FIM interventions within Medication Therapy Management; and expanding collaboration with dietitians and community health workers. The report also emphasizes developing seamless workflow systems, data interoperability, and technology solutions—like AI-assisted tools and bidirectional health record sharing—to support patient-centered, team-based nutrition care. Collectively, these strategies aim to make pharmacist-provided FIM services sustainable, measurable, and fully integrated within the broader health care ecosystem. 7
Intersection of Pharmacy Education and Culinary Medicine
Considerations for the Curriculum—Mapping It the ACPE.
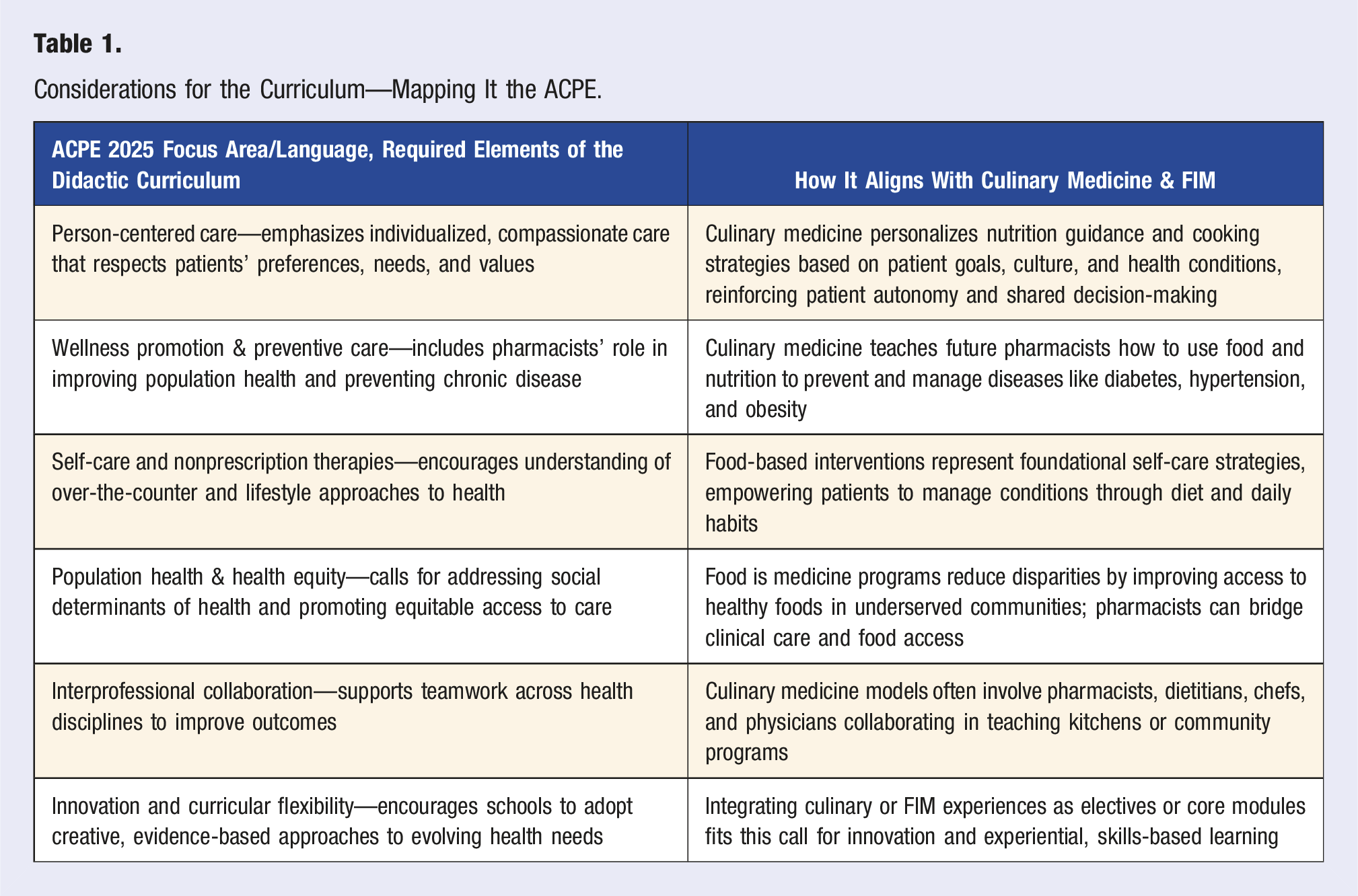
Example from the Culinary Medicine Approach
From the same example we started with, a culinary medicine approach, even with basic culinary training, could start by asking the patient, “Can you walk me through what a typical day of meals looks like for you? What foods do you really enjoy or grew up eating? That helps me provide recommendations that fit your life.” After understanding the patient’s preferences, the pharmacist could recommend options to help manage blood pressure and blood sugar, including adding vegetables, whole grains, and lean proteins to meals. The pharmacist might advise flavoring foods with herbs and spices instead of salt and suggest incorporating beans, lentils, and leafy greens for heart and glucose health. Additionally, the pharmacist could encourage the patient to check out cooking classes at the library or use cookbooks that adapt the foods they grew up enjoying into healthier versions, and refer them to a dietitian for more personalized guidance.
In this culinary medicine-informed counseling approach, the pharmacist maintains the same clinical goals but begins the conversation with curiosity and collaboration, asking the patient about their favorite meals and cooking habits. By linking sodium intake to the foods the patient actually eats, the pharmacist helps identify where salt “sneaks in,” whether during home cooking or when eating out. The pharmacist offers practical, achievable swaps, such as using herbs, garlic, and citrus instead of salt, rinsing canned foods or choosing low-sodium broths, and preparing simple dishes at home with budget-friendly ingredients. A handout or quick recipe may be shared, and if available, the patient is referred to a community cooking class or online resource. This approach connects clinical education to daily life, increasing patient confidence and engagement through applied learning.
Conclusions
Food is central to health, and providing healthy eating recommendations that are patient-centered and individualized is essential. Utilizing an interprofessional team approach ensures that patients receive comprehensive support. For pharmacists who are especially interested, additional training in culinary medicine is available, allowing them to deepen their skills. At a minimum, this approach should be taught and integrated in some way, enabling pharmacists to help patients embrace health while still enjoying the foods they love.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.