
Abstract
When effectively implemented, lifestyle interventions can lead to significant improvements in glycemic control, often reducing the need for glucose-lowering medications. However, guidance on deprescribing these medications following lifestyle changes remains limited. This study aims to characterize the deprescribing practices of lifestyle medicine clinicians for glucose-lowering medications in patients with T2D who undergo lifestyle interventions. A cross-sectional survey assessing provider demographics, deprescribing protocols, monitoring practices, and follow-up approaches was conducted among lifestyle medicine clinicians with prescriptive authority or involvement in therapeutic decision-making. Data were analyzed using descriptive statistics, and qualitative themes from open-ended responses were summarized. A total of 67 providers completed the survey. More than half (53%) reported having no established protocol for deprescribing diabetes medications, although respondents detailed individualized approaches based on glucose monitoring and patient progress. Providers most frequently deprescribed medications associated with hypoglycemia risk first (e.g., sulfonylureas and meal-time insulin). Common monitoring strategies included hemoglobin A1c (99%), fasting lipid profiles (86%), and continuous glucose monitoring (59% preferred). Hypoglycemia was reported as rare or uncommon in patients undergoing lifestyle medicine treatment.
Close monitoring of individualized lifestyle medicine treatment, while deprescribing diabetes medications, offers a surveilled method to reduce the morbidity and mortality associated with overtreatment.
Background
An estimated 462 million individuals are diagnosed with type 2 diabetes (T2D) around the world, corresponding to 6.28% of the global population. 1 T2D has acute and chronic impacts on both health and quality of life. Acute complications consist of hyperglycemia, diabetic ketoacidosis and coma, and hypoglycemia secondary to diabetes treatment. 2 Chronic complications include microangiopathy and macroangiopathy leading to hypertension, coronary artery disease, and diabetic retinopathy, nephropathy, and neuropathy. 2
Although lower rates of hyperglycemic emergencies are seen with increasing intensity of T2D management over the past decades, rates of hospital admissions for hypoglycemia secondary to overtreatment have increased. 3 Both internal guidance from healthcare systems and clinical practice guidelines focus their recommendations for the initiation of medications rather than their discontinuation. 4 However, deprescribing of medication is an essential component of effective medication management among clinicians, especially when patients make significant lifestyle changes. 4
Although family health history and ethnicity are associated with T2D risk, addressing modifiable risk factors such as low physical activity, unhealthy diets, obesity, and other environmental influences can promote diabetes prevention.5,6 Intensive dietary change has been shown to rapidly decrease the need for insulin, and even produce remission of T2D when patients adhere to a lifestyle-based protocol.7-10 Guidelines from the American Association of Clinical Endocrinology emphasize lifestyle modification and treatment of overweight/obesity as key pillars in the management of prediabetes and diabetes mellitus. 11 Other lifestyle modifications are also supported in an expert consensus statement from the American College of Lifestyle Medicine (ACLM), which identifies a diet of whole, plant-predominant foods as the most effective dietary intervention for achieving T2D remission. 12
The goal of T2D management is to maintain quality of life and prevent complications of diabetes. 13 This requires an individualized, multifactorial approach that balances treatment intensity, escalating care when goals are unmet and scaling back when patients are overtreated. 13 De-escalation, or deprescribing, is the process of reducing or withdrawing inappropriate medication, supervised by a healthcare professional with the goal of improving outcomes. 14 Some reasons for deprescribing are to manage polypharmacy, reduce medication-related adverse effects, and improve patient outcomes and quality of life. 15 Deprescribing rates in people with diabetes are typically low to moderate and only marginally influenced by participants’ comorbidity or frailty. 16 Providers are hampered in managing deprescribing due to lack of knowledge, fear of disease state worsening, poor communication and collaboration between healthcare providers, and lack of guidance resources. 17 Prior studies show that providers find relevant training and resources in deprescribing helpful in initiating related discussions with their patients.17,18 Established protocols thus vary, as at the time of data collection for this study, there had been no standardized guidance for deprescribing or de-escalating T2D medications in the context of reduced need for medication following lifestyle modifications.
The current study builds upon previous work in a case series of provider-deprescribing protocols, which demonstrated the feasibility of deprescribing glucose-lowering medications and provided preliminary insight into the practices of providers with experience in doing so. 15
The objective of this current study was to characterize the practices of a larger sample of lifestyle medicine clinicians for deprescribing glucose-lowering medications following lifestyle interventions among patients with T2D.
Methods
Survey Design
The cross-sectional survey was developed iteratively with the research team, with the initial draft substantially informed by the previous qualitative work 15 done to characterize the deprescribing practices of lifestyle medicine clinicians. A pharmacist with experience in deprescribing was also consulted to review questions and answer choices. The survey was revised by the principal investigator, consulting pharmacist, and reviewed by lifestyle medicine clinicians with experience in deprescribing T2D medications. 15
Survey Administration
This study was reviewed by the University of New England Institutional Review Board. All respondents provided informed consent. The survey was hosted in QuestionPro (https://www.questionpro.com), a secure survey platform for research, and was open for 8.5 weeks, from October 12 to December 12, 2022. Members of ACLM as well as registrants of the past annual ACLM conferences (totaling n = 9357 at the time of administration) were contacted via email with an invitation to complete the anonymous survey, with one email reminder sent before the survey closing date.
Data Analysis
Survey responses were included in the analysis if the participant was 18+ years, answered “yes” to being involved in the care of patients who have been treated using lifestyle medicine interventions, answered “yes” to having prescriptive authority or making therapeutic decisions under a collaborative practice agreement, and had provided any answer to the key question of interest: Do you have an established protocol for diabetes medication management and care? Analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC), with quantitative data summarized to produce descriptive statistics. The principal investigator reviewed free-text data and identified and summarized themes that emerged; these themes were compared to raw data and confirmed by a second team member. This study was reviewed by the University of New England IRB. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of the research.
Results
Characteristics of Participants and Practices.
SD, standard deviation; T2D, type 2 diabetes.
aParticipants could select multiple options so percentages will not add to 100.
bCountries outside of the United States of America include Canada, Chile, Colombia, India, Iran, Namibia, the Philippines, Poland, and the Republic of North Macedonia.
cOther clinical degrees include PhD in physiology-endocrinology and Masters of Public Health.
dOther ABMS specialties include cardiology, pediatrics, endocrinology, obesity medicine, emergency medicine, neurology, radiology, registered medical practitioner for general practice, and functional medicine.
eDemographic of patient population served as reported by physicians.
fOther health professionals include psychologist (behavioral health), case manager, plant-based chef, counselor, health psychologist, licensed practical nurse, certified, medical assistant, and midwife.
Approximately one-third of respondents were from the Southern United States (33%), followed by the West (21%), and Midwest (17%). Fourteen percent of respondents were from outside of the United States. The most commonly reported credentials included Doctor of Medicine (66%), Doctor of Osteopathic Medicine (14%), or physician associates/assistants (11%). Thirty-six percent of respondents reported being in practice for less than 10 years (36%), while 30% reported over 20 years.
The majority of providers were board-certified in lifestyle medicine (50%), while 29% were pursuing certification. The most represented medical specialty was family medicine (36%), followed by internal medicine (26%), and preventive medicine (5%). Seventy-seven percent of respondents practiced lifestyle medicine in part, and 18% reported that their practice was entirely lifestyle medicine.
Respondents practiced across a variety of settings, including private practices (22%), hospitals or non-academic health systems (21%), academic health systems (19%), community health settings (18%), and residencies (9%). Of the health systems represented, many were a part of a larger network (18%) or integrated delivery network (12%). Thirty-three percent of respondents reported practicing in an accountable care organization and an additional 33% in remote monitoring or telehealth, followed by 27% in a Medicare Merit-based Incentive Payment Systems.
The majority of respondents worked as part of medical teams incorporating a variety of different healthcare professionals treating T2D patients including other physicians (62%), registered dieticians or nutritionists (39%), and nurse practitioners (33%). The most common patient populations served were White (84%), Black or African American (54%), and Asian (31%), with 54% reporting serving patient populations that were Hispanic or Latino. Most frequent challenges faced among these patient populations, as reported by respondents, were residence in low-income or underserved areas (64%), having food insecurity and low access to healthy options (57%), backgrounds that were racially, ethnically or culturally diverse (52%), and low literacy levels (40%).
Deprescribing and Monitoring Practices.
aOther fasting methods include waiting at least an hour after waking to eat, and finishing eating at least 2-3 h before bedtime.
bOther ranges include 70-89 mg/dl, 80-130 mg/dl, <130 mg/dl, <100 mg/dl, under 7 mmol/L, ranges customized based on age and comorbidities, and differing ranges in Canada.
cOther ranges include 70-89 mg/dl, 80-130 mg/dl, <130 mg/dl, <100 mg/dl, under 7 mmol/L, ranges customized based on age and comorbidities, and differing ranges in Canada.
The most commonly reported fasting blood glucose ranges by respondents were 70-110 mg/dL (42%) and 90-130 mg/dL (42%) during the lifestyle medicine active treatment and maintenance phases, respectively. In terms of post-prandial blood glucose monitoring, target ranges during lifestyle medicine active treatment were 110-150 mg/dL (35%), less than 180 mg/dL (29%), and 70-110 mg/dl (3%).
The majority of respondents (56%) determine how frequently they monitor blood sugar on a case-by-case basis, followed by 21% monitoring once a week, and 12% monitoring once a day. The most common method of having patients perform self-management of blood glucose was through a glucometer (89%); however, the top preferred method of patients’ self-management was through continuous glucose monitoring (CGM) (59%). Many providers (69%) prefer practicing both in-person and virtual follow-ups with patients who have had medications deprescribed, 46% of providers follow-up in 3-4 weeks regarding diabetes medication management, while others (34%) follow-up in 1-2 weeks.
Glucose Monitoring and Deprescribing Rationale.
ADA, American Diabetes Association; BMI, body mass index; CGM, continuous glucose monitoring; GLP-1 receptor agonists, glucagon-like peptide-1 receptor agonists.
aOther circumstances: Occurs when discontinuing medications, and low-literacy patients do not obey the prescription and the orders correctly.
bOther instructions: Whole fruits, fiber bars, glucose gel, protein-carb snacks, medication adjustments, and preventive education. Some advised waiting if symptoms were mild and no medication was involved.
Cases of hypoglycemia were triggered among patients undergoing lifestyle medicine treatment most commonly while taking sulfonylureas (51%), basal insulin (43%), and meal-time insulin (39%). A total of 25% of cases occurred during the first 1-2 weeks of active treatment, while 2% occurred during the maintenance phase of treatment. Most providers instruct patients to manage a hypoglycemic episode by having juice or hard candy (79%), oral glucose tablets (15-16 g) (51%), or through a glucagon subcutaneous/intramuscular injection (12%).
Free-text responses from individual survey respondents describing how they make specific de-escalation decisions per medication are found in online supplemental Tables S1-S4. Themes expressed by respondents in free-text answers regarding reasoning behind the de-escalation decisions by medication type were summarized as follows:
Meal-time insulin: Most providers decrease over days or weeks based on post-prandial glucose measurements and continue monitoring regularly.
Basal insulin: Many providers decrease over days or weeks by regular amounts with consistent intervals, with some decreasing larger intervals initially. Some make decisions based on blood sugar readings and the severity of hypoglycemia.
Insulin secretagogues: Most providers either stop completely or decrease the dose by half. This class is often deprescribed earlier due to associated adverse effects.
Glucagon-like peptide-1 receptor agonists: Some taper by monitoring A1C levels; providers may not discontinue this class as quickly because patients appreciate the associated weight loss.
Sodium-Glucose Cotransporter-2 (SGLT2) inhibitors: Varying criteria for deprescribing; some decrease later in the deprescribing process, or not at all for the potential cardio-protection. Others also stop more quickly or at least taper off as soon as possible.
Metformin: Most providers decrease over months. Metformin is often the last medication to be discontinued. Continue monitoring based on patients’ A1Cs.
Other oral medications—Dipeptidyl Peptidase-IV inhibitors, Thiazolidinediones: Most providers stop this class as soon as possible. A few reported beginning with a larger initial decrease of this class, and others stated not using this class at all.
Respondents suggested a variety of factors influence decisions about how much insulin to drop at a time as reported in Table 3. Respondents report this decision is data driven using discrete blood glucose measurements (57%), informed by the degree of dietary change that is adopted (45%), data driven via CGM device (42%), or as a preemptive dose reduction for safety (34%). The most important factors in making this decision are represented in Figure 1. Considerations for deprescribing insulin. 1n = 9 preferred not to answer. Abbreviations: BMI: body mass index; CGM: continuous glucose monitoring; HOMA-IR: homeostatic model assessment of insulin resistance.
De-escalation practices vary in the context of specific glucose-lowering medications. When a patient is on metformin, 81% of respondents report an initial taper of metformin dose before discontinuation, while 13% would discontinue metformin completely. When a patient is on pioglitazone, 48% of respondents reported an initial taper of medication dose prior to discontinuation, while 42% reported discontinuing pioglitazone completely. In patients taking glucagon-like peptide (GLP) analogs, 48% of providers reported an initial taper of medication before discontinuing, while 39% reported discontinuing GLP analogs completely.
The most frequently reported order of medications to deprescribe is represented in Figure 2. Most frequently reported class of medication deprescribed first. 1n = 3 prefer not to answer. *Next option based on patient preferences. Abbreviations: GLP-1 receptor agonists: glucagon-like peptide-1 agonists; SGLT2 Inhibitor: sodium-glucose cotransporter-2 inhibitors.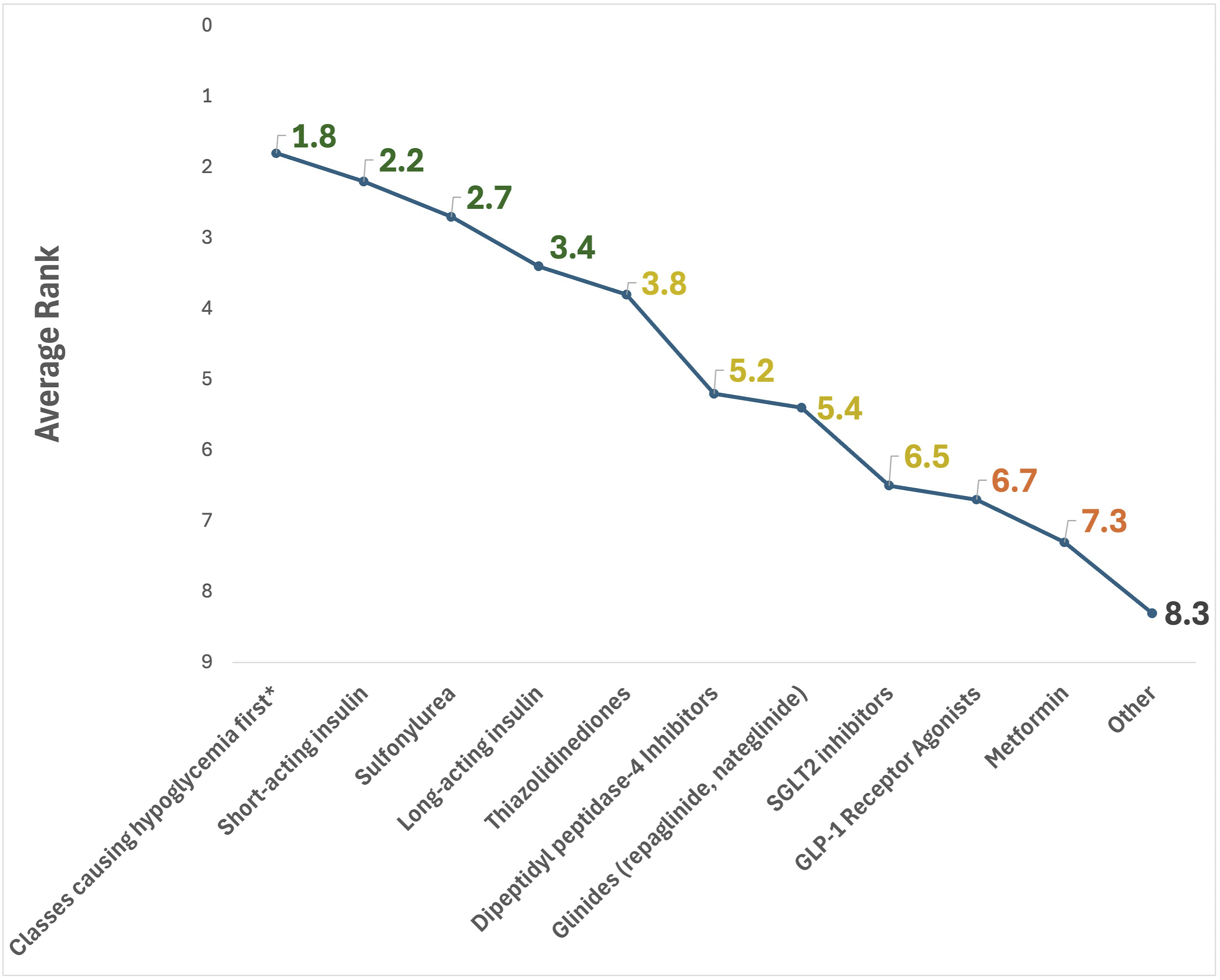
Most providers deprescribe classes of medication that cause hypoglycemia first, and the next option is based on patient preferences. This is followed by the de-escalation of short-acting insulin, followed by sulfonylureas. The reasons for deprescribing in the order represented in Figure 2 are related to the medications most likely to cause hypoglycemia (90%), other negative side effects (67%), patient preferences (36%), and cost (34%).
In cases of patients who are on oral medications and injectable insulin, respondents most frequently prioritized de-escalating injectable short-acting insulin or medications most likely to cause hypoglycemia. Long-acting insulin was prioritized less frequently, and oral meds or non-insulin injectable medications were prioritized least frequently (data not shown).
Discussion
This study deepens the understanding of how providers deprescribe glucose-lowering medications in T2D patients following lifestyle medicine treatment. Of the providers surveyed in our study, over half (53%) did not have an established protocol for deprescribing diabetes medication, though nearly all providers shared specific considerations on how they approach decision-making based on prior experience. This is related to the lack of evidence-based guidelines at the time of survey administration for deprescribing practices. Although treatment for T2D patients must be individualized based on their health status and other comorbidities, this data offers insight into how providers customize their deprescribing decisions.
Although specific care and decisions must be made in the individual context of each patient, there were consistent responses among providers on how to monitor patients’ blood glucose levels through the deprescribing process. The most common laboratory tests used are hemoglobin A1c, fasting lipid profile, microalbumin/creatinine ratio, and comprehensive metabolic panel, aligning with the ADA’s recommendation for routine hemoglobin A1c testing in all patients with diabetes at initial assessment and during ongoing care. 19 The ADA also recommends annual testing for albuminuria at diagnosis of T2D, and assessing insulin resistances or hyperinsulinemia by measuring plasma lipid/lipoprotein concentrations. 20 Target fasting blood glucose ranges identified by study respondents (70-110 mg/dL during active lifestyle medicine treatment and 90-130 mg/dL in the maintenance phase) align closely with the ADA’s recommendations of 80-130 mg/dL for pre-prandial and under 180 mg/dL post-prandial among nonpregnant adults. 19
Respondents in this survey reported several repeating perspectives, in particular, the importance of tailoring treatment to the individual based on monitoring. Most clinicians (56%) reported the frequency at which they request their lifestyle medicine patients to check their blood sugars varies based on the circumstances of the case, suggesting that a framework for deprescribing should be flexible. Clinicians understand that deprescribing, just like prescribing, must be individualized.
Both self-monitoring of blood glucose (SMBG) via glucometer and CGM enable patients to individually monitor their glycemic control. 19 This promotes autonomy for patients and patient-centered care for providers. Our results suggest that patients prefer SMBG as current systems are easy to use, require minimal blood samples, and provide efficient readings. 21 Many, but not all, of the available SMBG systems meet the required standards of accuracy.21-23
Healthcare providers should be familiar with accurate SMBG options for their patients, such as those listed by the Diabetes Technology Society Blood Glucose Monitoring System Surveillance Program. 19 While CGM is the preferred method among providers in this survey, the most common method is SMBG via glucometer. A systematic review found CGM use in T2D significantly lowers hemoglobin A1c compared to SMBG. 24 The 2026 ADA Standards of Care recommend CGM for adults on multiple daily injections, insulin pumps, and select basal insulin users, as well as adolescents with T2D on intensive insulin therapy. 25 While CGM enhances care by allowing clinicians to detect trends, adjust treatment proactively, and reduce hypoglycemia risk, SMBG via glucometer remains an option for those without access. ADA guidelines recommend assessing glycemic status with hemoglobin A1c and CGM metrics at least twice a year. 25
The surveyed providers emphasized the importance of developing a tailored follow-up plan for deprescribing with their patients. 26 In this study, providers most often follow up either in-person or virtually within 3-4 weeks (46%) or 1-2 weeks (34%) of the initial deprescribing. This is consistent with results from the prior qualitative study. 15 According to the ADA, follow-up visits for comprehensive medical evaluation of T2D patients should occur at least every 3-6 months, and then annually; a recent study, however, found benefits in increasing encounter frequency among patients who had not yet achieved cardiometabolic control. 27 Thus, a follow-up frequency of at least 3-4 months with further assessments made on a case-by-case basis may be optimal. “Intensive therapeutic lifestyle change” interventions which produce more rapid changes in glucose and insulin may require more frequent monitoring.
One of the most serious complications T2D patients may face is hypoglycemia from overtreatment during a period of lifestyle change. At the time the survey used in this study was created, the ADA defined hypoglycemia as a plasma glucose of <70 mg/dL and <54 mg/dL as clinically significant hypoglycemia. 28 The Standards of Care published in 2026 define hypoglycemia into three levels: Level 1 < 70 mg/dL but ≥54 mg/dL, Level 2 < 54 mg/dL, and Level 3 as a severe event of altered mental or physical functioning that requires assistance, regardless of glucose level. 19 Respondents in this survey stated that cases of clinically significant hypoglycemia of less than 70 mg/dL in patients undergoing lifestyle medicine active treatment are rare or uncommon. This is in contrast to a 2014 study from the Centers for Disease Control and Prevention that reported an estimated 97,648 emergency departments visits for insulin-related hypoglycemia and errors, with almost one-third resulting in hospitalization. 29
Drug-induced hypoglycemia can also be a concern, with a prior study suggesting a relative frequently of 46%. 30 Previous studies show that most cases of hypoglycemia occur in patients with diabetes who are undergoing intervention with meglitinides, sulfonylureas, or insulin.19,31 Additionally, certain medications, particularly incretin mimetics (GLP-1 and GIP/GLP-1 combinations), can impact appetite and lead to a reduction in calorie intake. Without corresponding adjustments to other medications, this can increase the risk of hypoglycemia in patients. In our study, providers tended to deprescribe the medications that are most likely to cause hypoglycemia first, followed by deprescribing injectable short-acting insulin, sulfonylureas, and then long-acting insulin among others. When a patient is on oral glucose-lowering medication and injectable insulin, however, respondents tend to de-escalate injectable short-acting insulin first, followed by the deprescribing of medications that are most likely to cause hypoglycemia, and then long-acting insulin.
Lifestyle interventions, even when dosed intensively, will not cause hypoglycemia unless T2D medications are also in use. A number of clinical trials of T2D stopped all T2D medications when they put the subjects on very low energy diets or fasts. For this reason, clinicians may be less skeptical about deprescribing T2D medications during or following lifestyle changes. Close monitoring of individualized lifestyle medicine treatment, while deprescribing diabetes medications, offers a surveilled method to reduce the morbidity and mortality associated with overtreatment.
This order of deprescribing aligns with studies showing long-acting insulin has lower hypoglycemia rates than intermediate-acting insulin, particularly in patients using both oral glucose-lowering medications and long-acting insulin, while short-acting and rapid/ultra-rapid insulins (e.g., lispro, aspart, and fast-acting insulin aspart) are more likely to cause post-prandial hypoglycemia.32-35 The most common reasoning behind specific orders of deprescribing among respondents in this study was the medications most likely to cause hypoglycemia, other negative side effects, and patient preferences. Other negative side effects of insulin therapy include weight gain and rarely electrolyte disturbances, such as hypokalemia. 35 Glucose-lowering medications have many non-specific adverse effects as well, such as nausea, vomiting, diarrhea, and elevation of hepatic enzymes. 36
Although there are previous studies on current practices of deprescribing of T2D medications, there is limited consensus among recommendations. One study found that deprescribing strategies were limited to newer agents and insulin management for elderly individuals. 37 They also found that the dose reduction of SGLT2-inhibitors and GLP-1 receptor agonists depends on adverse events. 37 The results summarized in this study, however, mostly were specific to medication use among patients with specific characteristics or comorbidities, such as de-escalating insulin therapy among older adults and discontinuing SGLT2-inhibitor therapy in patients with symptoms of diabetic ketoacidosis. 37 The authors also emphasized the lack of a standardized approach for deintensification of medications, and suggested gradually discontinuing medications, starting with sulfonylureas and transitioning to metformin and Dipeptidyl Peptidase-IV inhibitors, although specifically among frail patients. 37 A randomized, controlled trial among patients with poorly controlled T2D examining de-escalation from advanced insulin therapy (AIT), found that stepping down from AIT to “combined use of metformin, SGLT2i, GLP-1 receptor agonists and basal insulin” may be better than a multiple daily insulin injection approach. 38 These methods are consistent with the recently published clinical practice guideline from ACLM on lifestyle treatment for T2D and prediates in adults, which does provide recommendations on de-escalation of glucose-lowering medications in the context of lifestyle treatment, and also prioritizes deprescribing first those medications that are most likely to cause hypoglycemia such as sulfonylureas, insulin, and meglitinides. 39
The results of our study align with both ACLM's formal clinical guidance 39 and those from the previous case series that outlined the deprescribing protocols of nine different providers, in which all but one reported working with an interdisciplinary team of allied healthcare providers. 15 Seven providers reported not using a published, externally documented protocol or algorithm for medication deprescribing. 15 This is consistent with the 53% of providers surveyed in this current study who reported not having an established protocol for diabetes medication management and care. It is the authors' hope that such clinicians will use the now published recommendations from ACLM 39 going forward. Laboratory testing parameters and target ranges of blood glucose were similar between these two studies with both finding that the most common tests were basic metabolic panel and comprehensive metabolic panel, hemoglobin A1c, and C-peptide level. 15
Providers in this previous study had a similar order of and rationale behind deprescribing of insulin and other glucose-lowering medications, with an individualized approach, focused on starting with sulfonylureas, insulin, and other medications known to cause hypoglycemia first, followed by metformin and GLP-1 receptor agonists later or to continue these medication classes in the patient’s treatment regimen. 15 This study also indicated rare reports of hypoglycemia; in addition, clinicians reported targeting sulfonylureas first because of the potential to accelerate decline in beta-cell function, and thiazolidinediones were commonly targeted due to concerns of weight gain and exacerbation of heart failure. 15
Limitations of this study include its relatively small sample size (n = 67); however, it should be noted that this study does build upon a previous case series (n = 9) on the same topic. This study aims to understand deprescribing among those who practice LM; thus, we intentionally surveyed lifestyle medicine clinicians with prescriptive authority or involvement in therapeutic decision-making. Results may not be generalizable outside of this setting. Another limitation is that this analysis does not prospectively follow adverse events. This study offers novel information in summarizing a stepwise process of and rationale behind deprescribing practices among clinicians. A strength of the survey utilized in this study is that it was designed in close collaboration with clinicians and pharmacists with expertise in clinical decision-making related to glucose-lowering medications. Finally, this survey was administered to a sample of clinicians who reported having expertise in the deprescribing of glucose-lowering medications following lifestyle medicine intervention, which contributes to the credibility of the findings.
Although improvements in glycemic control are commonly used to guide medication deprescription in T2D, underlying beta-cell reserve is also an important determinant of sustained medication discontinuation. Individuals with preserved beta-cell function may be more likely to tolerate deprescription concurrent with lifestyle intervention, whereas those with reduced pancreatic capacity may require ongoing pharmacologic support. Emerging approaches, such as assessment of beta-cell function using HOMA2-B, may help guide deprescribing decisions beyond insulin resistance-focused metrics (HOMA2-IR) or glycemic indices alone in future studies. For example, misclassification of diabetes subtype, particularly latent autoimmune diabetes in adults (LADA), remains a clinically relevant concern. Future studies of lifestyle-based deprescription would benefit from more precise diagnostic stratification, including phenotypes characterized by primary pancreatic insufficiency in older adults (type 4 diabetes) and reduced pancreatic capacity related to poor maternal nutrition in utero (type 5 diabetes) among others.
Conclusion
Results of this study can better inform providers in need of example methods for making decisions on deprescribing patients from glucose-lowering medications after initiation of the lifestyle medicine diabetes management. Self-reported observations of hypoglycemia from providers suggest that adverse events in the context of lifestyle interventions and deprescribing are rare, and lifestyle treatment, when supervised by experienced providers, is safe for patients with T2D. More evidence and research are necessary to continue to create guidance documents on the best deprescribing practices of glucose-lowering medications in patients with T2D.
Supplemental Material
Supplemental Material - Medication Deprescribing Practices Among Lifestyle Medicine Providers: A Cross-Sectional Survey
Supplemental Material for Medication Deprescribing Practices Among Lifestyle Medicine Providers: A Cross-Sectional Survey by Joeita Macfield, Kara L. Staffier, John Kelly, Rohit Moghe, and Micaela C. Karlsen in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors wish to thank the lifestyle medicine clinicians who responded to this survey and shared their experience, as well as the American College of Lifestyle Medicine staff involved in sending the survey recruitment emails.
Author Contributions
MCK and JK contributed to the original conception and design of the study methods with feedback from RM. MCK and KLS participated in data collection and analysis. JM led the writing with support from all other authors who offered critical feedback. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ardmore Institute of Health (AIH) and the American College of Lifestyle Medicine (ACLM). AIH had no involvement in the design or execution of the study or analysis of the data. All authors were affiliated with ACLM, either as staff or members.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kara L. Staffier and Micaela C. Karlsen are employed as staff by the American College of Lifestyle Medicine (ACLM). John Kelly and Rohit Moghe are members of ACLM, and Joeita Macfield is an independent consultant of ACLM.
Data Availability Statement
De-identified data generated from the study are available from the corresponding author upon reasonable request and in accordance with IRB guidelines.
Supplemental Material
Supplemental material for this article is available online.