
Abstract
Attention-Deficit/Hyperactivity Disorder (ADHD) persists into adulthood for many and can also be newly diagnosed in adults. ADHD coaching is a form of support that can be used independently or integrated into a multimodal treatment approach. This report presents pre-post intervention findings from a single-arm mixed-methods study of a 12-session individual ADHD coaching engagement for adults. Coaches meeting defined criteria recruited clients through their private practices, screening for study eligibility. The coaching engagement followed a manualized approach, and coach-client working alliance was high. Goal attainment yielded positive results; and from pre- to post-test, statistically significant improvements, with medium to large effect sizes, were found using validated instruments measuring ADHD symptoms, executive functioning (EF), and functional impairment. The training, credentialing, and experience of coaches and the fairly homogenous client sample (e.g., gender, race, and education) must be considered in generalizing the results.
“Using widely accepted, valid self-report measures, statistically significant improvements in ADHD symptoms, executive functioning, and functional impairment were documented with medium to large effect sizes.”
Background
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by inattention, hyperactivity/impulsivity, or a combination. 1 ADHD is increasingly understood to impact the executive functions (EFs) of the brain, the neuropsychological processes that organize and manage cognitive functions and goal directed behavior. Studies have also linked ADHD to functional impairments across major life domains, 2 and untreated ADHD has been associated with an increased risk of personal and public health concerns. 3
While previously considered largely a disorder of childhood, according to the CDC, more than 15 million adults in the US have ADHD, half of whom received their diagnosis in adulthood. 4 The prevalence of ADHD in adults is in the range of 2.5% to 6.8%. 5
ADHD Treatment
Although stimulant medication is the most common treatment for ADHD, multimodal care is now understood to be optimal. Such care typically involves medication management; therapy for the emotional challenges inherent in living with ADHD and its common comorbidities; as well as behavioral modalities, typically Cognitive Behavioral Therapy (CBT) and/or ADHD coaching. Behavioral modalities are generally considered key for achieving improvements in functional areas, including organizational skills and academic and employment success.6,7 Specialized ADHD coaching has shown benefit in a number of studies. 8
Literature Review
Research on ADHD Coaching
Employed since the early 1990s, ADHD coaching is defined by the ADHD Coaches Organization as a “collaborative, supportive, goal-oriented process in which the coach and the client work together to identify the client’s goals and then develop the self-awareness, systems, skills, and strategies necessary for the client to achieve those goals and full potential.” 9
Some 20 studies on ADHD coaching outcomes—three of which were randomized controlled trials (RCTs)—vary in size (sample sizes ranging from 1 to 1782 participants) and research design and, as a whole, demonstrate evidence of improvement in clients’ executive functioning and, in some cases, ADHD symptoms, functional impairment, and/or well-being. 8 Maintenance of gains, and high client satisfaction have also been documented.
While ADHD coaching is offered across the age span, most research on ADHD coaching outcomes has been conducted with college students, and several studies have focused on children and teens. To date, three published outcome studies,10-12 two qualitative studies,13,14 and a case report 15 have examined coaching for adults with ADHD.
ADHD Coaching for Adults
Among the three quantitative studies exploring ADHD coaching for adults, Bloemen et al reported on eight weekly 2-hour long group coaching sessions for ten adults, demonstrating improvement from pre- to post-coaching in daily functioning, measured by the Weiss Functional Improvement Rating Scale, and in symptoms, reported by significant others (e.g., spouses), but no self-reported symptom improvement on the Attention Deficit Self Rating Scale. 10 Kubik examined outcomes of seven group ADHD coaching sessions, among 45 adults, assessing outcomes with a 41-item measure addressing 22 “areas of concern.” 12 A “strong impact” of ADHD coaching was reported across varied dimensions including cognition, distractibility, inattention, and social and behavioral outcomes (p. 450), measured at a one-to-four-year post-coaching period. Additionally, Ebrahimi et al examined outcomes of 11 sessions of individual executive function coaching for 17 adults, finding statistically significant improvements in select neuropsychological tests. 11
A qualitative study of perceptions of ADHD coaching among 23 adults documented that, for some, a coaching model offers an approach to addressing ADHD concerns that is preferred over mental health counseling. 13 A qualitative case series of three women reported that participants valued coaching for reasons including: re-evaluating their self-identity; receiving psychoeducation about the neurobiology of ADHD and executive functioning; and training in executive function skills. 14
In the broader health and wellness coaching literature, coaching has shown benefit for health promotion, and both disease prevention and management, in hundreds of studies for adults with a wide range of conditions, including some mental health concerns.16-18
Coach Effects and Working Alliance
Both practitioner effects and therapeutic alliance can account for some variation in client outcomes in psychotherapy, and possibly coaching.19,20 The use of experienced practitioners, trained in a manualized intervention, can minimize practitioner effect. 21 To date, neither coach effect nor working alliance has been explored in the ADHD coaching literature.
Study Purpose and Hypotheses
The study reported here is a single-arm prospective investigation that was part of a larger mixed-methods study of ADHD coaching for individual adults.
Hypotheses: A 12-session ADHD coaching engagement is related to improvements in: ○ ADHD symptoms ○ Executive functions (EFs) ○ Functional impairment
Exploratory Question: What is the client experience of goal attainment as a result of 12-sessions of ADHD coaching?
Methods
This single-arm pre-post study of a 12-session coaching engagement was part of a larger mixed-methods study approved by the Institutional Review Board (IRB) at Maryland University of Integrative Health. This investigation was funded by the IOC-ICF coaching research grant program, which is led by the Institute of Coaching and funded by the International Coaching Federation. Coaches and clients who participated provided informed consent. This report follows the guidelines of the Boutron et al 2008 extension of the CONSORT statement for reporting non-pharmaceutical RCTs, 22 taking into account that this study was not an RCT.
The study purpose was to examine the effects of coaching on ADHD symptoms, executive functioning, and functional impairment as well as client goal attainment. Outcomes of a 6-week follow-up survey and qualitative aspects of the study are reported separately.23,24
Coach and Client Recruitment
The study recruitment and data collection took place between November 2022 and February 2025. A convenience sample of ADHD coaches was recruited through various outreach efforts and snowball sampling. Coaches met the following eligibility criteria: Minimum of 60 hours coach training Minimum of 25-35 hours ADHD-specific coach training Minimum of 1 year ADHD-specific coaching experience Coach credential from the International Coaching Federation and/or the Professional Association of ADHD Coaches Minimum 75% of clients in the US
The recruited coaches were oriented to study procedures, including both how to enroll clients in the study and a previously developed manualized coaching intervention (ACE-MI) providing guidelines for a 12-session coaching engagement for adults with ADHD.25,26 Coaches received a small honorarium for participation in the training and for completing 12 post-session surveys per client, designed to assess fidelity to the manualized intervention. While 45 coaches were initially engaged, only 26 actually participated in the study by enrolling clients and coaching them. Of these 26 coaches, 21 had one or more clients complete the full study.
Study coaches could invite participation by any of their new adult clients who met eligibility criteria (Box 1). The study design resulted in a convenience sample of client participants, 60 of whom began coaching, and 45 of whom met inclusion criteria and completed the coaching engagement. Forty-three of these participants completed the post-coaching survey. Among the coaches, the distribution of the 43 participants was as follows: ten coaches had one client each; six had two each; one had three; two had four each; and two, five each.
Coaching fees and arrangements were managed directly between each coach and client. For the part of the larger study reported here, participating clients completed surveys online via Survey Monkey before coaching started and at the conclusion of the 12-session coaching engagement. Clients received a modest honorarium for completing all aspects of the study.
Power calculations for the study instruments indicated that approximately 40 paired data points from adult ADHD coaching clients would be needed to detect an effect size of 0.5 with 80% power and an alpha of 0.05. This sample size also accounted for an approximately 20% attrition rate. Box 1. Client Eligibility Criteria • Inclusion criteria: ○ Adults 21 years of age and over ○ ADHD diagnosis (client report) ○ High school graduate or GED ○ First engagement working with a coach ○ Fluent in English • Exclusion criteria: ○ Substance Use Disorder (past 3 months) ○ Psychotic disorders ○ Active suicidal ideation ○ Eating disorders ○ Organic neurological conditions ○ Organic mental disorders ○ Full time student
Coaching Engagement (Intervention)
Experienced ADHD coaches holding credentials from the International Coaching Federation and/or the Professional Association of ADHD Coaching, with training specific to ADHD, utilized a previously developed manualized intervention (ACE-MI) for the 12-session coaching engagement.25,26 The ACE-MI allows for individualization to the coach and client dyad, as is common practice. The frequency of the 12 sessions was determined by each coach and client, and each dyad was free to continue coaching, or not, at the conclusion of the 12-session engagement.
Data Collection
Coach and client demographic data was collected through online surveys, using SurveyMonkey. The initial client survey (pre-test) was conducted before coaching began, and the post-coaching survey was completed at the conclusion of the 12-session coaching engagement. Several adverse events reported to the IRB (client personal or family health concerns) briefly impacted the participation of four clients in the study. None required a client to drop out or led to changes in the study methodology.
Study Measures
This study used the scales listed below for pre- and post-coaching measurement of the key outcome variables of ADHD symptoms, executive functioning, and functional impairment: ADHD symptoms: The 18-item ADHD RS-SRV
27
was modified for this study, with permission of its author, to focus only on symptoms in the one month preceding completion of each survey. Because an incomplete scale would be difficult to interpret, we required responses to every question on this scale. Executive functioning: The 20-item short form Barkley Deficits in Executive Functioning Scale, self-report version (BDEFS-SF for Adults)
28
was modified to focus only on symptoms in the one month preceding completion of each survey. Since an incomplete scale would be difficult to interpret, we required responses to every question on this scale. Functional impairment: The 69-item Weiss Functional Impairment Rating Scale - Self Report version (WFIRS-S).
29
Data on therapeutic alliance was collected at the post-coaching timepoint, as a possible control variable, using the 12-item Working Alliance Inventory - Short Revised version (WAI-SR). 30 For the version used in this study, items were rated from 1 (seldom) to 5 (always). The wording of all the questions was modified to assess coach–client rather than therapist–client alliance.
Additionally, several questions were included in the post-coaching survey to explore the study question “What is the client experience of goal attainment as a result of 12-sessions of ADHD coaching?”
Data Analysis
All data analysis was completed in the latest version of R available (4.4.3 or 4.5.1). Analysis included the following steps: Basic descriptive statistics (means, SDs, medians, percentages, and counts) were used to summarize both coach and client participant characteristics, as appropriate for the data types and respective distributions, and for the exploratory questions. Fidelity of implementing the manualized intervention was calculated as the percentage of “yes” coach responses to survey items about each component of the 12 sessions of the manualized intervention (ACE-MI) for the coaching engagement. Overall compliance with 60-80% or more of the required components was considered indicative of fidelity to the manualized intervention.
31
For study measures, the ADHD-RS-SRV and the BDEFS-SF were each scored by summing the items. The WFIRS-S was scored by calculating a mean of the item scores, after removing N/A and missing items. The WAI-SR survey was scored as a total sum. For one participant, the value for one item on the WAI-SR was missing, and that item score was imputed by taking the mean scores of the responses to the other items. Demographic characteristics of individuals completing the coaching engagement and post-coaching survey (completers) were compared to those of individuals starting but not completing the coaching (non-completers) using absolute differences in percentiles. The preliminary analysis used multi-model inference with Akaike information criterion (AIC)
32
to compare statistical models and identify the best-fit equation for each outcome variable while accounting for a penalty based on the number of independent variables. For all three outcome variables (ADHD RS-SRV, BDEFS-SF, and WFIRS-S), the best-fit model included the variables coach and client within coach; for the BDEFS-SF and WFIRS-S, the model also incorporated question variation. These served as control variables for further analysis related to each outcome. Working alliance (WAI-SR) did not contribute to the best-fit equation in any case. For hypothesis testing, the best-fit model for each outcome variable, determined by AIC, was used to assess the change in scores from pre- to post-coaching, using a t-test. Statistical significance was set at P < 0.05 for hypothesis testing. Cohen’s D effect size of the period differences was obtained, using a client-to-client standard deviation. Generally, effect sizes of 0.2, 0.5, 0.8, and 1.2 are considered small, medium, large, and very large.
33
Post-hoc analysis examined the effect of the following variables on the change in each outcome. Measured at pre-test: severity of ADHD symptoms (ADHD RS-SRV cut-off of 37); ADHD medication use; comorbidities (anxiety, depression, bi-polar, and/or PTSD); concurrent therapy; and concurrent use of other supports. Measured at post-test: working alliance and duration of the 12-session coaching engagement (days). For analysis, we included these variables in an ANCOVA model and applied the type IV t-test in the regression tables.
34
These tests are likelihood ratio tests (not AIC) comparing the full model to the model without the specific regression variable. Statistical significance was set at P < 0.05. These variables were not included in the main analysis in this study but, as relevant, could be included in a more complex model in future research. As a separate post-hoc analysis to explore coach effect, the intraclass correlation coefficients (ICCs) were calculated by decomposing client-to-client variation into coach-to-coach variation and client-nested-within-coach variation, with the coach-to-coach variation serving as the ICC numerator.
Findings
Client Enrollment
As illustrated in Figure 1, a total of 68 clients were enrolled in the study and completed the pre-coaching data collection; oversampling was purposeful due to an early attrition rate of 33%. Four of these clients did not meet inclusion criteria, and four dropped out before starting coaching. Forty-five clients meeting inclusion criteria completed the 12-session coaching engagement; only 43 of these completed the post-coaching data collection. Client Participant Flow Chart.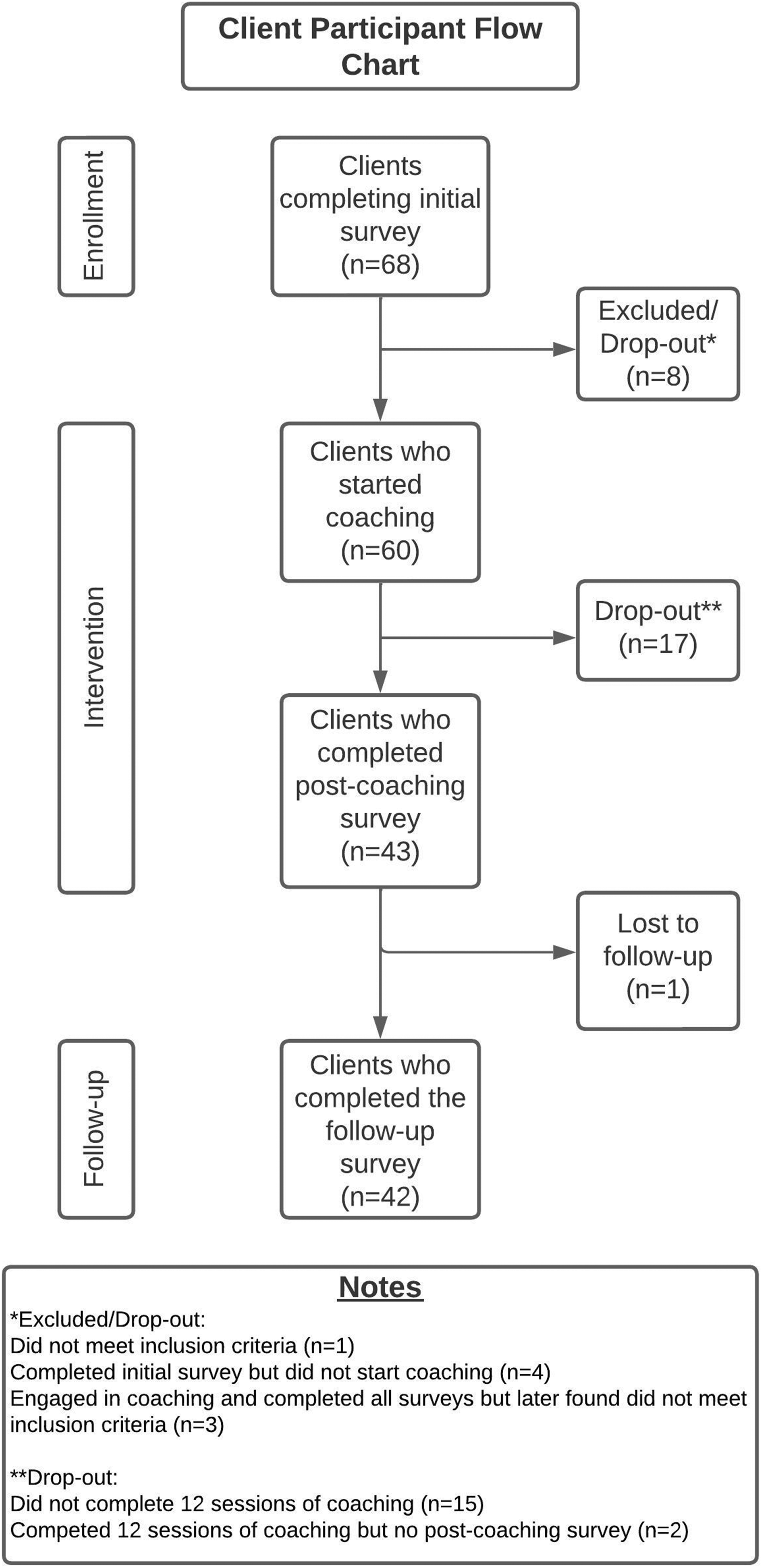
Descriptive Findings
Coach Characteristics.
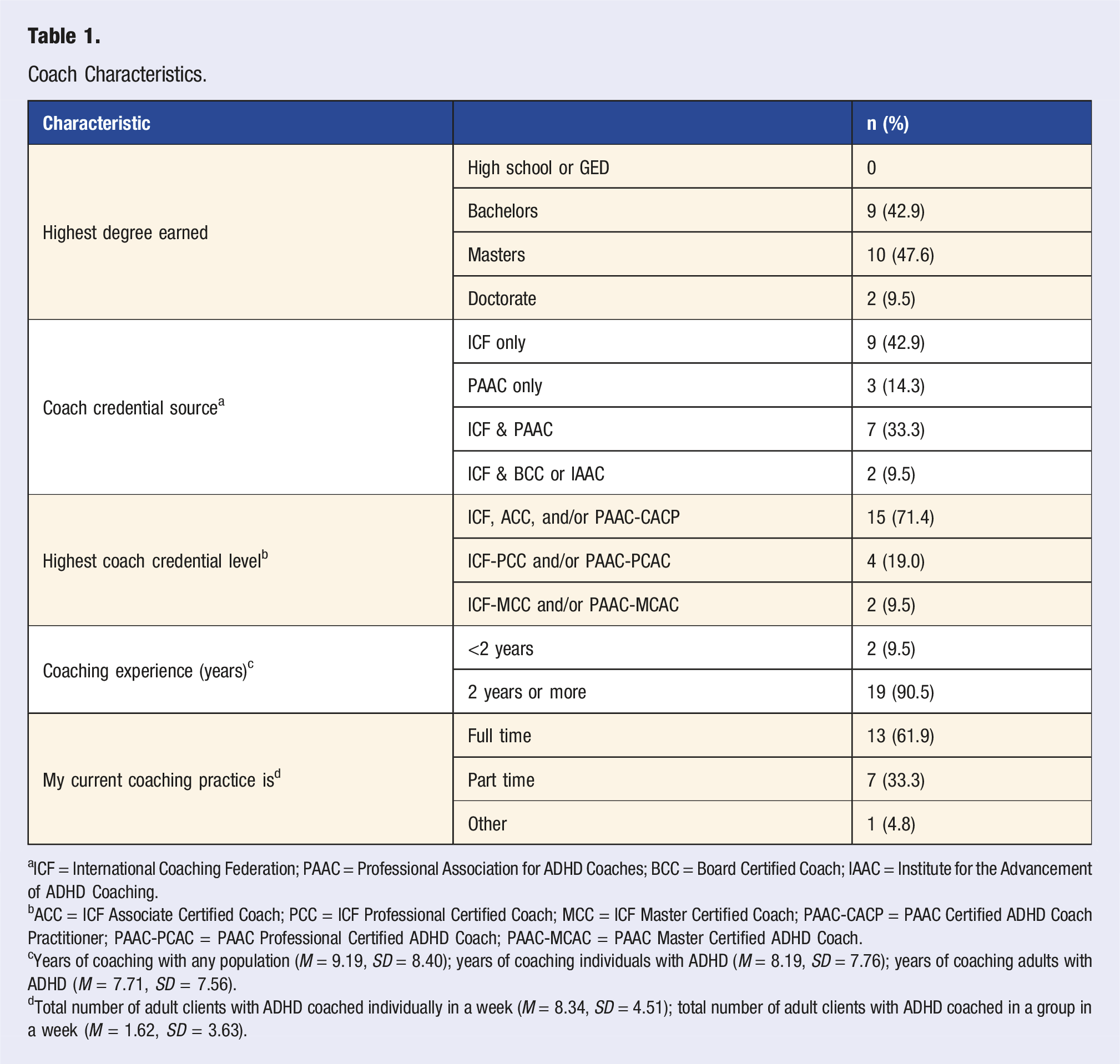
aICF = International Coaching Federation; PAAC = Professional Association for ADHD Coaches; BCC = Board Certified Coach; IAAC = Institute for the Advancement of ADHD Coaching.
bACC = ICF Associate Certified Coach; PCC = ICF Professional Certified Coach; MCC = ICF Master Certified Coach; PAAC-CACP = PAAC Certified ADHD Coach Practitioner; PAAC-PCAC = PAAC Professional Certified ADHD Coach; PAAC-MCAC = PAAC Master Certified ADHD Coach.
cYears of coaching with any population (M = 9.19, SD = 8.40); years of coaching individuals with ADHD (M = 8.19, SD = 7.76); years of coaching adults with ADHD (M = 7.71, SD = 7.56).
dTotal number of adult clients with ADHD coached individually in a week (M = 8.34, SD = 4.51); total number of adult clients with ADHD coached in a group in a week (M = 1.62, SD = 3.63).
Client Demographic Characteristics.
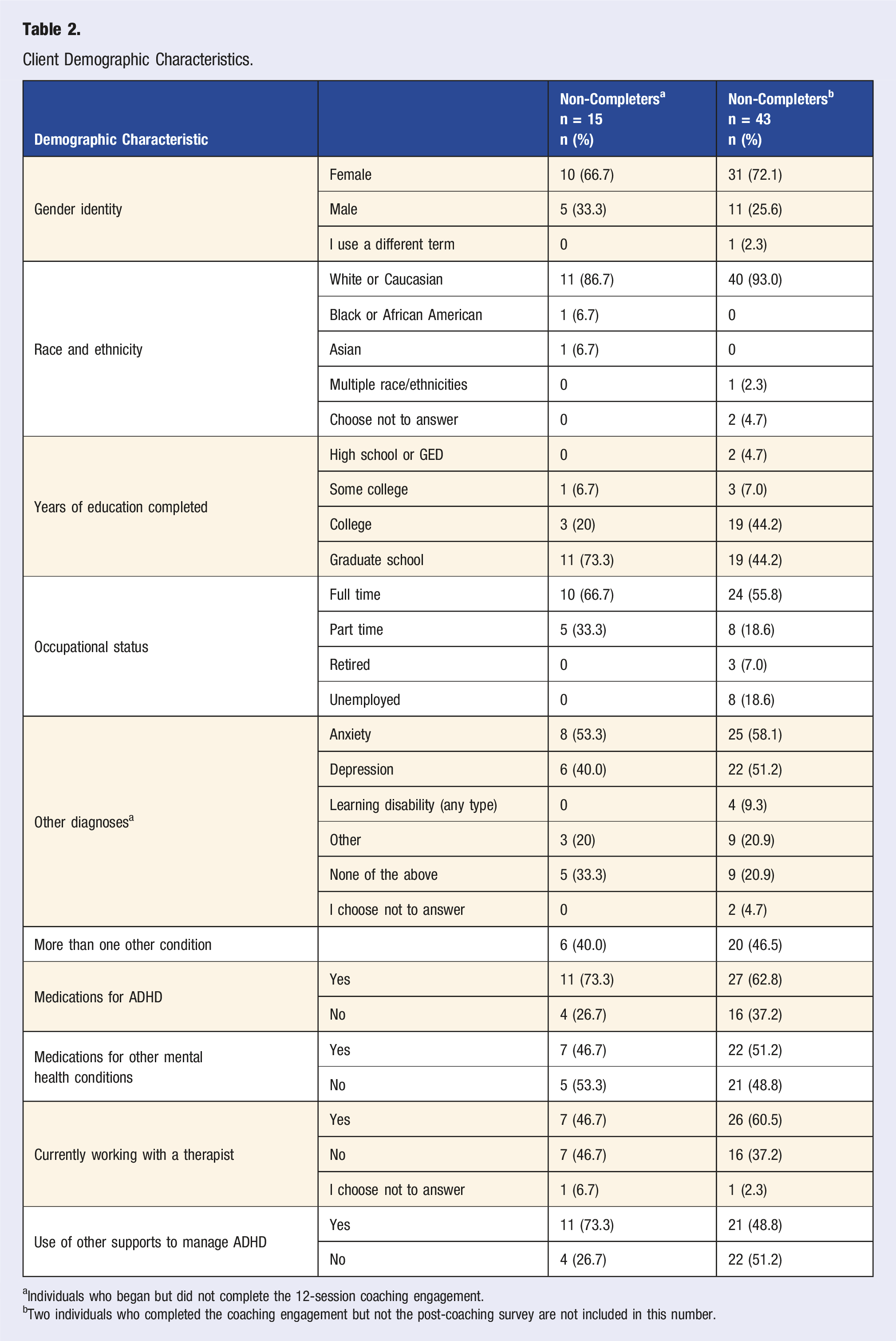
aIndividuals who began but did not complete the 12-session coaching engagement.
bTwo individuals who completed the coaching engagement but not the post-coaching survey are not included in this number.
As illustrated in Table 2, while there was a different distribution in the percentages of completers and non-completers who went to college and graduate school, the absolute difference between those having and not having any higher education was under 5%. The completers and non-completers had absolute differences in the 5-10% range for several demographic characteristics: gender, race, and having more than one comorbidity. There was also a 5-10% difference in the number of completers and non-completers retired, and a 10% or higher absolute difference both in full time and in part time status and, correspondingly, unemployed status. There was a 10% or higher absolute difference for: the presence of any vs no comorbidity, and both use of medication for ADHD and concurrent use of a therapist. There was an absolute difference of over 20% in the use of other supports (undefined).
The mean age (SD) of the 43 clients completing the coaching engagement and post-coaching survey was 43.53 (12.08) years. Additional client demographic data is provided in Table 2. Of note, from pre- to post-coaching, there was no significant difference in the number of “completer” participants taking any medication, whether for ADHD or other mental health conditions.
The coaching engagement consisted of 12 sessions in all cases and, on average, lasted 4-4.5 months. However, the duration of the 12-session engagement varied from 70-248 days (10-35.4 weeks); the mean (SD) was 124.2 (42.9) days; and the median [IQR] was 112 [97,139 days].
Fidelity
The median fidelity percentages for the initial, ten ongoing, and the closing sessions were 90.7%, 86.0%, and 95.3%, respectively. The average across 12 sessions was 87.2%.
Coach Effects and Working Alliance
Coach effect contributed to the best-fit AIC model for all outcome variables, indicating that variation among coaches affected all outcomes. This was controlled for in the analysis. Post-hoc exploration indicated that 34%–68% of the client-to-client variation in post–pre change scores was explained by coach effect, consistent with the relational nature of coaching interventions.
In this study, the working alliance scores (WAI, potential score range 12-60) had a median of 54, mean of 51, and range of 17.9 to 60. Although there are no established cut-off scores for low, medium, or high alliance on this measure, the median and mean scores of 54 and 51 out of a maximum score of 60 suggest a generally high level of working alliance.
Exploratory Findings
At the post-coaching data collection, on a scale of 0-10, mean (SD) client satisfaction with progress on coaching goals was 8.02 (2.07). Using a scale of 0-100, the mean (SD) percent success clients had in reaching their coaching goals was 70.02% (26.30).
The following number (%) of participants either agreed or strongly agreed with the following statements: I have a better understanding of how ADHD affects my life (39 [90.7]) I am more aware of my own thinking and behavior patterns (40 [93.0]) I am better able to manage negative self-talk (34 [79.1]) When I am stuck, I imagine the questions my coach would ask me (28 [65.1])
Hypothesis Testing
Hypothesis Testing: Statistical Significance and Effect Size.
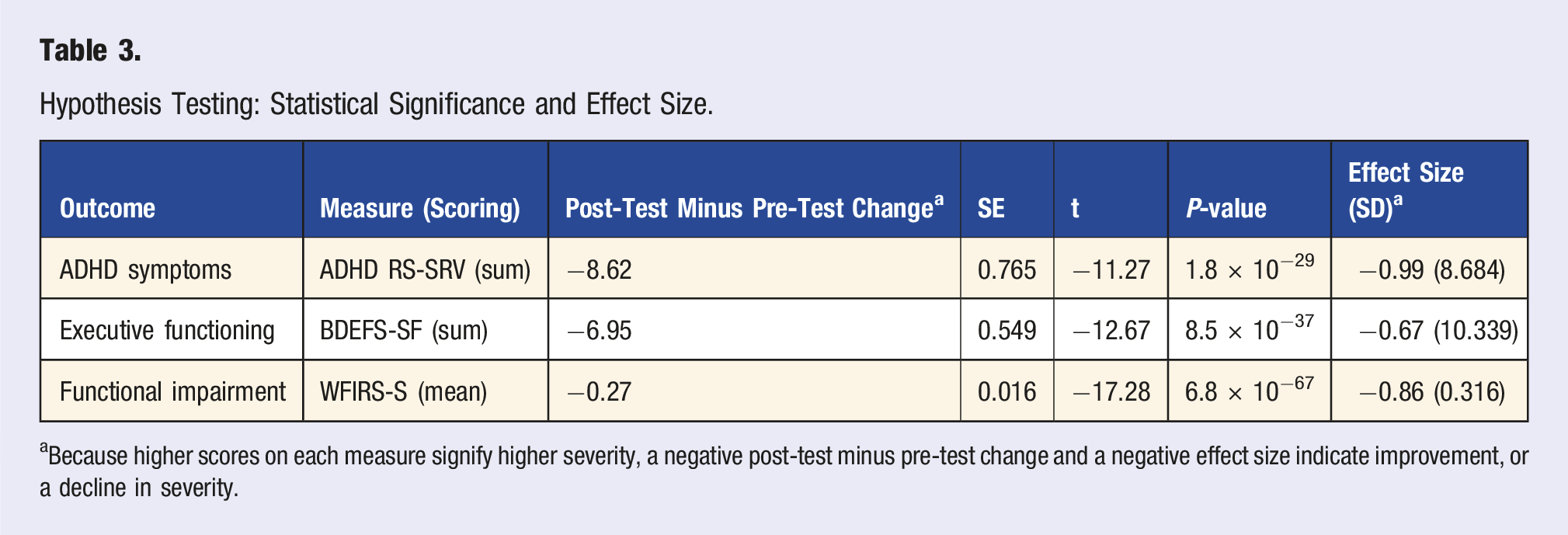
aBecause higher scores on each measure signify higher severity, a negative post-test minus pre-test change and a negative effect size indicate improvement, or a decline in severity.
Post-hoc Analysis
Post-hoc Analysis: Significant Findings.
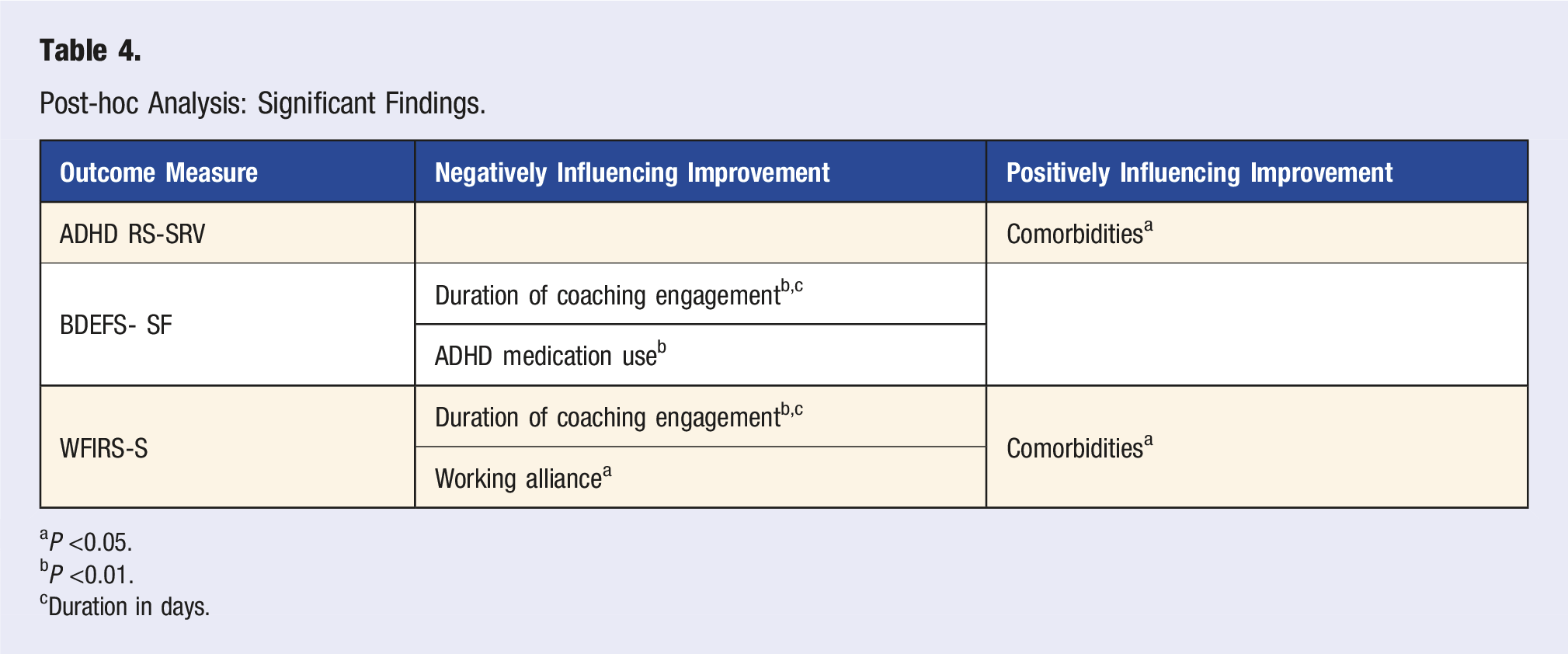
aP <0.05.
bP <0.01.
cDuration in days.
Discussion
This prospective study examined adult client outcomes related to a 12-session ADHD coaching engagement, finding high satisfaction and success with goal attainment as well as statistically significant improvements in ADHD symptoms, executive functioning, and functional impairment, with medium to large effect sizes. This is the fourth study to investigate outcomes of ADHD coaching for adults, the second to explore outcomes of individual coaching for adults with ADHD (one was more narrowly focused EF coaching), and the only one to examine these three specific outcomes. This discussion reviews aspects of the study design, the study outcomes, and potential confounding variables, as well as implications for research and practice. Strengths and limitations of this study are integrated into the discussion of study findings below.
Study Design
Attrition
Sixty clients who met eligibility criteria began this study, and 45 completed the 12-session coaching engagement, for a coaching retention rate of 75%. This is comparable to the 75.6% of participants who completed at least 7 of 12 sessions of CBT and CBT with medication for ADHD in the Pan et al 2019 study. 35 We are unsure whether this rate is common for ADHD coaching, but, in their study of ADHD coaching for college students, Field et al observed a higher attrition rate (only 35% of participants completed 90% or more of the planned sessions). In comparison, our attrition rate is quite low. 36
Two of the 45 clients who completed the coaching did not complete the post-coaching survey, leaving 43 clients who completed coaching for the analysis. Baseline characteristics were generally comparable between the 43 participants who completed our study and the 15 who began but did not complete the 12-sessions of coaching. Several variables exhibited modest absolute differences, in the range of 5-10%, typically considered small, especially with the low number of non-completers, and unlikely to have meaningfully influenced study findings. However, a limited number of characteristics demonstrated differences greater than 10%, suggesting potential baseline imbalance between completers and non-completers. These characteristics were: employment status, presence of co-occurring conditions, use of medication for ADHD, concurrent use of therapy, and concurrent use of other (non-therapy) supports. Differences between completers and non-completers across these characteristics may reflect differential attrition that must be considered when interpreting the results. These characteristics may also be important to examine more fully in future research.
We did not collect data on reasons clients chose not to complete a coaching engagement. Unsolicited anecdotal reports from some coaches in the present study indicated that clients discontinued coaching due to major life transitions, health issues, or financial concerns. In care for individuals with ADHD, maintaining client engagement, and consequently retention, is a documented challenge. 37 Future studies could monitor attrition and collect data on why clients discontinue coaching. This might help identify factors predictive of not only attrition but also lack of benefit or, alternatively, coaching success.
Design
The single-arm pre-post study design is used commonly in evaluation and when studying a new topic, such as in the present study.
38
Single-arm prospective studies offer stronger evidence than cohort studies, which compare groups who are naturally exposed and not exposed to a condition, often used to explore risk factors and incidence.
39
Single-arm prospective studies also offer a practical balance between “ideal” methodology (e.g., an RCT or perhaps pragmatic trial) and both recruitment and financial feasibility. Additionally, according to Wang, et al
39
: Single-arm trials have certain ethical advantages over randomised controlled trials, such as providing equitable treatment, [and] respecting patient preferences…. While single-arm trials do not adhere to the principles of randomisation and blinding in terms of scientific rigour, they still incorporate principles of control, balance and replication, making the design scientifically reasonable.39(p1)
However, because this design is not as rigorous as a randomized controlled trial (RCT)—due, for example, to the lack of a control group, greater potential for confounding, and higher risk of bias related to placebo or time effects—the single-arm pre-post trial can be more difficult to interpret and is not generally considered as robust a source of causal evidence. Wang et al suggest that this study design is typically only used for evidence when sample sizes are adequate and either historical controls are carefully chosen (not used in this study) or the effect size is clinically significant. 39 In this study we found medium to large effect sizes.
To our knowledge, only three RCTs of ADHD coaching have been published to date, and none focus on coaching for adults.36,40,41 By comparison, there are numerous RCTs, and even some meta-analyses, exploring cognitive behavioral therapy for adult ADHD. Clearly more research is needed on coaching for adults with ADHD. Given the encouraging findings of the current study, we recommend that funding for future research on ADHD coaching for adults both emphasizes the importance of, and provides support for, conducting RCTs.
An interesting strength of this study is its similarity to a pragmatic trial, “designed to evaluate the effectiveness of interventions in real-life routine practice conditions”42(p217) with “participants… similar to [clients] who would receive the intervention if it became usual care.”43(p455) Although the use of inclusion/exclusion criteria and a manualized intervention, and the lack of a control group, differ from a typical pragmatic trial, recruiting clients through coaches’ actual practices, and using manualized guidelines endorsed by coach participants as essentially the same as their usual coaching approaches, allow this study to provide a view of “real-life” coaching for typical clients.
Self-Report Measures
While employing widely used, reliable and valid instruments to measure outcomes, this study relied on client self-report measures. Varied, more “objective” measures have been used in certain other studies of ADHD coaching, including neuropsychological tests, 11 perspectives of spouses/partners, 10 and grades, or GPA,44-46 for example. Clinician or life partner ratings might have added a different perspective to the outcomes measured in this study, and some research suggests the benefits of more than one perspective in assessment of ADHD and related impairment. 37 Still, we contend that, ultimately, the client’s perception of outcomes, based on their lived experience, is the most meaningful assessment of outcomes. 47
Forced-answer questions, used in two surveys in this study have the advantages of eliminating missing data, and enabling scale summation. Research on this method has shown mixed results regarding potential bias when respondents are not given a “not-applicable” choice.48-50 However, this bias is most concerning when questions are very sensitive 49 or when respondents lack enough categories to make a choice, 51 not conditions that applied in this study. Response fatigue is another possible source of bias, 51 which we avoided by timing survey completion as part of designing the study. Future studies of individuals with attentional issues should keep this consideration in mind.
Study Intervention
Number of Sessions and Duration of Coaching Engagement
Twelve sessions was selected as the number for the ADHD coaching engagement in this study for several reasons: (1) it is anecdotally a common length for an initial coaching engagement; (2) a key health and wellness coaching text suggests that 12 sessions is generally considered the minimum amount of time necessary for coaching to bring about effective health behavioral change 52 ; and (3) across six prior ADHD coaching studies for college students, all reporting improvements in executive functioning, 12 was the mean number of weekly sessions. 8 Of note, cognitive behavioral therapy for ADHD has also typically been a 12-session program, though reported approaches vary from 6-30 sessions. 53
Also of note is the wide range in duration of the 12-session engagement in this study (10 - 35.4 weeks). It appears that the variation in duration for the 12-session coaching engagement occurred because several clients took long gaps at one or more points during the engagement. However, we did not collect systematic data on reasons for the gaps. Post-hoc analysis indicated that a longer duration of the coaching engagement (days) may have negatively influenced outcomes on the BDEFS-SF and WFIRS-S. Gaps in coaching might make sense in this regard. A nationwide survey of ADHD coaches reported that, in most instances, coaching sessions were held weekly, and the median duration of an engagement was 6 months (range 1-75). 54 Future research might both collect data on reasons for gaps in a coaching engagement and explore frequency and duration as potential modifiers of coaching outcomes.
Two reviews of executive and workplace coaching suggest that neither the number of coaching sessions nor the duration of an engagement are key factors in effectiveness.55,56 Similarly, a rapid systematic review of health and wellness coaching studies found that varied numbers of sessions, and varied durations of a coaching engagement, all led to sustained improvements. 57 Notably, the studies reviewed differed widely in design and also in both the focus of coaching (e.g., diagnosis) and study outcomes.
Perhaps more relevant information about the impact of the number of ADHD coaching sessions on outcomes can be gleaned from the Evans et al study of coaching for high school students with ADHD. 40 In this study, a dosage-analysis found that the number of sessions did affect outcomes, with more sessions having a greater effect on family and academic impairment than on ADHD symptoms. Future research examining coaching “dosage” in relation to different outcomes would be helpful. Such research should investigate the impact of the number of sessions and the duration of a coaching engagement using a consistent coaching approach and uniform outcome measures.
Fidelity
Consistency is important in researching any intervention. In this study, session checklists were used to measure fidelity to the manualized intervention for the coaching engagement, a widely accepted approach 58 ; and fidelity exceeded 87%. Typically, fidelity over 80% is considered high.31,58 In fact, a review of health behavior change literature found that only 15.5% of psychosocial interventions achieved at least 80% fidelity. 59 Fidelity assessment is rare in the coaching literature, making both fidelity assessment and the high fidelity scores noteworthy in this study. Future coaching research using multiple coaches should incorporate fidelity assessment to ensure consistency in the study’s coaching intervention.
Study Outcomes
Epstein and Weiss have argued that it is important to assess a variety of outcomes when studying interventions for individuals with ADHD. 60 In this study we examined goal attainment, ADHD symptoms, executive functioning, and functional outcomes.
Goal Attainment and Exploratory Outcomes
Grant has described goal setting as a key aspect of coaching, as well as one feature distinguishing coaching from therapy.61,62 Some earlier research on ADHD coaching examined how coaching influences goal management and attainment among college students.46,63 Most participants in the present study reported both success in achieving their goals during the coaching engagement and high satisfaction with their progress.
In ADHD coaching, goal pursuit serves as a focus that may lead to, or be accompanied by, exploration of executive functioning, self-awareness, and even aspects of identity.13,14 In this study, participants endorsed outcomes such as: better management of negative self-talk, increased awareness of their own thinking and behavior patterns, and a deeper understanding of how ADHD impacts their lives. A qualitative component of this mixed-methods study, reported elsewhere, 24 along with other qualitative studies of ADHD coaching for adults,13,14 indicate that ADHD coaching clients value such outcomes.
Improvements in ADHD Symptoms
This study of ADHD coaching for adults demonstrated statistically significant improvements in participants’ ADHD symptoms from the pre- to the post-coaching period, measured by the ADHD RS-SRV. The large effect size (0.99) is higher than that found in a network meta-analysis of 113 studies for stimulants (effect sizes 0.39 - 0.71) and atomoxetine (0.38 - 0.51) at 12 weeks, and more robust than the small to medium (0.12 - 0.76) effect sizes observed for CBT. 64 For CBT, this same network meta-analysis only found improvements greater than placebo when clinicians, not clients themselves, rated improvement. However, another meta-analysis focused on CBT for adults with ADHD, reported a medium pooled effect size, from 26 studies, of 0.63 for overall symptom improvement, most often using self-report scales. 65 Pan et al reported that both CBT and CBT plus medication led to significant improvement in ADHD symptoms, and a similar number of adults achieved remission in each group, but effect sizes were not reported. 35
The improvements in ADHD symptoms in our study align with findings from at least five prior studies of ADHD coaching reporting improvements in ADHD symptoms, measured in various ways, for both young people40,66,67 and adults.10,12 As the third study of ADHD coaching for adults demonstrating symptom improvement, this study reinforces and extends prior findings.
Improvements in Executive Functioning
This study found statistically significant improvements from pre- to post-coaching in executive functioning, measured by total scores on the BDEFS-SF. The medium effect size of 0.67 compares favorably with results observed for the effects of medication, CBT, and a combination, on select components of executive functioning. An effect size of 0.64 has been reported for improved executive functioning with CBT in college students, 68 and reported effect sizes range from 0.36 - 0.64 for stimulant and non-stimulant use in adults. 69 Pan et al found that both CBT and CBT plus medication led to statistically significant improvements in global executive functioning, with the combined treatment having a positive impact on more aspects of executive functioning than CBT alone; effect sizes were not reported. 35
Our study’s findings confirm and extend the results of prior research on ADHD coaching and executive functioning. Eight studies of ADHD coaching for college students previously demonstrated improvement in EF skills,36,46,70-75 and two additional studies provided qualitative reports of improved EF 76 or goal attainment 63 among youth. Additionally, Ebrahimi et al found pre- to post-coaching improvements in select neuropsychological tests related to executive functioning among adults. 11 These findings support consideration of coaching as a valuable tool in managing executive functioning challenges for adults with ADHD.
Improvements in Functional Impairment
Some research now considers ADHD within an epidemiological framework, as a condition with significant adverse impacts on “nearly every major domain of life activity.”77-79 In fact, Weiss et al suggest that “ultimately, it is the magnitude of improved functioning that is predictive of long-term beneficial outcomes” of an intervention.80(p155)
The pre- to post-coaching improvement in functional impairment observed in this study, measured using the WFIRS-S, was statistically significant with a large effect size (0.86). This compares favorably with findings of a 2017 systematic review in which Coghill et al reported that medication had a “statistically or nominally” significant effect on functional impairment, measured with generic, not ADHD-specific measures, in nine of ten studies, but with effect sizes above 0.5 (in at least one domain of an instrument) in only one study. 81 More recently, Kosheleff et al reported that pharmacological treatment showed benefit for a wide range of functional impairments in adults with ADHD. 2 Our findings also compare favorably with outcomes on the WFIRS-P parent rating scale in studies of medication use among children (effect sizes 0.77 - 0.92). 82 Less has been reported regarding CBT and functional impairment in adults, but our findings compare favorably with cognitive and/or behavioral intervention outcomes on impairment in adolescents, identified in a systematic literature review (effect sizes 0.48 - 1.27). 83
Other studies of ADHD coaching have reported positive outcomes in various aspects of client functioning. For young people, this has included social behaviors40,45,84,85 and grades or academic impairment.40,44-46,86 Among adults, Bloeman et al found that participant scores on the WFIRS improved from before to after a coaching engagement. 10 The present study also used the WFIRS-S and is only the second study of ADHD coaching to examine functional impairment in adults. The finding of improvement from pre- to post-coaching offers important insight into the type of support coaching can offer to adults with ADHD.
Quality of Life
Life satisfaction and quality of life can be impaired for adults with ADHD, especially for those diagnosed in adulthood or who are untreated.87,88 Several previous quantitative and qualitative studies of ADHD coaching found benefits for quality of life,67,76 positive expectations in life, 63 or well-being. 36 However, these did not focus on adults. Although quality of life was not directly measured in this study, improvements in ADHD symptoms, executive functioning, and functional impairment found in this and other studies of ADHD coaching, have all been associated with improvements in quality of life.81,87,89,90
To date, no research on ADHD coaching for adults has directly measured quality of life as an outcome. However, a mixed-methods study of ADAPT, a coaching-like intervention for adults with ADHD, found that ADHD-related quality of life—but not health-related quality of life—was the variable most sensitive to the intervention. 91 Additionally, the Sanders-Williams 14 and Schrevel et al 13 qualitative studies of coaching for adults with ADHD both described benefits that could suggest improved quality of life. Quality of life is an important outcome to explore directly in future research on ADHD coaching for adults.
Potential Confounders
Research on coaching in different settings suggests the importance of beginning to look at moderators and mediators of outcomes. 92 For this reason, we conducted AIC exploration and post-hoc testing to examine the potential impact of a number of variables on study results. The number of coaching sessions and duration of the coaching engagement are potential confounders we discussed earlier. Coach effect, working alliance, concurrent use of medication or therapy, and various client factors are addressed below.
Coach Effect and Working Alliance
Although research suggests it may contribute to between 0.2 and 10% of variance in outcomes,20,93 coach effect has not been accounted for in the ADHD coaching literature to date. Existing work on coach effects tends to emphasize coach behaviors and relational processes as predictors of outcomes.94-96
To reduce variability in coach behavior, we used a manualized intervention, with high fidelity, and selected coaches who met minimum thresholds for training, credentialing, and experience. Thus, coaches were relatively homogeneous on these key professional characteristics, limiting scope for these variables to explain outcome differences. Nonetheless, in this study, coach effect contributed to the best-fit models and was controlled in subsequent analyses. Post-hoc exploration indicated that 34%–68% of the client-to-client variation in post–pre change scores was explained by coach effect, consistent with the relational nature of coaching. We suggest it as an important variable to explore in future studies. Future research might also further explore the impact of specific coach characteristics on client outcomes.
Research also suggests both therapy and coaching outcomes can be influenced by the therapeutic alliance.19,97 The working alliance was strong in this study, did not contribute to the best-fit (AIC) models for analysis, and, in the post-hoc analysis, was only a significant variable with respect to outcomes on the WFIRS-S, and not the ADHD RS-SRV or the BDEFS-SF. Still, because of its potential effect, working alliance may be useful to explore further in future research.
Medication
Medication is considered the “first-line” treatment for ADHD, and for many individuals, when used, it can improve symptoms. It can also positively impact executive functioning and functional impairment, although its impact on functional impairment for adults has been less often explored.2,60,64,69,81,98 The number of participants in this study using medication—for either ADHD or for other mental health conditions—did not change significantly from pre- to post-coaching. Based on the post-hoc testing, the use of ADHD medication at the onset of coaching may have influenced outcomes measured by the BDEFS-SF, although not the ADHD RS-SRV or the WFIRS-S. Because of the importance of medication in the management of ADHD, future research might both compare effects of coaching with that of medication and also explore the combined effects of coaching and medication on key outcomes.
Therapy
CBT is the most widely studied approach to therapy for adults with ADHD. Studies have demonstrated a beneficial impact of CBT on ADHD symptoms, executive functioning, and functional impairment, although functional impairment as an outcome of CBT in adults has been explored less often.35,60,64,65,68 In the present study, 60.5% of clients were concurrently working with a coach and therapist, but post-hoc analysis showed no effect of concurrent therapy—or the concurrent use of other supports—on any of the study outcomes explored. In a study of group coaching for adults with ADHD, Kubik found that coaching alone had a broader impact on ADHD symptoms than coaching plus therapy. 12 Nonetheless, future exploration comparing outcomes of coaching and therapy, and/or examining their concurrent use, would be valuable.
Client Factors
McKenna and Davis suggest that client factors may account for up to 40% of the variance in therapeutic outcomes 99 ; one could assume that the same might also be true in coaching. In a study of the impact of long-acting amphetamine treatment for ADHD on symptoms and quality of life, factors such as age, gender, ADHD severity, and treatment-naive status moderated improvements in symptoms. 90 In the present study, all clients were naive to coaching; the mean (SD) age of clients was 43.53 (12.08); and 72.1% of participants identified as female. However, we did not examine the effect of age or gender on outcomes. These variables could be explored in future research.
ADHD severity and comorbidities are additional factors to consider. In a study on amphetamines as treatment, Weiss et al found that ADHD severity moderated improvements in symptoms. 90 In our study, the post-hoc analysis indicates that ADHD severity, measured before coaching, did not affect any of the three study outcomes. Also, although results were not definitive, Kininger’s thesis suggested that anxiety might moderate the effects of ADHD coaching on college students, with subjects having lower levels of anxiety potentially benefitting more from coaching. 41 In our study, the post-hoc analysis identified the opposite effect. Comorbidities had a positive effect on improvements for both the ADHD RS-SRV and the WFIRS-S, although no effect was observed for the BDEFS-SF. Both severity and the presence of comorbidities are client factors that may be important to examine or control for in future research. Exploring these and other client characteristics that might contribute to completing a coaching engagement, minimizing gaps between sessions, and/or predicting outcomes, would be a useful and interesting focus for a future study.
Implications for Research and Practice
The Broader Coaching Literature
The effectiveness of ADHD coaching, now demonstrated in over 20 varied studies, including four of adults, can be compared to that of health and wellness coaching (HWC), which has a much broader research base. As of 2023, a compendia and two addenda, have examined HWC outcomes in over 450 studies,16-18 finding coaching to be a “promising intervention for chronic diseases”16(p436) and “a favorable intervention with treatment potential in all [disease] categories.”17(p155) Authors of the 2023 addendum to the compendium suggests that the “evidence base underscores HWC’s utility as a key intervention for chronic disease management, preventive care, and whole-person health.”18(p1) In this context, the positive outcomes of this study of ADHD coaching receive additional support.
Lack of Diversity
All the clients in our study pursued coaching independently. Most participants were women, White/Caucasian, with an average age of 43.5 years, and had completed college or graduate school. In a nationwide survey of ADHD coaches, with 481 respondents, Sibley et al reported similar client demographics, though gender and age were not reported. 54 Based on the participant demographics, we think our sample may be fairly representative of the population typically using ADHD coaching services at this point. We cannot generalize about how coaching might affect a more diverse group of adults with ADHD. More research involving a diverse client demographic would be valuable.
Costs of Coaching
Insurance does not cover the costs of ADHD coaching. This study also did not cover these costs. As we were recruiting clients from coaches’ private practices, coaches set their own fees. We did not collect data on coaching fees, but a nationwide survey of ADHD coaches (n = 481) reported that 90-100% of coaching clients pay out of pocket, and the median session fee is $150 (range $0 - $750). 54 These fees are certainly out of reach for many who might benefit from ADHD coaching. Since we did not collect data on costs, we can only assume that the costs of coaching may have affected the diversity of clients recruited for this study.
In the Field et al study, ADHD coaching for college students was provided at no cost. 36 Of the 121 students referred for coaching, only 88 (72%) completed the application, intake, and at least one session. Additionally, of the 88 students beginning the coaching, only 35% completed 90% or more of the planned sessions (an attrition rate of 65%). Clearly cost was not the only factor affecting recruitment or attrition. In our study the coaching attrition rate over 12 sessions was only 25%. Several coaches told us, anecdotally, that some clients discontinued coaching due to major life transitions, health issues, or financial concerns. We cannot surmise to what extent costs of coaching may have been a factor in attrition. We do note that those completing the study included a number of clients who were unemployed while the non-completers were all employed full or part-time.
As efforts are currently underway to establish CPT codes for billing for health and wellness coaching—which will likely make this form of coaching more affordable to consumers 100 —consideration of eventual insurance coverage for ADHD coaching might be one way to make this supportive service more widely accessible.
Credentialed, Specialized Coaches
Coaching is not a licensed profession. However, all of the coaches participating in this study were trained, experienced, credentialed coaches. They had a minimum of 60 hours of coach training with at least 35 hours of specific training in coaching individuals with ADHD and were also oriented to a manualized approach to the study's 12-session coaching engagement. A credential (e.g., through International Coaching Federation and/or the Professional Association of ADHD Coaching) indicates that a coach has both received specific training in, and has demonstrated, coaching skills and competencies. Use of manualized intervention guidelines, with high fidelity, assured consistency across coaches in the 12 sessions of the coaching engagement. These two factors are strengths of this study.
A mixed-methods study of CBT reported that participants with ADHD found that “generic” CBT, not adapted to ADHD, was “unhelpful, overwhelming, and at times harmful to their mental well-being.”101(p10) Both Knouse and Ramsay 102 and Ramsay 103 recommend that CBT must be adapted for adults with ADHD and delivered by individuals who are properly trained and use an ADHD lens. We argue the same for ADHD coaching.
For this reason, the findings of this study cannot be extended to coaches who lack credentialing, or training specific to ADHD, as it is not possible to determine what they actually offer as “coaching” or whether they employ an ADHD-specific lens. Consequently, individuals with ADHD seeking coaching should generally be encouraged to look for coaches with a credential from the Professional Association for ADHD Coaches (PAAC) or the International Association of ADHD Coaches (IAAC), which ensures ADHD training, or, alternatively, coaches holding a Board Certified Coach (BCC), International Coaching Federation (ICF), or National Board Certified Health and Wellness Coach (NBC-HWC) credential, along with specific training and experience in coaching individuals with ADHD.
Coaching Practice
According to the International Coaching Federation, coaching can be defined as “partnering with clients in a thought-provoking and creative process that inspires them to maximize their personal and professional potential.”104(p11) Wright describes ADHD coaching, specifically, as: “a seamless blend of three elements employed by the coach as needed.”105(pp22-23) These elements are: Life coaching Psychoeducation related to ADHD Assisting a client to develop individualized external systems and strategies that shore up executive functioning skills
The strength of this study’s findings—across outcomes including goal achievement, ADHD symptoms, executive functioning, and functional impairment—suggests the value of coaching as a support service for adults with ADHD. Additionally, the findings bolster existing literature on ADHD coaching, supporting it as an evidence-based practice. In this way, the present study can enhance coaches’ confidence in the value of their contributions, as well the confidence potential clients, and any referring professionals, might have about this service.
Multimodal Care
Multimodal care has increasingly been recognized as optimal for ADHD treatment. 4 Coaching is one of a number of potential supports adults with ADHD can use in a multimodal approach, along with medication and therapy, typically CBT.
While research has explored combined effects of CBT and pharmacologic treatments,35,60,106 little research has explored coaching in conjunction with other supportive approaches—such as medication and/or CBT. Kubik reported that clients perceive a combination of coaching with medication and therapy as the most effective treatment. 12 However, in that study, coaching alone had a statistically significant benefit in five areas of concern while coaching plus therapy was only effective in two. Post-hoc analysis in our study did not indicate that either concurrent use of therapy, or use of medication, influenced the improvements observed in either ADHD symptoms or functional impairment. However, medication use, but not therapy, appeared to adversely impact improvements in executive functioning.
Dobrosavljevic et al suggest that more research is needed to identify optimal treatment approaches for adults with ADHD. 107 Certainly the potential interaction of therapy, medication, and coaching, for a fulsome approach to multimodal care, deserves further research attention. Attention to interprofessional communication may also be important.15,108
Conclusions
ADHD coaching has been a growing field since the 1990s, focused on support for individuals with ADHD across the lifespan. At present, ADHD coaching is understood to be: distinct from treatment modalities109-111; complementary to other approaches9,66,112,113; and uniquely valued by adults with ADHD.13,14 Additionally, numerous studies have identified benefits of ADHD coaching, and it is increasingly regarded as a useful component of multimodal care for adults with ADHD.114-117
Matheson et al suggest that unmet needs of adults with ADHD for supportive services may be “substantial.”118(p184) Cortese et al call out “a critical need for high-quality research on publicly available non-pharmacological interventions for ADHD in adults.”37(p362) Two prior studies explored group coaching for adults with ADHD, and one prior study focused narrowly on executive function coaching, all finding positive outcomes.10-12 This study is the first to investigate individual ADHD coaching for adults.
Twelve sessions of ADHD coaching were provided by experienced, credentialed coaches trained to work with individuals having ADHD. Using widely accepted, valid self-report measures, statistically significant improvements in ADHD symptoms, executive functioning, and functional impairment were documented with medium to large effect sizes. These effect sizes are comparable to, and in some cases larger than, those seen in studies of the effects of pharmaceutical treatments and CBT on similar outcomes. The results are also in line with findings from studies of ADHD coaching in other age groups. Because of the study’s single-arm pre-post study design, RCTs or pragmatic trials will be important to substantiate these findings.
Further research will also be helpful to explore for whom, at what dosage, and under what conditions, ADHD coaching is most effective, as well as to investigate coaching in combination with other supportive interventions. Nonetheless, this study offers a unique contribution to the literature on ADHD coaching—and the literature on multimodal support—for individuals with ADHD. It adds to a growing body of research demonstrating that ADHD coaching has a meaningful role to play as an effective support service, providing significant value to adults with ADHD, and across the age span, both offered on its own and as a part of multimodal care.
Footnotes
Acknowledgments
Members of the Faculty Research Group at Maryland University of Integrative Health provided both encouragement and a wealth of ideas to help boost coach recruitment. The Health and Wellness Coaching Department at Maryland University of Integrative Health provided funding for the earlier development of the manualized intervention used in this study. Daryl Nault, MS provided statistical assistance.
Ethical Approval
This study was approved by the Institutional Review Board at Maryland University of Integrative Health [05.AHM.04.22.2; approved, April 29, 2022]. Informed consent was obtained online, prior to survey access.
Funding
This investigation was supported by the IOC-ICF coaching research grant program, which is led by the Institute of Coaching and funded by the International Coaching Federation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.