
Abstract
Doctor of Physical Therapy (DPT) students encounter substantial academic and psychological challenges, yet there is limited consensus on effective interventions. This 4-year longitudinal program evaluation describes the integration of lifestyle medicine into both curricular and co-curricular components of a DPT program, and examines associated changes in student wellness, psychological capital, and social network development. Guided by the Social Ecological Model, the programmatic assessment highlights the multifaceted influences on student wellness, extending responsibility beyond the individual to include faculty, institutional leaders, external partners, and policy makers. Outcome measures comprised the 5 Factor Wellness Inventory (FFWEL), Psychological Capital (PsyCap) Questionnaire, and Social Network Peer Connection analyses across 4 student cohorts. Results revealed increased peer network connections and cohesion over time, emphasizing the significance of social support and collaborative learning. Improvements in FFWEL and PsyCap scores further indicate progress in well-being. These findings demonstrate the effectiveness of intentional, multi-level strategies for collective well-being, and underscore the utility of the Social Ecological Model. The results presented offer a foundation for preparing graduates to promote lifestyle medicine in varied professional contexts.
Keywords
“The findings indicate that FFWEL scores consistently exceeded cohort norms, and PsyCap scores remained elevated throughout the study period.”
Introduction
Lifestyle-related diseases, including cardiovascular disease, diabetes, and obesity, constitute a significant and growing public health burden. 1 These conditions are largely driven by modifiable risk factors such as poor nutrition, risky behaviors, physical inactivity, inadequate sleep, and chronic stress. Within this context, physical therapists (PT) serve a pivotal role in promoting disease prevention and wellness. 2 By advocating for evidence-based pillars of lifestyle medicine, 3 PTs encourage healthy behaviors, design and implement exercise interventions, and provide patient education on wellness strategies. The effectiveness of PTs in these endeavors may be further enhanced when they themselves prioritize personal well-being and resilience, serving as exemplary role models and delivering higher quality care. 4
However, the journey to becoming a PT includes academic and psychological challenges that can impact health and wellness. 5 Students in health professions programs, including Doctor of Physical Therapy (DPT), encounter intense competition, demanding schedules, and rigorous study requirements that often result in elevated stress levels and compromised mental and physical health. 5 A systematic review 6 highlighted the lack of consensus regarding effective interventions for building student resilience, yet research indicates that psychological capital, (including the positive psychological constructs of hope, self-efficacy, resilience, and optimism) facilitate adaptive functioning. 7 Combined with social support mechanisms, these become vital resources for coping with adversity and maintaining well-being. 8 Despite this support, students report that peer connections and institutional resources, such as counseling services, are not always sufficient to meet their needs. 9 Additionally, studies have documented declines in physical fitness, exercise, and sleep quality among DPT students,4,10 with perceived stress negatively impacting academic performance. 11
The complex factors affecting student wellness and success highlight the need for integrated approaches in health professions education. Currently DPT curricula do not proactively include lifestyle medicine pillars—optimal nutrition, physical activity, restorative sleep, stress management, risky substance avoidance and connectedness—or strategies for both individuals and institutions.
To address these challenges, our project introduces an innovative, multifaceted approach that weaves lifestyle medicine principles throughout the DPT curriculum. Guided by the Social Ecological Model, 12 this initiative leverages interrelated strategies at the individual, cohort, program, and institutional levels, fostering a comprehensive culture of wellness. By aligning curricular content, co-curricular activities, and institutional policies, we aim to enhance student success and well-being.
Theoretical Grounding: Social Ecological Model Framework
We used the Social Ecological Model 12 as the foundation for this project to examine relationships across multiple levels of influence (individual, cohort, program, institution). This model illustrates that student wellness is not the sole responsibility of the individual, the faculty, nor academic program. Instead, it emphasizes the interconnected roles, including those of institutional facilitators, external partners, and state and federal policymakers. By recognizing these layered and interdependent factors, our project addresses the complex influences shaping student wellness.
The central research question guiding this study is: How does a comprehensive integrated lifestyle medicine program within a DPT curriculum influence student wellness outcomes over time, including measures of psychological capital and social network development?
Methods
Study Design
A longitudinal descriptive program evaluation study design was used to track outcomes over time based on multiple data sources and time points.
Participants
Physical therapy students in the DPT program at an R1 academic health science center in the Midwest were recruited for this study during a seminar course held in the first semester of the program. All students enrolled in the DPT program were eligible and invited to participate, and every participant provided informed consent. Participant confidentiality was ensured by issuing a unique identifier, separated from participant name.
Only students enrolled in the DPT Program from August 2019 to May 2025 (in the graduating classes of 2022, 2023, 2024 and 2025) were eligible for inclusion. The University of Nebraska Medical Center Institutional Review Board approved this project (583-19-EX).
The DPT program is an eight-semester (33 month) program that includes didactic courses, labs and clinical education covering biological, physical, behavioral and movement sciences necessary for entry-level practice. The student cohorts are distributed across 2 campuses, which are approximately 200 miles apart. Each academic year, 1 campus enrolls 50 students, while the other enrolls 16 students. Faculty members are physically present on both campuses during all experiential laboratory sessions to ensure hands-on instruction. Didactic components of the curriculum are delivered synchronously, with lectures that are streamed live from one campus to the other. During these sessions, students attend class in person at both the originating and remote sites, with faculty lecturing live from the originating campus.
To operationalize the Social Ecological Model within the DPT curriculum, a coordinated series of student support mechanisms and educational strategies were implemented. These efforts were designed to foster student well-being at multiple levels, addressing both individual and collective needs through intentional integration of wellness-focused practices. The following section details how advising practices and the 6 pillars of lifestyle medicine are systematically embedded within the curriculum and co-curricular activities to promote holistic development and professional readiness among DPT students.
Advising
Advising within the DPT program is structured to provide targeted support across the 3 years of study, balancing the development of meaningful faculty-student relationships with the practical limitations of time and workload. Each student is assigned a faculty advisor and is required to meet with their advisor twice in the first semester, with third and subsequent meetings scheduled as needed. Faculty typically advise 4-5 students per cohort, though this number may vary based on faculty availability.
In addition, students participate in a mental health “Quick Check” facilitated by the institution’s Counseling and Psychological Services office, which offers a confidential, 15-minute session designed to identify individuals who may benefit from further mental health support.
In the second year, there are no mandatory advising sessions. Instead, course coordinators and laboratory instructors monitor student wellness and academic performance, offering informal support and guidance as needed. Students are encouraged to meet with their advisors on an as needed basis to develop strategies to support academic success and well-being.
During the third year, students participate in a final required advising meeting focused on discussing their professional development plans. The meeting serves to support their transition into professional practice, ensuring that those needing additional assistance are identified and supported as they complete the program.
At the programmatic level, student support and oversight are facilitated by the Student Success and Performance Evaluation Committee (SSPEC), a standing body within the Physical Therapy Program dedicated to promoting the success of students. The committee is responsible for fostering meaningful advising interactions between faculty and students, overseeing the development and implementation of remediation plans, and ensuring coordination and compliance with Americans with Disabilities Act accommodations in collaboration with our institution’s Accessibility Services Center. To maintain defensible support practices, the SSPEC committee emphasizes thorough documentation when assisting students. Additional responsibilities include recommending candidates for scholarships and awards and conducting outcome analyses in partnership with the physical therapy Program Curriculum Committee. The committee’s structure comprises standing subcommittees focused on advising, scholarship and awards, and accommodations and remediation.
Building on the foundation of robust advising and student support structures, the curriculum further integrates each of the 6 lifestyle medicine pillars 13 through a combination of coursework and co-curricular activities that collectively promote wellness for future licensed PTs.
Integration Points for Lifestyle Medicine Pillars Across the Curriculum
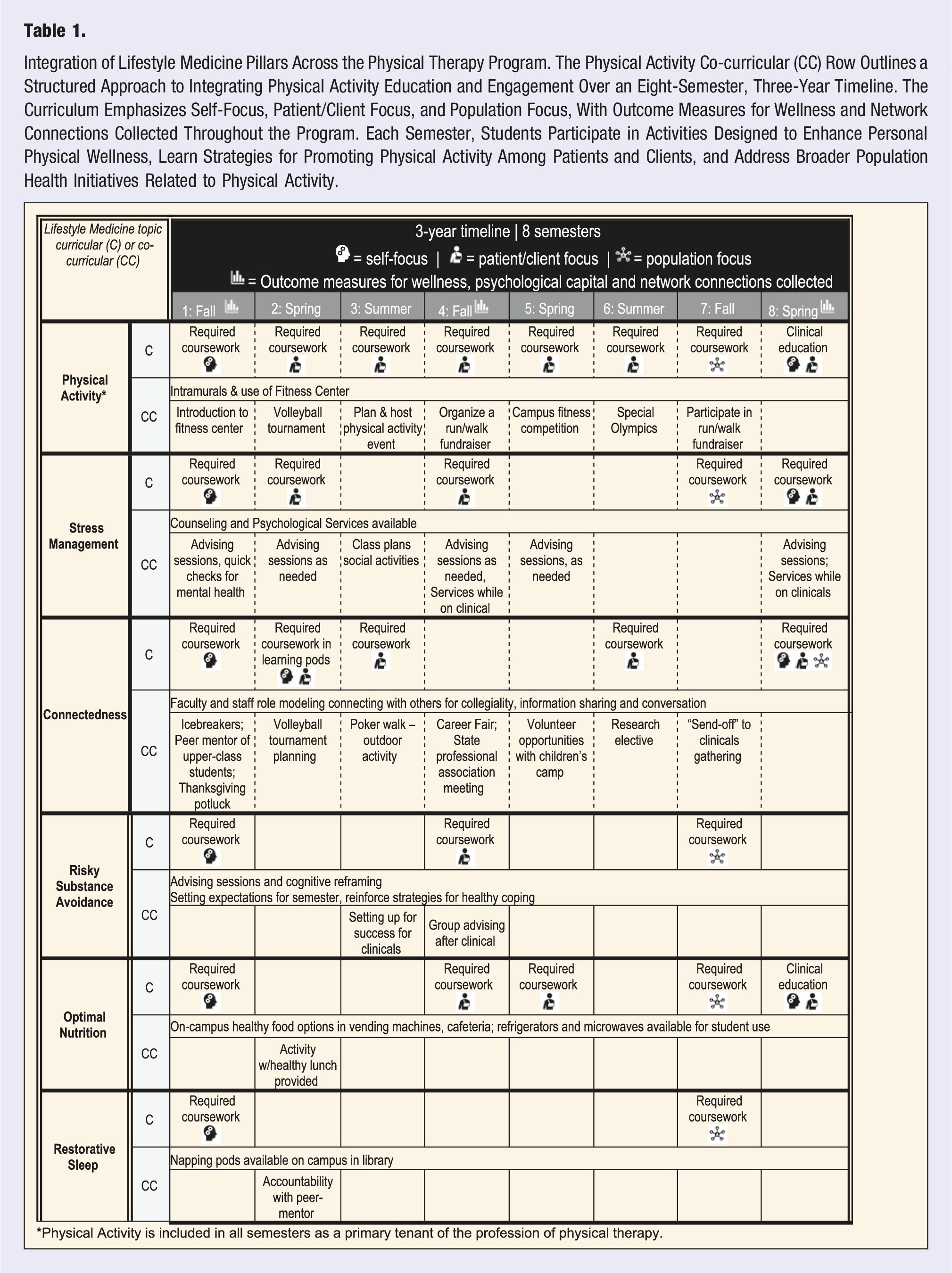
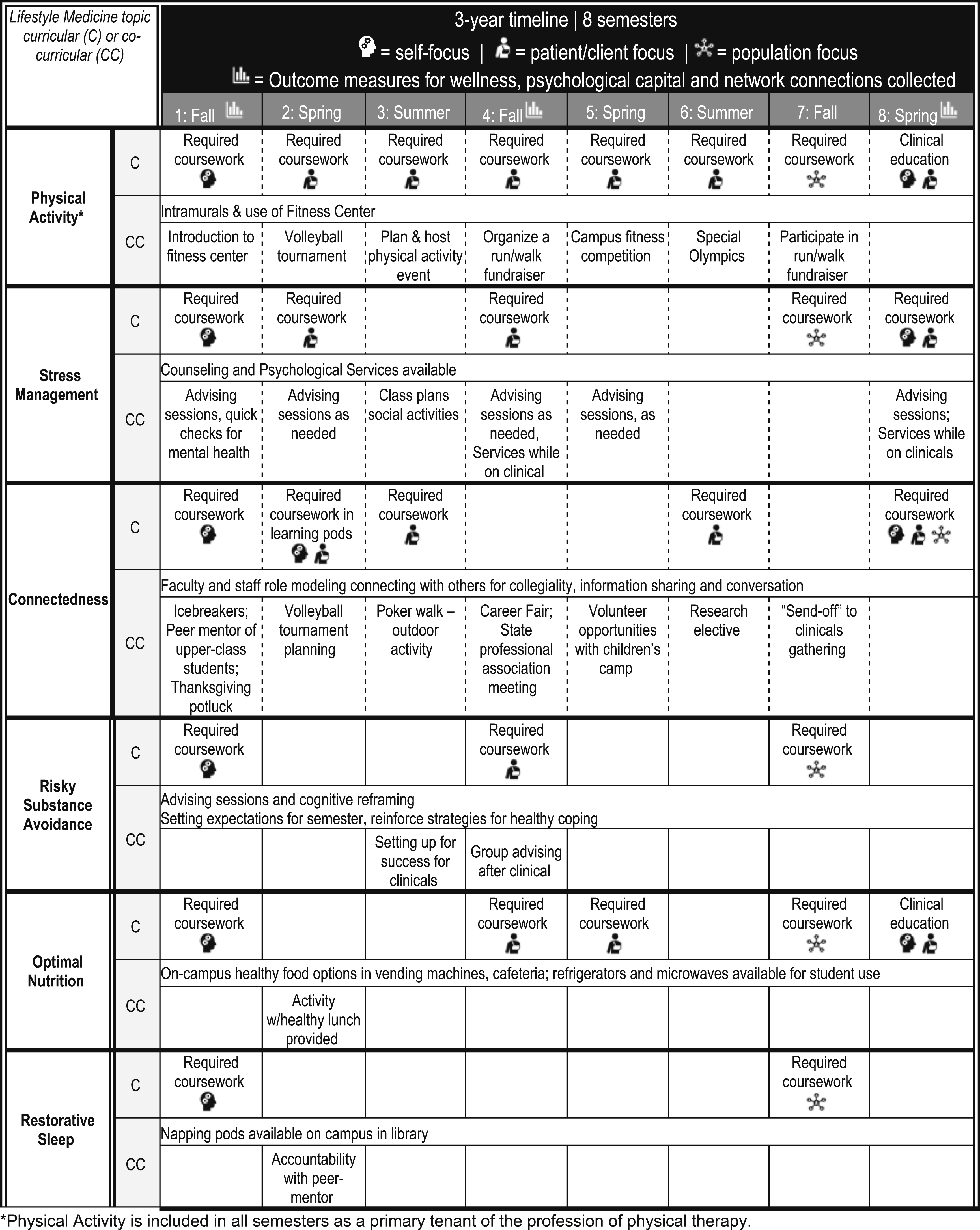
Integration of Lifestyle Medicine Pillars Across the Physical Therapy Program. The Physical Activity Co-curricular (CC) Row Outlines a Structured Approach to Integrating Physical Activity Education and Engagement Over an Eight-Semester, Three-Year Timeline. The Curriculum Emphasizes Self-Focus, Patient/Client Focus, and Population Focus, With Outcome Measures for Wellness and Network Connections Collected Throughout the Program. Each Semester, Students Participate in Activities Designed to Enhance Personal Physical Wellness, Learn Strategies for Promoting Physical Activity Among Patients and Clients, and Address Broader Population Health Initiatives Related to Physical Activity.
Physical Activity
Physical Activity is comprehensively integrated across the curriculum through didactic content, laboratory experiences, and clinical education. Foundational concepts in therapeutic exercise, including muscle activation and exercise prescription, are introduced early and reinforced through lectures, labs, and group assignments. Students apply and adapt exercise interventions in case scenarios and practical exams, addressing impairments in strength, balance, coordination, and more. As coursework progresses, students learn to tailor exercise strategies for different practice patterns across the lifespan through targeted courses and community-based learning. Clinical education further develops these skills by providing hands-on opportunities to implement and progress exercise plans with real patients and community groups under the supervision of a licensed PT.
Physical activity co-curricular initiatives are systematically integrated to promote student wellness and engagement. These activities include automatic membership and orientation to the campus fitness center including participation in intramural sports, group fitness classes, and use of exercise equipment. Additional co-curricular experiences feature an all-night volleyball tournament to benefit a community organization, organization of class run/walk fundraisers, and involvement in FunFitness and MedFest screenings for Special Olympics athletes.
Stress Management
The integration of self-reflection assignments with service-based required activities within the curriculum has not only facilitated professional development and maturation but also contributed substantively to student stress management. By requiring explicit instruction in reflective practices and providing faculty training and dedicated time for individualized written feedback, the program equips students with skills in self-assessment and coping. These structured opportunities for reflection allow students to identify sources of stress, evaluate their personal well-being, and develop adaptive strategies in collaboration with faculty advisors. The resulting one-on-one engagement between advisors and students fosters supportive relationships, promotes open dialogue about wellness, and encourages proactive management of stressors encountered during academic and clinical training.
Students begin with self-assessment and self-discovery to better understand their individual levels of wellness, including identifying their support networks. For example, a required seminar course activity prompts students to engage in both small and large group discussions that includes how their support network can assist with stress management. Through this interactive class session, students learn ways to support others in their networks while also receiving support themselves. Additionally, students develop an objective plan to address necessary changes, all while building relationships within their cohort and with faculty advisors.
At the program level, we continuously review our policies, procedures, and curriculum to identify high-stress points, enhance co-curricular activities, and create opportunities for meaningful change. Throughout multiple courses, students receive instruction in evidence-based stress management techniques, ensuring ongoing support and development in this vital area.
Connectedness
Established literature indicates that individuals tend to form social connections with others who share similar characteristics, commonly referred to as the “birds of a feather flock together” phenomenon. 14 We address this concept in the seminar course, where students are presented with visualizations of their class social network and engage in discussions about evidence-based strategies for forming new connections.
Social integration within the program is intentionally facilitated through a peer-mentorship model pairing first-year physical therapy students with second-year students. This peer-support culture is initiated prior to matriculation and continues throughout at least the first year of study. Additional co-curricular activities further promote social cohesion, including a Thanksgiving potluck attended by students, faculty, and staff, as well as ice-breaker activities held during the annual career fair, an event bringing together students from both campuses.
Students also collaborate through their professional association to organize a fundraiser for the state arthritis foundation which fosters community partnerships with local teams, sponsors, and other event organizers. The program hosts a “welcome back from clinical” event, and each student is required to attend a state professional association meeting that provides opportunities for networking with students from other programs, local clinicians, and invited speakers. Social connections are further strengthened through participation in an optional research elective, where students engage directly with study participants, especially in projects involving human subjects or community partners. The program also organizes a “send-off” event prior to students’ final clinical experiences, offering continued support and relationship-building at a key curricular milestone.
Faculty actively model collegiality by engaging in team-teaching, sharing information, and fostering professional conversations. The curriculum includes structured requirements to facilitate social interaction, such as assigned learning pods where students collaborate intensively with a consistent group of peers over several weeks.
Risky Behavior Avoidance
The program integrates both curricular and co-curricular approaches to educate students on recognizing and avoiding risky behaviors. Required coursework in the first semester incorporates self-reflection activities, while later coursework addresses the psychosocial aspects of health care, including the identification, management, and appropriate referrals of patients exhibiting risky behaviors. Additionally, the curriculum includes a population health component toward the end of the program, further equipping students with the knowledge and skills to address risky behaviors at both the individual and community levels. Students participate in class sessions focused on achieving success during clinical education and managing stress, with various mindfulness and stress-reduction techniques introduced and practiced during each clinical education preparatory session. A culture of peer and faculty support networks encourages engagement and may mitigate maladaptive coping strategies for stress.
The faculty advising sessions emphasize cognitive reframing and the establishment of clear expectations each semester, reinforcing healthy coping strategies. Group advising sessions are conducted following clinical experiences, providing a forum for students to discuss clinical education experiences with patient encounters that involved risky behaviors and to reflect on their own responses as developing PTs. These integrated strategies ensure that students are prepared to recognize, address, and mitigate risky behaviors with appropriate screening and referral throughout their professional training.
Optimal Nutrition
Nutrition-related curricular content is integrated throughout the program in several key areas. Within Seminar 2, students engage in self-reflection activities that address nutrition. Clinical coursework incorporates nutrition education relevant to patient care. Students are educated to identify and address nutrition-related concerns across developmental stages, including the assessment of infants and children in the domains of physical (nutrition, growth, strength), cognitive, language, and social-emotional development to ensure appropriate referrals. Additionally, adult populations are considered, with curricular content addressing nutritional needs for individuals with wounds or athletes whose caloric requirements may differ.
In the advanced stages of the program, specifically within the health promotion and policy course, students are instructed on the application of the Malnutrition Screening Tool. They learn to recall and utilize three screening questions applicable to both inpatient and outpatient settings, enhancing their competency in identifying malnutrition risk within different patient populations.
To support healthy eating behaviors on campus, the institution ensures the availability of nutritious food options in vending machines and cafeterias. Additionally, refrigerators and microwaves are accessible for student use, facilitating the storage and preparation of healthy meals and snacks. Students are also given information about community food resources such as food pantries.
Restorative Sleep
Early in the curriculum, students engage in structured self-reflection activities as part of the initial seminar series, as previously outlined. Furthermore, the curriculum emphasizes the significance of adequate sleep and delineates the PTs' responsibility in screening and educating patients regarding sleep health, including sleep hygiene. To further support student wellness, the campus library is equipped with comfortable chairs providing students with opportunities to rest and manage fatigue effectively.
Outcome Measures
Outcome measures were collected at 3 timepoints including the beginning of the program within the first few weeks of matriculation, mid-program near the middle of semester 5 and at the time of graduation. The outcome measures were gathered at the student respondent level and analyzed at the cohort level and across all cohorts. The time points are illustrated in Table 1.
Five Factor Wellness Inventory (FFWEL)
The 5 Factor Wellness Inventory (FFWEL) was developed to identify factors which are central to healthy living where personal responsibility and choice have positive effects. 15 This tool has even been called the “gold standard of wellness assessments.” 16 Reliability analyses demonstrated strong internal consistency, as indicated by Cronbach’s alpha coefficients for each of the 5 factors: Creative Self (α = .96), Coping Self (α = .89), Social Self (α = .96), Essential Self (α = .95), and Physical Self (α = .90). The total wellness score also exhibited excellent reliability (α = .98). 17
The total score represents an overall assessment of wellness, providing a comprehensive evaluation of an individual’s total well-being. The subsequent 5 scores correspond to the distinct dimensions of wellness, each reflecting one of the five specific factors measured by the instrument.
15
1. Creative Self “includes components of thinking, emotions, control we have, work and positive humor. It is the combination of attributes that forms individuals to make a unique place among others in social interactions and to positively interpret the world.”
15
2. Coping Self “includes the components of leisure, stress management, self-worth and realistic beliefs. It is the combination of elements that regulate the responses to life events and provide a means for transcending their negative effects.”
15
3. Social Self “includes friendship and love components and social support through connections with others in our friendships and relationships.”
15
4. Essential Self “is comprised of components of spirituality, gender identity, cultural identity and self-care. It is meaning-making processes in relation to life, self, and others.”
15
5. Physical Self “includes components of exercise and nutrition. This encompasses the biological and physiological processes that comprise the physical aspects of functioning.”
15
Psychological Capital Questionnaire
The Psychological Capital Questionnaire (PCQ) is a well-validated measure of an individual’s positive psychological state (PsyCap), comprising hope, self-efficacy, resilience, and optimism (HERO). 18 Studies consistently confirm its four-factor structure and higher-order PsyCap construct through factor analyses.19-21 Reliability is strong, with Cronbach’s alpha typically ranging from .70 to .93 for subscales and total scores, and test–retest correlations above .80 indicate stability over time. Validity evidence includes construct validity (CFA/EFA), and criterion validity through positive associations with performance, engagement, and well-being.
Each HERO trait contributes uniquely to the lifestyle medicine pillars: Hope relates to goal-setting and thinking about the future; Self-Efficacy includes an empowerment of individuals to take action and persist through challenging situations; Resilience supports recovery from setbacks, may improve adherence to healthy behaviors and help mitigate risky behaviors and promotes positive coping; and Optimism fosters a positive outlook, that could reduce psychological barriers to living in a healthy way.
Social Network Peer Connections
To collect the peer connections, the study participants were provided with a roster of all classmates then asked to mark their level of closeness on a 1-7 scale for each classmate. The question read: How close do you consider yourself to each classmate you know? “Think of very close as someone with whom you have a deep relationship with and would go to for advice or support with a particular issue whether or not it was school or work related.” (1 = not close at all, 7 = very close). This question was drawn from prior work in physical therapy education examining network connections.22-24
A matrix of connections was created with “close ties” defined as someone with a connection score of at least 4/7 by 1 of the 2 classmates. The matrix was symmetrized with 1 renamed for closeness greater than or equal to 4/7 and 0 for all others.
Whole network analysis includes findings about the connections among the entire cohort. We examined 2 network measures. Degree is the average number of close connections between students and group connectedness measured cohesion among the class and can be monitored over time. Cohesion is the proportion of pairs of students that can reach each other by a path. 25
Each outcome measure in this study demonstrates a distinct alignment with the pillars of lifestyle medicine. Notably, several subcomponents of the 5 Factor Wellness Inventory closely correspond in both terminology and conceptualization to these pillars. The HERO constructs of psychological capital further exemplify the multidirectional influence exerted across all lifestyle medicine pillars. Social network analysis, along with its visual representations, offers a direct evaluation of peer relationships within the cohort.
Social Ecological Model
We analyzed each tier of the Social Ecological Model. This multi-layered perspective facilitated an examination of how a variety of interconnected factors influence both wellness and academic achievement among students.
Statistical Analysis
The FFWEL total and component scores were summarized at each of the 3 points for each of the 4 study cohorts and for the aggregation of all 4 cohorts using means and standard deviations. These results were compared to norms published by the instrument’s creators. 15 A Sankey diagram was used to show how students’ FFWEL total score changed over the course of the program. The FFWEL scores at the beginning of the program were divided into tertiles (labeled Level 1 through Level 5 for the lowest to highest tertiles). Using the same cut point values for defining the levels, students were assigned to the appropriate level at the other 2 time points with the diagram showing how many students moved up or down and how far during each transition.
For PsyCap measures, the scores for each construct were summarized at each time point for the 2022 and 2023 cohorts and at the final time point for the 2024 and 2025 cohorts, both by cohort and with all available cohorts aggregated using means and standard deviations. All FFWEL and PsyCap analyses were done using Stata v18.5 (StataCorp, LLC, College Station, TX).
Social network analysis was used to describe the whole network including group analysis of number of connections (i.e., degree) and connectedness as a measure of cohesion. UCINET 26 software was used to conduct the social network analysis.
Results
Study Participant Characteristics
The FFWEL, PsyCap and network connection data were systematically collected at 3 distinct time points, program start, mid-program, and graduation, for the graduating classes of 2022 and 2023. Due to challenges and resource limitations resulting from the COVID-19 pandemic, data collection at program start and mid-program was not conducted for the classes of 2024 and 2025 for PsyCap and the network. Despite these constraints, complete outcome data for all 3 measures are available for all 4 cohorts at the time of graduation.
Study Participant Characteristics by Cohort Year.
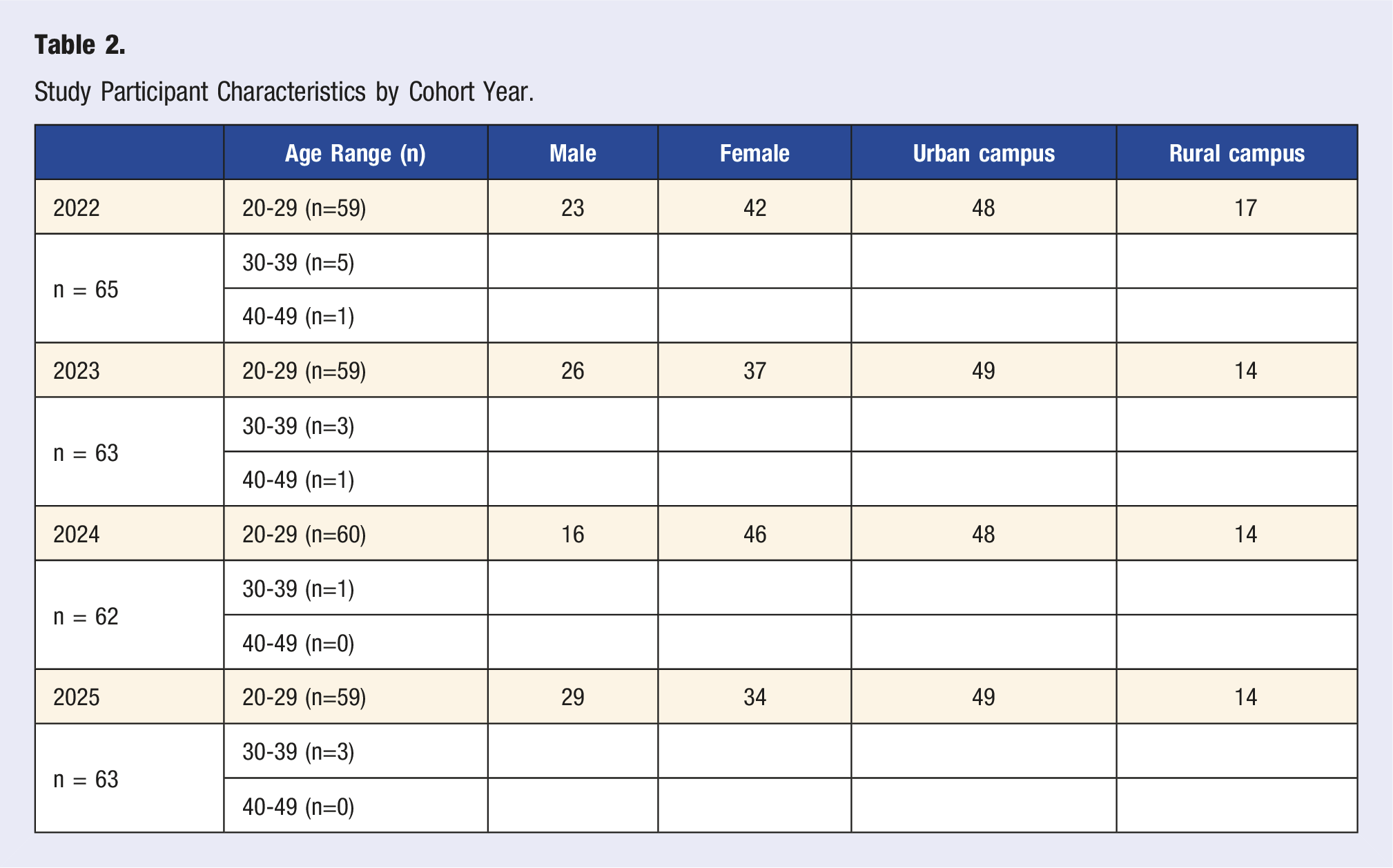
The age distribution of participants was predominantly within the 20-29 year range, accounting for much of each cohort and 93% (n = 235/253) of total participants. A smaller proportion, 4.7%, of students fell into the 30-39 age bracket (n = 12/253), and only 2 participants were aged 40-49, reflecting the typical age profile of entry-level physical therapy students. 27
Gender representation varied across cohorts, with each class including both male and female students. The data indicate a consistent majority of female participants in each cohort and 63% (n = 159/253) of the total, which aligns with national trends in physical therapy education. 27
Geographically, students were distributed between two campuses—urban and rural—located approximately 200 miles apart. The urban campus consistently graduated
This sample provides a foundation for evaluating the longitudinal impact of curriculum interventions.
Five Factor Wellness Outcomes
5 Factor Wellness Inventory Mean (SD) Scores for the Each Cohort Over Time.
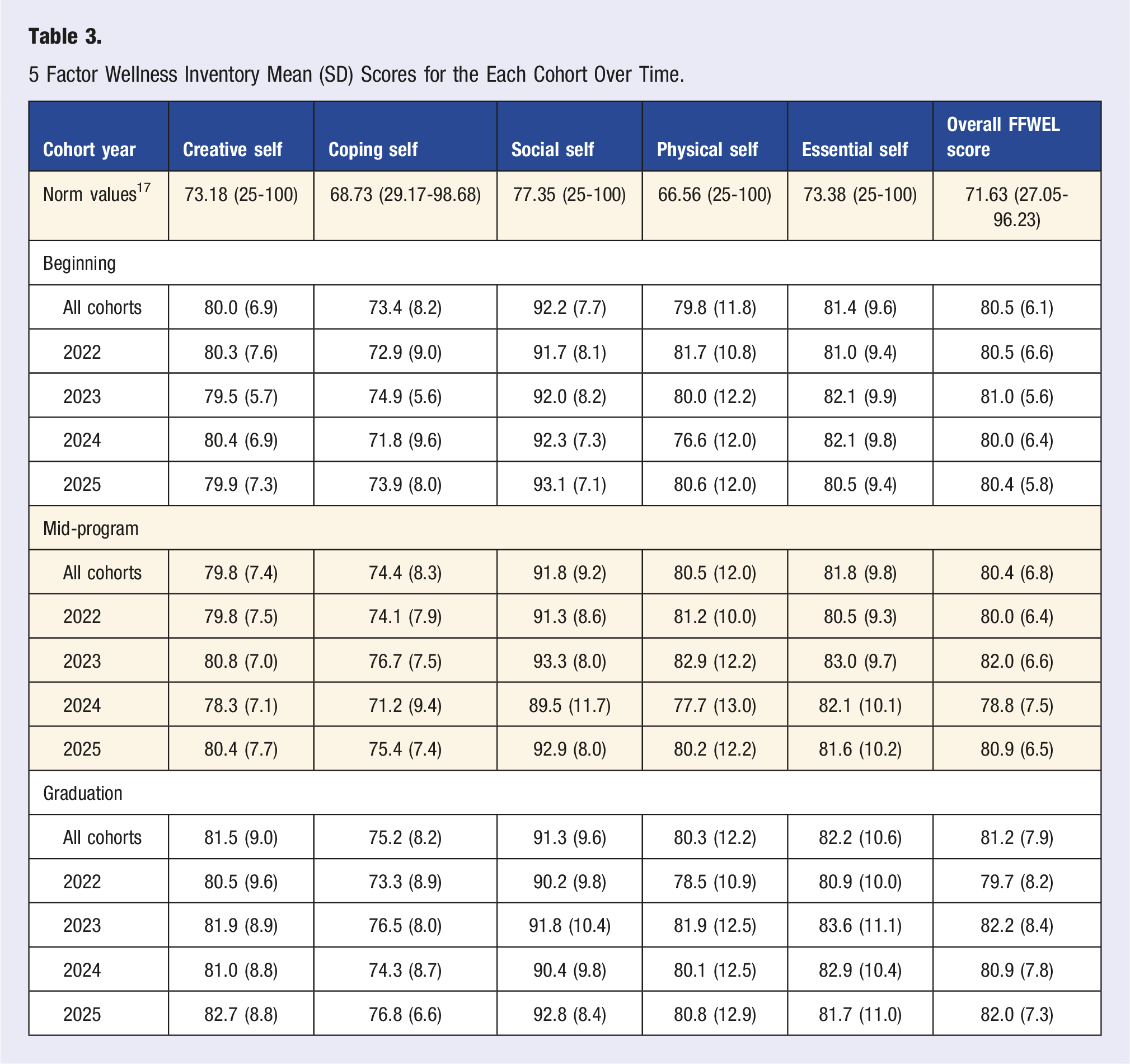
The Social Self domain of the FFWEL demonstrated consistently higher scores across all cohorts and time points. At the beginning of the program, the mean Social Self score for all cohorts was 92.2 (7.7), which remained elevated mid-program at 91.8 (9.2), and at graduation, the score was 91.3 (9.6). Individual cohort scores also reflected this trend, with values ranging from 89.5 (11.7) to 93.3 (8.0) over time. These results indicate that participants consistently reported strong social wellness relative to published norm values (77.35) and suggest that social self was the highest scoring domain among the 5 factors, regardless of cohort year or program stage. This mean difference between all individual cohort measures at each point and the mean norm value was largest for Social Self (mean = 14.43), followed by Physical Self (mean = 13.62), Overall (mean = 9.07), Essential Self (mean = 8.45), Creative Self (mean = 7.28), and Coping Self (mean = 5.59).
The Sankey diagram (Figure 1) illustrates how students’ total FFWEL scores changed throughout the program. At the program’s start, FFWEL scores are grouped into 5 levels, labeled Level 1 (lowest) through Level 5 (highest). The connecting lines in the diagram represent the number of students who moved up or down between these levels at the mid-program and graduation checkpoints, showing the direction and extent of student’s progress over time. Sankey Diagram of Longitudinal Changes in Students’ Five Factor Wellness Scores Grouped by Level.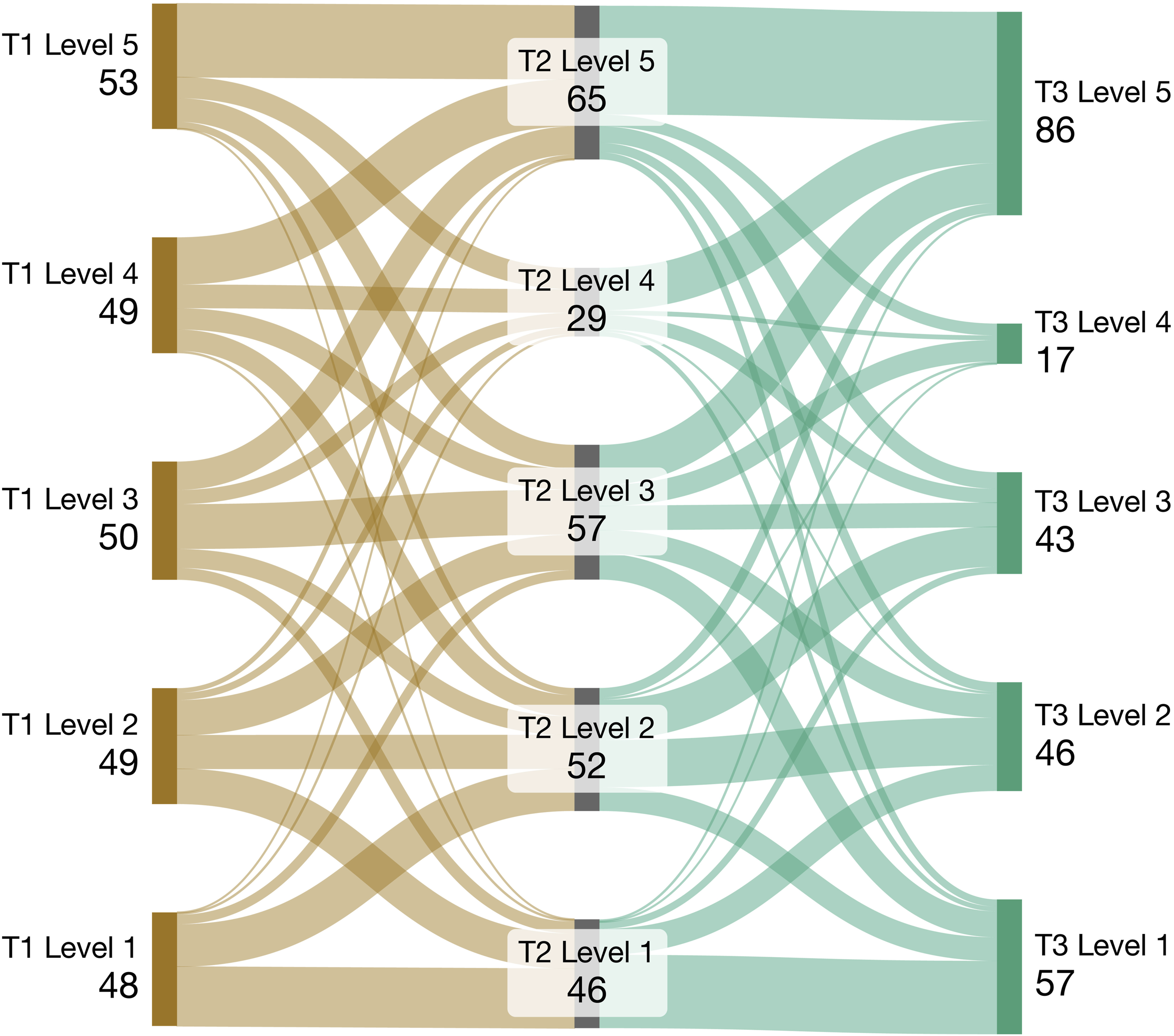
Psychological Capital Outcomes
Mean Scores (SD) for the Psychological Capital Scores.
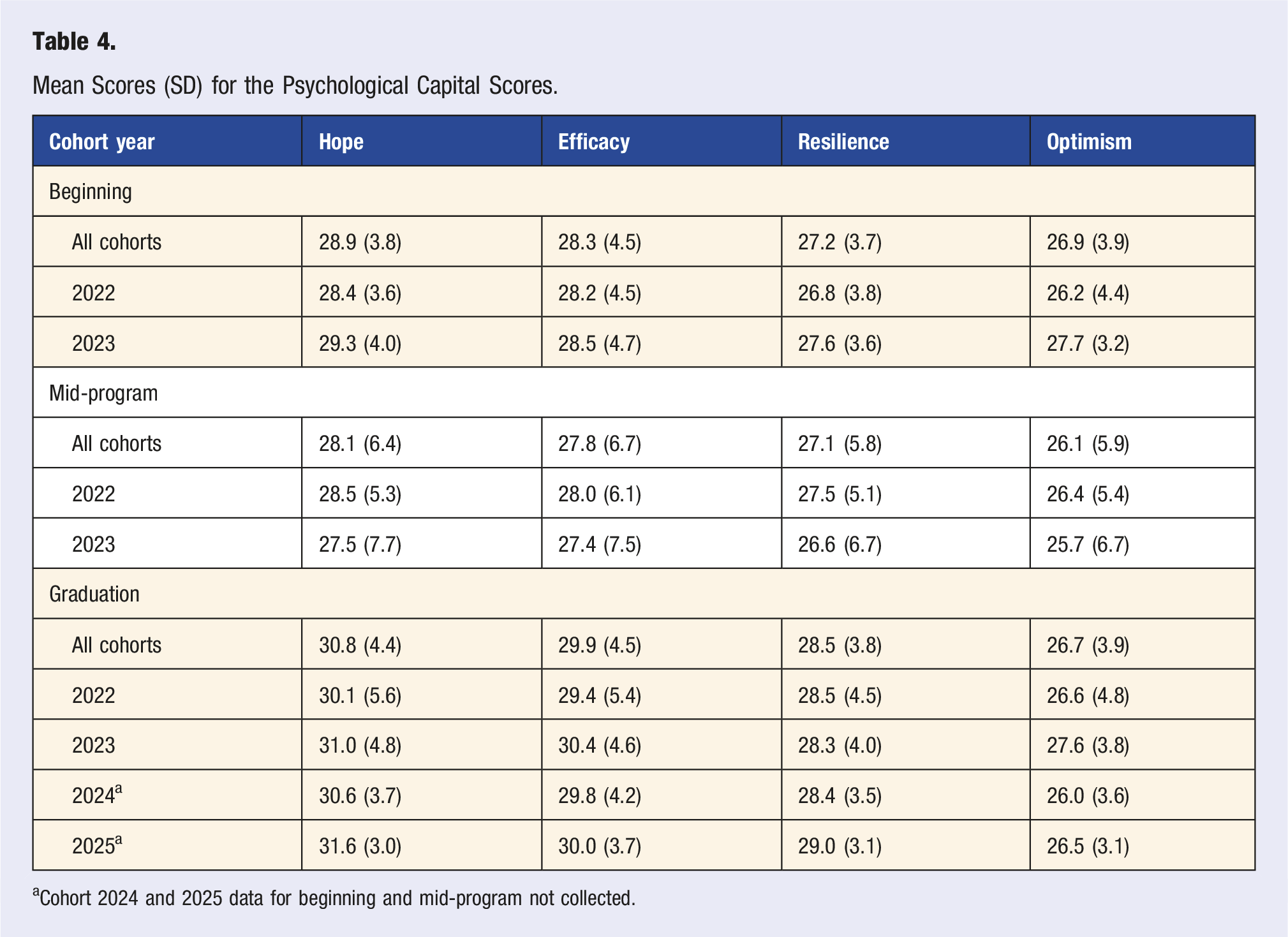
aCohort 2024 and 2025 data for beginning and mid-program not collected.
Social Network Analysis
Network Analysis of Close Connections and Connectedness.
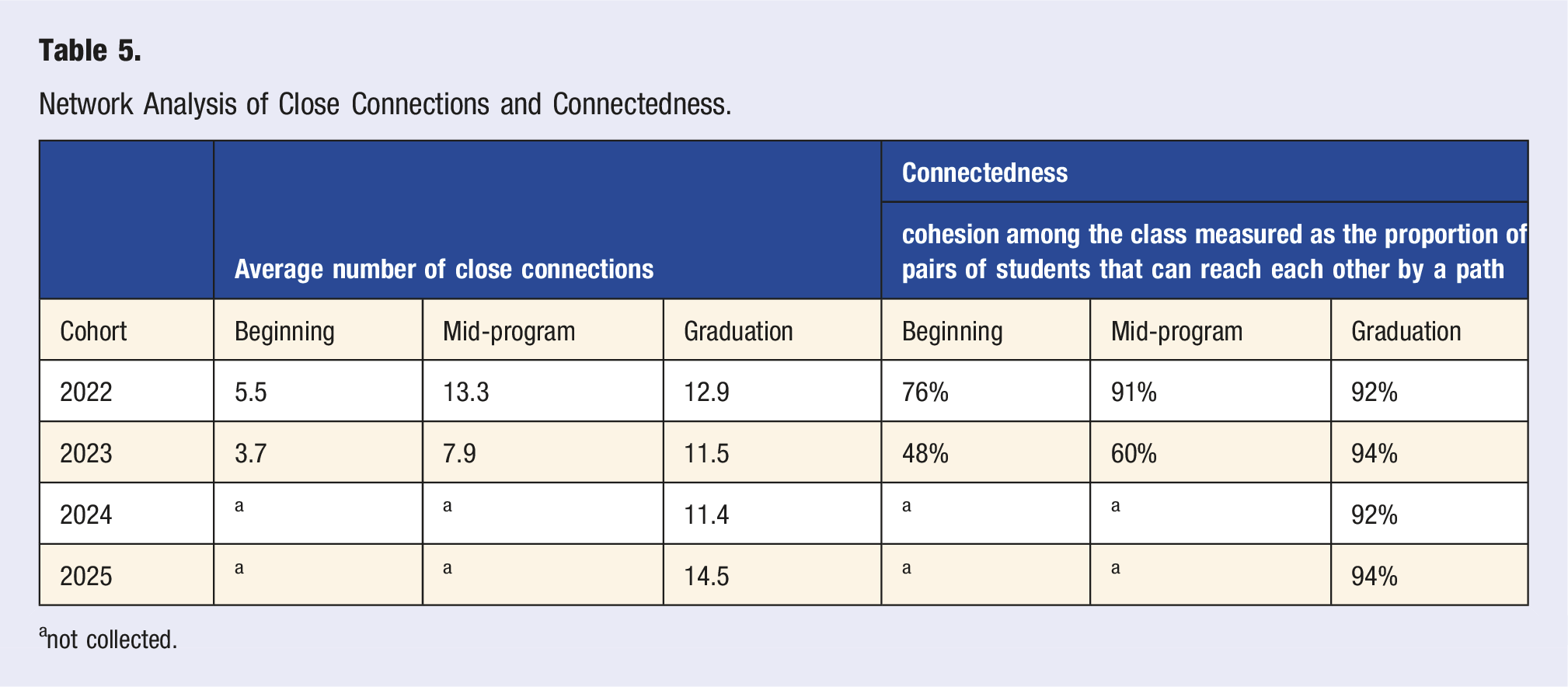
anot collected.
To illustrate the evolving patterns of peer connectivity throughout the program, the network visualizations depict the growth in close relationships among students across cohorts (Figure 2). Each icon (e.g., circle) represents 1 student. A line between them is a tie indicating a close connection. Students are placed closer to other students in which more connections are shared. Network connections visualizations for each cohort.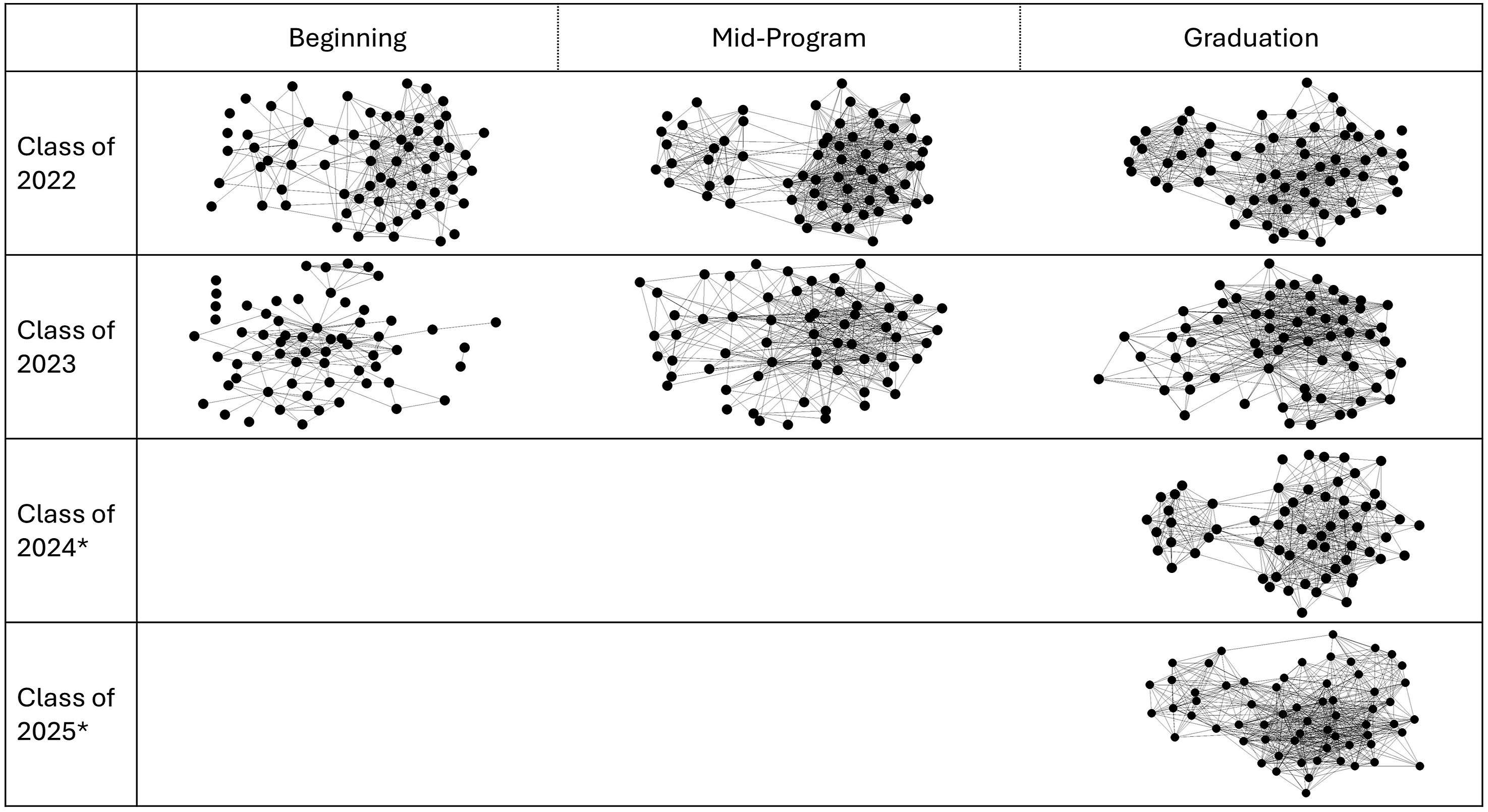
Social Ecological Model
An inventory of the interconnected roles for students, cohort, program, institution and external factors for supporting a curriculum integration of lifestyle medicine concepts is shown in Figure 3. The Social Ecological Model illustrates the multi-level influences on student well-being and learning. The model’s concentric circles emphasize the nested and interactive nature of contextual factors that shape student experiences. At the external level, influences include accreditation standards, licensing boards, access to health care, and broader issues such as social injustice and social determinants of health. The institutional level encompasses policies and procedures related to due process, financial aid and counseling services, and the complexity of operating across multiple colleges and programs. The program level highlights curricular and relational structures, including reflection assignments with faculty feedback, one-on-one student–faculty advising, mental health quick checks, and the importance of faculty role modeling and commitment to the curriculum. The cohort level reflects shared learning such as director’s student advisory committee, seminar series, psychosocial and interprofessional coursework, TeamSTEPPS® education, and class-based networking or fundraising activities. At the core of the model is the student level, which includes student senate participation, access to counseling and accommodations, and engagement in interprofessional education. Together, the figure underscores that student outcomes are shaped not by isolated interventions but by coordinated, multi-level supports operating across the educational system. The Social Ecological Model with examples for each area.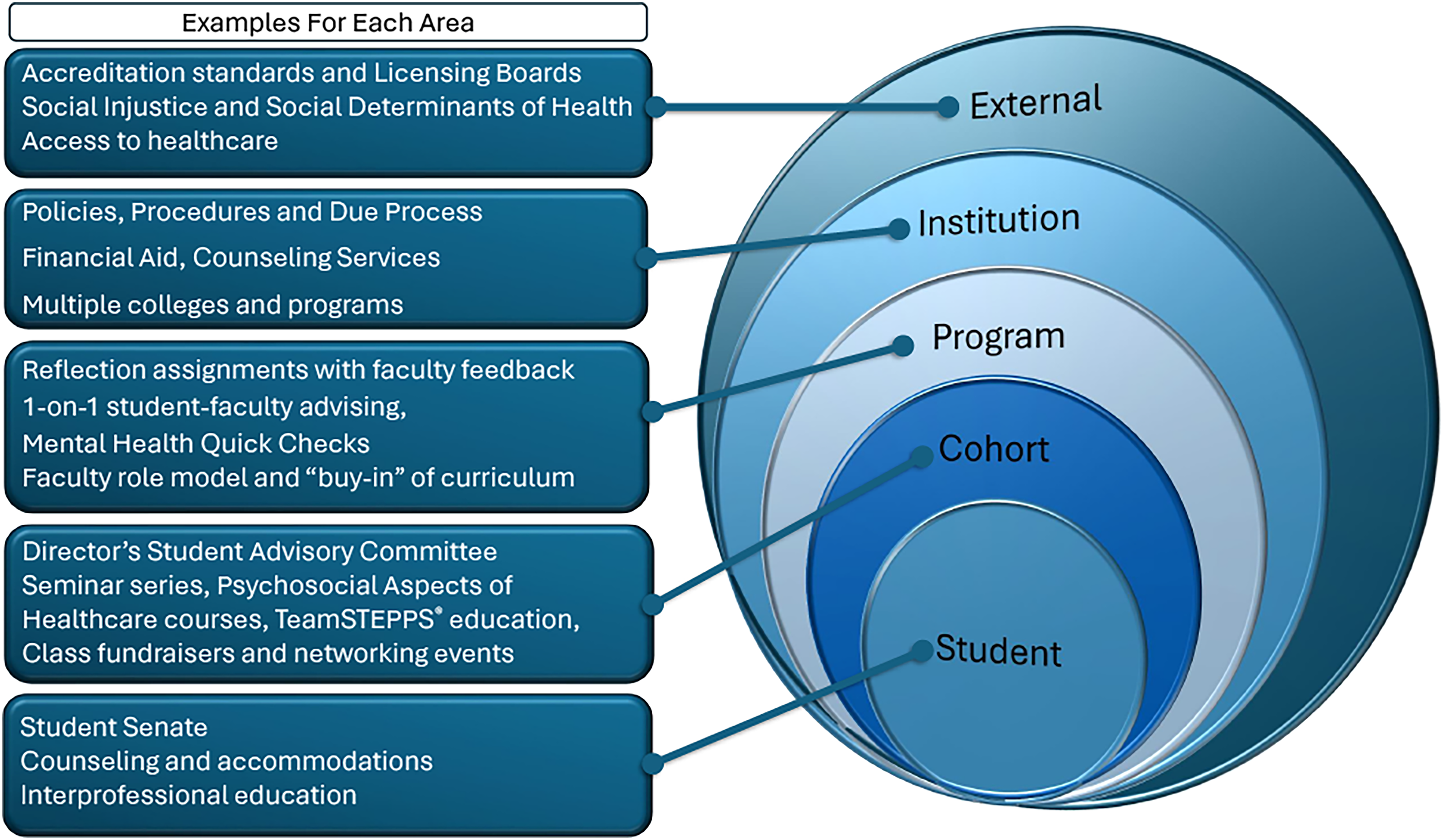
Discussion
The integration of lifestyle medicine into health professional education has been increasingly advocated, however, reported efforts are focused on individual courses, brief interventions, or single wellness domains rather than longitudinal, curriculum-wide approach.28-33 Studies in health science education have demonstrated that introducing lifestyle medicine principles, such as physical activity, stress management, nutrition, and social connection, can improve learner knowledge, attitudes, and self-reported well-being, though these initiatives are often short-term and variably embedded within curricula.28-34
Consistent with this emerging literature, early experiences with lifestyle medicine curriculum implementation suggest that even relatively brief, scalable educational interventions can meaningfully enhance learner knowledge, confidence, and readiness to apply lifestyle medicine principles across clinical and educational settings.34,35 Our findings suggest that intentional exposure to lifestyle medicine concepts is associated with positive student wellness outcomes; however, our program extends prior work by operationalizing these concepts across multiple curricular and co-curricular touchpoints over the entirety of a DPT program. Moreover, previous research has documented declines in physical activity, sleep quality, and mental health among health professions students over the course of training, particularly during periods of high academic and clinical demand.4,5,10
In contrast, the consistently elevated wellness and psychological capital scores observed in this study suggest that a multi-level, longitudinal approach may mitigate commonly reported declines and support sustained well-being. By situating lifestyle medicine within the Social Ecological Model, our findings align with broader health promotion research emphasizing that behavior change and resilience are most effectively supported when interventions extend beyond individual responsibility to include peer networks, faculty role modeling, and institutional structures.34,36,37
Key findings from integrating lifestyle medicine into physical therapy education include 3 highlights.
First, PTs can be ambassadors for health promotion.38,39 This study demonstrates that students who graduate from this program are uniquely positioned to champion lifestyle medicine by leveraging their expertise in movement systems and embracing additional pillars such as nutrition, stress management, and social support. Embedding lifestyle medicine concepts throughout physical therapy education—via both required curriculum and co-curricular activities—promotes holistic student development. This approach not only fosters readiness for the workforce but also may cultivate a sense of responsibility for personal health behaviors, preparing students to model and advocate for healthy practices in their future professional roles. The educational environment, when intentionally designed to support these principles, should contribute to the formation of a resilient and health-focused workforce.
Second, institutions play a critical role in promoting student success, and faculty should systematically review and revise policies, procedures, and support systems.36,37 Alignment with the Social Ecological Model ensures that support is provided at multiple levels—including individual, cohort, program, and institutional domains. Key strategies include the development of intentional curricula, provision of adequate infrastructure and resources, and fostering interdepartmental collaboration. Comprehensive student support should encompass accessible policies, effective absentee management, robust accommodations, counseling services, and readily available financial aid.40-43 These measures create an environment where students can thrive academically and personally.
Third, utilizing outcome measures and analyzing the impact of social connections was an effective approach for assessment. We employed 3 distinct outcome measures—wellness inventory, psychological capital assessment, and social network analysis—to longitudinally assess students, including during the COVID-19 pandemic. The results highlight the importance of social connection and psychological capital in fostering student success. Increases in cohort network connections over time underscore the value of peer support and collaborative learning, particularly during periods of disruption such as a global pandemic. These findings reinforce the established literature on the positive impact of peer groups and social support networks, emphasizing the need for programs to nurture social bonds and implement strategies that enhance well-being and academic achievement.40,44,45
Furthermore, the findings indicate that FFWEL scores consistently exceeded cohort norms, and PsyCap scores remained elevated throughout the study period. This sustained high performance may be attributable to students actively engaging with both the curriculum and co-curricular supports, as well as their intrinsic motivation and clear professional goals associated with self-selecting into the physical therapy profession. Such factors likely contribute to the development and maintenance of robust psychological resources and well-being among participants.
Taken together, these findings extend prior work by demonstrating that a longitudinal, multi-level integration of lifestyle medicine within a DPT curriculum supports student wellness, psychological capital, and social connectedness across the duration of professional training.
Limitations
While our analyses utilized aggregate data for outcome measures, it may be beneficial to examine individual students whose scores fall below cohort norms. Identifying these students could allow for targeted interventions and personalized support, thereby enhancing overall student well-being and success within the program. Ongoing evaluation of institutional and external factors is essential, particularly as policies evolve and programs adapt to address their effects on students and the overall curriculum.
This study was conducted within a single DPT program at an academic health science center, and findings should be interpreted within this context. Although the cohort demographics align with national trends in physical therapy education, program-specific factors such as curriculum structure and faculty engagement may have influenced outcomes. Accordingly, these findings are most applicable to similar health professions programs and may not be generalized to all health professions educational settings.
Conclusion
In conclusion, this exemplar of integrating lifestyle medicine concepts into physical therapy education demonstrates significant promise for enhancing both student outcomes and future professional practice. By embedding these principles across curricular and co-curricular experiences, PTs are prepared to serve as advocates for health, benefiting from a supportive institutional environment that prioritizes adaptable policies and comprehensive resources.
These findings support the need for intentional strategies in education that foster both individual and collective well-being, suggesting that a multi-level approach—aligned with the Social Ecological Model—can cultivate a resilient, health-focused workforce ready to promote lifestyle medicine in diverse settings.
Footnotes
Acknowledgments
The authors would like to acknowledge the current, retired and emeritus physical therapy faculty at the University of Nebraska Medical Center for their contribution to curriculum discussions and implementation.
Ethical Considerations
The Institutional Review Board of the University of Nebraska Medical Center approved this study #583-19--EX.
Author Contributions
• Lead the concept, design, acquisition, analysis and interpretation of data
• Drafted the article
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Made a significant contribution to the concept, design, acquisition, analysis and interpretation of data
• Significant contribution to the drafted article
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Made a significant contribution to the concept, design, acquisition, analysis and interpretation of data
• Significant contribution to the drafted article
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Made a significant contribution to the concept, design, acquisition, analysis and interpretation of data
• Significant contribution to the drafted article
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Made a significant contribution to the analysis and interpretation of data
• Significant contribution to the drafted article
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Made a significant contribution to the concept (literature review), design interpretation of data
• Critically revised draft for important intellectual content
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Made a significant contribution to the concept (literature review), design interpretation of data
• Critically revised draft for important intellectual content
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity
• Primary role in establishing the concept, design, acquisition, analysis and interpretation of data
• Significant contribution to the drafted article
• Approved the final version of the article for publication
• Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity with the corresponding author.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
It is not possible to share the data based on the IRB approval. The data is part of the student’s academic record and part of ongoing research.