
Abstract
The aim of this systematic review and meta-analysis (registration: CRD420251179983) was to examine the combined effects of diet and physical activity interventions on depression and anxiety in adult populations of any health status. Eligibility criteria included adults >18 years old, healthy and patients of any disease and any comorbidity and potential medicine intake, who undertook combined interventions of any type and intensity of exercise/physical activity and any diet, of >2 weeks. We searched PubMed, Ovid and Sport Discus databases from their inception to October 2025. Using the GRADE analysis and the Cochrane handbook for interpretation, we found moderate quality of evidence that the combinations of “exercise + low fat diet,” “exercise/physical activity + calorie restriction,” “exercise/physical activity and balanced diets in specific amounts of carbohydrates, fats and proteins” and “exercise + high protein diet” likely reduce depression. Also, we found low quality of evidence that the combination of exercise/physical activity and diet interventions may reduce anxiety. To determine implications of these findings future randomized controlled trials should examine the effects of specific exercise interventions, along with low fat diets or calorie restriction or high protein diets with potential dose-response effects of these interventions.
“Exercise releases neurotransmitters crossing the blood brain barrier to mediate brain-derived neurotrophic factor expression, stimulating hippocampal neurogenesis.”
Introduction
Depression is a mental health condition, characterized by loss of pleasure or interest in life activities for a long time of period, which may affect relationships with family, friends and society. People with past experiences of abuse and/or severe losses are more vulnerable in this mental condition. 1 Depressive symptoms include feeling sad, irritable, poor concentration, hopelessness about the future, thoughts about dying or suicide, changes in appetite or weight and feeling very tired or low in energy. A 4% of the world population—approximately 332 million people—experience depression, while in 2021, 727 thousand people lost their lives to suicide, due to depression. 1 Anxiety disorder is a common mental disorder affecting 359 million people in 2021—approximately 4.4% of the global population. It is characterized by an excessive fear or worry about a specific situation and includes symptoms such as difficulty in concentrating or making decisions, irritability, feeling tense or restless, nausea, heart palpitations, sweating, trembling or shaking, panic etc. 2 People who have experienced abuse, severe losses or other unfavorable life experiences, are likely to be affected by anxiety disorder. 2
Depression and anxiety are associated with the development of chronic non-communicable diseases such as cardiovascular disease and diabetes type 2,3,4 while the suggested treatment interventions include antidepressant medications.1,2 However, only 13,7% in lower-middle income, 22% in upper-middle income and 36.8% in high-income countries patients receive mental health treatment. 5 This suggests that alternative interventions are necessary to mitigate depressive and anxiety disorders or symptoms. Exercise suggested to be an effective intervention for depression and anxiety treatment in both populations suffering from depressive and anxiety disorder and those that experience depressive symptoms.4,6 The suggested mechanism for this favorable effect of exercise is the production of endogenous opioid peptides in the brain, especially β-endorphin, which is synthesized in the anterior pituitary gland and cleaved from pro-opiomelanocortin and causes euphoria. 7 The amount of β-endorphin and opioids production during exercise seems to be positively associated with sufficient exercise intensities, 8 which is why exercise has been proposed as an alternative to medication treatment for improving symptoms of depressive and anxiety disorders.7,9
Diet and nutrition have also been suggested as alternative interventions for prevention and treatment of depression and anxiety. Indeed, nutrients such as vitamin B6, B12, folic acid, glutamic acid, tyrosine and tryptophan are considered essential to trigger production of relevant neurotransmitters such as serotonin, dopamine and norepinephrine. 10 Also, omega-3 fatty acids may reduce depression and anxiety by triggering the production of serotonin and dopamine.11,12 These neurotransmitters are highly involved in mood state, positively affecting depressive and anxiety symptoms. 13 Therefore, inadequate dietary patterns to increase these neurotransmitters may negatively affect mood state and consequently may trigger depression and anxiety symptoms. 13 Collectively, physical activity and diet patterns may play a role in regulating depressive and anxiety symptoms in both clinical and general populations. To the best of our knowledge, the effects of physical activity/exercise and diet/nutrition on depression and anxiety as sole interventions have been comprehensively investigated to date. However, the combined effects of physical activity and diet have not been extensively studied. In this light, the aim of this systematic review and meta-analysis was to examine the combined effects of diet and physical activity interventions on depression and anxiety in adult populations of any health status.
Materials and Methods
A systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, 14 while we followed instructions of the Cochrane Library Handbook. 15 Our protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number: CRD420251179983). 16
Eligibility Criteria
We employed the population, intervention, comparator, outcome, study design (PICOS) method to determine the eligibility criteria, as following: (a) Population: Adults >18 years old, healthy and patients of any disease and any comorbidity and potential medicine intake, of both genders. Individuals of any physical activity and diet background, at any body mass index (BMI). Studies conducted in populations <18 years old, were excluded. (b) Intervention: Combined interventions of any type and intensity of exercise/physical activity and any diet, of >2 weeks. We accepted interventional studies that used physical and/or remote counseling, behavioral models, education as a combined exercise/physical activity and diet intervention, as long as the intervention included specific and measurable instructions of exercise/physical activity and diet. (c) Comparator: Post intervention data of a control group (i.e., without combined interventions of diet and exercise, or usual care) for randomized and non-randomized controlled trials (CT), or baseline data for single arm design interventional studies (SAS). (d) Outcome: Any measurements of depression and anxiety. (e) Study design: Randomized controlled trials (RCT), CT and SAS. We excluded animal studies, reviews, study protocols, editorials, conference publications, magazines, and gray literature.
Search Strategy and Data Sources
Using PICOS, relevant to our research question keywords were selected. We then searched PubMed, Ovid and Sport Discus databases from their inception to October 2025. The searching key word algorithms for all databases can be found in supplementary methods. The searches were performed by PCD and were checked by GSM.
Systematic Review Procedure
PCD, CZ, MK and NN provided rigorous training to the students who are listed as co-authors in the current paper, for selection, data extraction and risk of bias assessment procedures. Nine teams of students were formed, each of which contained 3-12 members, who performed all processes. CZ, MK and NN acted as second reviewers to the outcomes of the selection, data extraction and risk of bias assessment procedures of all teams, while GSM acted as a referee in case of conflicts.
Study Selection Process
Using the EndNote software PCD removed the duplicated, reviews, conference publications, editorials, protocols, reports, animal studies, no interventional studies, studies conducted in children and adolescences and qualitative or mixed methods studies, from the total number of retrieved publications. The selection process then started from the teams of students as described above. GSM, MP and ASV acted as referees, to resolve any conflict. Finally, CZ screened the reference lists of the eligible publications, to identify potential publications that fulfill the eligibility criteria and did not appear in the initial searching procedure.
Data Extraction
Using the method described above (systematic review procedure), data extracted from the eligible studies as following: (a) First author and year of publication, (b) study design, location and funding, (c) patients characteristics (age, gender, BMI), (d) exercise/physical activity intervention, (e) diet intervention, and (f) outcomes. Also, PCD, CZ and ASV extracted the data suitable for meta-analysis, in relevant excel files.
Risk of Bias Assessment
We assessed the quality of the eligible studies, using the method described above (systematic review procedure). For the eligible RCT, we used the updated Risk of Bias 2 Cochrane library tool. 17 For the eligible CT and SAS we used the Research Triangle Institute Item Bank tool. 18
Data Synthesis
We identified six eligible studies19-24 that did not offer suitable data for a meta-analysis (i.e., reported changes from baseline in percentages) and therefore, we used a narrative data synthesis for these studies. For the remaining 44 eligible studies, we conducted random-effect model meta-analyses due to heterogeneity in participants’ characteristics, health status, diet and exercise interventions, duration of the intervention as well as tools of measurements. Continuous meta-analyses for the outcomes of depression, anxiety and depression + anxiety were conducted to calculate standardized mean differences (SMD; due to different measurement units). For RCT and CT eligible studies, we used post intervention data between an intervention and a control group. In case of eligible SAS, we used baseline and post intervention values. In cases that a standard error was given instead of a standard deviation (SD), we converted it into SD using the equation: SD = standard error*√n. 15 When SD were not reported and could not be estimated, we imputed SD using the coefficient of variation (CV), following previously published methodology. We calculated the mean CV from the remaining studies (CV = SD/Mean) and applied it to the mean of the study lacking SD information to obtain an imputed SD.15,25 Data that were reported in figures were extracted via the WebPlotDigitizer 5.2, 2024 software, 26 which displays >13000 citations in Google Scholar, has shown intercoder reliability of 99.7% and agreement of 98.7% with the values reported in original research 27 and it has been suggested to be used in data synthesis of systematic reviews. 28 For one eligible study, 29 we calculated the means and SD from medians and the 1st-3rd quartiles, according to: mean=(q1+m + q3)/3; SD=(q3-q1)/n(n). 30 For one eligible study, 31 we multiplied the mean value with −1, due to direction of the tool used for measuring the effect value, which was different from the measurement tools used in the other eligible studies included in meta-analyses. 15 For two eligible studies,31,32 we calculated SD from 95% confidence intervals (CI), using the following equation: SD = √n * (upper limit – lower limit)/1.96, due to the sample size was <100. 15
Fourteen eligible studies29,32-44 even though they are RCT, their data were treated as SAS, given that their control groups followed exercise and diet interventions and therefore, do not fulfill the eligibility criteria regarding the comparator element. To identify potential heterogeneity, we performed subgroup meta-analyses using combined interventions of diet and exercise/physical activity as following: (1) Exercise + low fat diet, (2) Exercise/physical activity + calorie restriction, (3) Exercise + control diet for carbohydrates (CHO), proteins and fat, (4) Exercise/physical activity + Mediterranean diet, (5) Physical activity + control diet for CHO, proteins and fat, (6) Exercise/physical activity + Paleolithic diet, (7) Exercise + high CHO diet, (8) Exercise + vitamin D supplementation, (9) Exercise + high protein diet and 10) Physical activity + corrective diet (i.e., personalized). Similarly, we performed subgroup analyses for the locations that the studies were conducted (i.e., Europe, Asia, North America, Australia, Africa), health status of the participants (i.e., healthy, metabolic syndrome, cardiovascular disease, cancer, diabetes and other diseases) and study design (RCT vs non-RCT). Subgroup analyses that violated meta-analysis principals 15 (i.e., included only one study), were not considered in the final interpretation. Publication bias was calculated with the Egger test, 45 while we also provide funnel plots in the supplement (Figures S9, S10). Finally, we performed meta-regression analyses using a random-effect model, the Cohen’s d effect size and restricted maximum likelihood (RELM) for the following moderators: sample size, BMI, age, sex and intervention duration (weeks). All meta-analyses and meta-regressions were conducted using the IBM SPSS statistics 31.0.2.0 software.
Evidence of Effectiveness and Interpretation
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) analysis, to assess the quality of evidence in meta-analyses that displayed statistically significant outcomes. 46 For the GRADE analysis, we considered risk of bias, inconsistency (heterogeneity), indirectness, imprecision and publication bias to reduce the quality of evidence, while we considered the magnitude of effect to increase the quality of evidence. The quality of evidence GRADE was defined as very low, low, moderate and high, while the magnitude of effect of each statistically significant meta-analysis was expressed as <0.2 = trivial, 0.2-0.5 = small, 0.5-0.8 = moderate and >0.8 = large, according to Cohen d effect size. 46 We determined a final interpretation of each statistically significant outcome using specific terminology as this suggested by the Cochrane handbook; by combining the quality of evidence we obtained from GRADE analysis and the magnitude of effect of each meta-analysis. 15
Results
A PRISMA checklist is given in supplementary materials, Table S5.
Searching and Selection Results
Figure 1 displays a PRISMA flow diagram showing the searching and selection processes outcomes. Specifically, the searching retrieved 5186 publications from which 1055 were duplicated and removed. From the 4131 remaining publications, we removed 1033 reviews, editorials, conference publications and protocols, 1393 non-interventional studies, 47 studies conducted in animals, 145 studies conducted in children and adolescences and 45 studies that used qualitative methods. As such, 1468 publications were screened in titles and abstracts to remove 1233 of them that did not fulfill the eligibility criteria. Consequently, 235 full texts were assessed for eligibility and 191 of them excluded as non-eligible, which led to 44 articles that included as eligible. We then screened 2268 citations that included in the reference lists of the 44 eligible articles, to include as eligible six more articles. As a result, 50 articles were finally included in the systematic review. PRISMA flow diagram.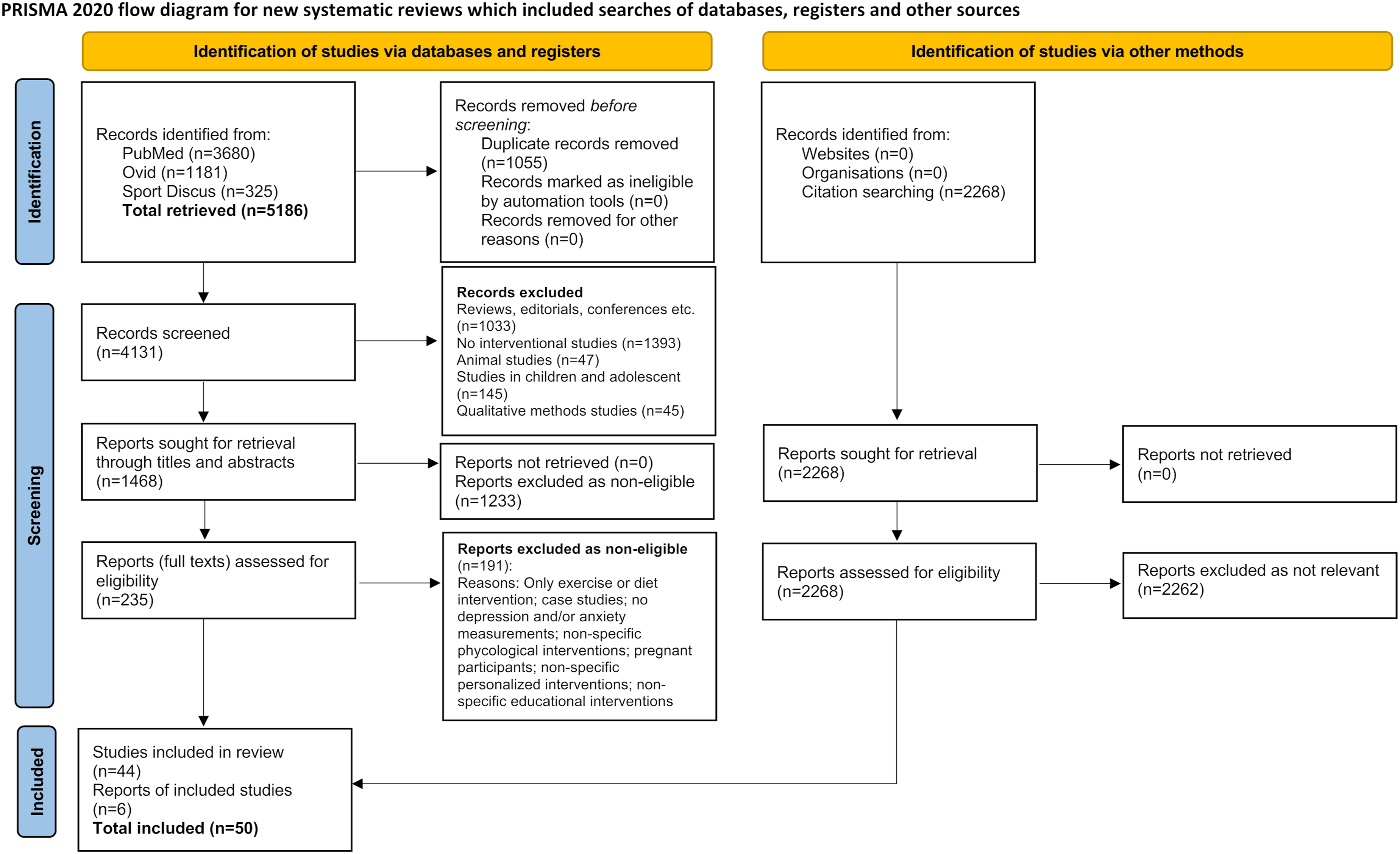
Study Characteristics
The characteristics of the eligible studies can be found in Table S1, in the supplement. The studies included in the systematic review showed an average of 26.1 weeks of intervention. They included participants with an average age of 55.31 years and an average BMI of 31.51 kg/m2. Thirty four percent of the eligible studies involved healthy participants, 10% patients with metabolic syndrome, 10% cardiovascular disease patients, 12% cancer patients, 14% diabetic participants, 4% polycystic ovary syndrome, 4% multiple sclerosis and 4% depressed patients, and 8% participants with various diseases. Twenty four percent of the eligible studies were conducted in Europe, 22% in Asia, 40% in North America, 12% in Australia and 2% in Africa. Eighteen eligible studies were non-RCT design studies,20,21,24,37,47-60 and 32 eligible studies were RCT, from which 13 eligible RCT29,32-36,38-44 were treated as SAS in the meta-analysis.
Risk of Bias Assessment Outcomes
Risk of bias assessment outcomes can be found in the supplement.
Data Synthesis Evidence of Effectiveness Outcomes and Interpretation
The narrative data synthesis of three eligible RCT19,22,23 that did not provide data for a meta-analysis revealed: (a) no effect of the combined energy restriction and aerobic + resistance exercise intervention on depression and anxiety, 19 (b) a reduction in depression and anxiety due to the combination of Mediterranean diet with aerobic exercise intervention 23 and (c) a reduction in depression and anxiety due to the combination of energy restriction, Mediterranean diet with resistance exercise intervention. 22 One 24 out of three eligible non-RCT showed an increase in depression due to the combined Mediterranean diet with physical activity intervention. The remaining two eligible non-RCT showed a reduction in anxiety and depression due to aerobic + resistance exercise in combination with hypocaloric Mediterranean diet intervention 20 and due to aerobic + resistance exercise in combination with anti-inflammatory plant-based diet. 21
Depression
Meta-analysis showed that the intervention significantly decreased depression [SMD = −0.59, confidence interval (CI) = −0.81, −0.36, I2 = 97%, P < 0.01]. Subgroup analysis between RCT and non-RCT revealed no differences in the effect estimate between groups (x2>0.05, Figure S3). For the type of intervention, subgroup analysis detected significant differences between groups (x2 = 0.04, Figure 2). Specifically, a reduction in depression due to “exercise + low fat diet” intervention was found (SMD = −1.58, CI = −2.48, −0.68, P < 0.01). Similarly, depression decreased due to “exercise/physical activity + calorie restriction” intervention (SMD = −0.34, CI = −0.64, −0.05, P = 0.02), “exercise + control diet in CHO, fat and proteins” (SMD = −0.44, CI = −0.66, −0.22, P < 0.01) and “exercise + high protein diet” (SMD = −0.59, CI = −0.81, −0.36, P < 0.01). No effect of “exercise + Mediterranean diet,” “exercise/physical activity + Paleolithic diet” and “exercise + vitamin D” on depression was found (P > 0.05), while the subgroup of “exercise + high CHO diet” included only one study and as such could not be considered.
15
Forest plot for depression outcome. Subgroup analysis for intervention type.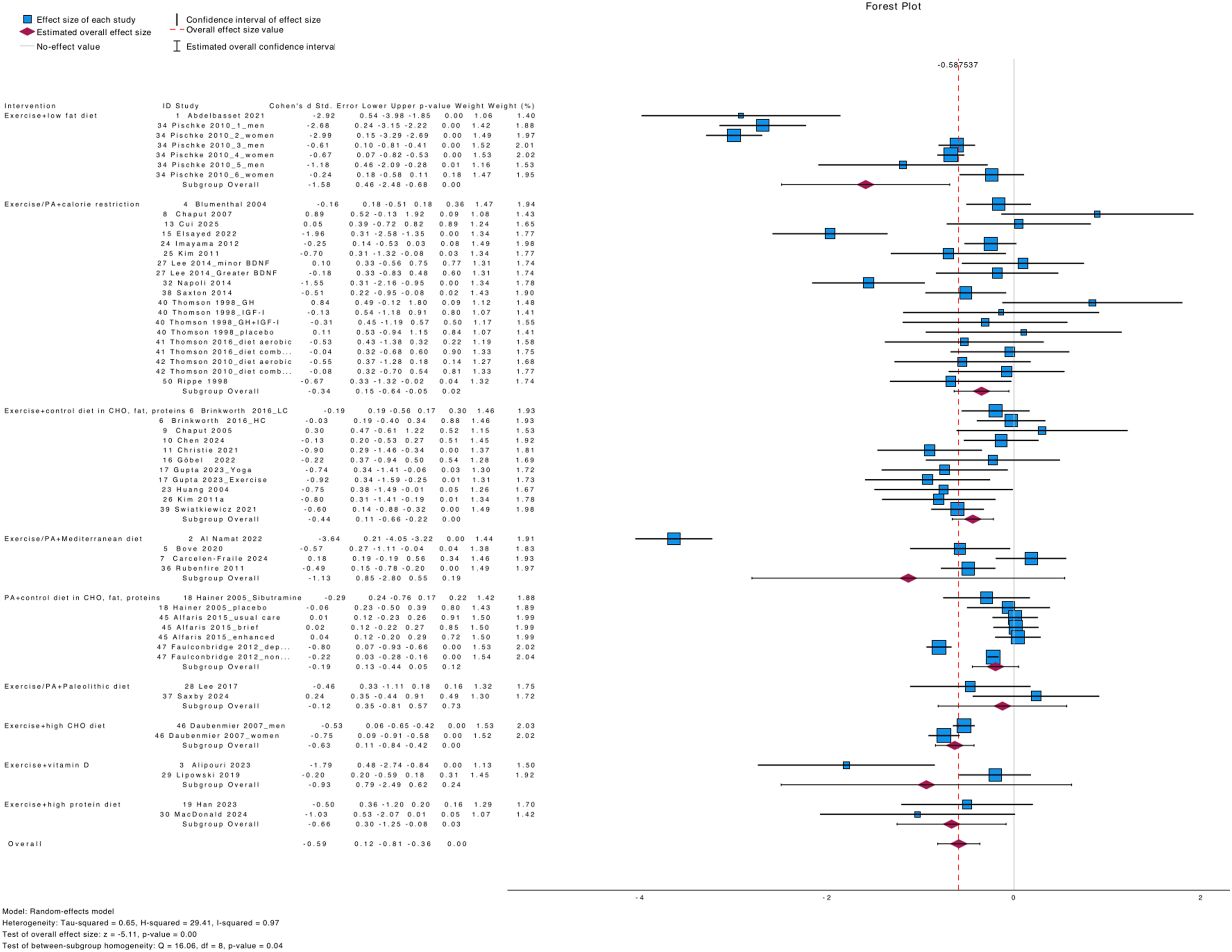
Subgroup analysis for the location that the eligible studies were conducted, revealed significant differences between groups (x2<0.01, Figure S4). Specifically, eligible studies that conducted in Europe (SMD = −0.75, CI = −1.44, −0.07, P = 0.03), in Asia (SMD = −0.69, CI = −1.22, −0.17, P = 0.01) and North America (SMD = −0.53, CI = −0.84, −0.21, P < 0.01), showed a reduction in depression due to intervention. Studies conducted in Australia showed no effect (P > 0.05), while we found only one study that conducted in Africa, which could not be considered as a subgroup. 15 We found no differences in depression between groups regarding the subgroup analysis for health status (x2>0.05, Figure S5). Specifically, the subgroup analysis revealed a significant reduction in depression in “metabolic syndrome” patients (SMD = −0.74, CI = −1.33, −0.14, P = 0.02), in “cardiovascular disease (CVD)” patients (SMD = −1.21, CI = −2.39, −0.03, P = 0.04), in cancer patients (SMD = −0.69, CI = −0.99, −0.39, P < 0.01), in “diabetic” patients (SMD = −0.40, CI = −0.65, −0.16, P < 0.01) and in “other disease” patients (SMD = −0.56, CI = −0.96, −0.15, P < 0.01). Subgroup analysis for “healthy” participants was not significant (P > 0.05).
Meta-regression analysis for sample size showed no significant outcomes (Wald x2 = 0.01, P > 0.05, Figures S11, S12). Meta-regression for BMI showed no association, (Wald x2 = 0.12, P > 0.05, Figure S13; Wald x2 = 0.08, P > 0.05, Figure S14; Wald x2 = 0.04, P > 0.05, Figure 15), while for age we also found no associations (Wald x2 = 0.05, P > 0.05, Figure S16; Wald x2 = 0.03, P > 0.05, Figure S17; Wald x2 = 0.01, P > 0.05, Figure 18). Similarly, analysis for male percentage showed no associations (Wald x2 = 0.64, P > 0.05, Figure S19; Wald x2 = 0.01, P > 0.05, Figure S20), as for female percentage (Wald x2 = 0.64, P > 0.05, Figure S21; Wald x2 = 0.01, P > 0.05, Figure S22). Finally, intervention duration was not associated with the effect estimate (Wald x2 = 0.05, P > 0.05, Figure S23).
Anxiety
Meta-analysis showed that the intervention significantly decreased anxiety (SMD = −0.44, CI = −0.78, −0.10, I2 = 91%, P = 0.01). Subgroup analysis between RCT and non-RCT revealed no differences in the effect estimate between groups (x2>0.05, Figure S6). For the type of intervention, subgroup analysis detected no significant differences between groups (x2>0.05, Figure 3). Specifically, only “exercise/physical activity + calorie restriction” intervention reduced anxiety (SMD = −0.18, CI = −0.35, −0.01, P = 0.03). The interventions of “exercise + control diet in CHO, fat and proteins,” “exercise/physical activity + Mediterranean diet” and “exercise/physical activity + Paleolithic diet” showed no effect (P > 0.05), while the intervention of “physical activity + corrective diet” included only one study and as such was not considered as a subgroup.
15
Forest plot for anxiety outcome. Subgroup analysis for intervention type.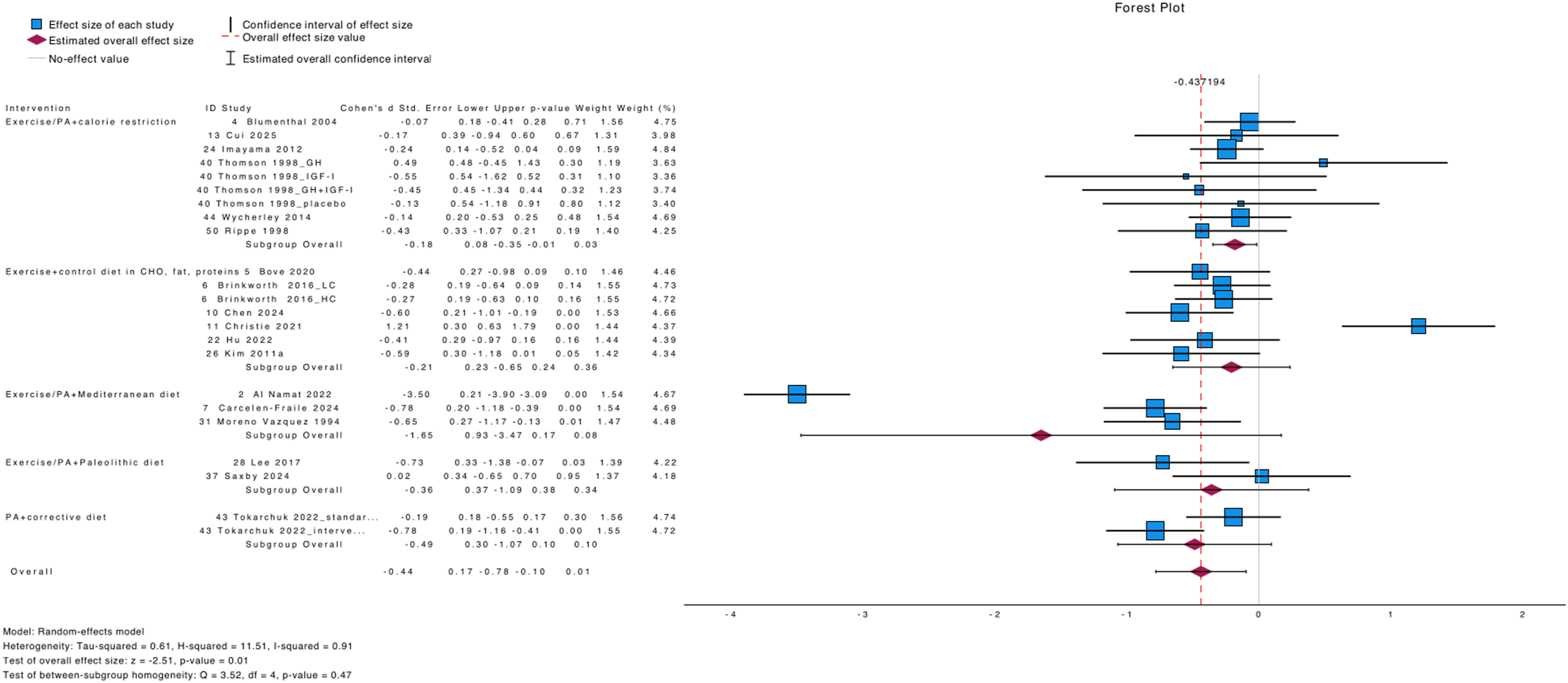
Regarding the subgroup analysis for the location that the studies were conducted, we found no differences between groups (x2>0.05, Figure S7). In specific, studies that were conducted in Europe (SMD = −1.06, CI = −2.04, −0.08, P = 0.03), in Asia (SMD = −0.50, CI = −0.77, −0.23, P < 0.01) and in Australia (SMD = −0.44, CI = −0.78, −0.10, P = 0.01), showed a significant reduction in anxiety due to intervention, while studies that were conducted in North America showed no effect (P > 0.05). Finally, we detected no significant differences between groups for subgroup analysis of health status (x2>0.05, Figure 4). Specifically, interventions in “healthy” participants (SMD = −0.37, CI = −0.56, −0.18, P < 0.01), in “diabetic” patients (SMD = −0.23, CI = −0.45, −0.02, P = 0.04) and in “other diseases” (SMD = −0.60, CI = −0.86, −0.34, P < 0.01), showed a reduction in anxiety, while interventions in “CVD” and “cancer” patients, showed no effect (P > 0.05). Forest plot for anxiety outcome. Subgroup analysis for health stratus.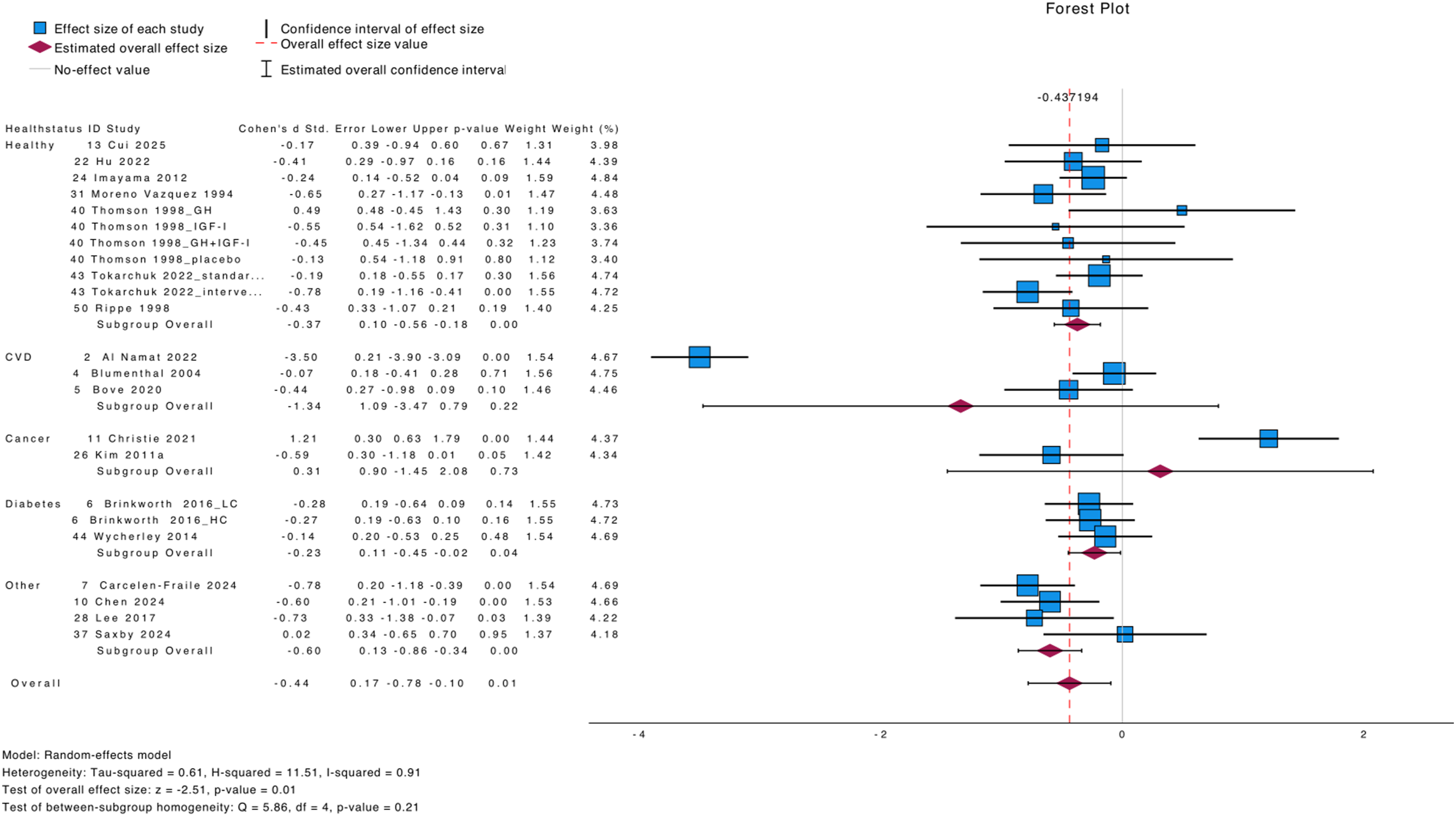
Meta-regression analysis for sample size experimental and control groups showed no significant outcomes (Wald x2 = 0.04, P > 0.05, Figure S24, Wald x2 = 0.33, P > 0.05, Figure S25, respectively). Meta-regression for BMI showed no association, (Wald x2 = 0.17, P > 0.05, Figure S26; Wald x2 = 0.01, P > 0.05, Figure S27; Wald x2 = 0.01, P > 0.05, Figure 28), while for age we also found no associations (Wald x2 = 0.05, P > 0.05, Figure S29; Wald x2 = 0.01, P > 0.05, Figure S30; Wald x2 = 0.01, P > 0.05, Figure 31). Similarly, analysis for male percentage showed no associations (Wald x2 = 0.04, P > 0.05, Figure S32; Wald x2 = 0.01, P > 0.05, Figure S33), as for female percentage Wald x2 = 0.05, P > 0.05, Figure S34; Wald x2 = 0.01, P > 0.05, Figure S35). Finally, intervention duration was not associated with the effect estimate (Wald x2 = 0.03, P > 0.05, Figure S36).
Depression and Anxiety
Meta-analysis for depression and anxiety as one outcome, revealed no effect of the intervention (P > 0.05; Figure S8).
GRADE Analysis Outcomes
Meta-Analysis and GRADE Analysis Outcome.
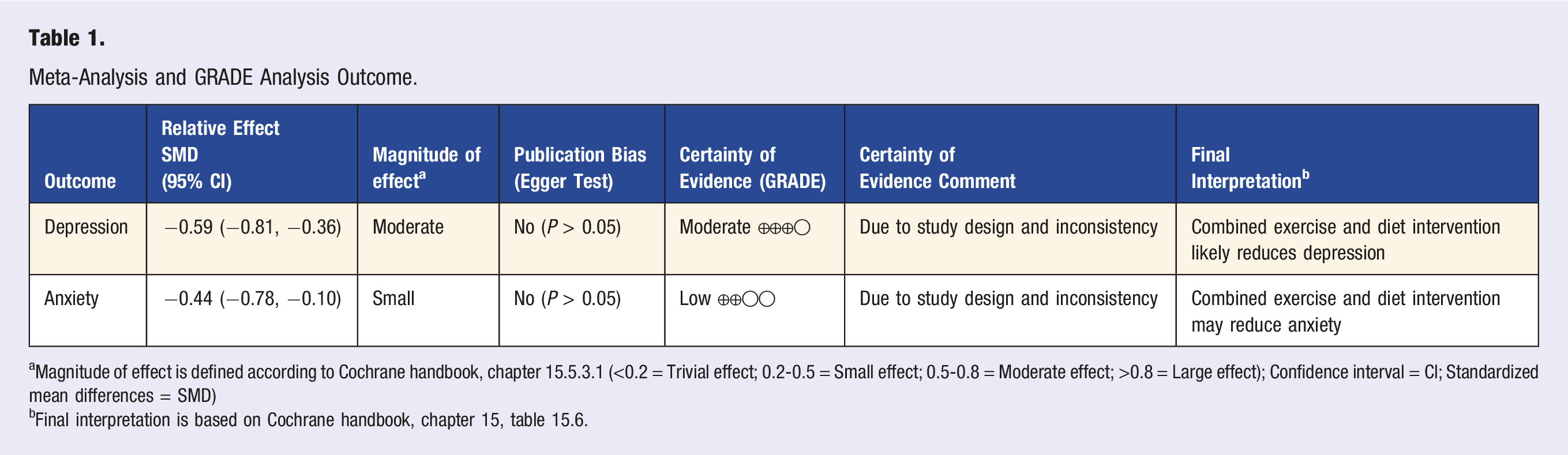
aMagnitude of effect is defined according to Cochrane handbook, chapter 15.5.3.1 (<0.2 = Trivial effect; 0.2-0.5 = Small effect; 0.5-0.8 = Moderate effect; >0.8 = Large effect); Confidence interval = CI; Standardized mean differences = SMD)
bFinal interpretation is based on Cochrane handbook, chapter 15, table 15.6.
Discussion
The aim of the current systematic review and meta-analysis was to examine the combined effects of diet and physical activity interventions on depression and anxiety in adult populations of any health status.
Completeness and Applicability of Evidence
We found enough evidence to examine the effects of combined exercise and diet interventions on depression and anxiety outcomes, given that the overall sample size of the meta-analyses was >6000 and >950 participants, respectively. According to the Cochrane handbook, these sample sizes are larger than a sample size of a typical RCT for these populations, and therefore, are considered as optimal sample sizes. 15 On the other hand, the sample size for the depression + anxiety outcome was relatively small (n = 103), given that only two studies included in this meta-analysis, which showed no effect of the intervention and therefore, no further analysis was considered, for this outcome.
We found moderate quality of evidence and a large effect (SMD = −1.58) that the combination of “exercise + low fat diet” likely reduces depression. Previous evidence demonstrates that exercise and physical activity can reduce depression, especially in clinical populations such as hypertensive and CVD patients. 7 Indeed, in our subgroup analysis regarding the health status of the participants, the healthy displayed no effect (P > 0.05), while the clinical populations including metabolic syndrome, CVD, cancer and diabetes patients, showed a significant reduction in depression due to intervention (P < 0.05). However, the subgroup analysis suggests inconsistency between subgroups (x2<0.05). This finding may support a previous reported opinion that exercise and physical activity can be used as therapeutic means for acute and chronic depression. 7 The mechanism that exercise and physical activity reduce depression, includes the opioid system, which plays a key role in mediating analgesia and social attachment, through the production of β-endorphin.61,62 Regarding the low fat diet, previous evidence is conflicting whether can affect depression or not. Even though some data showed that diet low in fat may reduce depression,63,64 other data showed that low cholesterol levels—that usually arise from high fat diet—are associated with high risk of depression, 65 due to reduction of serotonin levels. 66 A recent meta-analysis however, demonstrated that low fat diet has a slight beneficial effect on depression in mentally healthy individuals. 67 Therefore, considering our finding in the current meta-analysis, we may support that the combination of exercise and low fat diet likely reduces depression in a synergistic manner, especially in clinical populations.
We also detected that the combination of “exercise/physical activity + calorie restriction” likely reduces depression. Previous evidence indicates that reduced neurogenesis is implicated in the development of depression, 68 while calorie restriction promotes survival of newly generated cells in the hippocampus 69 and thus, reduces depressive symptoms. Also, calorie restriction enhances cerebral blood flow, which is a protective effect against depression, due to neurovascular activity that is associated with decreased mammalian target of rapamycin. 70 These calorie restriction favorable effects on depression however, may be considered as short-term effects, due to calorie restriction may also activate the hypothalamic–pituitary–adrenal axis, which increases glucocorticoids and ameliorates depressive symptoms. 68 Considering both, the favorable effects of exercise/physical activity on depression described above and the favorable effects of calorie restriction on depressive symptoms, we may support that “exercise/physical activity + calorie restriction” likely reduces depression.
We also found that the combination of exercise/physical activity and control balanced diets in specific amounts of CHO, fats and proteins, likely reduces depression. Specific balanced diets in macronutrients (e.g., 65% CHO, 15% fat, 30% protein) have been shown to reduce depression, however, given the diversity of diets the existing data are somewhat conflicting. 71 Actually, it depends on the quality of macronutrients included in these diets, to positively affect depression symptoms. 71 For instance, diets rich in saturated of both fats and proteins may not have a beneficial effect on depression. 71 Therefore, balanced diets in macronutrients are only suggested, if the quality of macronutrients is sufficient (e.g., unsaturated fats and proteins). In this light, we may support that the combination of exercise/physical activity and control balanced diets in specific amounts of CHO, fats and proteins likely reduces depression, if the planned diets do not include saturated fats and proteins.
Another finding of our meta-analysis is that the combination of “exercise + high protein diet” likely reduces depression. Indeed, consumption of adequate amounts of proteins may offer essential amino acids, like tryptophan, that may generate mood-stabilizing neurotransmitters such as serotonin, dopamine, and norepinephrine, which may reduce depression. 10 However, recent evidence suggests that only plant-based protein consumption is associated with lower levels of depression, whereas animal proteins consumption may not. 72 Furthermore, we found that the combination of exercise/physical activity and diet interventions may reduce anxiety. A recent meta-analysis showed that exercise participation is associated with reduced levels of anxiety, especially mid-body exercises. 73 Exercise releases neurotransmitters crossing the blood brain barrier to mediate brain-derived neurotrophic factor expression, stimulating hippocampal neurogenesis. This improves mood control and thus, reduces anxiety. 74 Another potential mechanism to reduce anxiety through exercise participation is the stimulation of monoamines that generate pleasure and satisfaction, while reducing fatigue.75,76 These exercise effects in combination with diets low in fat and sugar, enough in tryptophan intake and adequate in CHO, may reduce anxiety. 77
Our finding that the combination of exercise/physical activity and either Mediterranean or Paleolithic diet has no effect on depression, may be due to Mediterranean and Paleolithic diets were initially created to reduce risk for non-communicable diseases such as CVD, type 2 diabetes and metabolic syndrome and not for affecting mood state. Similarly, our finding that the combination of exercise/physical activity and diet interventions showed no effect on depression in Australian populations, may be random. To the best of our knowledge there is no reason for this population to not responding to this combined intervention. Recent evidence also showed that Australians may decrease through physical activity participation depressive and anxiety symptoms by 4.4% and 6.4%, respectively. 78
Strengths and Limitations
A strength of our systematic review is our approach to use the Cochrane handbook recommendations to interpret the outcomes of our meta-analyses, based on both the quality of evidence (GRADE analysis) and the magnitude of effect of each meta-analysis. 15 A limitation of our study is that the duration of the interventions, participants’ characteristics and types of interventions, varied among the eligible studies, however, we used a random-effect model meta-analysis that is suitable for heterogenous data, 15 while we considered heterogeneity in GRADE analysis, to reduce the quality of evidence. In this regard, we framed as far as was possible the type of the interventions used by the eligible studies. Another limitation is that the effects of the combined exercise and diet interventions included in our meta-analysis, may represent independent effects of either the exercise or the diet interventions. This however, cannot be calculated in the current meta-analysis, while the rationale of our study was to detect the combined effects of exercise and diet interventions. Also, we included both RCT and non-RCT studies in our meta-analysis, which may pose a risk of bias due to the major differences in study design and quality between RCT and non-RCT. Nevertheless, we included a subgroup analysis between RCT and non-RCT for each outcome, which showed no differences in the effect estimate between them. Furthermore, we could not consider potential medicines taken by the clinical populations included in the meta-analyses, due to poor reporting by the included studies. Finally, we could have considered including only RCT in our systematic review research question, which might have increased the overall quality of the evidence generated by our meta-analysis. However, this would have constituted a major deviation from our published protocol.
Deviation From the Published Protocol
We report no important deviations from the published protocol.
Conclusions and Implications for Practice or Research
We conclude the following: (a) The combination of “exercise + low fat diet,” “exercise/physical activity + calorie restriction,” “exercise + control diet in CHO, fat and proteins” and “exercise + high protein diet” likely reduce depression. (b) The combination of exercise/physical activity and diet interventions may reduce anxiety. (c) The combination of exercise/physical activity and either Mediterranean or Paleolithic diet has no effect on depression. (d) The combination of exercise/physical activity and diet interventions showed no effect on depression in Australian populations.
Research implications of the findings of our meta-analysis include future RCT studies that will examine the effects of specific exercise interventions (e.g., aerobic, resistance etc.), along with low fat diets or calorie restriction or high protein diets, given that in our meta-analysis the data were not suitable to distinguish the type of exercise in the subgroup analysis. Also, the duration of the intervention should be examined to identify potential dose-response effects of the interventions.
Supplemental Material
Supplemental Material - Combined Effects of Diet and Physical Activity Interventions on Depression and Anxiety. A Systematic Review and Meta-Analysis
Supplemental Material for Combined Effects of Diet and Physical Activity Interventions on Depression and Anxiety. A Systematic Review and Meta-Analysis by Petros C. Dinas, 5104 Research Group, Constantine Zalagkitis Marianthi Karaventza, Nikolaos Ntelis, Maria Papagianni, Aristidis S. Veskoukis, George S. Metsios in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Not applicable.
Data Availability Statement
The data used for the meta-analyses are available by the authors upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.