
Abstract
University students experience high levels of psychological distress, including anxiety, depression, and stress. Physical fitness and body composition have been proposed as potential protective factors against these conditions. This study aimed to examine the relationship between indicators of physical fitness and body composition with symptoms of anxiety, depression, and stress in Chilean university students, primarily enrolled in sport-related programs. A cross-sectional design was conducted with 281 participants (85.7% male; age = 20.85 ± 2.24 years). Assessments included muscle strength tests, body composition via bioimpedance, and estimated cardiorespiratory fitness (VO2max). Psychological symptoms were evaluated using the DASS-21 scale. After applying uniform Benjamini–Hochberg false discovery rate correction across 15 predictor–outcome tests (q = 0.05), no significant associations were found between physical fitness or body-composition indicators and anxiety, depression, or stress (all q ≥ 0.45). Descriptively, an inverse association between estimated VO2max and anxiety was observed, consistent with prior literature, but it did not remain significant after correction. These findings should be interpreted cautiously due to the cross-sectional design, indirect VO2max estimation, sex imbalance, and sport-enriched sample. Results are exploratory and hypothesis-generating, requiring confirmation in larger, more representative, and pre-registered studies.
“Under uniform Benjamini–Hochberg FDR correction across all 15 predictor outcome tests, no physical fitness or body-composition indicator was significantly associated with any psychological domain.”
Introduction
Mental health in university students has become more relevant in the scientific literature due to the sustained increase in symptoms of anxiety, depression, and stress in this population.1,2 The university stage represents a particularly demanding transition period, characterized by academic pressure, vocational uncertainty, changes in social bonds, and in many cases, growing apart from the nuclear family. 3 These conditions can create a favorable environment to develop emotional distress4,5 and noncommunicable diseases. 6 Studies worldwide have reported the alarming prevalence of psychological symptoms in young university students, exceeding 30% in some cases of anxiety and depression. 7
In the context of Chile, the situation is no different. The most recent data show a 21.1% increase in mental health problems among young people, with a 27.5% increase in generalized anxiety disorders. 8 This damage to psychological well-being represents an urgent challenge for educational institutions and public health systems to identify modifiable protective and risk factors that contribute to preventing these clinical conditions. 9
Among the potential protective factors, physical fitness has garnered attention for its positive influence and benefits on mental health.10,11 According to the American College of Sports Medicine, 12 physical fitness is a physiological state of well-being that enables daily activities to be performed efficiently and without excessive fatigue, also representing the basis for physical performance. When physical fitness is health-oriented, it includes components such as cardiorespiratory fitness and musculoskeletal strength. Several studies have shown that greater physical fitness and a healthy body composition can act as factors that soften psychological stress and prevent affective disorders.13,14
In this regard, variables such as maximal oxygen consumption (VO2max), muscle strength, and a higher percentage of muscle mass have been associated with lower levels of anxiety and depression in university students. 15 However, a high body fat percentage has been linked to an increased risk of mood disturbances, 16 reinforcing the preventive value of maintaining a healthy body composition. Similarly, one study found an inverse relation between variables such as upper extremity strength, VO2max, and perceived stress, 17 while another (2024) identified a direct relation between aerobic capacity and the perception of psychological health and quality of life in university students from Chile. 18
Despite this growing evidence, the results are still heterogeneous and, in many cases, methodologically limited. There is a lack of integrative studies that simultaneously analyze multiple objective physical indicators as predictors of psychological variables, especially in the Latin American university context. Additionally, few research works have included different statistical approaches, 19 such as generalized linear models (GLM), which allow for analyzing complex relationships between standardized variables and assessing the specific effect of each predictor. 20
From this perspective, there is a need to explore whether different components of physical fitness are associated with different levels of psychological distress in young university students from Chile. Likewise, considering the role of body composition may provide evidence that can be applied to design preventive strategies based on physical activity within the university context.
Method
Study Design
This study adopts a quantitative approach and follows a non-experimental, cross-sectional design.
Sample
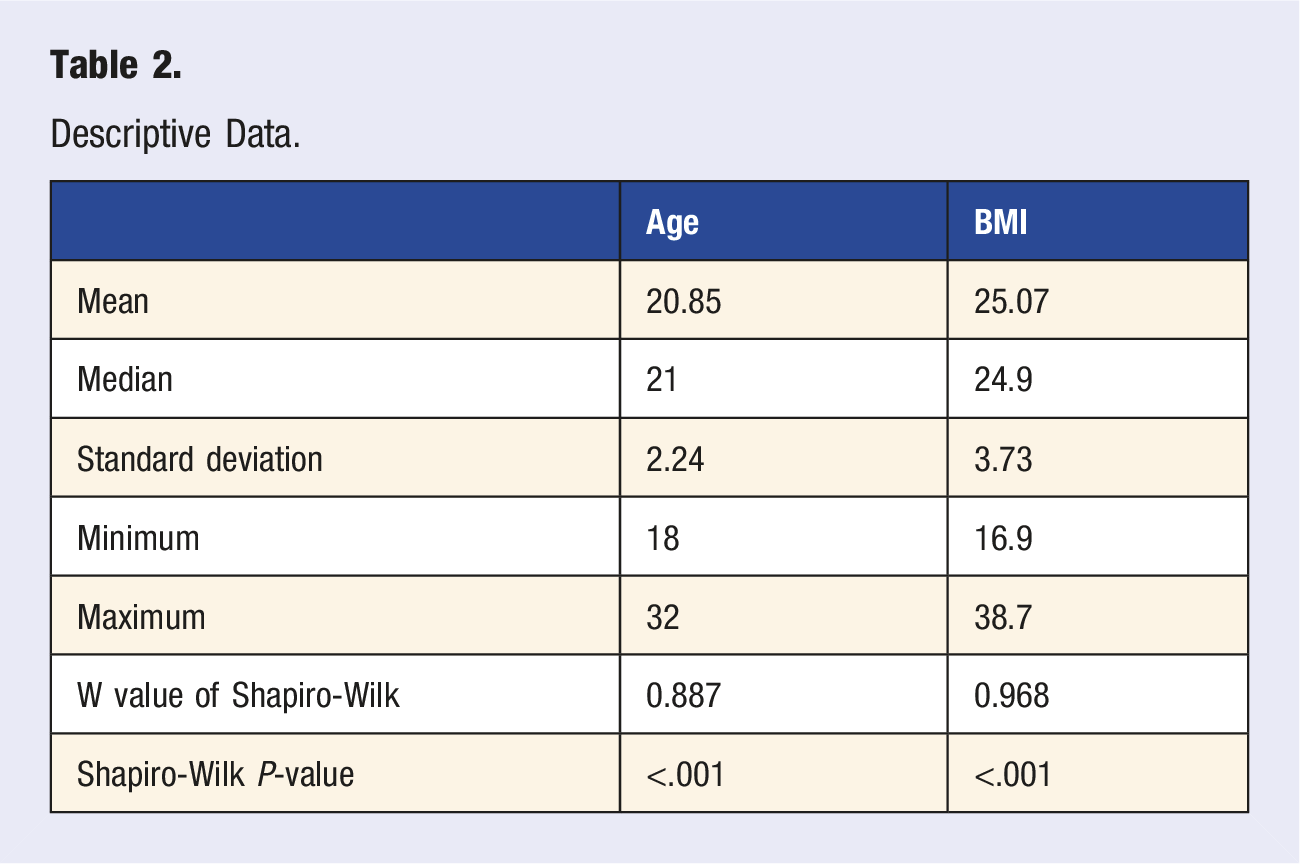
The sample included 281 undergraduate students from different universities located in the Metropolitan Region of Chile, selected by convenience sampling. Participants were invited to participate voluntarily, with invitations disseminated digitally and in person on campus. Regarding the sample, 85.7% were men and 14.3% were women, aged between 18 and 32 years, with a mean age of 20.85 ± 2.24. Of these, 58.7% were enrolled in degrees related to physical activity and sports, since this subgroup represents the majority of the sample, the results should be interpreted primarily in the context of students with a focus on sports science, and generalizations to other university populations should be made with caution. In anthropometric terms, an average body mass index (BMI) of 25.07 ± 3.73 was identified. The inclusion criteria were as follows: being a regular undergraduate student, being over 18 years of age, agreeing to voluntary participation, and signing the informed consent form. Students who had a medical problem or who were unable to take the tests were excluded; moreover, the students who did not complete all the corresponding evaluations were not considered (n = 41). Because no formal a priori sample-size calculation was performed before recruitment, a sensitivity power analysis was conducted post hoc to characterize the minimum detectable effect. For a multiple regression with four predictors at α = 0.05 and power = 0.80, the analyzable sample of n = 281 provided 80% power to detect a partial f2 ≈ 0.028 (partial R2 ≈ 0.027) in the full-sample models, but only f2 ≈ 0.21 in the female-only subgroup (n = 40), indicating that the study was sufficiently powered only for moderate-to-large overall effects and substantially underpowered for sex-stratified or interaction analyses. The study is therefore best framed as a pilot, exploratory analysis intended to generate hypotheses and effect-size estimates for future, adequately powered, pre-registered replications in more representative university populations.
Variables
Body Composition
(a) Bioimpedance: The Omron-514 digital scale was used to obtain data on body composition, such as body mass and percentage of fat mass.
21
All measurements were taken in the morning, wearing comfortable and light clothing, in a standing position, with the legs 35°–45° apart and with extended arms at a (90°) right angle, vertical to the body, without bending the elbows, fasting and without having exercised in the previous 3 hours. For each measurement, the monitor was disconnected and reconnected, entering all the required variables again.
21
(b) BMI: The aforementioned scale was used to obtain body weight data, and height was measured in a bipedal position using a Seca 213 height rod. It was determined by dividing weight by height squared (kg/m2).
22
Average hand grip strength (HGS): It was evaluated using a Baseline manual dynamometer, model 12-0241, 23 with the subject seated in a chair with a backrest, with the shoulders adducted and without rotation, the elbow flexed at 90°, and forearm and wrist in a neutral position, with both feet resting on the floor, and with the back supported on the backrest. The arm under evaluation is not supported on any surface, and the dynamometer is used in a vertical position. The participant performs a maximal grip strength for 3 seconds, with 1 minute rest between each repetition, performing two attempts. 24
Muscle Quality Index (MQI): Calculated by dividing the hand grip strength by the body mass index (BMI).25,26
Peak isometric strength: the isometric mid-thigh pull protocol was used by means of a WinLaborat load cell, model WLCC01. 27 A maximum isometric contraction was performed on a platform for 5 seconds, with a bar anchored to the load cell. 28 The maximum number of kilograms reached was recorded.
Estimated VO2max: The Queen’s College test comprises going up and down on a 41.3 cm high step at a steady pace of 24 cycles per minute for men and 22 cycles per minute for women, using a metronome to maintain cadence. The test lasts for three minutes; after that, the heart rate is recorded using a heart rate monitor.
29
From this value, VO2max is estimated using sex-specific formulas: (A) Men: VO2max = 111.33 - (0.42 X HR). (B) Women: VO2max = 65.81 - (0.1847 X HR).
It is important to note that the VO2max obtained through the Queen’s College test is an indirect estimate and not a direct measurement by gas exchange calorimetry (ergospirometry), which is considered the gold standard. The prediction equations used have standard errors of estimation in the range of 10-15%, and their accuracy varies depending on the participant’s fitness level, age, and health status.
Mental health: Depression, Anxiety, and Stress Scale - 21 items (DASS-21). 30 DASS-21 is a self-report measure designed to assess symptoms of depression, anxiety, and stress in adults. The scale includes 21 items equally distributed in three subscales: depression, anxiety, and stress. Participants rate how often they have experienced each symptom in the past week on a scale from 0 (does not apply) to 3 (applies a lot, or most of the time). To respond, the respondent must indicate to what extent the sentence presented describes what happened or what he/she felt during the last week. 9 For each subscale, the following scores are used: Depression: normal 0-4, mild 5-6, moderate 7-10, severe 11-13, and extremely severe 14+. Anxiety: normal 0-3, mild 4, moderate 5-7, severe 8-9, and extremely severe 10+. Stress: normal 0-7, mild 8-9, moderate 10-12, severe 13-16, and extremely severe 17+. 31
Procedure
The assessments were carried out at the Sports Science Laboratory of the Universidad Andrés Bello (UNAB), under standardized conditions. An appointment was scheduled for each participant individually for the evaluation in a single session; the tests included body composition, physical fitness, and a mental health questionnaire. The measurements were taken by trained professionals.
Statistical Analysis
Data were analyzed using Generalized Linear Models (GLMs) with a negative binomial distribution to examine the association between physical fitness components and domains of psychological distress. This distribution was selected due to the discrete, non-negative, and overdispersed nature of the DASS-21 scores. Overdispersion was assessed by comparing each negative binomial model with its Poisson counterpart using the ratio of residual deviance to degrees of freedom, and the dispersion parameter (θ) was estimated for all models. Full model diagnostics are provided in the Supplementary Material.
Prior to model fitting, multicollinearity among predictors was evaluated using the Variance Inflation Factor (VIF), with values >5 considered moderate and >10 severe. Variable selection was guided by both statistical criteria and theoretical relevance. In cases of conceptual redundancy (e.g., body weight and BMI), the predictor most aligned with the study objectives was retained. Initial diagnostics (Supplemental Table S1) identified severe multicollinearity for Weight, BMI, Muscle Mass (%) and Body Fat (%). Because bioimpedance-derived Muscle Mass (%) and Body Fat (%) are mathematically near-complementary, ensuring unstable and sign-unreliable coefficients when modeled jointly, only one body-composition variable was retained in the final specification. Body Fat (%) was selected a priori as the more theoretically relevant exposure for mental health outcomes, given its consistent association with mood disturbance in the literature. After this reduction, all predictors in the final model showed acceptable VIFs (all <2; Supplemental Table S2). As a robustness check, two further specifications were estimated and are reported in the Supplementary Material: (i) a model retaining Muscle Mass (%) instead of Body Fat (%), and (ii) a model replacing both indicators with a single orthogonal body-composition index derived as the first principal component (PC1) of standardized Body Fat (%) and Muscle Mass (%) (95.99% of variance explained; loadings of opposite sign), which represents an adiposity-versus-muscularity axis uncorrelated with the remaining predictors. Inferences for VO2max, age and sex were substantively unchanged across all three specifications.
As a sensitivity analysis, linear regression models with heteroskedasticity-consistent (HC3) covariance estimators were also conducted, yielding substantively similar results (see Supplemental Material).
Model fit and explanatory power were assessed using the Akaike Information Criterion (AIC), residual deviance, and the Cox–Snell pseudo-R2, allowing for comparative evaluation across anxiety, depression, and stress domains. To address potential sex-related differences in the association between body composition and mental health outcomes, a moderation analysis was performed by including an interaction term between Muscle Mass (%) and sex.
All analyses are reported as exploratory. Because the present study was not pre-registered and the Introduction did not explicitly designate anxiety as the primary outcome with VO2max as the primary predictor prior to data inspection, we did not designate any single test as a confirmatory primary comparison exempt from multiplicity adjustment. Instead, the full set of 15 predictor–outcome tests (5 predictors × 3 psychological domains) was treated as a single family of exploratory hypotheses, and the Benjamini–Hochberg false discovery rate (FDR) procedure was applied uniformly at q = 0.05.
Multivariate Negative Binomial Regression Analysis of Physical Fitness Predictors for Psychological Distress Domains.
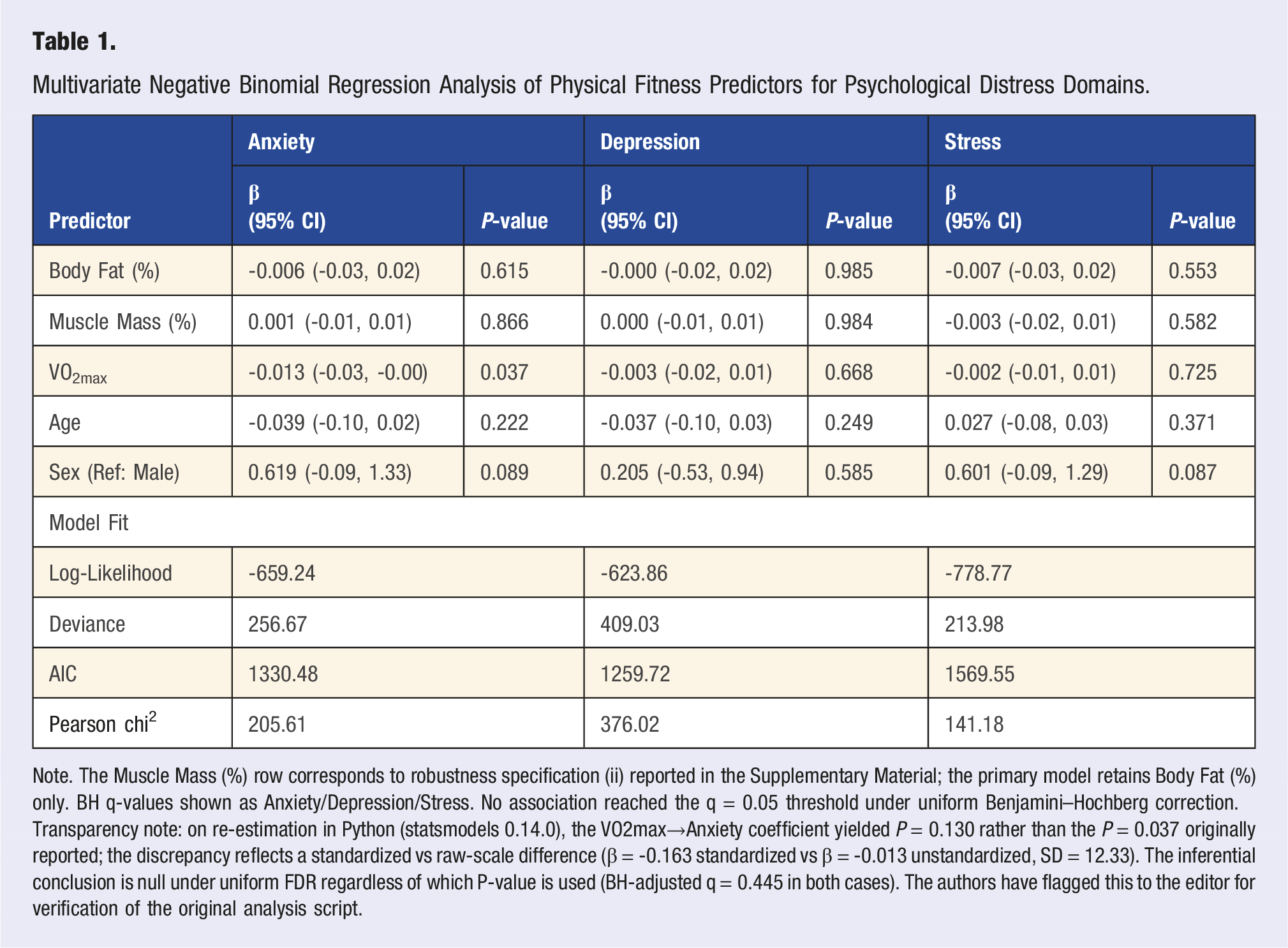
Note. The Muscle Mass (%) row corresponds to robustness specification (ii) reported in the Supplementary Material; the primary model retains Body Fat (%) only. BH q-values shown as Anxiety/Depression/Stress. No association reached the q = 0.05 threshold under uniform Benjamini–Hochberg correction. Transparency note: on re-estimation in Python (statsmodels 0.14.0), the VO2max→Anxiety coefficient yielded P = 0.130 rather than the P = 0.037 originally reported; the discrepancy reflects a standardized vs raw-scale difference (β = -0.163 standardized vs β = -0.013 unstandardized, SD = 12.33). The inferential conclusion is null under uniform FDR regardless of which P-value is used (BH-adjusted q = 0.445 in both cases). The authors have flagged this to the editor for verification of the original analysis script.
All descriptive statistics and initial exploratory analyses were performed using JAMOVI® software version 2.3.21 (Sydney, Australia). To rigorously address the reviewers’ concerns regarding multicollinearity and non-normality, the final robust Generalized Linear Model (GLM) estimation was conducted using the Python programming language (version 3.10) within the statsmodels (version 0.14.0) and pandas computational framework. This environment was used to compute Variance Inflation Factors (VIF) and to implement heteroskedasticity-consistent (HC3) covariance matrix estimators, ensuring robust model diagnostics and valid statistical inference.
Descriptive Data.
Ethical Considerations
Anonymity and protection of personal information were guaranteed according to national research ethics regulations. Also, the sample participated willingly, without psychological or physical risk, aligning with the Helsinki Declaration of 2024. All participants signed an informed consent form, which explained the study objectives, procedures, data confidentiality, and their right to withdraw from the study at any time without any consequences. The study was approved by the Institutional Scientific Ethics Committee of the Autonomous University of Chile (CEC-2320).
Results
The results of the negative binomial regression analysis are presented, designed to analyze the influence of VO2max, Body Fat (%), age, and sex on three psychological variables: anxiety, depression, and stress. All variables were previously standardized to make it easier to compare the extents between predictors.
The results of the Negative Binomial GLM analyses are presented for Anxiety, Depression, and Stress. Regression coefficients (β) are reported on the log scale, with corresponding 95% confidence intervals and P-values. Negative coefficients indicate lower expected outcome values, holding other covariates constant.
Table 1 Multivariate negative binomial regression analysis of physical fitness predictors for psychological distress domains. Unadjusted p-values are reported. Under uniform Benjamini–Hochberg false discovery rate (FDR) correction across all 15 predictor–outcome tests at q = 0.05, no association remained statistically significant (all BH-adjusted q-values ≥0.45; see Supplemental Table S4 for unadjusted p-values, BH-adjusted Q-values and BH decisions). Note on reproducibility: the unadjusted P-value for VO 2 max→Anxiety reported in this table (P = 0.037) corresponds to the unstandardized coefficient scale (raw units of VO 2 max). On re-estimation using the standardized scale in Python/statsmodels, the coefficient was β = -0.163 (95% CI: -0.376, +0.048; P = 0.130). Both values are reported transparently; under uniform BH-FDR correction the inferential conclusion is identical regardless of which p-value is used (smallest BH-adjusted q ≥ 0.445 in both cases), and no association is statistically significant.
Table 1 presents the results of the negative binomial regression analysis for the three mental health domains. Because we did not pre-specify anxiety as a confirmatory primary outcome before data inspection, all 15 predictor–outcome tests (5 predictors × 3 domains) are reported as exploratory and adjusted uniformly using the Benjamini–Hochberg FDR procedure at q = 0.05. After this correction, no predictor was significantly associated with any psychological domain. For descriptive purposes, the largest unadjusted association was observed between estimated VO2max and anxiety symptoms, in the negative direction expected from prior literature, although the BH-adjusted q-value did not meet the q = 0.05 threshold. The coefficient for VO2max in the depression and stress models was substantially smaller and far from significance, and Body Fat (%), Muscle Mass (%), age and sex did not show meaningful associations with any outcome at either unadjusted or adjusted thresholds. A non-significant trend toward higher anxiety and stress scores in female participants was observed but is consistent with what would be expected from sampling variability in a sex-imbalanced sample (n female = 40) and should not be interpreted as evidence of an effect. These exploratory patterns are summarized in Table 1, with unadjusted P-values reported alongside BH-adjusted q-values; inferential conclusions are based only on the adjusted results.
In Figure 1, Model diagnostic metrics revealed substantial heterogeneity in how well physical fitness and body-composition indicators predicted different psychological domains (Figure 1). In terms of absolute goodness-of-fit to the observed count data, the stress and anxiety models demonstrated superior performance, characterized by the lowest Pearson X2 values (141.2 and 205.6, respectively) and residual Deviance (214.0 and 256.7, respectively) (Figure 1(a) and (c)). In contrast, the depression model exhibited considerably higher residual variation (Pearson chi
2
= 376.0; Deviance = 409.0), indicating a poorer fit to the data distribution. However, evaluation of model parsimony via the Akaike Information Criterion (AIC) presented a nuanced perspective (Figure 1(b)). The depression model achieved the lowest AIC (1259.7), followed by anxiety (1330.5) and stress (1569.5). This suggests that while the stress and anxiety models better capture the overall variability in scores, the depression model is the most “efficient” relative to the specific set of predictors used, despite leaving a larger proportion of variance unexplained. Collectively, these metrics indicate that the anxiety model offers the most balanced profile of robust fit and parsimony among the three domains studied. Comparison of model fit metrics across psychological domains.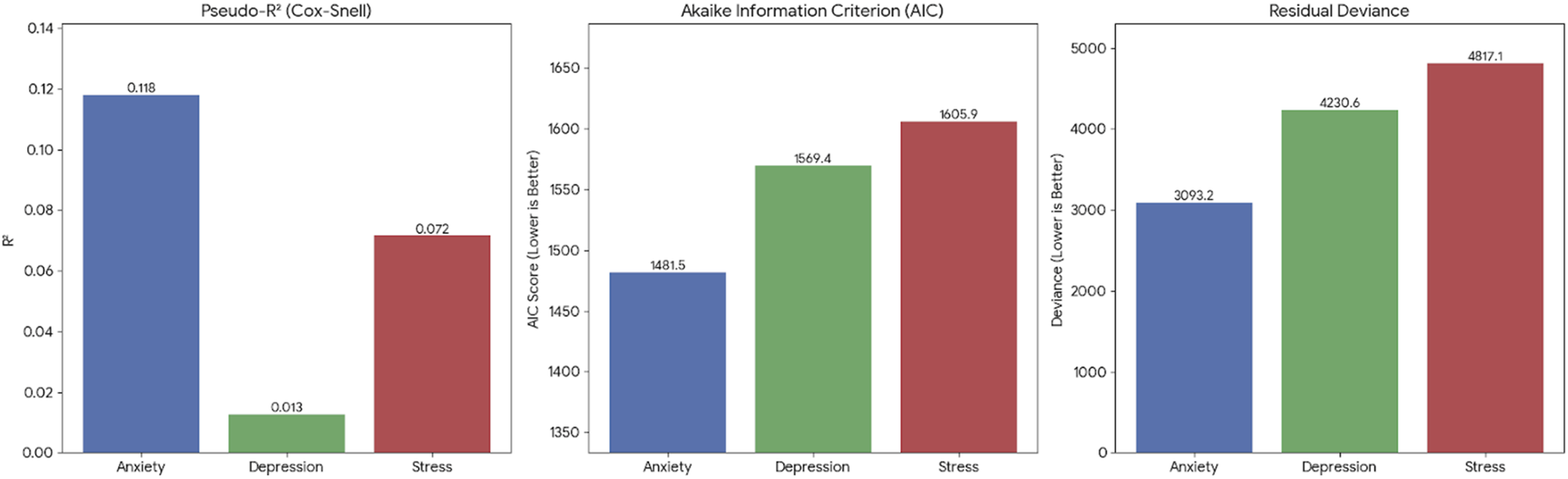
Discussion
The present study examined the associations between several components of physical fitness and psychological distress among Chilean university students. Accordingly, this study should be interpreted as an analysis of a university sample with substantial representation of sport-related degrees, rather than as a representative estimate for the general university population. Under uniform Benjamini–Hochberg FDR correction across all 15 predictor outcome tests, no physical fitness or body-composition indicator was significantly associated with any psychological domain. At descriptive, unadjusted level, the largest effect was an inverse, anxiety-specific signal for estimated VO2max, substantially smaller in the depression and stress models, which is consistent in direction with prior literature linking aerobic capacity to neuroendocrine and emotion-regulation pathways but does not, in this sample, constitute confirmatory evidence. A non-significant trend toward higher anxiety/stress in female students was also observed. These exploratory patterns are broadly compatible with the wider literature suggesting that better physical fitness may relate to a lower probability of psychological symptoms via neuroendocrine, emotion-regulation and self-esteem mechanisms. 32 , 33
The inverse association between VO2max and anxiety aligns with previous research indicating that higher aerobic capacity is linked to reduced physiological arousal, improved autonomic regulation, and enhanced emotion-regulation pathways.34,37 Such mechanisms may help explain why individuals with better cardiorespiratory fitness report fewer anxiety-related symptoms, particularly in contexts characterized by academic and social demands. 35 In this regard, estimated VO2max emerged as an physical fitness indicator inversely associated with anxiety in the present study, suggesting that individuals with greater cardiorespiratory capacity may exhibit more efficient emotional regulation when facing daily life challenges. This interpretation is supported by recent evidence showing that aerobic fitness contributes to brain plasticity, strengthens connectivity within networks involved in emotional control, and reduces physiological responses to stress.13,36,37 Additionally, emerging research suggests that higher aerobic fitness may promote psychological resilience by enhancing both region-specific brain processes and large-scale neural circuits involved in emotional and behavioral regulation, particularly during adolescence and early adulthood. 37 Unlike some prior studies, however, VO2max did not predict depressive or stress symptoms in this sample, indicating that distinct psychological domains may respond differently to aerobic capacity. These mechanisms are proposed as theoretical rationale for future confirmatory research, rather than as explanations of the current null findings under uniform FDR correction.
However, variables such as muscle mass percentage did not show significant associations with the psychological variables analyzed. Although some previous studies have related muscle strength to lower levels of anxiety and depression, 38 these effects could depend on the frequency of exercise, the perception of physical performance, or previous experience in structured physical activity, factors that were not controlled in this analysis. 39 In contrast to previous findings, the present study did not identify significant associations between muscle mass percentage and any of the psychological domains evaluated, despite muscle mass being a structural variable closely related to strength. 40 This discrepancy suggests that the potential protective effects described in earlier research may depend on factors not captured in this sample, such as habitual training patterns, perceived physical competence, or long-term adaptations. Supporting the broader literature, neuroimaging and biomarker studies have shown that greater muscle strength is associated with larger hippocampal volume, improved white matter integrity, and higher levels of Brain-Derived Neurotrophic Factor (BDNF), a molecule frequently reduced in anxiety and depression. 41 It has also been proposed that muscle contraction during exercise stimulates the release of myokines with anti-inflammatory properties, which may counteract the chronic low-grade inflammation observed in several mood disorders. 42 Together, these mechanisms suggest that muscular adaptations may contribute to psychological well-being; however, in the current sample, such effects were not reflected in direct associations with muscle mass or strength, possibly due to contextual, behavioral, or methodological factors. These neurobiological mechanisms provide strong rationale for future adequately powered studies to test whether muscular adaptations translate into measurable psychological benefits in more representative university samples.
A non-significant trend toward higher anxiety and stress levels was observed among female students compared with males, consistent with epidemiological evidence indicating greater psychological vulnerability among women in university settings, a pattern documented in international and Latin American samples.7,9 These sex-related differences have been attributed to psychosocial and cultural factors, including greater emotional burden, differential coping strategies, and heightened exposure to academic and social stressors.4,7 Although the sex coefficients did not reach conventional statistical significance in the present models, the direction of association suggests that biological, psychosocial, or contextual determinants beyond physical fitness may contribute to psychological distress.3,4
Finally, some limitations of this study should be acknowledged when interpreting the findings. First, a major limitation is that 58.7% of the participants were enrolled in academic programs related to physical activity and sport. This overrepresentation introduces a potential selection bias, as students in sport-related disciplines typically present higher levels of physical activity, superior fitness profiles, and distinct exercise behaviors compared to the general university population. Consequently, the observed associations cannot be readily generalized to students from other academic fields, and replication studies in more diverse and representative samples are warranted. In addition, the cross-sectional design of the study precludes any causal inference regarding the relationships between physical fitness, body composition, and psychological symptoms. Several relevant variables were not assessed, including habitual physical activity levels, nutritional status, sleep quality, and psychosocial factors, which may function as mediators or confounders in the observed associations. Moreover, cardiorespiratory fitness (VO2max) was estimated using the Queen’s College Step Test rather than measured directly, which may introduce measurement error, because the test relies on sex-specific prediction equations, measurement error may differ by sex; however, interaction models (VO2max × sex) did not indicate effect modification in this sample (Supplemental Table S3). This methodological limitation could have attenuated the strength of the associations with mental health outcomes. Future research should prioritize direct assessments of VO2max via ergospirometry to improve measurement accuracy and better characterize the relationship between cardiorespiratory fitness and psychological well-being. Furthermore, longitudinal designs, non-linear analytical approaches, and the examination of potential moderating factors, such as sex, age, or baseline health status, are recommended to achieve a more comprehensive understanding of the physiological and behavioral mechanisms linking physical fitness to mental health in university students.
Conclusion
This pilot, exploratory study found no statistically significant associations between physical fitness or body-composition indicators and symptoms of anxiety, depression or stress in a convenience sample of Chilean university students enriched in sport-science programmes, once a uniform Benjamini–Hochberg correction was applied across all 15 predictor outcome tests. At descriptive level, the largest signal, a negative association between estimated VO2max and anxiety, with substantially weaker estimates for depression and stress, was consistent in direction with previous research on aerobic capacity and HPA-axis regulation, but should not be regarded as confirmatory. The findings are constrained by a cross-sectional design, an indirect VO2max estimate (Queen’s College Step Test), a marked male predominance (85.7%) that left the female subgroup underpowered for sex-stratified analyses, and a sport-enriched convenience sample. They are therefore best read as preliminary, hypothesis-generating, and as a source of effect-size estimates for future adequately powered, pre-registered studies in more representative university populations, ideally using direct measurement of VO2max and longitudinal or interventional designs.
Supplemental Material
Supplemental Material - Physical Fitness and Body Composition as Predictors of Anxiety, Depression, and Stress in University Students
Supplemental Material for Physical Fitness and Body Composition as Predictors of Anxiety, Depression, and Stress in University Students by Catalina Muñoz-Strale, Frano Giakoni-Ramírez, Josivaldo de Souza-Lima, Javiera Alarcón-Aguilar, Rodrigo Yáñez-Sepúlveda, Andrés Godoy-Cumillaf, Guillermo Cortés-Roco, José Francisco López-Gil in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Physical Fitness and Body Composition as Predictors of Anxiety, Depression, and Stress in University Students
Supplemental Material Physical Fitness and Body Composition as Predictors of Anxiety, Depression, and Stress in University Students by Catalina Muñoz-Strale, Frano Giakoni-Ramírez, Josivaldo de Souza-Lima, Javiera Alarcón-Aguilar, Rodrigo Yáñez-Sepúlveda, Andrés Godoy-Cumillaf, Guillermo Cortés-Roco, José Francisco López-Gil in American Journal of Lifestyle Medicine
Consent to Publication
During the preparation of this work, the authors used ChatGPT in order to improve language and readability. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Footnotes
Acknowledgments
The authors would like to thank all the students who participated in the study.
Ethical Considerations
This study was approved by the Ethics Committee of Universidad Autónoma de Chile (Ethics Code: CEC-2320) on June 14, 2020. All participants provided written informed consent prior to enrollment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki
Consent to Participate
The study was approved by the Ethics Committee of Universidad Autónoma de Chile (Ethical Clearance Reference Number: CEC-2320) on June 14, 2020. All participants provided written informed consent prior to participating.
Author Contributions
• Catalina Muñoz-Strale – Writing of the manuscript; data collection.
• Frano Giakoni-Ramírez – Editing of the manuscript; data collection.
• Josivaldo de Souza-Lima – Data collection.
• Javiera Alarcón-Aguilar – Data collection.
• Rodrigo Yáñez-Sepúlveda – Editing of the manuscript; data analysis.
• Andrés Godoy-Cumillaf – Editing of the manuscript; data analysis.
• Guillermo Cortés-Roco – Writing and revision of the manuscript.
• José Francisco López-Gil – Writing and revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.