
Abstract
The rapid growth of the older adult population and the increasing burden of chronic disease require coordinated, prevention-focused models of care. Lifestyle medicine (LM) provides evidence-based therapeutic interventions that target nutrition, physical activity, restorative sleep, stress management, social connection, and avoidance of risky substances. At the same time, the Age-Friendly Health Systems initiative promotes the 4Ms framework, which includes What Matters, Medication, Mentation, and Mobility, to optimize outcomes for older adults. Although these approaches are conceptually aligned, they are often implemented independently. This manuscript describes an interprofessional framework integrating LM and the 4Ms to advance whole-person, age-friendly care. The framework positions What Matters at the center, organizes care through the remaining domains (Medication, Mentation, and Mobility), and embeds the 6 lifestyle pillars as modifiable drivers of health. Implementation across interdisciplinary educational initiatives—including case conceptualizations, Project ECHO (Extension for Community Healthcare Outcomes) participation, community health worker training, internships, an asynchronous LM course, and a culinary medicine teaching kitchen—demonstrates feasibility in academic and community settings. Descriptive evaluation findings indicate interdisciplinary engagement, high satisfaction, perceived relevance to practice, and reported improvements in confidence and clinical application. Integrating lifestyle medicine within interprofessional structures offers a scalable strategy to strengthen workforce development and support healthy longevity.
Keywords
“85.3% of post-course respondents reported making minor or significant changes in their own health behaviors.”
Introduction
The United States is experiencing a profound demographic shift, with approximately 78.3 million Americans projected to be aged 65 years or older by 2040. 1 Older adults disproportionately experience multimorbidity, with approximately two-thirds living with multiple chronic conditions. 2 The complexity of chronic disease management, including polypharmacy, functional decline, cognitive impairment, and social determinants of health, requires coordinated, team-based approaches.
Lifestyle medicine (LM) has emerged as an evidence-based discipline that addresses the root causes of chronic disease through structured behavior change interventions that target 6 modifiable pillars: nutrition, physical activity, restorative sleep, stress management, positive social connection, and avoidance of risky substances. 3 Despite growing evidence, formal education in LM and behavior change counseling remains inconsistently integrated across health professions training. 4
At the same time, healthcare systems place growing emphasis on collaborative practice. Interprofessional education (IPE) is defined as learning that occurs when 2 or more professions learn with, from, and about each other to improve collaboration and the quality of care. 5 IPE is widely endorsed as a foundational strategy, yet prevention-focused, lifestyle-centered content that is specific to older adult care is often absent from IPE initiatives.
The Age-Friendly Health Systems movement introduced the 4Ms framework as a pragmatic structure to improve care for older adults. 6 The 4Ms identify core issues that should drive decision-making in older adult care and help organize care around wellness and strengths rather than disease alone. Although LM and the 4Ms share foundational goals, they are frequently implemented in parallel rather than through intentional integration. To address this gap, an interprofessional framework was developed to intentionally align LM and the 4Ms within educational and clinical contexts.
Conceptual Integration of Lifestyle Medicine and the 4MS
The 4Ms framework organizes age-friendly care around 4 essential domains that should be assessed and acted on for every older adult: ● What Matters: Aligning care with individual goals, values, and preferences ● Medication: Optimizing pharmacologic regimens while minimizing harm ● Mentation: Prevention, identification, and management of cognitive impairment, mood, and delirium ● Mobility: Preserving safe and functional movement
The 6 pillars of LM directly influence each of these domains. Nutrition and physical activity affect metabolic control, sarcopenia, medication burden, and fall risk. Sleep and stress management influence mood, cognitive function, and resilience. Positive social connection supports mentation and aligns with individual priorities. Avoidance of risky substances reduces adverse events and polypharmacy complications.
Recognizing this overlap, the Optimal Aging Lifestyle Medicine (OALM) framework was developed to intentionally integrate these models (Figure 1). Optimal Aging Lifestyle Medicine (OALM) framework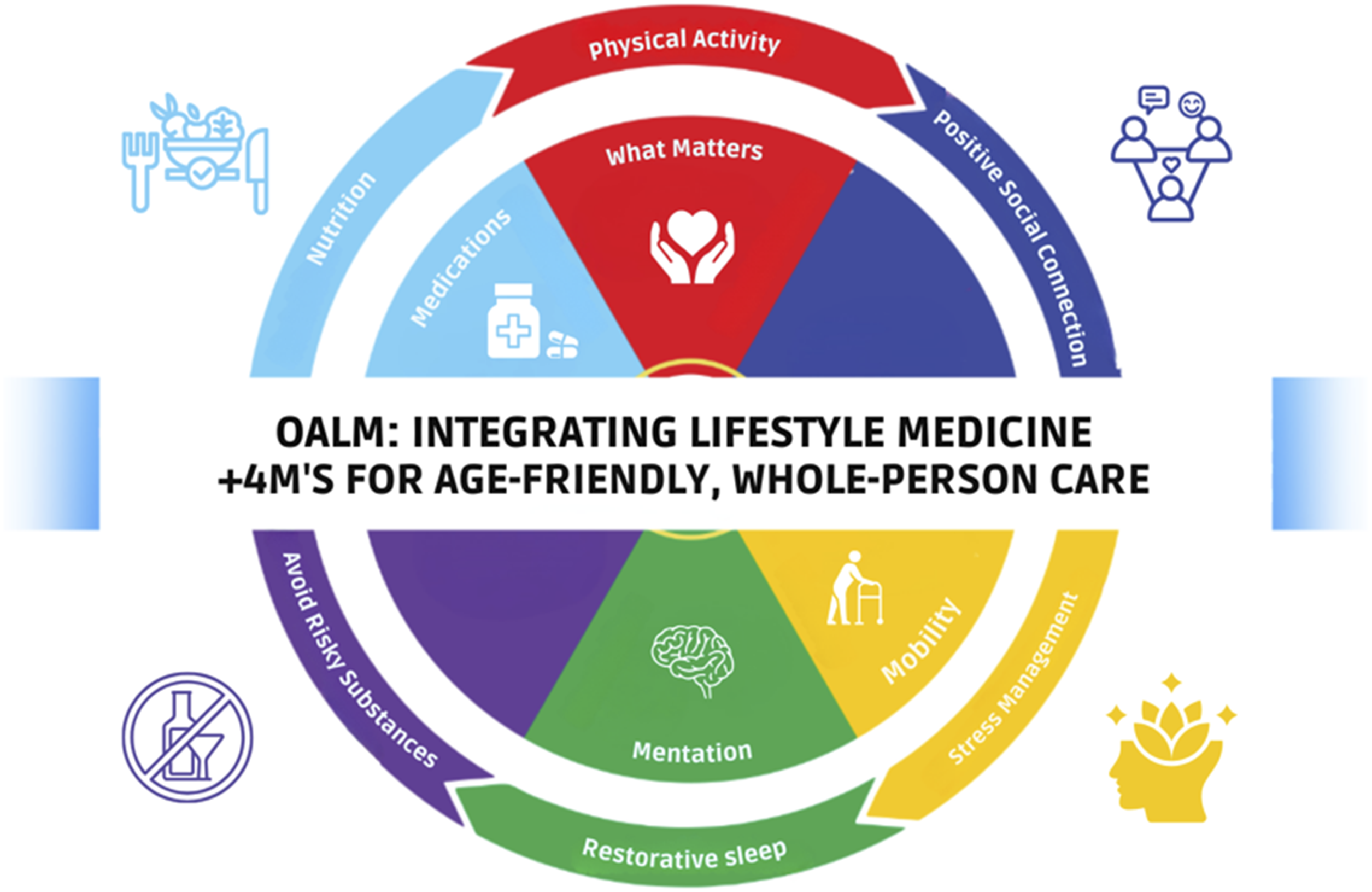
The Optimal Aging Lifestyle Medicine (OALM) Framework
The OALM framework places What Matters at the center. This position reinforces the role of each person’s goals and preferences as the anchor of clinical decision-making and behavior change interventions. Surrounding this core are the domains of Medication, Mentation, and Mobility, which provide the organizing clinical lens for assessment and care planning.
Encircling the 4Ms are the 6 LM pillars, which represent modifiable drivers of health that influence each domain. The circular configuration reflects the interdependence of lifestyle factors and clinical outcomes as well as the dynamic nature of whole-person care and shared accountability across disciplines. Rather than creating a separate preventive model, the OALM framework embeds LM within an established age-friendly structure that is already familiar to many clinicians and health systems.
The framework functions both as a clinical organizing tool and as an educational scaffold. It offers learners a practical map for applying LM principles within an age-friendly lens and supports translation of LM concepts into case discussions, care planning, and interprofessional team-based care for older adults.
Interprofessional Educational Implementation
The OALM framework was implemented through multiple interprofessional educational initiatives that were designed to integrate LM into existing structures in academic and community settings. These initiatives include case-based learning, clinical experiences, virtual tele-mentoring, asynchronous coursework, and hands-on culinary medicine training.
Case-Based Interprofessional Learning
Learners from medicine, nursing, social work, pharmacy, psychology, and community health backgrounds collaboratively analyze complex older adult cases using the OALM framework. A case example may feature a 77-year-old woman living with diabetes, hyperlipidemia, obesity, chronic pain, and social isolation, which prompts learners to identify LM opportunities, 4Ms considerations, social needs, and team-based care approaches. Structured case conceptualization sessions allow learners to present their own patient cases and receive interprofessional feedback that reinforces shared language and role clarity.
Clinical Interprofessional Experiences
Learners are embedded in interprofessional care management huddles at an academic aging institute, where they observe and participate in real-time team discussions that center on complex older adults. These huddles involve learners and professionals in medicine, nursing, social work, dentistry, pharmacy, and more who jointly address social determinants of health while applying LM and the 4Ms. This structure helps learners see how LM and age-friendly care are operationalized within clinical workflows.
Project ECHO: Care of Older Adults
A monthly virtual Project ECHO (Extension for Community Healthcare Outcomes) series focuses on the care of older adults, and LM themes are integrated into every other session. Participants include clinicians, community health workers, community-based organizations, and caregivers and together they create a community of practice that extends beyond a single institution. The ECHO model uses case-based tele-mentoring to disseminate expertise and to support adoption of LM and the 4Ms in rural and underserved settings.
Community Health Worker and Paraprofessional Training
Educational modules embed the OALM framework into community health worker and paraprofessional curricula, with application during supervised apprenticeship experiences. Because they frequently address social needs and support behavior change in community settings, community health workers are positioned as key team members in implementing LM-informed care for older adults.
Social Work and Nursing Internships
Social work and nursing interns complete rotations in which they apply LM and the 4Ms directly with older adults in clinical and community-based settings. Interns practice lifestyle counseling, care coordination, and goal setting that is aligned with What Matters, and they address medication, mentation, and mobility considerations as part of interprofessional teams.
Asynchronous Optimal Aging Lifestyle Medicine Course
The OALM course is a fully asynchronous online micro-credentialing program with modular content that participants can complete flexibly. The course has been offered to medical, nursing, social work, pharmacy, dental, physical therapy, occupational therapy, community health, and other learners and professionals and it emphasizes accessibility and broad reach. The curriculum is built around practical modules that apply lifestyle medicine core competencies and the 4Ms framework and uses interactive cases, brief videos, quizzes, and reflective activities to build skills in age- and dementia-friendly LM care.
Culinary Medicine Teaching Kitchen
A flipped-classroom culinary medicine course uses an ACLM-aligned culinary curriculum to strengthen practical nutrition counseling skills. Learners review evidence-based LM content before in-person, hands-on sessions where they practice culinary skills, meal planning, and translation of nutrition science into everyday meals. The teaching kitchen environment supports confidence in discussing nutrition, cost, accessibility, and realistic behavior change with older adults and helps learners experience LM in a tangible way.
Evaluation
A total of 695 learners registered for the OALM course, with 225 completing the program (32.4% completion rate). Pre-course assessments were completed by 72 participants, and post-course assessments were completed by 68 participants, representing approximately 30% of course completers.
Participants represented a range of health professions, including nursing, medicine, dentistry, pharmacy, community health workers, social work, and other allied disciplines. This interdisciplinary distribution reflects the intended audience and supports the interprofessional design of the framework.
Knowledge and Confidence
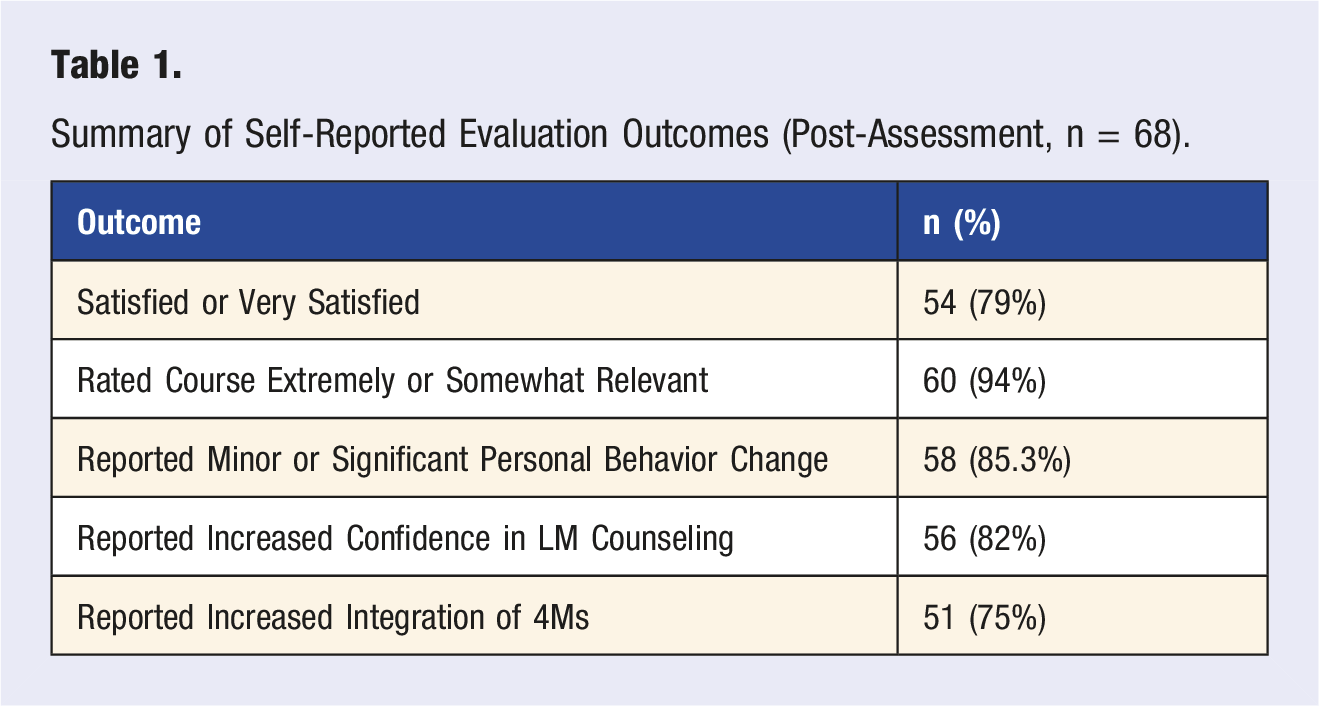
Summary of Self-Reported Evaluation Outcomes (Post-Assessment, n = 68).
Clinical Practice Application
Post-course responses indicated increased frequency of discussing lifestyle medicine interventions with patients and incorporating elements of the 4Ms framework into clinical practice. Participants reported greater alignment between preventive counseling and age-friendly care priorities.
Personal Behavior Change, Satisfaction, and Relevance
85.3% of post-course respondents reported making minor or significant changes in their own health behaviors. Most participants reported being satisfied or very satisfied with the course, and a substantial majority (94% of post-course respondents) rated the content as extremely or somewhat relevant to their clinical practice.
Qualitative feedback reflected perceived improvements in holistic thinking and practical application. One community health worker noted, “This course helped me think more holistically about patient care.” An advanced practice registered nurse shared, “I saved so many resources—action plan worksheets, tools, and more.”
Because pre- and post-assessments were not paired at the individual level, inferential statistical comparisons were not conducted. Findings are descriptive and reflect self-reported outcomes.
Taken together, these findings indicate that embedding LM within an age-friendly, interprofessional framework is feasible, well-received, and associated with improved knowledge, confidence, and self-reported practice change.
Replication and Scalability
The integration of the OALM framework does not require the creation of entirely new educational programs. Instead, it can be embedded within existing interprofessional and clinical structures. Implementation begins by identifying current educational touchpoints such as case conferences, clinical rotations, care management huddles, interprofessional seminars, and continuing education programs where LM concepts can be aligned with the 4Ms.
Strategies for Integrating Lifestyle Medicine and the 4Ms Into Existing Educational Structures.
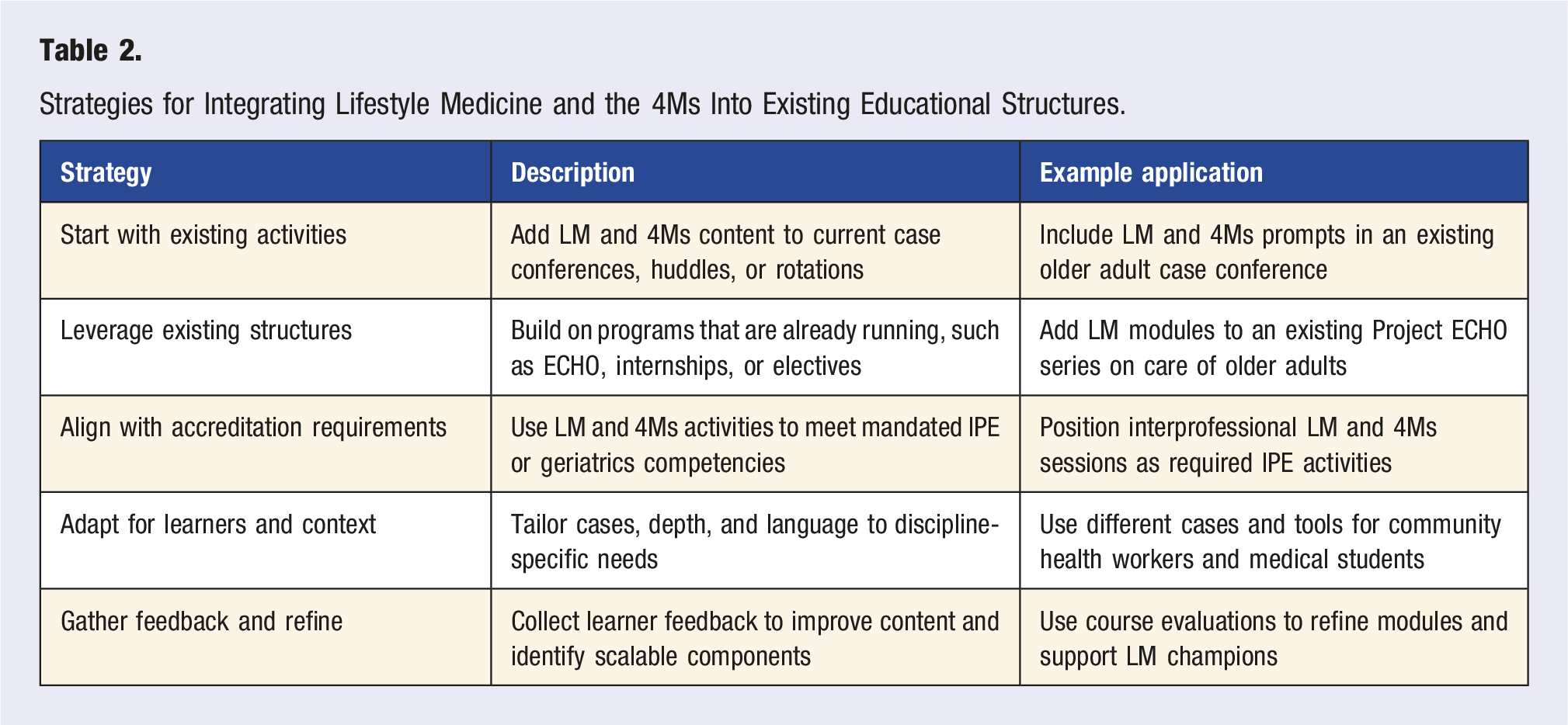
This approach improves feasibility, reduces curricular burden, and supports sustainability by aligning with existing accreditation standards and institutional priorities. Leveraging platforms, such as Project ECHO and teaching kitchens, allows programs to extend reach without requiring substantial new infrastructure. Identifying LM champions across disciplines and sites further supports diffusion of innovation and culture change.
Implications for Workforce Development
Preparing the healthcare workforce to care for an aging population requires prevention-focused and collaborative approaches that address multimorbidity, functional decline, and behavioral risk factors. Aligning LM with the 4Ms within interprofessional education strengthens readiness to deliver age-friendly, whole-person care.
Integrating these models reduces fragmentation by providing a shared framework for team communication and care planning that is centered on What Matters. The OALM framework also offers a practical pathway for institutions that wish to advance Age-Friendly Health Systems initiatives while meeting IPE and geriatrics education requirements. Future work should examine patient-level outcomes, interprofessional collaboration measures, and long-term workforce impacts associated with OALM-based training.
Conclusion
Aligning LM with the 4Ms through interprofessional education offers a structured and practical approach to advancing whole-person care for older adults. By embedding prevention-focused strategies within existing collaborative training environments, health systems may strengthen workforce preparedness and better support healthy aging and healthy longevity. Continued evaluation will clarify how integrated frameworks, such as OALM, contribute to sustainable, age-friendly transformation across diverse care settings.
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under the Geriatric Academic Career Award (GACA), Award Number 5K01HP49065-03-00, totaling $270,013.00, with 0% financed with non-governmental sources. The contents are those of the author and do not necessarily represent the official views of, nor an endorsement by, HRSA, HHS, or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.