
Abstract
Introduction
Nonpharmacological lifestyle interventions can prevent age-related cognitive decline, but people find adhering to healthy habits challenging. The
Objectives
To use examples of the individualized healthy aging goals and strategies created in the AgeWISE-AP program action-plan sessions to demonstrate the importance of considering what matters most when working toward lifestyle change.
Methods
Veterans (cognitively intact, age ≥60) in the action-plan component of AgeWISE-AP participated in eight one-on-one sessions to create and implement individualized lifestyle goals to support positive brain health outcomes.
Results
Participants (n = 36) developed up to four unique SMART (Specific, Measurable, Achievable, Relevant, Time-bound) brain health goals, generating 120 goals across brain health domains. Case examples demonstrate the process of engagement, goal setting, and implementation.
Conclusion
Participation in a nonpharmacological intervention focused on individualized selection of lifestyle changing goals can support healthy brain aging. Understanding what matters most to older adults (their “why”), together with personal interests and activities that motivate them to consistently participate in behavior goals (their “what”), may aid in the success of such interventions.
Introduction
Military Veterans are an important aging population; almost half are age 65 or older and more than a quarter are age 75 or older. 1 Maintaining cognitive health and reducing dementia risk are priorities for aging Veterans. Veterans are at an increased risk of experiencing physical, psychological, and social challenges uniquely tied to their service, which threaten brain health. For example, Veterans experience higher rates of post-traumatic stress disorder, anxiety and depression, and physical conditions such as hypertension and diabetes compared to civilian populations.2–6 Similarly, Veterans may be more vulnerable to social isolation, which has been linked to cognitive decline. 7 Given the above, focusing on brain health and reducing cognitive decline is imperative for supporting a successful aging experience for Veterans.
Research shows that nonpharmacological lifestyle interventions can improve brain health. Furthermore, studies have shown that cognitive changes that happen late in life are attributed more to environmental impacts than genetics. 8 As a result, one can have increased control over one’s brain health by making conscious lifestyle changes that protect against cognitive decline. The largest body of research focuses on exercise as one of the primary preventatives for cognitive decline.9–11 Studies have found that consistent exercise12–16 maintains brain health and protects against cognitive changes as one ages. Adequate sleep also impacts brain health. 17 Additionally, diet (specifically Mediterranean and plant-based diets) has strong evidentiary support for the prevention and management of cognitive decline.18–20 Proper diet has also been shown to reduce physiological risk factors (e.g., diabetes, high cholesterol, and high blood pressure) which can, in turn, decrease the risk of dementia.21–23 Socialization and engagement in leisure activities have been shown to be associated with improved cognition whereas social isolation7,24 and lack of engagement in intellectual activities can lead to decreased cognition and increased risk of dementia and cognitive decline.25,26 By making sustainable changes to lifestyle factors, one can be more successful at maintaining optimal brain functioning throughout the aging process. As the Veteran population ages, it is critical that there are innovative brain health programs available to educate and support lifestyle change within the Veterans Affairs (VA) health care system.
Within VA, the Whole Health model has been used to shift the focus from Veterans’ disease and comorbidities to caring for the entire Veteran, their overall health and well-being, and what matters most to them. This holistic and person-centered approach recognizes that the person is at the center of care and there are many different aspects of life that impact the person and their overall health.
27
Previous research has demonstrated that using the Whole Health model in patient care is associated with positive changes in chronic pain management and mental health outcomes, and a decrease in opioid use.28–31 Given the positive outcomes associated with the Whole Health model in the Veteran population overall, we specifically tailored the model to older adults and healthy brain aging. The adapted Whole Health Circle of Brain Health (Figure 1) focuses on lifestyle factors known to protect the brain from the risk of cognitive decline. It includes domains such as exercise/moving the body, physical surroundings, personal development, diet and nutrition, recharge and sleep, relationships, spirit and soul, and the power of the mind. Recent studies have shown that taking a holistic approach to cognitive health by focusing on multiple elements of an individual’s circle of health can support healthy brain aging.32–34 This evidence suggests that taking a multi-pronged approach to Veteran brain health by encouraging the selection of several nonpharmacological lifestyle goals across multiple domains may be most effective. Whole Health Circle of Brain Health.
In our previous work, we utilized the adapted Whole Health Circle of Brain Health in the context of the Aging Well through Interaction and Scientific Education (AgeWISE) brain health intervention. AgeWISE engages older Veterans in 12, 1-hour group education sessions focused on brain health education, up-to-date research regarding the impact of lifestyle factors on brain health, and the provision of practical techniques to manage functional changes associated with typical age-related cognitive decline observed in normal aging. Participants who completed AgeWISE reported feeling that they had more control over their brain health and felt more satisfied with their current cognitive abilities. 35 To further support participants and translate AgeWISE education into healthy brain lifestyle changes, the current study incorporates an additional 8-session, one-on-one action-plan component to the original AgeWISE group intervention. The AgeWISE-Action Plan (or AgeWISE-AP) includes both the 12-week AgeWISE group followed by the individual one-on-one action-plan sessions. Led by a Brain Health Interventionist (BHI), the action-plan sessions focus on supporting each participant in the creation and implementation of patient-centered lifestyle goals. 35 In this article, we will focus on the outcomes of the action-plan component of AgeWISE-AP, presenting case examples to illustrate the process participants undergo in selecting, implementing, and maintaining nonpharmacological lifestyle goals for healthy brain aging.
Methods
AgeWISE-AP Intervention
All participants were Veterans enrolled in the AgeWISE-AP program. Descriptions of the 12-week AgeWISE group sessions can be found in the published study protocol.
35
The first four individual action-plan sessions occurred during weeks 9-12 of the AgeWISE group, with Veterans attending both their weekly AgeWISE group session and their one-on-one action-plan meetings with the BHI (Figure 2). During weeks 13-20, after completion of the AgeWISE group, the Veteran and BHI met every other week for the remaining four action-plan sessions. AgeWISE-AP group and individual sessions timeline.
The one-on-one action-plan sessions were collaborative, with the BHI guiding the participant through the creation of a personalized action-plan focused on the domains of the adapted Whole Health Circle of Brain Health. The BHI was a doctoral-level occupational therapist (OT). OTs receive education and training in psychosocial approaches and techniques including motivational interviewing, goal setting, and supporting self-efficacy. 36 OT’s scope of practice includes supporting individuals in participating in meaningful, functionally relevant goal setting.37,38 The BHI facilitated the identification of what matters most to the Veteran, their values, and what drives them (conceptualized as their “why”), as well as what interests them, and their previous experience in setting and achieving goals (conceptualized as their “what”). The BHI used the understanding of the Veteran’s “why” and “what” to support participants in creating, adapting, and maintaining healthy brain aging goals.
The first four sessions were weekly, 1-hour sessions designed to support Veterans in creating 2-4 Specific, Measurable, Achievable, Realistic, and Time-bound (SMART) goals across lifestyle factors associated with the domains of healthy aging (exercise, diet, sleep, socialization, etc.). Once an action-plan was created to address the SMART goals, the BHI then met with the Veteran every other week (4 sessions over 8 weeks) to monitor improvements, identify barriers to progress, and revise the action-plan as needed. The BHI developed a manualized protocol so that each action-plan session was structured similarly across all participants. However, given the diverse experiences, goals, values, interests, and abilities of the Veterans, action-plan sessions were highly personalized, and the brain health action-plans were unique to each participant.
Throughout the 12-week engagement in the action-plan component, the BHI provided one-on-one guidance, support, and resources to participants. The BHI helped Veterans find local resources and coordinated referrals to VA and non-VA programs that could support goal attainment. This included but was not limited to providing physical handouts or virtual links for information on VA and non-VA programming within the domains of healthy aging like fitness classes or book clubs, collaboratively identifying requirements for participation in desired programming, and prompting participants to use one-on-one time to sign up for programming. Further real-time hand-offs were provided in session where the BHI connected participants with external supports if needed. For example, action-plan session time was used to seek out desired referrals from a participant’s VA health care team for resources like mental health treatment, or approval to use the VA recreation center. For this study, data related to goals and participant progress was organized into a goal matrix, tracking goals created, changes to goals across the action-plan sessions, participant reflections verbalized during sessions, and BHI post-session notes.
Participants
Veterans highlighted in this article were participants of a larger study entitled: A 20 week, Randomized Controlled Trial to Determine the Efficacy of the Aging Well through Interactions and Scientific Education – Action Plan (AgeWISE-AP) Program in Older Veterans. 35 This study was reviewed, approved, and monitored by the VA Central Institutional Review Board. Veteran participants (n = 128) were recruited, consented, and enrolled from the Bedford VA Health care System and randomly assigned to the AgeWISE-AP intervention or a waitlist control.
Veteran eligibility criteria for the study included being 60 years or older with concerns about, and interest in, brain aging, and the ability to speak and read English. Exclusion criteria included scoring less than 24/30 on the Montreal Cognitive Assessment (MoCA) during the screening process, and/or a self-reported diagnosis of Alzheimer’s disease, Parkinson’s disease, dementia, or other brain disorders impacting cognition. Additional details on eligibility criteria and methods for the larger study are available in the published study protocol. 35
Procedures
During the one-on-one individualized action-plan sessions, participants created no more than 4 SMART goals within at least 2 domains (out of 8) in the Whole Health Circle of Brain Health with the guidance of the BHI. Participants were asked to self-identify what domain(s) in the Whole Health Circle of Brain Health their goals fell under. Veterans were encouraged by the BHI to identify 1 domain per goal; however, some participants identified up to 2 domains if they felt their goals touched on both domains equally (e.g., for some participants, participating in an exercise class fell under both exercise and socialization domains equally). No participant felt that any one of their goals fell under three domains. The BHI took notes after each session and created a formalized field note at the end of the final session recording overall reflections and experiences with the participant.
Flexibility was built into the action-plan sessions, allowing participants to change certain aspects of their goals, or entire goals, as they went through the process of implementation. Permitting flexibility in goals allowed for the greatest possibility of maintaining the goals throughout the individual sessions and beyond. Because of that, data tracked via the goals matrix was subject to change and changes were notated and dated by the BHI. The reported outcomes highlight the final goals and domains present at the end of session 8 or the end of the Veteran’s participation in the program.
Below, we present the SMART goals and healthy brain aging domain outcomes of participants to date. Additionally, we present three exemplar cases selected both to highlight the diversity of the study population across age and sex, as well as to demonstrate the breadth of goals and domains selected in the intervention and the varied and interesting ways participants went about achieving their goals.
Results
Veteran Characteristics.
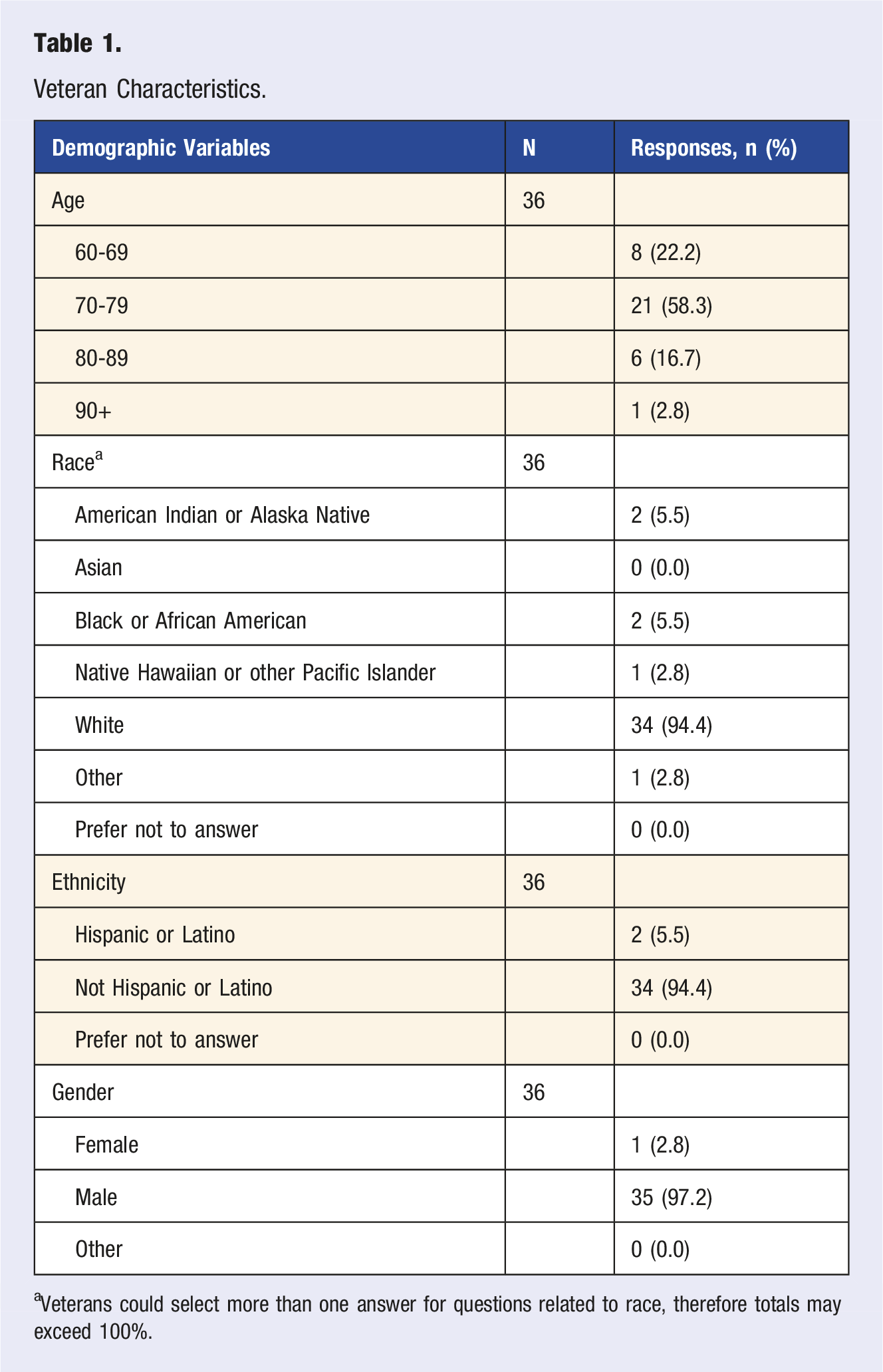
aVeterans could select more than one answer for questions related to race, therefore totals may exceed 100%.
Participants (n = 36) completed 282 individual action-plan sessions. Participants established up to four Whole Health Circle of Brain Health-aligned SMART goals each, with a total of 120 goals created by the end of session 8 or their participation in the program. Participants experiencing challenges adhering to their goals were allowed the flexibility to adjust their goals to be more aligned with their values, interests, daily schedules, etc. Out of 120 goals created, 35 goals were modified. Given the iterative process of collaboratively making goals, it was common for participants to modify goals for myriad reasons at varied times throughout the sessions, sometimes making multiple changes at different times. Of those who adjusted their goals, some Veterans modified for content, where they decided to change what they wanted to participate in (e.g., they tried running but decided to change to walking) while others modified for duration (e.g., they tried running for 10 minutes but decided to increase their time to 15 minutes). Some participants modified their goals for timing (e.g., instead of running on Monday, Wednesday, and Friday, they decided running on Tuesday, Thursday, and Saturday was better for their schedule) and some discontinued certain goals altogether. The reasons for these adjustments varied, but often participants modified their goals to increase or decrease the challenge, to better fit their personal schedule, or to align with their personal interests or values. Therefore, reflecting on the nature of the modification instead of the number of overall modifications more accurately reflects the action-plan goal-setting process. The outcomes reported in the following section highlight the finalized goals and domains present at the end of session 8 or the final session the participant attended.
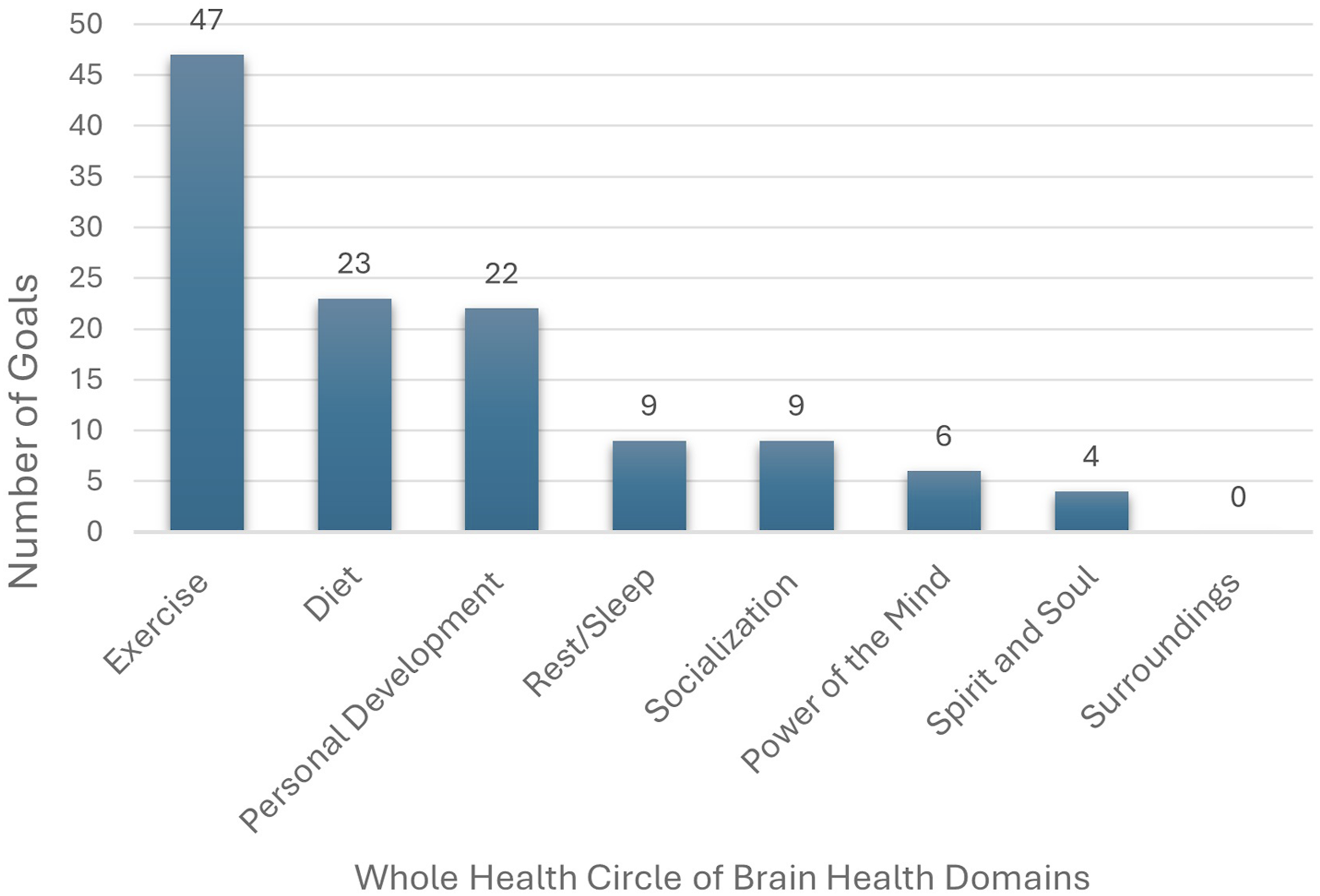
The number of goals per each Whole Health Circle of Brain Health domain are outlined below and displayed in Figure 3. No participants chose to create goals within the Surroundings domain. Examples of common goals for each domain are as follows: • Exercise (47 goals): group fitness classes, weightlifting, walking • Diet (23): vegetable increase, red meat decrease, cooking at home • Personal Development (22): art or music endeavors, reading, volunteering • Rest/Sleep (9): sleep hygiene practices, caffeine decrease • Socialization (9): senior center luncheons, Veterans groups • Power of the Mind (6): Journaling, mindfulness groups • Spirit and Soul (4): Attending religious services, individual morning/evening prayer, religious leadership roles. Number of goals per Whole Health Circle of Brain Health domain.
Case Examples
Veteran 1
Veteran 1, a male in his mid-70s, joined the AgeWISE-AP program because he used to be very active and engaged when he was working, but once he retired, he felt less connected to his routines and roles that supported healthy brain aging. Veteran 1 identified early in the action-plan sessions that introspection and family connection were central to his motivation to join the study (Veteran 1’s “why”). Throughout the individual sessions, his primary goal was to create a writing practice, using reflective journaling prompts he and the BHI found online. His writing process included brainstorming, writing, editing, and finalizing multiple journal entries a week, supporting engagement in his healthy aging goal (Veteran 1’s “what”). Even though he periodically experienced challenges with motivation or a lack of free time to spend writing, Veteran 1 collaborated with the BHI to identify what motivates him (his “why”), which facilitated his renewed engagement in his goal. At the end of the AgeWISE-AP program, Veteran 1 reported a renewed sense of motivation, and a strengthened sense of purpose. He even set the intention to continue to write his history and perspective into a book or memoir for family and friends after the intervention ended. This case demonstrates how having a clear understanding of what one values can drive participation and continued engagement to achieve healthy brain aging goals.
Veteran 2
Veteran 2, a male in his mid-60s, entered the AgeWISE-AP program seeking ways to strengthen healthy routines while managing a history of behavioral addiction. When asked what drives his desire to manage these challenges, he stated that being there for his family and community, both personally and financially, as well as connecting with his faith was what mattered most to him (Veteran 2’s “why”). He identified that the addictive behaviors he dealt with took money and time away from the things he truly cared about, and he often felt lonely, confused, and empty when participating in them. The BHI connected Veteran 2 to VA groups for behavioral health and individual mental health treatment as well as provided him with additional information regarding community-based behavioral addiction programming. In the one-on-one sessions, the BHI was able to support Veteran 2’s participation in his chosen behavioral addiction groups by implementing strategies like calendaring and mindfulness (such as body scans and meditation). He also spent time focusing on his additional goal of establishing a regular prayer practice (his “what”). With less time spent on behavioral addiction, Veteran 2 reported being more active with his family and in his church community, even trying out for the church choir. Veteran 2’s experience demonstrated the importance of reflecting on one’s “why” and “what” and utilizing formal clinical resources to help set and maintain healthy habits.
Veteran 3
Veteran 3, a female participant in her late 60s, started the AgeWISE-AP program with many healthy lifestyle habits already in place. In the initial action-plan sessions, she shared that her goal was to remain as independent and active as possible as she ages so she can be there for her family (Veteran 3’s “why”). Although retired, she remained highly involved in part-time work as well as hobbies like gardening, walking, and taking college-level classes. While Veteran 3 was doing well in many domains of healthy brain aging, she expressed interest in fine-tuning her habits and goals. Veteran 3 reported that learning about the positive associations between exercise, socialization, and cognitive health enhanced her motivation to sustain and intensify her healthy aging routines. In collaboration with the BHI, who helped Veteran 3 identify local fitness classes that fit her schedule and provided links to virtual yoga for Veterans, Veteran 3 established goals, including attending martial arts fitness classes and personal training sessions, participating in virtual yoga and stretching classes, and volunteering at her local church (Veteran 3’s “what”). Throughout the action-plan sessions, Veteran 3 demonstrated a high level of confidence in her ability to achieve her goals and often spontaneously increased the frequency of her participation. This case demonstrates how an individual who already has strong healthy lifestyle habits can benefit from fine-tuning goals, increasing frequency of participation, and diversifying activities.
Discussion
Older Veterans, a fast-growing section of the Veteran population, are facing unique and compounding factors associated with the potential for cognitive decline as they age. 4 While there is strong evidence that the utilization of nonpharmacological lifestyle interventions helps to promote healthy brain aging, there is less research on how to implement tailored, person-centered interventions to support older adults in translating brain health education into behavioral change. The AgeWISE-AP program focused on bridging the gap between education and action by providing one-on-one guidance, support, and resources for Veterans to create personalized action-plans focused on lifestyle changes for a healthy brain.
Throughout the AgeWISE-AP group portion of the intervention (the original AgeWISE group), participants were educated in all aspects of healthy brain aging. Increases in exercise and improvements in diet have the most evidence in the literature to support healthy brain aging, therefore AgeWISE-AP group participants were presented with evidence demonstrating the positive impacts of regular physical exercise and a Mediterranean-style diet on brain health as one ages.39,40 Given this, it is unsurprising that exercise and diet became natural focal points for participants’ brain health goals in the action-plan sessions. Even with the BHI following each participant’s lead and supporting them in creating healthy brain aging goals within domains that interested them, most participants chose to make changes to their diet and exercise routines. This suggests that participants were actively drawing from the knowledge gained in the group as they engaged in individual, behavior change work.
Many participants also created at least 1 or 2 goals outside the diet and exercise domains. There were equally as many personal development goals created (n = 22) as diet goals (n = 23). While diet has strong evidentiary support for healthy brain aging, it was clear that personal development was a high priority area for behavior change for many Veterans as well. To address the personal development domain, Veterans created goals focused on activities such as reading, music, art, and learning a language. Specific activities chosen under the personal development domain were unique to each Veteran (their “what”), highlighting the importance of both the Veteran understanding the “me” in the center of the Whole Health Circle of Brain Health, as well as the BHI successfully assisting and supporting the Veteran in goal creation and participation throughout the sessions. Maintaining SMART goals within the personal development domain hinged on each Veteran understanding their values, and what mattered most to them (their “why”).
Veteran 1 chose to create a reflective journaling goal, answering multiple questions each week that prompted him to think about his past experiences and what he hoped for in the future. This goal provided him with a structured way to reflect as well as share his thoughts with family and friends via a compilation of entries. Because of the variety of questions and his overall interest in reflecting on his experiences, Veteran 1 was able to maintain the goal throughout the intervention. For Veterans 2 and 3, choosing to engage in activities that aligned with their personal values as well as interests, like joining a choir or volunteering at their church, respectively, helped them to sustain participation in healthy brain aging goals.
Previous literature on meaningful activities and goal setting in older adults supports the experience of the AgeWISE-AP participants, finding that the more person-centered the goal is, the more likely participants are to engage in that goal consistently. Goal setting research in rehabilitation for older adults finds that collaboration between patient and clinician in choosing goals that align with patient values and available resources strengthens patient autonomy, motivation, and self-efficacy.41–44 Furthermore, dementia researchers have identified the various elements of an activity that make it meaningful for older adults. Per researchers, 45 activities need to be enjoyable, linked to identity, suited to physical and cognitive abilities, engaging with the “just right” challenge, and goal-related. Participants also need to have access to the activity and the resources required to participate in the activity. 45 Many participants of the AgeWISE-AP program were able to tap into these elements to help them sustain their healthy brain aging goals.
Meanwhile, researchers found that having a strong understanding of meaning and purpose in life was also an essential factor for maintaining participation in behavior change goals.46,47 In the action-plan sessions, when asked what brings Veterans meaning and purpose in life and what really matters to them (their “why”), many reported that their personal autonomy and independence were important, along with relationships with family and friends, and their community. Veteran 1 found that participating in his reflective journaling goal allowed him to spend more time and connect more deeply with his family and friends, therefore strengthening his bonds with loved ones. Veteran 2 desired to stop participating in addictive coping behaviors which he found took time away from his community and faith. The motivation behind the goal helped him to retain focus and implement strategies to become successful. Moreover, many Veterans stated that the drive to participate in positive lifestyle behaviors stemmed from the desire to stay independent and healthy as they aged so that they could live in their home as long as possible or watch their grandchildren grow up. Veteran 3 was already focused on the domains that would support healthy brain aging; however, she desired to push herself even further so that she could enjoy her retirement and spend quality time with her family, travel, and be outside.
Research by Boyle and colleagues (2022) 46 supports this observation, finding that having a strong sense of purpose in life is connected to positive cognitive outcomes in older adults and may be protective against cognitive decline. More importantly, understanding what is important to someone holistically or what drives them can help to foster long-term positive lifestyle changes.46,48 Similarly, recent research has supported the work done by Boyle et al, finding that having a strong purpose in life is a protective factor against dementia risk as well as a potentially effective target for early intervention and implementation of nonpharmacological lifestyle interventions. 49
In the current study, we examined how Veterans’ broad understanding of values, meaning, and purpose in life (their “why”), together with their personal interests and activities that motivate them (their “what”), may shape their engagement in lifestyle behavior change. Aligning these elements may contribute to positive outcomes.
Limitations and Future Directions
While we had 36 participants complete the AgeWISE-AP program to date, the case examples presented are a small snapshot of the participants' overall experience in the action-plan sessions and therefore are not generalizable to the larger population of older adult Veterans. Similarly, while the case examples were chosen to highlight the age and gender diversity of the study, the overall sample (predominantly white male Veterans) lacks diversity, which can also limit the generalizability of our findings to a larger, non-VA audience. Moreover, the participants who met eligibility criteria and enrolled in the study were expected to participate in both the group and individual sessions of the AgeWISE-AP programs which required, at different time points, bi-weekly, weekly, and twice weekly, 1 hour, in-person group and individual meetings over a span of 20 weeks. This naturally limits individuals who are unable to meet such a commitment (due to employment, family commitments, or other constraints), and highlights those with more free time and interest in the study. This study represents a snapshot in time of the Veterans’ experiences implementing lifestyle goals focused on behavioral changes for healthy brain aging. Future research could gather a more expanded view of successful strategies for sustainability and goal progression over time, as well as an assessment of continued accountability and support needs post-intervention.
Footnotes
Acknowledgments
The authors thank all participants for taking the time to participate in the AgeWISE-AP Program and for supporting this study.
ORCID iDs
Ethical Considerations
The study has been approved and monitored by the VA Central Institutional Review Board (study number 23-55 1753578-1). Written informed consent was obtained from all study participants.
Consent to Participate
Written informed consent was obtained from all study participants.
Author Contributions
The entire research team, comprised of all the authors, made substantial contributions to this work. JEM served as BHI for study participants and was involved in creating and editing the AgeWISE-AP facilitator manual and participant AP workbook. LRM was involved in all aspects of study design, data interpretation, and dissemination. AHN maintained IRB approvals, regulatory documents, and records in a secure fashion. He was responsible for recruiting, consenting, and enrolling subjects, collecting and entering study data into a secure database, and assisting with manuscript and grant preparations. EEM was responsible for recruiting, consenting, and enrolling subjects, collecting and entering study data into a secure database, and assisting with manuscript and grant preparations. MLK was involved in intervention delivery and manuscript preparation. BF assisted with project planning, implementation, management, allocation generation, data fidelity, and data analyses. JJR served as a consultant on scientific design and analysis of study components concerning lifestyle factors and brain and cognitive health. YT was responsible for allocation generation, and data fidelity, management, and analyses. AAJS assisted with project implementation, data management and analyses, and dissemination. As PI, MKO provided oversight of all aspects of the project. She hired, trained, and supervised all study personnel. She provided oversight of participant recruitment, enrollment and retention, intervention delivery, data collection, analysis, and dissemination.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Merit Review Project number I01RX004828-01 (O’Connor, PI) from the United States Department of Veterans Affairs Office of Rehabilitation Research and Development Service (VA RR&D). The data from this study was collected as part of a larger clinical trial (NCT06006962). The contents of this publication do not represent the views of the Department of Veterans Affairs or the United States government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. To gain access, data requestors will need to sign a data access agreement.