
Abstract
Inflammatory bowel disease (IBD) is a chronic, multifactorial disease resulting from complex interactions between the immune system, gut microbiota, genetic susceptibility, and environmental factors. Although advances in pharmacologic therapies have improved disease control, increasing evidence indicates that lifestyle and environmental factors influence disease course and patient well-being. In this review, we assess the impact of lifestyle factors (diet, physical activity, sleep, mental health, and smoking) and environmental factors (pesticides, microplastics, and heavy metals) on IBD. Our manuscript highlights the importance of minimizing highly processed foods, such as those in the Western diet, while promoting a whole-food and Mediterranean diets, regular physical activity, and monitoring for micronutrient deficiencies. We also provide information on sleep disturbances, mental health, and disease activity, as well as interventions such as cognitive-behavioral therapy and mindfulness, which may improve the quality of life of these patients. Emerging evidence suggests that environmental pollutants, including microplastics and pesticides, may affect IBD risk and progression, highlighting the need for further research. Integrating structured lifestyle recommendations into clinical care may have a significant role in improving outcomes in patients with IBD.
“A low level of vitamin D has been associated with higher levels of inflammatory markers, increased disease activity, and clinical relapse.”
Introduction
The exact cause of Inflammatory Bowel Disease (IBD) remains unknown. However, several factors have been hypothesized to influence the development of the disease, including genetic, immune, and environmental factors. The role of each factor in the pathogenesis of the disease varies among patients, which may play a role in early or late onset of the disease in different patients. Significant progress has been made in identifying the many susceptibility gene loci, along with numerous discoveries of targets for disease management, which is reflected in the development of many new therapies.
1
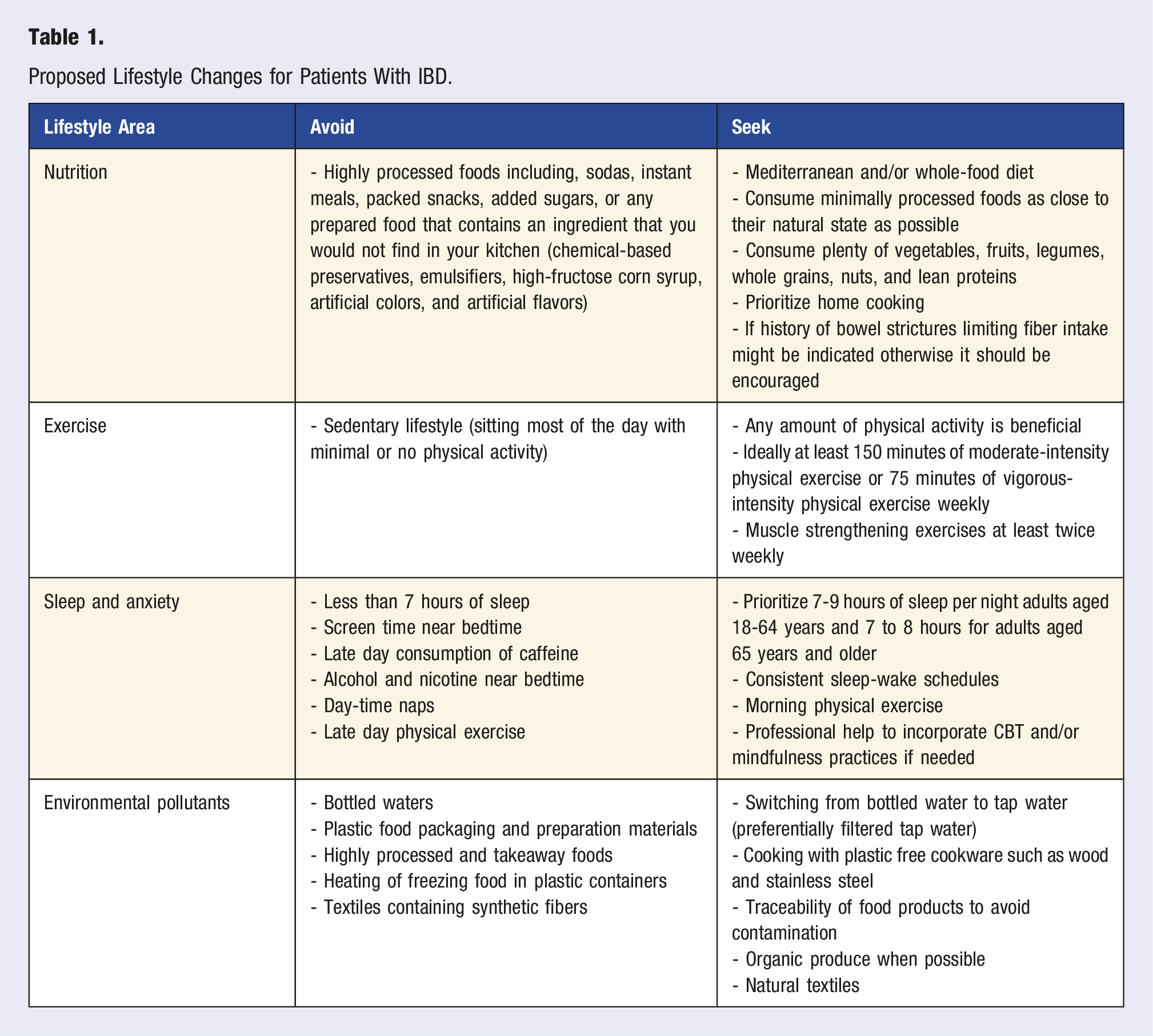
However, patients often inquire about the cause of their disease and are interested about a holistic approach to its management. Unfortunately, many gastroenterologists do not feel comfortable providing specific guidance beyond drug therapies and general dietary recommendations. While a drug-free approach may not be able to induce remission in many patients with IBD, the contributions of environmental factors, including lifestyle, should not be underestimated in the care of these patients. Lately, there has been a growing interest in studying the impact of lifestyle on the prevention and management of chronic diseases.2,3 Notably, recent research shows the benefits of dietary therapies in inducing and maintaining disease remission.4–6 Factors such as physical exercise, sleep, anxiety, and depression may correlate with disease activity.7,8 In addition, studies suggest that exposure to environmental pollutants, such as microplastics and pesticides, can also impact disease activity.9–14 Even though there are no specific guidelines regarding lifestyle changes in patients with IBD, there is evidence that optimizing each different lifestyle pillar can play a significant role in disease activity and quality of life in this patient population. For this reason, we review several environmental and lifestyle factors and suggest a practical approach to patient education (Figure 1 and Table 1). Lifestyle factors that may impact the risk and course of inflammatory bowel disease. Proposed Lifestyle Changes for Patients With IBD.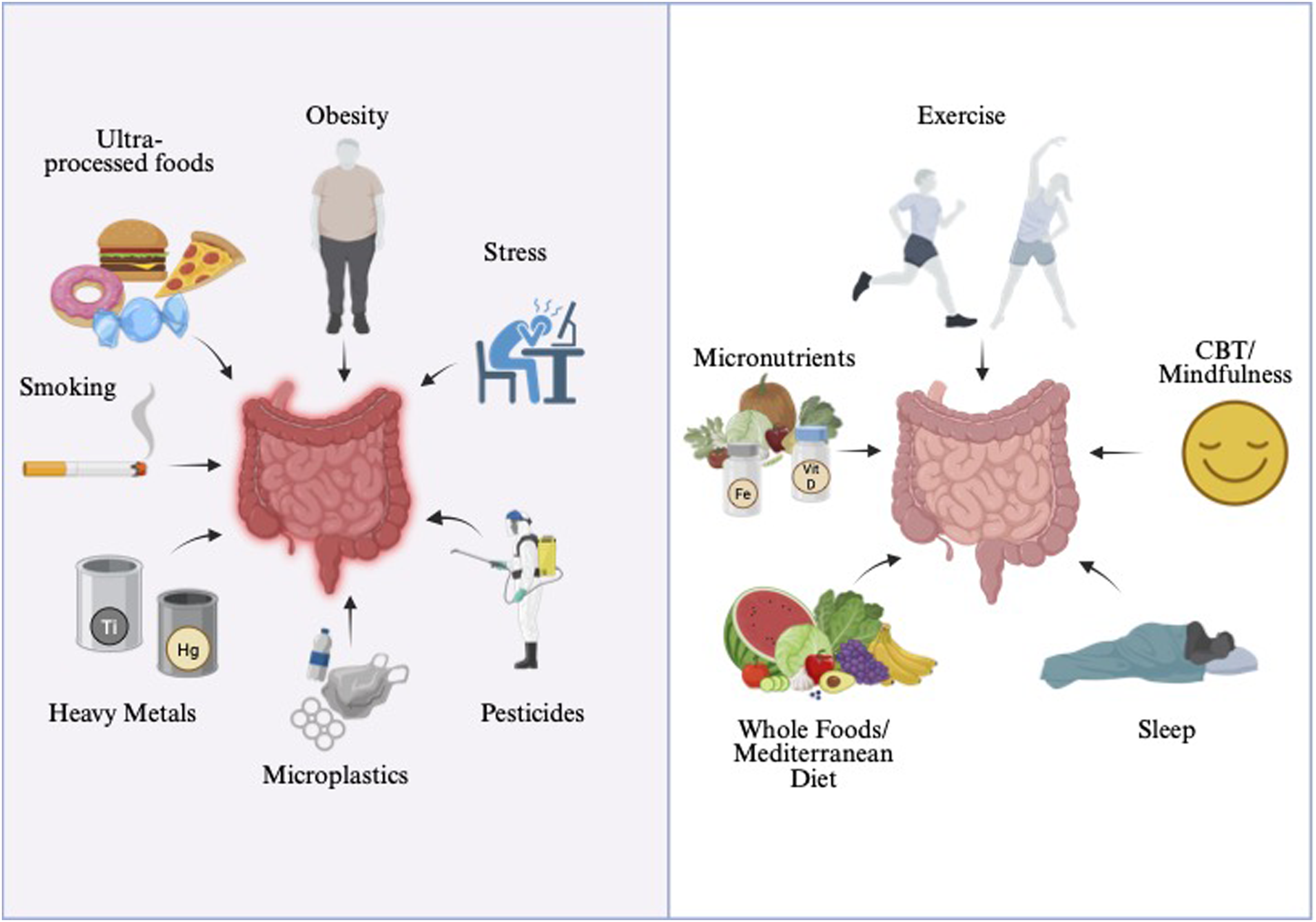
Environmental Pollutants
Microplastics and Other Endocrine Disruptors
The term microplastics (MPs) refers to plastic polymers that are less than 5 mm in size. 15 These are pollutants of concern due to their increasing accumulation in the environment and their inevitable consumption by humans through contamination of food and water.10,11 In addition, MPs have been associated with many adverse health outcomes.16,17 There are no studies demonstrating direct causality between MPs and IBD; however, several studies suggest their negative impact on gut health.10–12
For instance, an experimental study demonstrated that polystyrene MPs increase colonic permeability, exacerbate histopathological damage and inflammation, and reduce mucus secretion in mice with colitis. 18 Moreover, this study also showed that polystyrene MPs promoted secondary liver injury in mice with colitis, which can be significant in patients with IBD, especially those with concomitant primary sclerosing cholangitis. Other studies showed similar gut and liver toxicity effects in mice with colitis exposed to polystyrene MPs.19,20
Other types of MPs, including polyethylene and polypropylene, have also been linked to intestinal dysbiosis, inflammation, and increased permeability. 11
Direct correlation between the severity of IBD and the presence of MPs in feces was observed in the study of Yan et al. 10 The authors found significantly higher concentration levels of MPs in the feces of patients with IBD compared to healthy individuals. Moreover, they observed a positive correlation between the concentration of fecal MPs and the severity of IBD. Another study revealed a positive correlation between the level of MPs and fecal calprotectin levels. 12 However, it is important to know that these findings do not demonstrate causality and could suggest that IBD exacerbates the retention and/or excretion of MPs in the feces.
Bisphenol A (BPA) is a known endocrine disruptor associated with many health risks. A study in mice exposed to BPA revealed changes in the gut microbiome, including increased proportions of certain bacteria (Bacteroides, Mollicutes, Prevotellaceae, Akkermansia, Methanobrevibacter, and Sutterella) that have been linked to IBD. 21 A similar study showed that mice exposed to BPA had increased levels of Helicobacteraceae, which may also be associated with IBD. 22
The ubiquity of MPs makes their ingestion, inhalation, and dermal absorption inevitable. However, certain modifications to daily habits can help reduce its exposure. Water plays a key role in MPs consumption, with tap water containing significantly less plastic than bottled water. 23 In addition, higher levels of food processing are associated with increased amount of MPs contamination, hence reducing the consumption of highly processed foods can help decrease MPs intake. 24 The type of food packaging, the storage time and temperature also influence the transfer of plastic to food. 25 For this reason, prioritizing fresh unpackaged produce, avoiding plastic food containers and utensils, and opting for cookware made from ceramic, glass, or stainless steel is advised. Besides contamination from direct contact with plastic, MPs also accumulate in various species consumed by humans. Mollusks and crustaceans contain the highest MPs concentrations per gram of tissue. 26 When comparing fish muscle to beef, the amount of MPs exposure is relatively low and similar between the two. 24 On the other hand, dietary fiber may lower MP bioavailability in the GI tract by reducing transit time and by absorbing and entrapping plastic particles, thereby facilitating their excretion through feces. 27 Moreover, fiber is associated with higher production of SCFAs and may reverse MPs induced dysbiosis. 28 Importantly, store-bought fiber supplements can be contaminated with plastic, thus its primary source should come from whole foods. 29
Synthetic textiles such as nylon, rayon, elastane, or polyester significantly contribute to MPs exposure in the household through inhalation, dermal absorption, and ingestion. 30 Opting for natural fibers (cotton, linen, wool, and hemp), using HEPA-filtered vacuums, and improving indoor ventilation can reduce indoor concentrations of MPs. 31
Herbicides and Pesticides
Studies have shown a detrimental effect of herbicides and pesticides on the gut microbiome and, consequently, the potential to contribute to gastrointestinal-related diseases, including colorectal cancer.32–37 Moreover, these environmental pollutants can cause intestinal inflammation by affecting gut immune responses.38,39
The most widely used herbicide is glyphosate, also sold under the trademark Roundup®. Levels of glyphosate have been increasing in water at alarming levels, posing a significant threat to food safety.
A Canadian experimental study exposed Muc2−/− mice to two different levels of glyphosate, an acceptable level considered by Environmental Protection Agency or EPA (1.75 mg/kg bw/day) and the North American dose, calculated by a registered dietician based on literature values of glyphosate found in food products (0.1 mg/kg bw/day). The mice ingested glyphosate with water. Mice exposed to EPA levels of glyphosate had an earlier onset and more severe colitis. 40
Furthermore, research has shown that glyphosate exposure negatively impacts villous height, crypt depth, antioxidant enzyme activity, mRNA expression levels of inflammatory cytokines and transcription factors, apoptosis-related genes, and the gut microbiome. 41 Specifically, glyphosate reduces the relative abundance of the phylum Firmicutes and the genus Lactobacillus, which is linked to IBD. 41
A unique study evaluated the use of pesticides and the incidence of IBD in 68,480 pesticide applicators and their spouses and found positive associations for ever vs never use of 14 different pesticides. 42 In this study, the hazard ratios were highest for ever use of dieldrin (HR = 1.59, 95% CI: 1.03, 2.44), toxaphene (HR = 1.61, 95% CI: 1.17, 2.21), parathion (HR = 1.42, 95% CI: 1.03, 1.95), and terbufos (HR = 1.61, 95% CI: 1.17, 2.21). However, there was no association between glyphosate and the incidence of IBD in this population.
Pesticide exposure is influenced by occupational, residential/environmental, dietary, and sociodemographic factors. For instance, agricultural workers have significantly higher urinary pesticide metabolite levels than the general population. 43 Living in proximity to agricultural fields has consistently been identified as a significant determinant of pesticide exposure. 44 Nonetheless, diet is the primary source of pesticide exposure in the general population. 45 A randomized controlled trial showed that switching to an organic diet reduced urinary pesticide excretion by 91% (17 vs 180 μg/day, P < 0.0001). 46 Household food processing, including washing with water and/or sodium bicarbonate, peeling, and boiling, is an effective strategy for removing surface pesticides. 47
Testing for chronic pesticide exposure includes serum organochlorine pesticide panels (reflect cumulative lifetime body burden) and urinary pesticide metabolite panels. However, these tests have significant limitations and can be influenced by factors such as age, BMI, weight changes, and lipids.48,49 Moreover, urine tests are limited by extreme temporal variability and require more than approximately 30 urine samples to make an estimate. 50 Thus, we cannot make a recommendation for the use of testing for pesticide exposure but rather emphasize measures to reduce its exposure.
Heavy Metals
Heavy metals or trace elements are metallic elements with high density and atomic weight. While some are essential to human life in trace amounts, others pose potential for significant toxicity even at low concentrations. Industry and manufacturing waste are a cause of heavy metal pollution in our environment.
Several studies have shown that aluminum, cadmium, nickel, and mercury, in general, harm the intestinal mucosa and epithelial barrier function by generating oxidative stress and increasing inflammation.51–54
A study from Canada showed that levels of aluminum (79% vs 38.6%, P < 0.001) and mercury (63% vs 37.2%, P < 0.001) were higher in patients with CD compared to healthy controls. 55 On the other hand, the levels of titanium were lower in CD (59%) and UC (14%) relative to healthy controls (84.1%), P-values <0.0002 and <0.0001, respectively. Another study revealed the deposition of nickel in tissue specimens affected by CD. 53 Furthermore, nickel particles precipitated and exacerbated colitis and autophagy in mice. 53
Evidence showed that zinc oxide nanoparticles increased the cell viability and decreased the rate of apoptosis in heat-stressed bovine intestinal epithelial cells. 56 In humans, zinc deficiency has been significantly associated with increased risk of hospitalizations, surgeries, and disease-related complications in patients with CD and UC. 57 Furthermore, normalization of zinc led to improvement in these outcomes in the same patients. Similarly, in a blind intervention study, 41 patients with UC received a daily dose of 35 mg Zn gluconate for 30 days. In these patients, the gene expression of metallothionein 1G and ZIP-14, a metal transporter that is upregulated by inflammation, was significantly reduced. 58
In a pediatric IBD population, the profile of trace elements concentration in the blood serum at the time of IBD diagnosis was significantly different than that of the healthy control group. 59 Specifically, development of IBD was associated with low levels of iron, selenium, and zinc and elevated levels of copper and manganese. Similarly, in a study with 84 patients with CD, the levels of Manganese, Arsenic, Cadmium, Lead, and Uranium were higher in the CD group compared to the healthy group. 60
Heavy metal exposure occurs through occupational factors (mining, smelting, battery recycling, welding, construction, and manufacturing), tobacco use (particularly cadmium), private well systems (increased lead exposure), cosmetics, and dietary factors. For instance, fish contribute to mercury exposure; rice is a major source of arsenic; root vegetables, leafy greens, and cereals accumulate cadmium; and lead can be found in a variety of foods. Of note, organic produce generally contains lower concentrations of cadmium and lead. 61 Some nutritional interventions can reduce the absorption of certain heavy metals and mitigate their detrimental effects. Iron and calcium deficiency are associated with increased lead and cadmium absorption.62,63 Moreover, zinc and selenium supplementation have been shown to have protective effects against cadmium toxicity.64,65 When there is a significant risk of heavy metal exposure, it is reasonable to measure serum levels in IBD patients. Furthermore, testing for iron, selenium, and zinc levels, along with appropriate supplementation, should be considered.
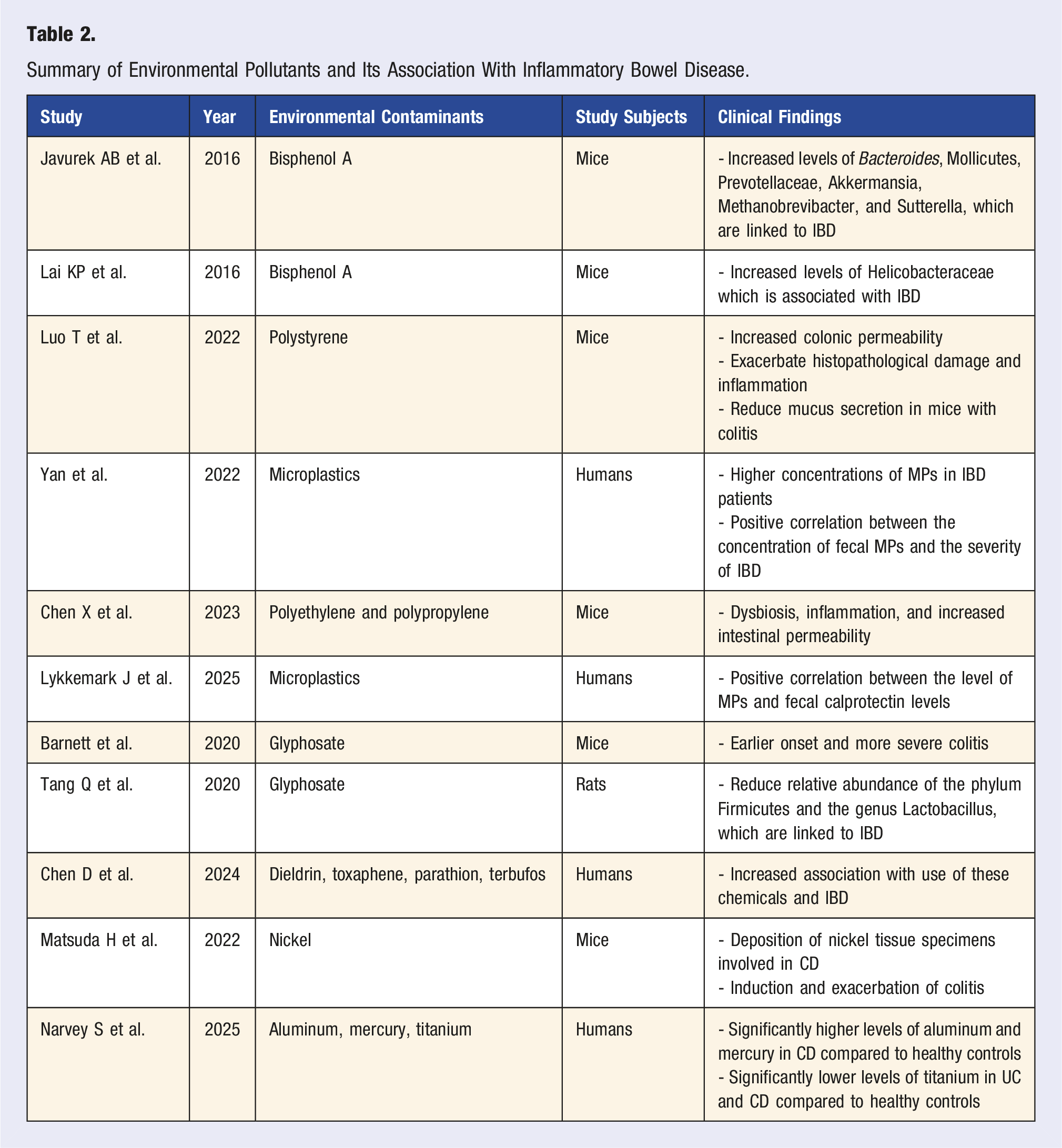
Summary of Environmental Pollutants and Its Association With Inflammatory Bowel Disease.
Lifestyle Factors
Exercise
Physical exercise has a positive effect on the immune system and may reduce systemic inflammation; however, there is limited data regarding its direct impact on the management of IBD. IBD patients report significantly lower levels of physical activity. 66 This may be related to the following barriers, including fatigue (53.9%), abdominal pain (25.7%), bowel incontinence (23.3%), and joint pain (22.3%).67,68
During physical exercise, skeletal muscles release several myokines that affect inflammatory pathways and exert autocrine, paracrine, and endocrine effects. 69 Physical exercise has been shown to increase the gut microbiome diversity and improve the functional metabolome, leading to enhanced host health. 69 This is especially important in IBD patients, given their lower microbiome diversity and abnormal immune response to the resident microbiota. 70 Moreover, physical exercise, particularly endurance training, increases short-chain fatty acid (SCFA)-producing bacteria. SCFAs play a significant role in the host by reducing inflammation through the inhibition of cytokines and inflammatory proteins. 71 Butyrate, a well-studied SCFA, induces the proliferation of colonic epithelium, promotes gut barrier integrity, and regulates host gene expression and immunity. 71
Women with UC have decreased lower limb strength, slower gait speed, and lower habitual physical activity compared to healthy women. 72 To address the skeletal muscle dysfunction and poor lower limb performance in women with IBD, 72 148 female IBD patients underwent an 8-week quadriceps progressive resistance training (20-minute sessions twice weekly), which resulted in significant improvement in quadriceps strength and overall intestinal symptoms. 73
Although physical activity has an overall positive effect on patients with IBD, its direct impact on disease activity remains controversial. 74 In a pilot study of 24 patients with IBD who completed an individualized exercise program (based on their fitness ability), a significant improvement in physical fitness, quality of life, systemic symptoms, and fatigue scores were reported, but disease control was not achieved. 75
A prospective study by Jones et al included 1308 patients with CD and 549 patients with UC or indeterminate colitis who were in remission. 76 At 6 months, a higher exercise level was associated with a significantly lower risk of active disease for CD (adjusted risk ratio: 0.72, 95% confidence interval: 0.55-0.94). Patients with UC/indeterminate colitis also had a lower rate of active disease, but this was not statistically significant (adjusted risk ratio: 0.78, 95% confidence interval: 0.54-1.13).
Another study evaluated the impact of a 16-week exercise program on quality of life and fatigue in 27 patients with IBD and showed a significant decrease in fat percentage and improved physical fitness. 7 In addition, there was an improvement in the quality of life (average 8 points on the IBDQ), systemic symptoms (mean difference 2.7; 95% CI 0.1-5.4, P = 0.043), and fatigue (Z = −2.296, P = 0.022). Unfortunately, disease control showed no significant improvement.
Despite several studies showing the overall benefit of physical activity in IBD, strenuous physical activity might pose a risk for intestinal mucosal damage. In 327 Japanese patients with UC, strenuous physical activity was inversely associated with mucosal healing (OR 0.45, 95% CI 0.23-0.89, P = 0.008) and complete mucosal healing (adjusted OR 0.24, 95% CI 0.07-0.62, P = 0.008). 77 The mechanism behind the link between strenuous physical activity and lack of mucosal healing in these patients is uncertain; however, underlying ischemia with subsequent pro-inflammatory cytokines might contribute to mucosal damage. 69
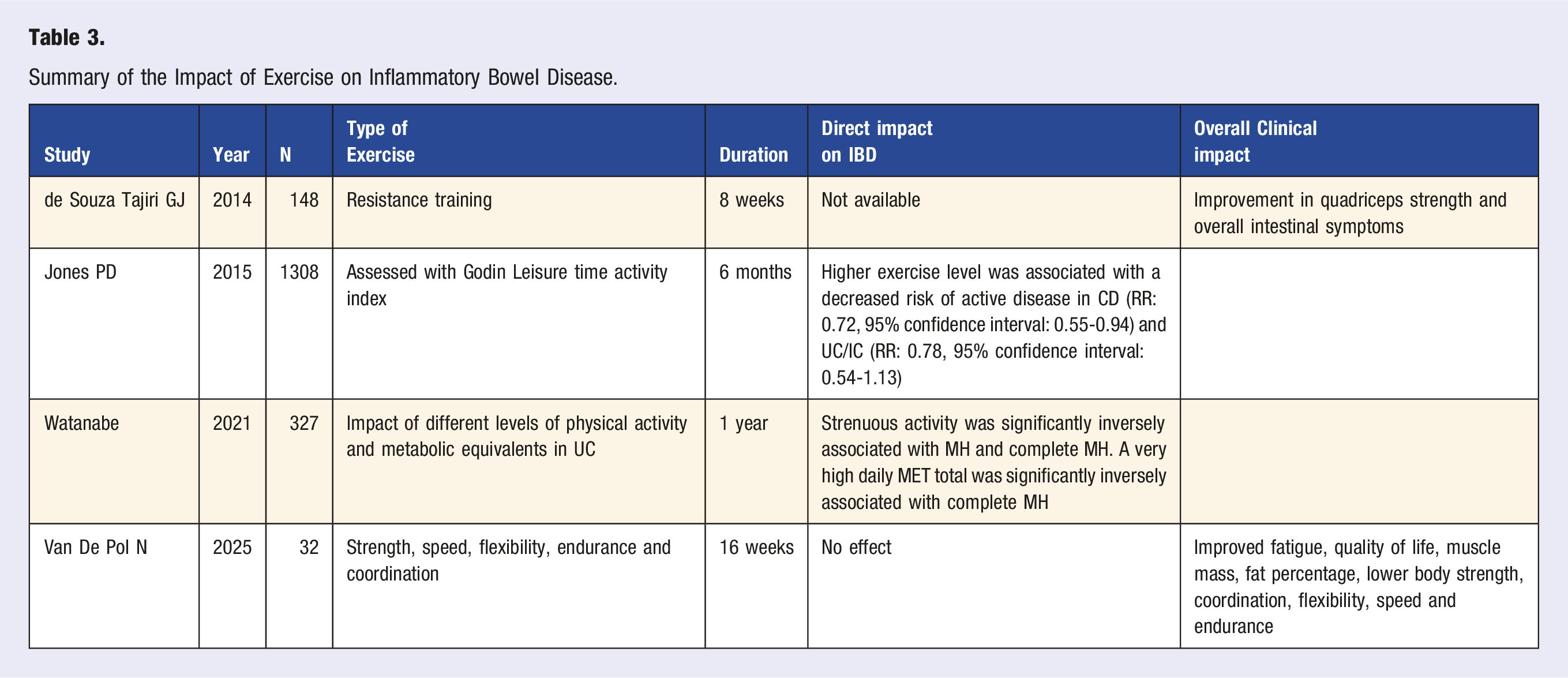
Summary of the Impact of Exercise on Inflammatory Bowel Disease.
Sleep Quality and Mental Health
Like other chronic diseases, IBD, particularly in active state, may adversely affect patients’ sleep and mental health, which can be detrimental to patients’ quality of life. Patients with active disease, anxiety, and higher financial burden experience lower quality of life. 78 A study of 2478 Chinese patients with IBD (55.33% UC, 44.67% CD) revealed a correlation between disease activity and anxiety, depression, sleep quality, and quality of life. 8 Sixty-two percent of patients had active disease, and from these, 29.5% had anxiety, 29.7% had depression, 71.1% reported sleep disturbances, and 50.1% had poor quality of life. In comparison, those patients who were in remission (38.2%) had significantly lower rates of anxiety (19.1%), depression (24.4%), and poor quality of life (17.4%), P < 0.001.
While a prospective study did not find a significant difference in the sleep disturbances among the IBD population with or without active disease,8,79 a systematic review and meta-analysis revealed that subjective and/or objective sleep disturbances were associated with an increased risk of disease activity. 80 The association between poor sleep and IBD is thought to be bidirectional, where increased disease activity can lead to worse sleep quality and inadequate sleep can be further detrimental to disease activity. 80 In addition, depressed mood, low quality of life, presence of disability, and extraintestinal manifestations have been identified as independent risk factors for sleep disturbance in the IBD population. 79
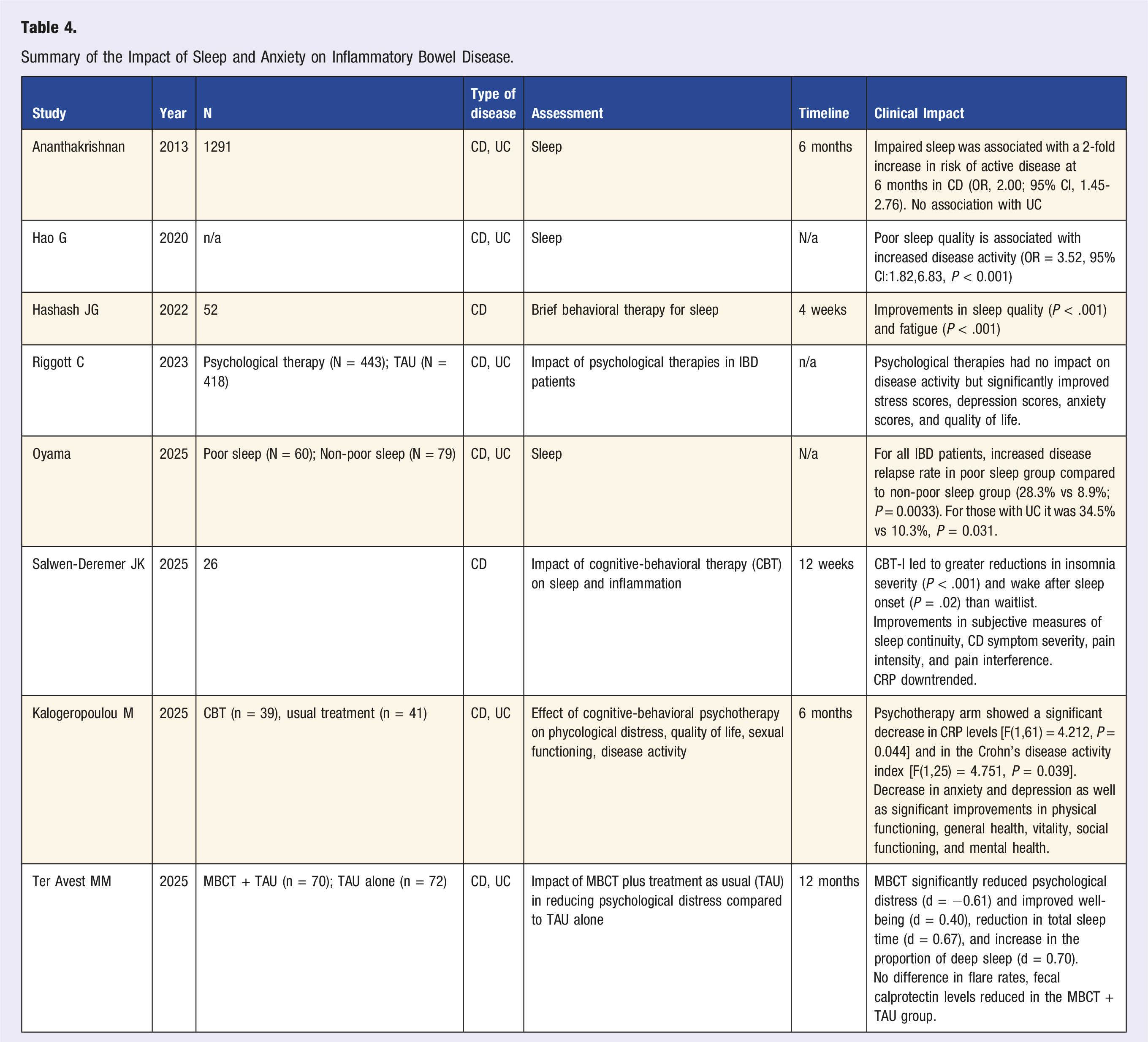
In a study involving 1291 patients with CD in remission, those experiencing sleep disturbances had a 2-fold increased risk of active disease at 6 months (adjusted odds ratio, 2.00; 95% confidence interval, 1.45-2.76). 81 Interestingly, in the same study, sleep disturbances did not impact disease activity in patients with UC. Despite the lack of association between sleep disturbance and disease activity in UC patients in the above study, a prospective Japanese study showed the opposite. 82 Among 139 patients with IBD, 60 (29 with UC and 31 with CD) reported chronic poor sleep. Those with chronic poor sleep had a significantly higher relapse rate (28.3% vs 8.9%; P = 0.0033). 82 Additionally, the relapse rate for UC was notably higher in the poor sleep group compared to the non-poor sleep group (34.5% vs 10.3%, P = 0.031). Furthermore, multivariate analysis revealed that chronic poor sleep was a clinical factor influencing IBD (OR = 6.69, 95% CI: 2.23-20.0, P = 0.0007) and UC (OR = 8.89, 95% CI: 1.57-50.2, P = 0.014) relapse.
In recent years, several clinical trials have shown possible positive results on the impact of cognitive-behavioral therapy (CBT) on sleep and inflammation in patients with IBD. 83 In a controlled pilot trial, 26 patients with insomnia and mild to moderate CD symptoms were randomized to receive CBT for insomnia or no intervention. 84 After 12 weeks, the treatment group experienced significantly greater reductions in insomnia severity and wakefulness after sleep onset compared to the control group. Furthermore, improvements were observed in the treatment group in subjective measures of sleep continuity, CD symptom severity, pain intensity, and pain interference.
Another multicenter randomized controlled trial included 142 patients with IBD in remission and at least mild levels of psychological distress and grouped them into 1) group delivered mindfulness-based cognitive therapy plus treatment as usual, and 2) treatment as usual. 83 Those who received mindfulness-based cognitive therapy had significantly reduced psychological distress (d = 0.61) and improved well-being (d = 0.4) post-intervention. Moreover, electroencephalography revealed a reduction in total sleep time and an increase in the proportion of deep sleep (d = 0.70). Interestingly, while there was no difference in flare rate between the two groups, fecal calprotectin levels were significantly reduced in the treatment group over a 12-month period (d = −0.49).
A 12-week two-phase open trial of CD patients evaluated the efficacy of a brief behavioral therapy (BBT) for sleep (4 weeks) followed by the addition of bupropion sustained release (8 weeks) for patients who continued to experience fatigue. 85 Significant improvement in sleep quality (P < .001) and fatigue (P < .001) was seen among 52 patients after 4 weeks of BBT. During phase II, 33 patients received BBT in addition to bupropion, and 19 received BBT only. At 8 weeks, both groups showed significant improvement in sleep, fatigue, anxiety, and depression without significant differences between the groups.
Carrying the diagnosis of IBD, particularly active disease, can have a negative impact on mental health. The rates of anxiety and depression are significantly higher in IBD patients compared to the general population, especially in patients with active disease. 86 A systematic review comparing IBD with healthy controls revealed that those with IBD had higher rates of anxiety (19.1% vs 9.6%) and depression (21.2% vs 13.4%). 86 In addition, when comparing patients with active vs inactive disease, those with active disease had higher rates of anxiety (66.4% vs 28.2%) and depression (34.7% vs 19.9%). Interestingly, patients were more likely to develop anxiety/depression before disease onset. 86
A recent prospective randomized controlled study evaluated the effect of cognitive-behavioral psychotherapy on psychological distress, quality of life, sexual functioning, and disease activity. 87 The study included a psychotherapy group and a treatment-as-usual (TAU) group. Regarding baseline characteristics, the two groups did not significantly differ in terms of age, type of disease, disease activity, type of therapy, and laboratory parameters. After 6 months, the psychotherapy arm showed a significant decrease in CRP levels [F(1,61) = 4.212, P = 0.044] and in the Crohn’s disease activity index [F(1,25) = 4.751, P = 0.039]. However, cytokine and calprotectin levels did not differ between the two groups. Furthermore, the treatment group reported a significant decrease in anxiety and depression as well as significant improvements in physical functioning, general health, vitality, social functioning, and mental health.
Large meta-analyses on the effect of psychological therapies on IBD show an overall improvement in patients’ quality of life, anxiety, and depression, especially in the short term.88,89 However, data do not support a substantial effect of psychological therapies on disease activity and risk for relapse. Nonetheless, larger randomized controlled trials are needed to evaluate disease activity outcomes using psychotherapies.
Summary of the Impact of Sleep and Anxiety on Inflammatory Bowel Disease.
Smoking
The Impact of Smoking in CD
The adverse impacts of cigarette smoking in CD have been well documented for several decades. 90 Smoking is associated with increased frequency of CD flares, more severe disease, and higher rates of surgery.90,91 A retrospective study with 3224 patients with CD showed that smokers had more strictures (22.6% vs 19.3%, P < 0.05) and less colonic involvement (7.2% vs 10.9%, P < 0.05) than nonsmokers. 92 In addition, treatment with steroids (91.6% vs 85.8%, P < 0.05), immunosuppressants (73.5% vs 63.6% P < 0.05), or anti-TNF drugs (31.4% vs 25.1%, P < 0.05) was significantly higher in smokers compared to nonsmokers. A systematic review revealed that smokers have higher odds of disease flares (OR, 1.56; 95% CI, 1.21-2.01), flare after surgery (OR, 1.97; 95% CI, 1.36-2.85), need for first (OR, 1.68; 95% CI, 1.33-2.12) and second surgery (OR, 2.17; 95% CI, 1.63-2.89) compared to nonsmokers. 93 In addition, CD patients who smoke, have higher rates of stricturing and penetrating disease. 94 Furthermore, a meta-analysis revealed a significant association of smoking and reduction of short-term clinical response and remission in CD patients treated with anti-TNFs. 95 However, another meta-analysis did not show a negative effect of smoking on initial response to infliximab in CD patients. 96 Importantly, the first study included a higher number of prospective studies compared to the second one.
Importantly, the odds of disease flare and the need for surgery in patients who quit smoking are not statistically different from those of nonsmokers.90,93 Moreover, smoking cessation reduces corticosteroid dependency compared to persistent smoking (24% vs 33%, P = 0.008). 97
The Impact of Smoking in UC
Studies have shown that smoking to be a possible protective factor for UC. A retrospective study with 556 patients with UC showed that smokers have a lower requirement for steroids and a lower risk for pancolitis than nonsmokers. 98 A study from 2001 showed that patients with UC who quit smoking had more severe disease with a higher rate of hospitalization, and a need for immunosuppressive therapy. 98 In this study, the rates of colectomy were similar between smokers, ex-smokers, and nonsmokers. However, this study only included 32 patients in each group (ex-smokers, nonsmokers, and current smokers). Other studies evaluated the use of transdermal nicotine and nicotine enemas for the treatment of UC and showed no benefit.99,100 A hospital-based cohort study revealed that smoking was associated with a reduced occurrence of UC and fewer hospitalizations (1.6 vs 2.5, P = 0.02) but increased the rate of new cancer development (16.0% vs 6.7%, P = 0.01) and mortality (16.0% vs 4.9%, P < 0.01). 94
A more recent study confirmed some protective effects of smoking in UC. Among 557 UC patients, current smokers had lower use of corticosteroids compared to nonsmokers. 101 Moreover, ex-smokers required a higher use of immunosuppressive therapies (36.2% vs 26.3%, P = 0.041) compared to current and never smokers. However, the rates of colectomy and hospital admission were not different amongst the groups.
In contrast to the results above, a nationwide population-based study with 6754 UC patients of whom 878 were smokers, showed that the rates in corticosteroid-requiring flares, thiopurine use, corticosteroid dependency, hospitalization, and colectomy were not different between smokers and nonsmokers. 102
Despite data on decreased risk of UC in smokers, the effects of smoking in the disease course in patients with UC are conflicting, and the risks of smoking outweigh any benefits.94,101–103
The Impact of Smoking on CD vs UC
To understand the contrasting effects of smoking on UC and CD, Miyauchi et al studied the microbiota composition of saliva, feces, and colonic mucosa, along with the fecal metabolite profile of IBD patients. 104 Patients with UC who smoked had higher levels of SCFAs and aromatic compounds in their feces compared to those who quit smoking, and smoking was linked to increased oral bacteria in the colonic mucosa. Furthermore, after the monocolonization of germ-free mice with Streptococcus mitis, one of the oral bacteria ectopically found in the colonic mucosa, interferon (IFN)-γ-producing T cells were induced in the colon. In addition, Streptococcus mitis also reduced inflammation in a mouse model of UC but worsened it in a model of CD.
Obesity
A significant number of patients with IBD are obese (15-40%). 105 Data on the influence of obesity on IBD course is conflicting, with some studies showing a negative effect while others show a positive one.106–109
A pooled analysis from 5 large prospective studies, including 601,009 participants, revealed that a BMI of ≥30 kg/m2 was associated with an increased risk of CD (pooled aHR, 1.34; 95% CI, 1.05-1.71, I2 = 0%) compared with a normal BMI. 110 There was no association between obesity and UC, though. Similarly, a meta-analysis with 1,044,517 participants demonstrated a significant association between obesity and risk of CD (HR: 1.42, 95% CI: 1.18-1.71, I2: 0.00) and no association between obesity and UC. 111
A cross-sectional and longitudinal study with 7296 patients with IBD (4748 patients with CD, 19.5% obese; 2548 patients with UC with intact colon, 20.3% obese) observed that obesity was independently associated with persistent disease activity or relapse in both patients with CD (class II or III obesity vs normal BMI: adjusted odds ratio, 1.86; 95% confidence interval, 1.30-2.68) and UC (adjusted odds ratio, 2.97; 95% confidence interval, 1.75-5.17). 109 Similarly, a study from Switzerland found that obese patients with CD were less likely to have disease remission (odds ratio 0.610, 95% confidence interval 0.402-0.926, P = 0.020) and more likely to have a complicated disease course (hazard ratio 1.197, 95% confidence interval 1.046-1.370, P = 0.009), but no negative effects were observed in patients with UC. 112
Opposite results were observed in the study of Pringle et al, a cross-sectional study evaluating the role of obesity in 846 patients with CD. 107 The authors found no associations between obesity and risk of perianal disease, stricturing disease, or surgery. Moreover, obesity was associated with a lower risk of penetrating disease (odds ratio [OR = 0.56; 95% confidence interval [CI], 0.31-0.99) compared to normal weight. Similarly, a retrospective study with 581 IBD patients showed that obese patients were less likely to receive anti-TNFs, require surgery, or hospitalization compared to non-obese patients (55.8 vs 72.1 %, P = .0001). 106
Several factors limit some of these results. For instance, weight loss can correlate with uncontrolled disease. Moreover, many of these studies lack assessment of visceral adiposity and total body fat (both of which may not correlate with BMI). In fact, a recent retrospective cohort study revealed that a higher visceral adipose tissue (VAT) to subcutaneous adipose tissue (SAT) ratio was associated with a shorter time to IBD flare (hazard ratio of 4.8 for VAT: SAT ≥1.0 vs VAT: SAT ratio <1.0) but this was not seen in regard to BMI (hazard ratio of 0.73 for BMI ≥25 kg/m2 vs BMI <25 kg/m2). 113 Another prospective study with 141 IBD patients on treatment with biologics and 51 healthy controls demonstrated that patients with higher intra-abdominal VAT were less likely to achieve corticosteroid-free deep remission (P < .001) or endoscopic remission (P = .02) compared to those with lower intra-abdominal VAT%. 114
Despite the conflicting data on obesity and disease activity, obesity is associated with higher anxiety, depression, fatigue, pain, and inferior social function scores in these patients.68,109
Malnutrition and the Role of Micronutrients
Unguided dietary changes are common in patients with IBD, particularly avoidance of certain foods such as those with gluten, dairy, vegetables, high fiber foods, and unprocessed red meat. 68 Around 76% of patients with IBD avoid certain food groups to prevent a disease flare, 86% avoid some food groups for fear of worsening a disease flare, and 67% modify their dietary habits after disease diagnosis. 115 These habits, along with the natural course of the disease, can lead to a poor nutritional status, with significant health impacts, including higher hospitalization, corticosteroid use, and disease flare.116,117 The degree of malnutrition amongst patients with IBD has consistently been shown to be worse than that of healthy controls. In a study involving 185 IBD patients, only 29% were well-nourished, compared to 79.3% in healthy controls. 2 A prospective study with 333 IBD patients showed a 16% prevalence of malnutrition, which was associated with a history of abdominal surgery, active disease, and food avoidance. 115 For these reasons, the American Gastroenterology Association recommends that all patients with IBD receive regular screening for malnutrition, which includes assessment of weight loss, edema, fluid retention, and fat and muscle loss. 6
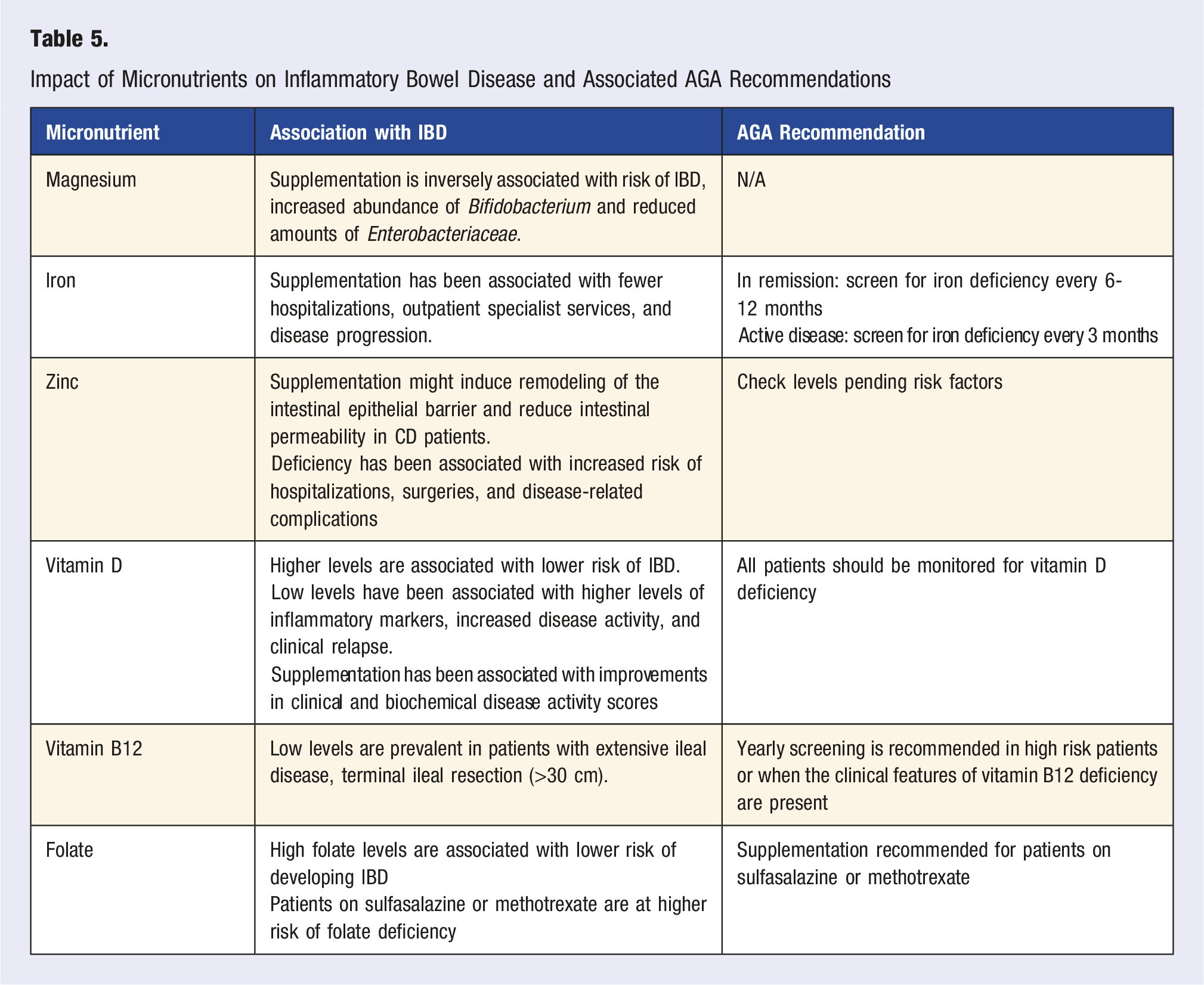
Even in the absence of malnutrition, insufficient essential minerals and vitamins are prevalent in patients with IBD (up to 78%).118,119 The etiology for these deficiencies are multifactorial, with intestinal mucosal inflammation, dietary restrictions, and anatomical changes related to surgeries playing roles.68,118 For this reason, patients with IBD should be regularly screened for micronutrient deficiencies.6,119 A study from New Zealand involving 213 patients with IBD, either with quiescent or mildly active disease, found inadequate intakes of calcium (69%), selenium (40%), and magnesium (26%). 68 Another study showed that CD patients with uncontrolled disease, have significantly lower serum levels of calcium and magnesium compared to CD patients who are in remission. 120 Magnesium plays a vital role in the immune system, gut barrier, and microbiome. 120 Furthermore, a high intake of magnesium has been inversely associated with the risk of developing IBD. 121 In colitic mice studies, magnesium supplementation increased the abundance of Bifidobacterium (associated with improved metabolic hemostasis, reduced intestinal lipopolysaccharide, and improved mucosal barrier function) and reduced the amount of Enterobacteriaceae (associated with dysbiosis, inflammation, and intestinal permeability). 122
Vitamin D deficiency is highly prevalent in the IBD population and significantly impacted by seasons. It has been shown that Vitamin D improves the intestinal barrier, enhances innate and adaptive immunity, and alters the microbiome. 123 In addition, a low level of vitamin D has been associated with higher levels of inflammatory markers, increased disease activity, and clinical relapse.123,124 Studies have shown a reduced risk of IBD with higher levels of vitamin D. 125 A meta-analysis of twelve randomized controlled trials and four observational studies evaluated the effect of vitamin D supplementation in IBD. 126 It revealed that supplementation is effective at correcting vitamin D deficiency and is associated with improvements in clinical and biochemical disease activity scores.
One in five patients with IBD has anemia, which is mainly related to iron deficiency. 127 The prevalence of iron deficiency in patients with active disease is approximately 71% and that of patients in remission is about 24%. 127 In addition, IBD patients with IDA are often under-treated. 128 A real-world analysis from Italy showed fewer hospitalizations, outpatient specialist services, and disease progression in patients with IBD on iron therapy compared to those without iron supplementation. 128 The appropriate type of iron replacement route should be taken into consideration in these patients. While oral iron supplementation is a more practical approach, there are concerns regarding its negative impact on intestinal microbiota by reducing beneficial bacteria and increasing species related to inflammation. 129 For these reasons, an individualized and careful selection is recommended. 129
Zinc plays an essential role in growth, immune function, and repair. Up to 40% of patients with IBD have zinc deficiency. 57 Based on limited data, zinc may have a positive impact on patients with IBD. It is thought that Zinc supplementation can induce remodeling of the intestinal epithelial barrier and reduce intestinal permeability (aka “leaky gut”) in patients with CD.130,131 In one study, the relative risk of CD was inversely associated with dietary zinc intake. 132 Moreover, zinc deficiency in IBD patients has been associated with increased risk of hospitalizations, surgeries, and disease-related complications. 57
CD patients with extensive ileal disease, terminal ileal resection (>30 cm), and patients who had undergone ileoanal pouch surgery are at high risk of vitamin B12 deficiency. The AGA recommends that IBD patients be evaluated for this deficiency every year. 6 The prevalence of B12 deficiency in CD is around 33% and for UC, around 16%. 133 However, given that body stores are underrepresented by serum levels, underdiagnosis of vitamin B 12 deficiency is common. 6 Once the deficiency is documented, these patients need lifelong replacement.
An umbrella review of meta-analyses identified that high folate levels were associated with a lower risk of developing IBD. 125 Patients on sulfasalazine or methotrexate have are at risk for folate deficiency and should be adequately supplemented. Although there is no data on the benefits of folate supplementation on disease progression, a systematic review and meta-analysis found a protective effect of folic acid supplementation on the development of colorectal cancer in patients with IBD, with a pooled hazard ratio of 0.58 (95% confidence interval, 0.37-0.80). 134
Impact of Micronutrients on Inflammatory Bowel Disease and Associated AGA Recommendations
Dietary Habits and the Risk of IBD
The Western diet is distinguished by the high consumption of processed meat, refined grains, sugar, sugar-sweetened beverages, high-fructose products, high-fat dairy products, fried foods, and ultra-processed foods (UPFs), along with a low intake of fiber-rich foods such as vegetables and fruits. 135 This dietary pattern has been shown to contribute to immune dysfunction, microbial dysbiosis, and disruption of the intestinal barrier. 136
Historically, the incidence and prevalence of IBD in Asian populations have been lower than in white population of Western countries; however, these rates are rapidly increasing among Asians. 137 To evaluate the impact of a Westernized diet on the development of IBD, one study examined the lifestyle of Asian immigrant children with IBD in the U.S. 3 Asian immigrant children with IBD had similar disease phenotypes as non-Asians, as well as a typical Westernized diet instead of a traditional Asian diet.
A recent systematic review and meta-analysis aimed at understanding the relationship between diet and IBD. The study included 2043601 participants; from these, 1902 developed CD and 4617 developed UC. An inflammatory diet (pooled aHR 1.63, 95% CI: 1.26, 2.11) and UPFs (pooled aHR 1.71, 95% CI: 1.36-2.14) were associated with an increased risk of CD. Furthermore, high fiber intake (pooled aHR 0.53, 95% CI: 0.41-0.70), Mediterranean diet (pooled aHR 0.59, 95% CI: 0.43-0.81), healthy diet (pooled aHR 0.70, 95% CI: 0.54-0.91), and unprocessed or minimally processed foods (pooled aHR 0.71, 95% CI: 0.53-0.94) were associated with a lower risk of CD. No association was found between diet and UC.
Dietary Therapies
Specific diets for the treatment of IBD have been studied. Exclusive Enteral Nutrition (EEN) can be an effective approach to induce remission in patients with CD, particularly in the pediatric population. 6 It consists of a 6 to 8-week therapy with commercially available liquid formulations. EEN is often recommended as a steroid-sparing therapy and shows similar and even superior clinical outcomes compared to corticosteroids in inducing remission in children. 138 Its positive impact is thought to be related to the beneficial changes in the microbiome and its low salt content. However, adults have difficulty adhering to EEN, which has led to limited studies in this population and underutilization in clinical practice. Nonetheless, several studies demonstrated that EEN is a safe and effective therapy to induce remission in adult patients with CD.139–141 Furthermore, it can treat malnutrition, reduce obesity, and increase lean mass.119,139
To improve the tolerability of Enteral Nutrition (EN), studies have investigated a Partial Enteral Nutrition (PEN) diet, which combines a solid diet with EN. Results from a randomized controlled trial in children with CD showed that PEN, when combined with an unrestricted solid diet, did not suppress inflammation in patients, while EEN suppressed inflammation. 142
However, the Crohn’s disease exclusion diet (CDED) combined with PEN is effective at inducing remission in patients with mild to moderate CD.143–145 In a study of children with mild to moderate CD, 37 children were given CDED plus PEN, and 31 children received EEN followed by PEN. 145 At week 12, 75.6% of children in the CDED plus PEN group were in corticosteroid-free remission compared to 45.1% of children who received EEN followed by PEN (P = 0.01; odds ratio for remission in children given CDED and PEN, 3.77; CI 1.34-10.59). Interestingly, a study including 11 adults and 10 children with CD, who lost response to a biologic despite dose escalation or combination therapy, and were treated with CDED combined with PEN for 12 weeks, showed favorable results. 143 Clinical remission, as determined by the physician’s global assessment and the Harvey-Bradshaw Index after 6 weeks, was achieved in 13 out of 21 cases (61.9%). The mean Harvey-Bradshaw Index decreased from 9.4 ± 4.2 to 2.6 ± 3.8 (P < 0.001), the mean CRP decreased from 2.8 ± 3.4 to 0.7 ± 0.5 (P = 0.005), and the mean albumin increased from 3.5 ± 0.6 to 3.8 ± 0.5 (P = 0.06).
Due to variability in studies regarding patient populations, types of formulas (polymeric vs elemental), and types of enteral nutrition therapy (partial vs exclusive), EEN and PEN are currently not recommended as maintenance treatments. However, studies show promising results on adopting the CDED plus PEN diet for maintenance of remission.146,147
Given the difficulty of adhering to the highly restrictive EEN and even PEN, some studies have assessed the impact of exclusively solid food diets in IBD. A meta-analysis showed positive results at inducing remission with an exclusive Mediterranean diet in children with mild to moderate CD and with the CDED in adults with CD. 148 A 2025 randomized controlled study compared a specific whole foods diet (Tasty&Healthy) that excludes processed food, gluten, and dairy to EEN. 5 It included 83 patients aged 6 to 25 years old, of whom 41 received the Tasty&Healthy diet, and 42 received the EEN. After 8 weeks, 56% of the Tasty&Healthy group vs 38% of the EEN group (aOR, 2.5; 95% CI, 0.98-6.3; P = .1; per-protocol: 67% vs 76%; P = .47) achieved symptomatic remission. fecal calprotectin <250 mg/g was observed in 34% vs 33% (aOR, 0.97; 95% CI, 0.37-2.6; P = .84) and Mucosal-Inflammation Noninvasive index score <8 in 44% vs 31% (aOR, 1.8; 95% CI, 0.7-4.5; P = .33) respectively. Furthermore, microbiome diversity improved in the Tasty&Healthy group and declined in the EEN group, and microbiome species associated with inflammation decreased in the Tasty&Healthy group and increased in the EEN group. Similar improvements of the microbiome were reported with the CDED. 145 The positive impact of the Mediterranean diet on IBD has been shown in a prospective randomized study of 100 IBD patients, aged 12 to 18 year, with mild to moderate disease activity. The study revealed that better adherence to the Mediterranean diet improved clinical scores (PCDAI and PUCAI) and most inflammatory markers (CRP, calprotectin, TNF-α, IL17, IL12, and IL13). 149 Similarly, a study analyzing the impact of a Mediterranean diet on IBD patients over 6 months found that fewer patients on stable therapy had active disease (UC T0 14 of 59 [23.7%] vs T180 4 of 59 [6.8%], P = 0.004; CD T0 9 of 51 [17.6%] vs T180 2 of 51 [3.0%], P = 0.011), along with reductions in inflammatory biomarkers. 150 Additionally, the quality of life improved in both UC and CD. Due to the significant benefits with a Mediterranean diet, the AGA guidelines suggest that, unless there is a contraindication, patients with IBD should follow a Mediterranean diet and avoid ultra-processed foods, added sugar, and salt. 6
Conclusions
IBD is a disease with a complex multifactorial pathogenesis involving the immune system, gut microbiome, and environmental factors. Our review highlights how several environmental and lifestyle factors may impact the disease course and the well-being of patients with IBD. Although there are several available advanced drugs for the treatment of IBD, physicians should not underestimate the importance of lifestyle factors including diet, exercise, sleep, mental health, and smoking cessation in these patients.
The detrimental effects of a Westernized diet along with the benefits of whole-food and Mediterranean diets on disease course, particularly in patients with CD, are well established and warrant greater emphasis in clinical practice. Patients should also be encouraged to engage in regular physical exercise given its effect on improving physical fitness, reducing fatigue, enhancing overall quality of life, and its possible role in lowering the risk of active disease in patients with CD.
Physicians should counsel patients who smoke on the importance of smoking cessation and remain vigilant in assessing micronutrient deficiencies, providing replacement therapy when indicated. While a direct relationship between sleep disturbances, mental health, and disease activity remains unclear, addressing sleep problems, anxiety, and depression with CBT and/or mindfulness can significantly improve overall well-being and systemic symptoms in IBD patients.
In an era of increasing exposure to environmental pollutants, including MPs, pesticides, and heavy metals, more studies are needed to understand their impact on IBD risk and disease course, along with strategies to minimize ingestion of these substances.
Incorporating a systematic approach to patient education focused on lifestyle modifications may have a meaningful and positive effect on disease outcomes in individuals with IBD.
Footnotes
Author Contributions
Proposed concept for review, collection of relevant information, drafting the article, and revised the manuscript with critical revisions (TD), edited the article, critical revision of the article, and final approval of the version to be published (HV).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.