
Abstract
“Supervised combined aerobic-plus-resistance training (CET) yields larger cardiometabolic benefits than unsupervised or usual-care programs.”
Introduction
Type 2 diabetes mellitus (T2DM) is a rapidly expanding global public health problem. An estimated 589 million adults (11.1%) currently live with diabetes, the majority (90 - 95%) being T2DM. Prevalence, morbidity, and mortality are projected to rise to 853 million by 2050.1–3 In the United States, in 2023, an estimated 40.1 million people (12%) had diabetes in 2023, of whom 90-95% had T2DM.4,5 Globally, diabetes accounted for more than 1.6 million deaths in 2021 and contributed substantially to premature cardiovascular mortality.2,3
T2DM is characterized by hyperglycemia, insulin resistance, and progressive β-cell dysfunction, which, if uncontrolled, can damage the heart, vasculature, eyes, kidneys, and nerves. 6 Adults with T2DM are commonly overweight, obese, or have remarkable abdominal adiposity. These characteristics, which drive the increasing prevalence of the disease, are inextricably linked to obesogenic diets, physical inactivity, and population aging.6,7 Regular physical activity (PA) remains a cornerstone strategy for the prevention and management of T2DM.7,8 Current guidance recommends combined aerobic and resistance training (e.g., ≥150 minutes/week of moderate aerobic activity across ≥3 days plus resistance training on ≥2 nonconsecutive days). Higher targets of 200-300 minutes/week are recommended by the ACSM and the ADA for overweight/obese adults with T2DM.5,9
Despite clear recommendations, adherence is poor: only about 24%–32% of adults with diabetes meet aerobic targets, about 11%–20% meet muscle-strengthening guidelines, and only 6%–12% meet both, with rates lower in nonmetropolitan and underserved communities.4,10 Barriers include limited access to supervised programs, unclear clinical referral pathways, socioeconomic constraints, comorbidity, low motivation, and insufficient community resources.11,12
Current evidence indicates that combined exercise training (CET) may exert a larger effect in improving glycated hemoglobin (HbA1c), body composition, lipid profiles, blood pressure BP), vascular function, and cardiorespiratory fitness (VO2max) more consistently than single-modality programs.13–16 Additionally, there is evidence to suggest that supervision of exercise may play a critical role in mitigating these cardiometabolic effects and improving motivation, physical literacy, self-efficacy, social support, and quality of life,17–20 which in turn could facilitate sustained behavior change and long-term adherence to exercise.
This synthesis will evaluate how supervised CET influences cardiometabolic outcomes, adherence, and QoL in adults with T2DM, identifying supervision features as effect modifiers, and will translate findings into equity-focused, practice-ready recommendations for clinicians, exercise professionals, and community program leaders.
Methods
We searched PubMed Central, ScienceDirect, and Google Scholar for English-language studies published from 2017 to 2026. Search terms combined synonyms for the clinical population, intervention, and outcomes using Boolean operators (e.g., “diabetes” OR “type 2 diabetes” AND “exercise” OR “physical activity” AND “combined” OR “combined training” AND “aerobic” AND “resistance” AND “adherence” AND “quality of life” AND “supervision”). Searches were limited to human studies of adults (≥18 years). Titles and abstracts were screened for relevance; full texts were retrieved when eligibility was uncertain.
Inclusion Criteria
We included studies of combined aerobic and resistance training in adults with T2DM that reported cardiometabolic outcomes (e.g., HbA1c, fasting glucose, lipids, blood pressure), adherence, or quality-of-life measures, with baseline and post-intervention data included. We prioritized randomized controlled trials (RCTs), controlled clinical trials, and high-quality observational and synthesis studies (systematic reviews/meta-analyses).
Exclusion Criteria
We excluded studies of type 1 or gestational diabetes, interventions that did not combine aerobic and resistance exercise, pediatric populations, non-human studies, and non-English reports.
Results
Twenty-three studies met the inclusion criteria. Designs comprised 12 RCTs, (13, 15, 16, 20, 22, 23, 24, 27, 28, 31, 32, 34), 5 systematic reviews/meta-analyses (14, 19, 25, 33, 35), 4 observational/epidemiologic or cohort analyses (1, 3, 4, 10), and 2 qualitative/adherence studies (17, 36). The RCTs were mainly short to medium-duration (8-52 weeks), with sample sizes ranging from ∼20-60 to ∼100-500. The largest pragmatic trials (e.g., STRRIDE-related) had the largest cohorts (15). The 5 syntheses pooled 6-20 trials each and reported pooled effects on HbA1c, fasting glucose, lipids, inflammatory markers, fitness, and body composition (14, 19, 25, 33, 35). Most RCTs enrolled mixed-sex samples (9 of 12: 15, 20-24, 28, 31, 32); 2 trials primarily recruited men, and one focused on postmenopausal women (34). Several syntheses conducted subgroup analyses by sex and other moderators when data allowed (19, 25).
Impact of Supervised CET on Cardiometabolic Risk Factors
CET involves aerobic + resistance training. Recent pooled evidence indicates that aerobic and resistance training can be performed in the same session, with dramatic cardiometabolic effects. 21 However, this synthesis will focus on separate-day training for aerobic and resistance training. The cardiometabolic outcomes reported include glycemic control, body composition, lipid profile, insulin sensitivity/resistance, systemic inflammation, cardiovascular factors, and VO2max.
Glycemic Control (HbA1c & FBG)
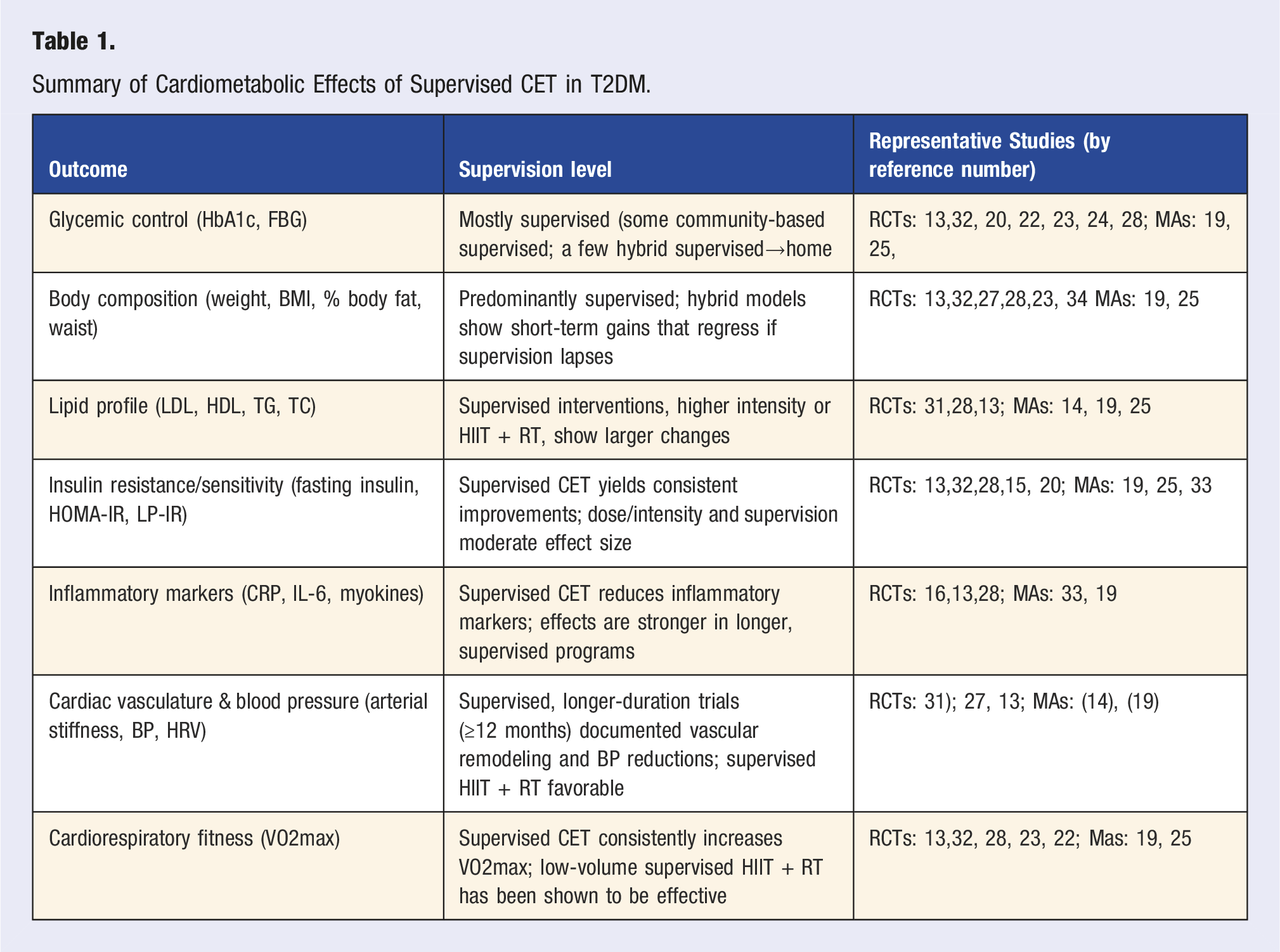
Five randomized trials, one systematic review, and one meta-analysis report that CET reduces HbA1c and FBG in adults with T2DM. A community-based trial found no HbA1c change with once-weekly CET but demonstrated frequency-dependent benefits (≥3×/week, ∼50% adherence) in the higher-frequency arm. 22 A 12-week trial showed significant reductions in fasting/postprandial glucose and HbA1c vs usual care, 20 and a 4-arm RCT reported lower FBG after CET vs controls. 13 An 8-week supervised CET program (HIIT or MICT) produced comparable 8-week HbA1c improvements, though gains largely regressed at 12 months when adherence fell. 23 In normal-weight adults, CET and strength training yielded similar HbA1c declines. 24 A meta-analysis of 20 studies (n = 1192) found significant HbA1c reductions in overweight/obese adults, 19 while a smaller meta-analysis reported no pooled HbA1c difference but greater FBG reductions vs aerobic training alone. 25 Overall, CET improves glycemia, but effect size and durability depend on dose, intensity, supervision, adherence, and study design; accompanying body-composition changes may partly mediate these benefits. 26
Body Composition
Four randomized controlled trials and one meta-analysis report meaningful improvements in body composition following CET. Banitalebi et al 27 found that sprint-interval and CET produced similar BMI reductions vs usual-care controls. Ambelu and Teferi’s head-to-head trial showed greater mean reductions in BMI and body-fat percentage in exercise groups after adjusting for diet, age, and sex. 13 Francois et al 28 demonstrated that body-fat declines following HIIT plus once-weekly resistance were attributable to training and not augmented by post-exercise protein supplementation. Supervision emerged as a key modifier: fully supervised interventions and supervised-to-home hybrid programs (e.g., Gajanand et al 23 ) produced significant fat-mass decreases at 8 weeks, whereas gains often regressed by 12 months when supervision and adherence waned; brief supervised-then-home protocols also improved body fat vs HIIT or standard care while supervision persisted. 20 A meta-analysis of 20 CET studies (n = 1192) reported a pooled significant reduction in BMI. 19 Collectively, evidence indicates that CET reliably reduces adiposity and BMI, which likely mediates improvements in insulin resistance and lipid profiles, and that sustained supervision/support enhances effect magnitude and durability.
Lipid Profile
Lipid abnormalities have been shown to contribute to insulin resistance, a metabolic component of T2DM, through multiple mechanisms. Conversely, insulin resistance can lead to lipid abnormalities. 29 The cluster of lipid abnormalities (Dyslipidemia)- includes high LDL cholesterol, low HDL cholesterol, and high triglycerides. 30 Of the included studies, one long-term RCT and 2 pooled analyses evaluated CET’s effects on lipids in adults with T2DM. In a 1-year trial comparing moderate-intensity continuous training + resistance (MCT + RT) vs high-intensity interval training + resistance training (HIIT + RT), Magalhães et al 31 found significant improvements in HDL, LDL, and total cholesterol only in the HIIT + RT arm. A meta-analysis of 6 RCTs (n = 366) likewise reported that combined aerobic-resistance programs produced significant reductions in LDL-C and triglycerides, and increases in HDL-C, compared with aerobic training alone. 25 A larger comparative systematic review of 15 studies (≈1794 participants) concluded that CET yielded the most pronounced cardiovascular lipid benefits, including an approximate 10% reduction in LDL cholesterol. 14 Collectively, supervised, adequately dosed CET, particularly when combined with higher-intensity aerobic work, appears to offer modest but clinically relevant improvements in lipid profiles among adults with T2DM.
Insulin Sensitivity/Insulin Resistance
Improvements in lipid metabolism frequently accompany enhanced insulin sensitivity. In a 10-week trial, Banitalebi et al 32 reported significant HOMA-IR reductions for both sprint-interval and combined training vs control. Other RCTs found CET with high-intensity aerobic plus resistance lowered circulating insulin and inflammatory mediators linked to insulin resistance.16,33 A comparative trial also showed greater HOMA-IR improvement for CET vs HIIT or usual care. 20 In a large 8-month RCT (n = 508) evaluating ten exercise modalities, Ross et al 15 identified CET among the 3 modes that significantly improved LP-IR and diabetes-risk scores. Two meta-analyses19,25 pooled multiple trials and confirmed combined training’s benefits on insulin-resistance biomarkers. Studies using supervised or supervised-to-home delivery generally reported larger, more durable improvements than unsupervised interventions, indicating supervision and adherence support are important effect modifiers. Improved lipid profile and insulin sensitivity are mechanistically linked to reduced systemic inflammation, better vascular function, and lower blood pressure in adults with T2DM.
Inflammatory Markers
CET reduces systemic inflammation in adults with T2DM across RCTs and meta-analyses. AL-Mhanna et al 19 reported significant reductions in CRP, IL-6, and related markers after CET, with larger effects for interventions >12 weeks. In their 12-week RCT (n = 59), Sabouri et al 16 demonstrated significant declines in IL-6 and CRP following CET and high-intensity protocols. A systematic review and meta-analysis 33 similarly found that CET programs improved inflammation markers in middle-aged and older adults with T2DM, supporting the anti-inflammatory effects of CET. The comparative systematic analysis by Mousavi Zadeh et al 14 corroborates these findings across multiple studies, showing greater reductions in inflammatory markers with CET vs single modalities. Additionally, one study reported lower circulating apolipoprotein J after CET intervention in postmenopausal women. 34 Collectively, RCTs and pooled analyses indicate that supervised, adequately dosed CT meaningfully lowers systemic inflammation in T2DM.
Cardiac Vasculature and Blood Pressure
CET yields consistent vascular and blood-pressure benefits in adults with T2DM across randomized trials and pooled analyses. A 1-year RCT reported vascular remodeling and improved arterial stiffness indices after CET. 31 Smaller intervention studies also show reductions in systolic and diastolic BP following combined training. 13 Meta-analyses and systematic reviews corroborate these findings: Al-Mhanna et al 19 found significant BP improvements after CET and a comparative review likewise reported larger cardiovascular gains, including 9/6 mmHg systolic/diastolic improvement in BP with CET vs single-modality training. 14 Overall, supervised, adequately dosed CET over months reliably improves vascular function and lowers BP in T2DM. These findings underscore the importance of CET in reducing cardiovascular risk in adults with T2DM.
Cardiorespiratory Fitness (VO2max)
Combined evidence from 4 randomized trials and one recent meta-analysis shows CET reliably increases VO2max in adults with T2DM. RCTs23,27,28 and related trials enrolled small-to-moderate samples (typically 20-150 participants per study) and ran from short (8-12 weeks) up to 1 year, reporting significant post-intervention VO2max gains following supervised CET protocols. The low-volume HIIT-style CET trial, 23 demonstrated meaningful improvements in VO2max with time-efficient sessions. Meta-analysis, 19 pooling multiple trials confirms pooled VO2max increases, with larger effects linked to greater total weekly volume, adequate resistance intensity, and supervised delivery.
Summary of Cardiometabolic Effects of Supervised CET in T2DM.
Exercise Prescription: Modalities, Intensity, Frequency, Duration
Strength Component
Across trials, resistance modalities included free weights, machines, resistance bands, and bodyweight. Intensity was typically moderate–high (60-80% 1-RM), with 2-4 sets of 8-15 repetitions per major muscle group, performed 2-3 nonconsecutive days per week. Programs incorporated progressive overload and were supervised to ensure technique and safe load progression, aligning with ACSM guidance for adults with T2DM. 9 Study durations ranged from 8 weeks to 12 months (commonly 12 weeks to 1 year).
Aerobic Component
Aerobic modalities included treadmill, cycling, and brisk walking, usually delivered ∼3 sessions/week (range 2-5). Continuous aerobic training was prescribed at moderate intensity (≈50-75% HRmax or 60-70% VO2max) for 30-60 minutes per session; HIIT protocols used brief high-intensity intervals (80-95% HRmax) with lower-intensity recovery. Programs were generally supervised or partly supervised with progressive overload to maintain targets. These combined, supervised prescriptions (aerobic + resistance) consistently produced the most reliable cardiometabolic improvements in adults with T2DM.5,9
Impact of Supervised CET on Adherence and Quality of Life
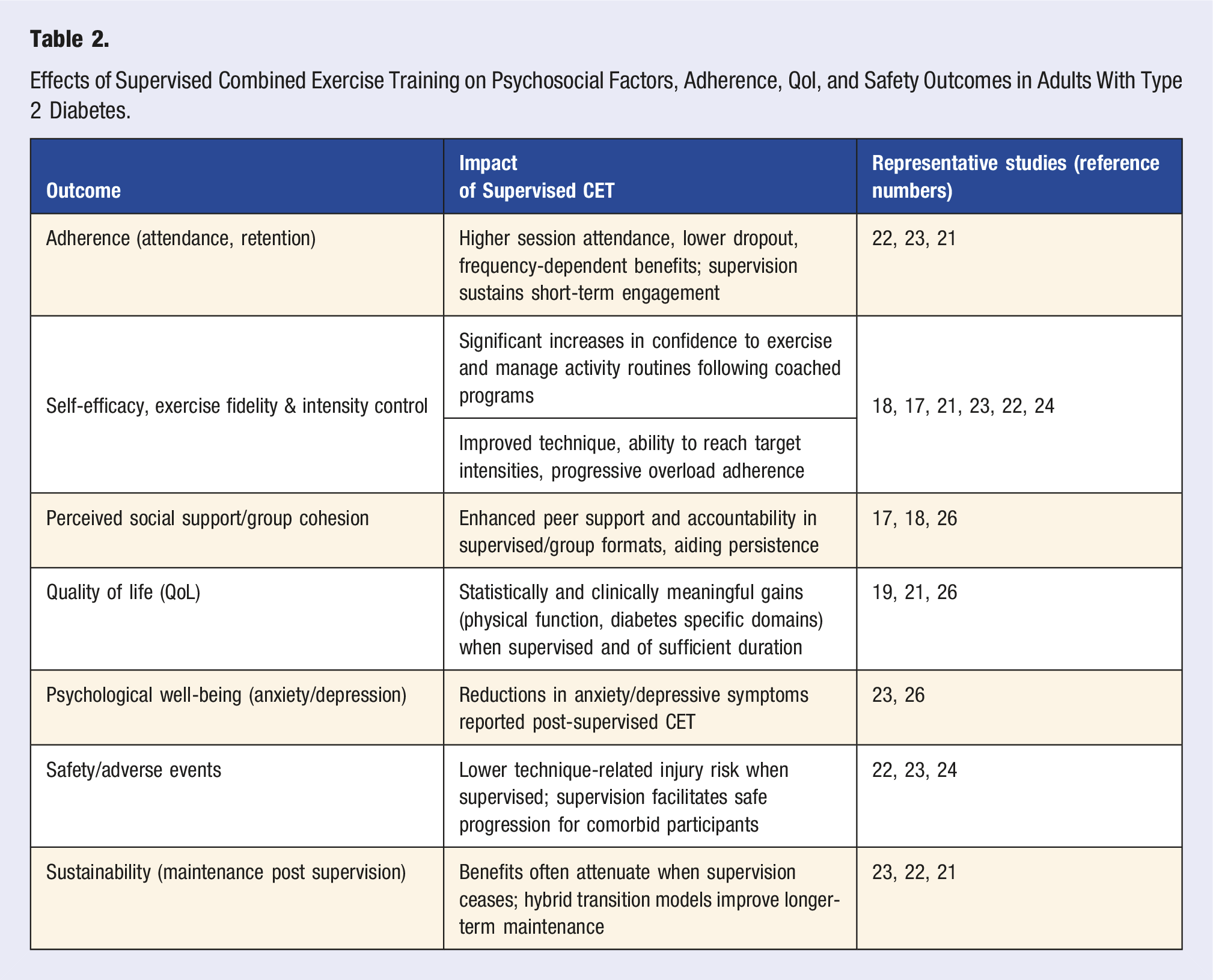
Supervised CET improves adherence and QoL in adults with T2DM across randomized trials and syntheses. Community-based supervised programs report superior engagement, retention, and greater cardiometabolic gains compared with less structured approaches. 22 Low-volume supervised HIIT + Resistance CET produced strong short-term adherence and clinically meaningful improvements in fitness and glycemic control during the coached phase, though benefits diminished at 12-month follow-up as supervision and adherence declined, underscoring the need for sustained support. 23 Supervision enhances psychosocial mediators of long-term adherence: structured, coached interventions increase self-efficacy and perceived social support, correlating with greater ongoing activity. 18 Qualitative analyses highlight that safe, supportive supervised settings foster competence and relatedness, transforming motivation and intrinsic engagement. 17 Group-based supervised formats further boost peer accountability and persistence.
Effects of Supervised Combined Exercise Training on Psychosocial Factors, Adherence, Qol, and Safety Outcomes in Adults With Type 2 Diabetes.
Conclusion
Supervised combined aerobic-plus-resistance training (CET) yields larger cardiometabolic benefits than unsupervised or usual-care programs. Randomized trials report greater reductions in HbA1c, fasting insulin/HOMA-IR, and blood pressure, as well as larger gains in VO2max and body composition with structured, supervised CET compared with routine or unsupervised exercise. Meta-analyses corroborate these findings, showing pooled improvements in glycemia, lipids, inflammatory markers, and BP for combined supervised training compared with comparators. Supervision consistently enhances adherence, exercise fidelity, and the magnitude and durability of metabolic gains. 13 – 27
Supervised CET also strengthens psychosocial mediators of long-term activity: supervised programs increase attendance, self-efficacy, perceived social support, and quality of life, which reinforce sustained exercise behavior and health gains. Key limitations include heterogeneity in CET composition, scheduling, supervision model, intensity, frequency, duration, and outcome/adherence metrics, limiting comparability and meta-analytic precision. Many trials are small, single-site, short-term, and underrepresent older adults, racial/ethnic minorities, and low-resource settings, and the reliance on self-report for psychosocial outcomes raises measurement concerns.
Clinical Implication
Clinicians, exercise professionals, and community program leaders should prioritize supervised or hybrid CET (∼30-60 min of moderate aerobic ≈ activity 3×/week plus resistance training 2-3×/week at moderate–high intensity with progressive overload and embedded behavioral supports (group sessions, coached feedback, scheduled accountability).
Research Priorities
Future research in adults with T2DM should aim to conduct head-to-head RCTs comparing scheduling and supervision, undertake larger pragmatic trials across diverse settings, and evaluate implementation and cost-effectiveness to inform policy and scale up supervised CET in diabetes care. For scalability, hybrid supervision models (community-led groups, telehealth coaching, structured tapering) can retain accountability and feedback while reducing resource needs; embedding behavior-change techniques (goal setting, feedback, self-monitoring) and community linkages during supervised phases support transition to self-management and sustain activity post-supervision.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.