
Abstract
Breast cancer (BC) survival has improved but is often offset by adverse effects, including reduced exercise capacity. Research in the general population suggests that social support may mitigate exercise capacity declines. However, this relationship in BC survivors has not been examined. This analysis sought to examine relationships between social support overall (and within social support subscales) and exercise capacity declines at 3 months in BC survivors during treatment in relation to cancer-free controls. In 230 BC (stage I-III) survivors and 128 cancer-free controls within the UPBEAT Study (NCT02791581), submaximal exercise capacity and social support were obtained via 6-Minute Walk Distance (6MWD) and MOS Social Support survey, respectively, at baseline and 3 months. Linear regression examined associations between social support and 6MWD declines in BC survivors and controls at 3 months. Declines in 6MWD were associated with social support (
“Women with BC had lower distance in their baseline 6MWD, lower fatigue score, and lower physical functioning score.”
Background
Against a backdrop of steady annual increase of breast cancer (BC) incidence in the last decade, mortality rates have continued to decrease. 1 The reduced mortality is largely due to the increased rates of screening and advancements in cancer treatment. 2 The increased survival, however, is offset by treatment-related morbidities. 3 Notably, BC survivors are at an elevated risk for developing heart failure, 4 for which a primary presenting symptom and predominant feature is reduced exercise capacity. 5 Declines in exercise capacity have been associated with reduced quality of life, impaired daily functioning, and an inability to return to work.6-8 Reduced exercise capacity is also associated with an elevated risk of cardiovascular disease mortality, 9 potentially due to declines in cardiac function. 10
Social support, too, has been associated with a myriad of health outcomes, ranging from quality of life to mortality. Social support is defined by the National Cancer Institute as a network of family, friends, neighbors, and community members who are available in times of need to provide psychological, physical, and/or financial assistance. 11 In women with BC, social support is most often composed of spouses, close relatives, and close friends. 12 A systematic review and meta-analysis showed that low social support negatively affected all-cause mortality in patients with coronary heart disease (risk ratio [RR] = 1.59; 95% confidence interval [CI]: 1.21-2.08). 13 With respect to breast cancer, research has shown that BC survivors who were more socially isolated had a 66% increased risk of all-cause mortality and a 2-fold increased risk of BC-specific mortality. 14 More recent evidence by Wang et al in postmenopausal women who were newly diagnosed with BC from the Women’s Health Initiative (N = 9154) showed that women with higher social support had significantly lower all-cause mortality (hazard ratio [HR] = 0.89; 95% CI: 0.81-0.90) when comparing the highest and lowest quartiles. 15 It is also postulated that low social support may induce chronic stress, which could affect prognosis and survival after BC diagnosis. Social support has been shown to be negatively correlated with depression and anxiety. 16 Conversely, social support may act as a protective factor for cognitive decline, 17 and may be positively associated with overall health related quality of life. 18
In addition, a positive correlation is seen between social support and physical activity, 19 which may be due to social support encouraging engagement in physical activity. This is supported by a systematic review of forty-four studies on barriers and facilitators of physical activity showing that higher levels of overall social support were associated with more leisure-time physical activity followed by travel-related physical activity. 20 Life satisfaction was also associated with higher social support (odds ratio [OR] = 3.27; 95% CI: 2.59-4.13) among older adults in a systematic review of 57 studies and meta-analysis of 78 studies. 21 Particular to BC survivors, a 2020 mixed-methods study demonstrated the multifactorial nature of the relationship between social support and physical activity when it noted BC survivors’ interest in connecting with other survivors to increase participation in physical activity and their willingness to involve professionals in social support. 22 Importantly, a 2019 randomized trial of BC survivors and their caregivers showed that social support was a modifiable factor. 23
Furthermore, physical activity has been shown in several studies to be associated with increased exercise capacity among cancer survivors. A systematic review and meta-analysis of randomized control trials (n = 15 studies) by Rodriguez-Canamero et al examining the impact of physical activity in advanced-stage cancer patients noted that interventions with aerobic training programs improved exercise capacity and physical function in patients undergoing active cancer treatment.24-28 It was also shown that insufficient physical activity in a study of women with stage I to III BC (n = 223) was associated with reductions in exercise capacity (P = 0.029) from baseline to 3 months. 10 Moreover, a study evaluating physical activity and survival following BC diagnosis (n = 9308 women, n = 1973 deaths) found that higher physical activity was associated with lower risk of all-cause mortality (HR = 0.69, 95% CI: 0.57-0.84). 29 Taken together, these studies suggest that an increase in social support in women with breast cancer could support increased participation in activities and therefore help them maintain their exercise capacity and potentially improve survival outcomes overall.
Objectives
The primary aims of this analysis were to examine how changes in social support (overall and in subscales) differed between BC survivors and controls, and to examine associations between social support and changes in submaximal exercise capacity over 3 months.
Methods and Variables
Study Population
The UPBEAT study is a longitudinal cohort of 244 women with stage I-III BC and 134 cancer-free controls (NCT02791581). Participants were recruited through academic and community-based medical centers affiliated through the NCI Community Oncology Research Program (NCORP) based at the Wake Forest NCORP Research Base. NCORP sites administered the study visits, including the 6-minute walk distance test (6MWD) and survey administration. The details of inclusion criteria for the UPBEAT study have been described elsewhere. 30 For this analytic cohort, women with missing data on the dependent variable, 6-minute walk distance test (6MWD) (n = 20) were excluded. Thus, the analytic cohort contained 230 BC survivors and 128 controls.
Data Measurement/Tools
Social support was measured using the Medical Outcomes Study (MOS) survey at baseline and 3 months. The MOS Social Support Survey was originally developed for patients with chronic conditions (e.g., hypertension, diabetes, coronary artery disease, depression) by Sherbourne and Stewart. 31 This survey is composed of 19 items that include 4 subscales: emotional support, tangible support, affectionate support, and positive social interactions (See Supplemental Material 1). These four subscales of social support were found to produce high reliability and have continued to be used in many chronic conditions since its inception. 32 In Sherbourne and Stewart’s multitrait scaling analyses, they reported that the scales are not only reliable (all alphas greater than 0.91) among the 4 different dimensions, but fairly stable over time. 31 Emotional support refers to love and empathy that is gained from the relationship. Tangible support is the support that is provided through material means such as finances or meal preparation. Positive social interactions refer to the time spent doing fun things. Meanwhile, affectionate support refers to the active display of love and care. 31 Items in the social support survey that cover the four subscales include “someone you can count on to listen to you when you need to talk (emotional support), “someone to take you to the doctor if you need it” (tangible support), “someone who shows you affection” (affectionate support), and “someone to have a good time with” (positive social interaction). The survey is graded on a 5-point scale ranging from “none of the time” to “all the time,” with higher scores indicating higher levels of support. The survey was devised to be easy, short, and readily administered to participants. The subscales can be used individually to better understand the specific component of social support that are associated with respective outcomes, 31 as was done in this analysis.
Submaximal exercise capacity was measured using the 6MWD. While there is not a standard normative value for the test, it may be used in comparison to healthy controls before and after interventions. 33 This test was used to measure submaximal cardiorespiratory fitness, which can be used to approximate the functional impacts of reduced exercise capacity on activities of daily living; it is an independent predictor of survival, and is highly reproducible when implemented with standardized protocols. 34 The 6-minute walk test used to create the 6MWD in this analysis was administered by trained staff at the NCORP sites according to established guidelines. 33 Participants were asked to cover as much distance as they could on an open track or open corridor within 6 minutes. 10 The 6MWD is considered submaximal exercise because it is self-paced, whereby the participant chooses their own intensity and rest during the test. Because the 6MWD is self-paced, participants are not explicitly instructed to go at maximal capacity as opposed to the instructions provided for a cardiopulmonary exercise test. 35 The 6MWD is easy to perform, is low cost, 36 and has been used to measure the response to interventions in different patient populations.37,38
Fatigue was ascertained through the Functional Assessment of Cancer Therapy-Fatigue (FACT-F) scale which assess the impact of fatigue on an individual’s daily activities. For this analysis, baseline fatigue was evaluated as a potential confounder. This is a 41-item scale where items are rated using a 5-point intensity scale that covers the domains of fatigue, physical, social/family, functional, and emotional well-being. The fatigue specific domain of the FACT-F contains 13 items whereby higher scores indicate greater fatigue levels. The questionnaire has been used to assess fatigue and anemia-related concerns among people with cancer. The fatigue subscale has reported strong internal consistency (coefficient alpha range = 0.93-0.95). 39
Physical functioning was measured through the Short Form Health Survey (SF-36). For this analysis, baseline physical functioning was evaluated as a potential confounder. The SF-36 scale encompasses 8 domains of physical functioning (10 items), physical role limitations (4 items), pain (2 items), health perceptions (5 items), vitality (4 items), social functioning (2 items), emotional role limitations (3 items), and mental health (5 items). 40 The score of these 8 domains and their weighted sums range from 0 to 100, with lower scores indicating greater disability and higher scores indicating lower disability. A systematic review by Treanor and Donelly found that the Cronbach’s alpha value of internal consistency were consistently greater than 0.7 in assessing health related outcomes particularly among BC survivors. 41
Physical activity was assessed through the Godin-Shephard Leisure-Time Physical Activity Questionnaire. Specifically, it asks “how many times on average do you do the following kinds of exercise more than 15 min during your free time?” This survey inquires participant’s physical activity that is stratified by strenuous (e.g., running, jogging, football), moderate (e.g., fast walking, baseball, bicycling), and light/mild exercise (e.g., yoga, archery, fishing, bowling) which are then multiplied by 9, 5, and 3, respectively. The 3 latter values correspond to metabolic equivalent of tasks (MET), which are a way to objectively quantify the intensity of physical activity. Self-reported leisure time using the Godin-Shephard Leisure-Time Questionnaire is common in oncology research to classify and summarize physical activity.10,42
Statistical Analysis
For descriptive statistics, continuous variables are presented as means ± standard deviations (SD); categorical variables are presented as counts and percentages. Bivariate statistics were used to evaluate group differences in social support variables using t-tests.
This study investigated the main effects of the relationship between self-reported overall social support (baseline and 3 months) as well as each of the social support subscales (baseline and 3 months) and submaximal exercise capacity (baseline and 3 months) in BC survivors by using a linear regression model. Potential confounding factors were examined, including age, baseline 6MWD, race, body mass index (BMI), cigarette smoking, diabetes, hypertension, heart failure, breast cancer status, fatigue (FACT-F), physical activity (Godin-Shephard Leisure-Time Physical Activity Questionnaire), physical functioning (SF-36), depression (CESD), pain (SF-36), and receipt of anthracycline chemotherapy. The final model selected was the most parsimonious model. To do so, we required that variables investigated for confounding factors met the criteria for confounding (i.e., they were associated with both the exposure (social support) and outcome (6MWD)). Only those which met the requirement for confounding and which changed the Beta coefficient by 10% (for social support) or more were retained in the model investigating social support. This same set of variables was included across all models for consistency. Ultimately, the model contained the confounders of
Results
Baseline Characteristics of Study Participants in the Analytic Cohort.
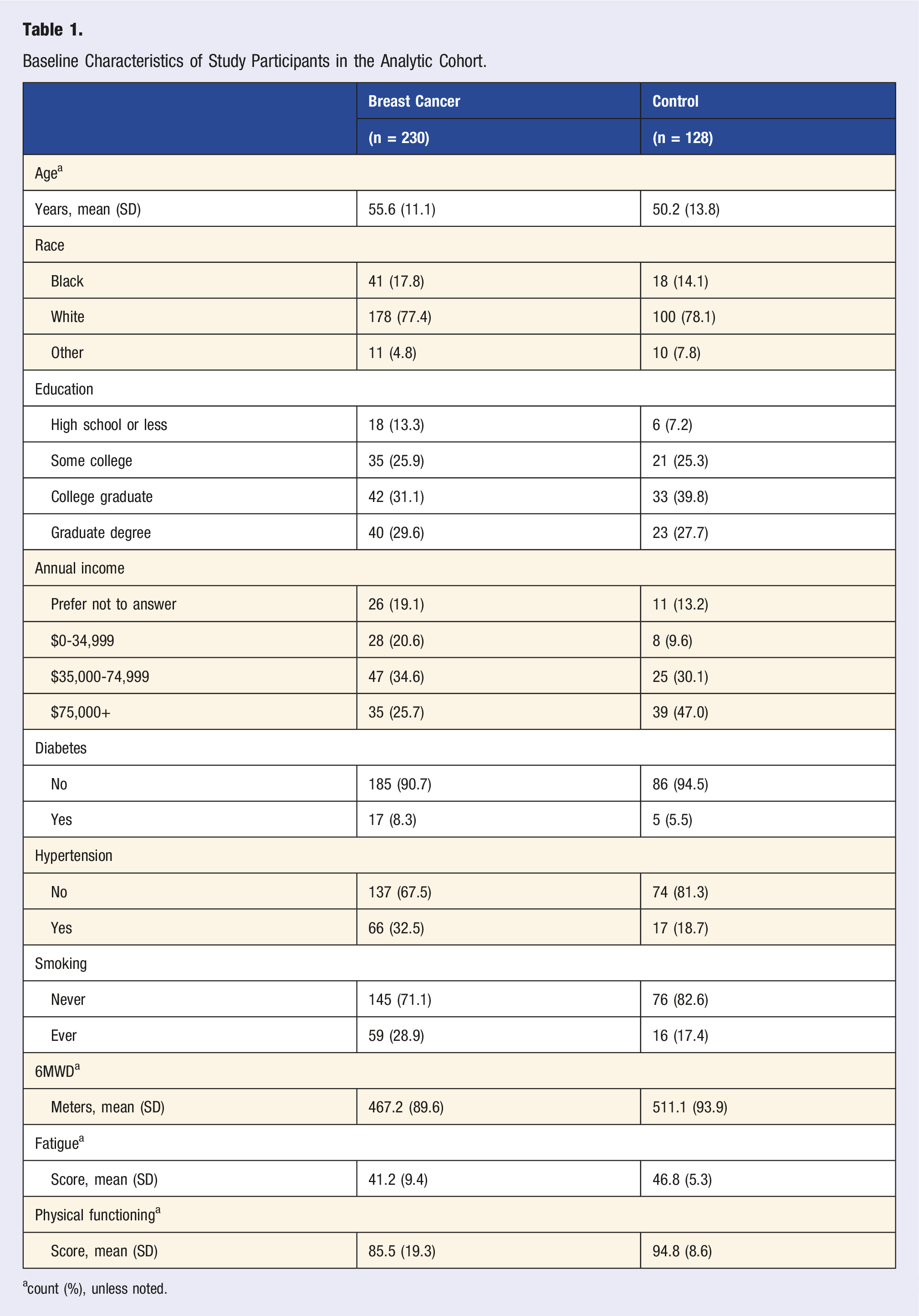
acount (%), unless noted.
Group Differences Between the Change in Social Support in Breast Cancer Cases and Control Women.
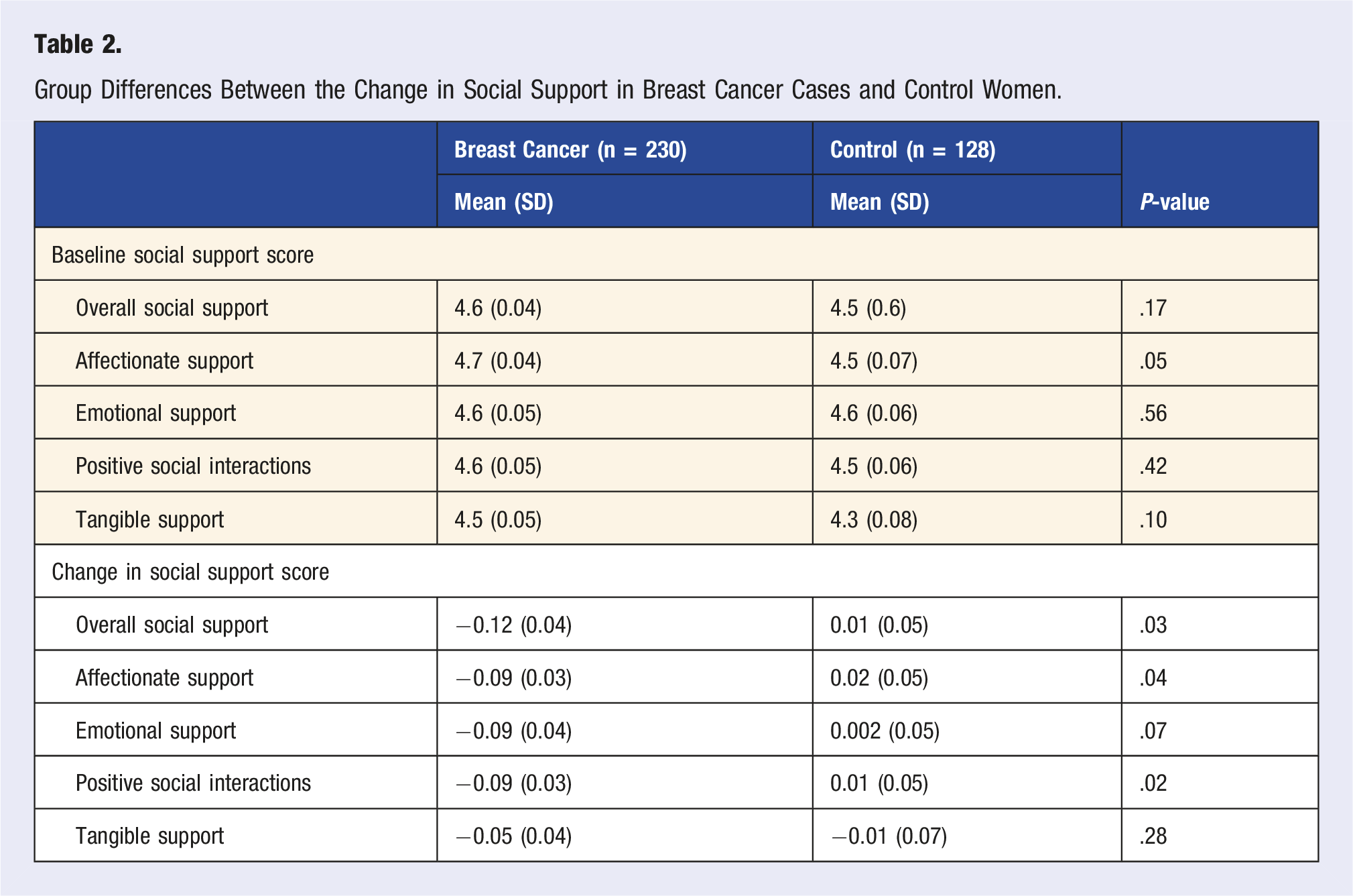
In bivariate analysis, we investigated the differences between BC survivors and controls in their changes in social support at 3 months (Table 2). There were statistically significant differences between BC survivors and controls in the change in overall social support (P = .03), in affectionate support (P = .04), and in positive social interactions (P = .02) from baseline to 3 months, whereas almost no difference was detected in controls in that timeframe. There were no statistically significant differences in the changes in subscales of emotional support (P = .07) or tangible support (P = .28) for BC survivors versus controls. Figure 1 shows the change in social support between baseline and 3 months (during treatment) in BC survivors and control women, with Figure 2 further exemplifying the association of positive social interaction with 6MWD. Change in self-reported social support at 2 timepoints in BC survivors and control women. *Indicates a statistically significant difference in change from baseline to 3 months in BC survivors versus cancer-free controls. Change in positive social interactions and 6MWD at 3 months.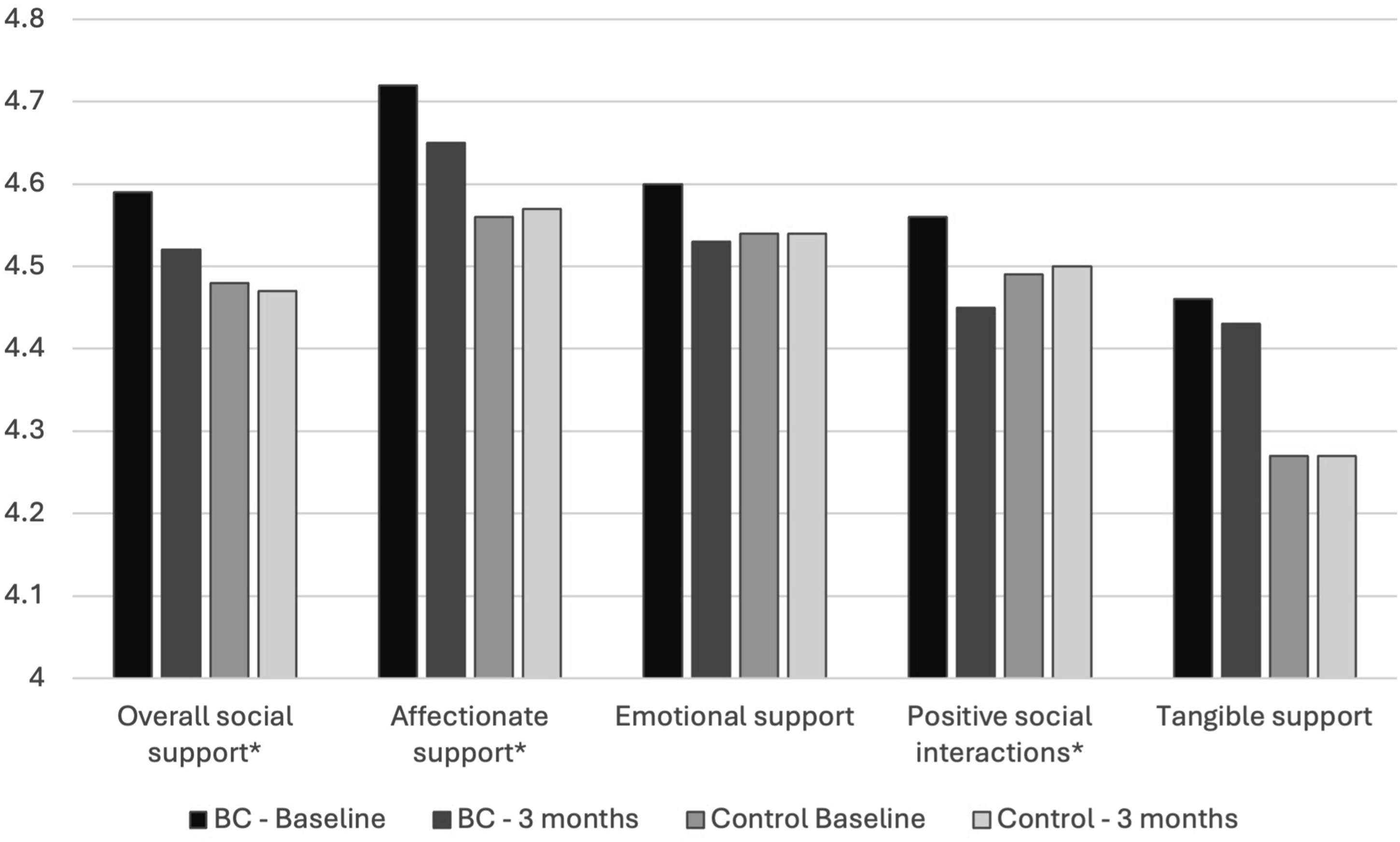
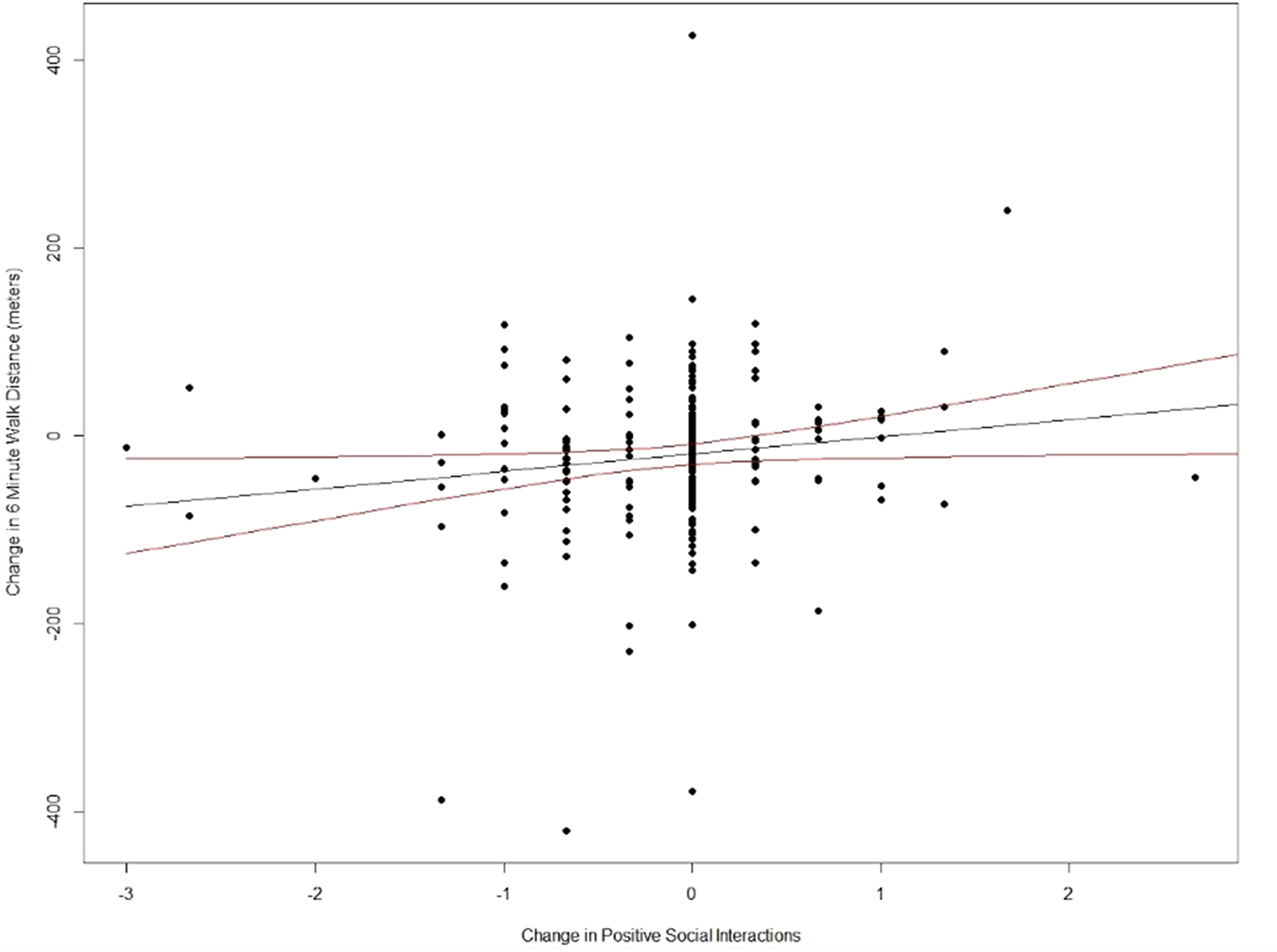
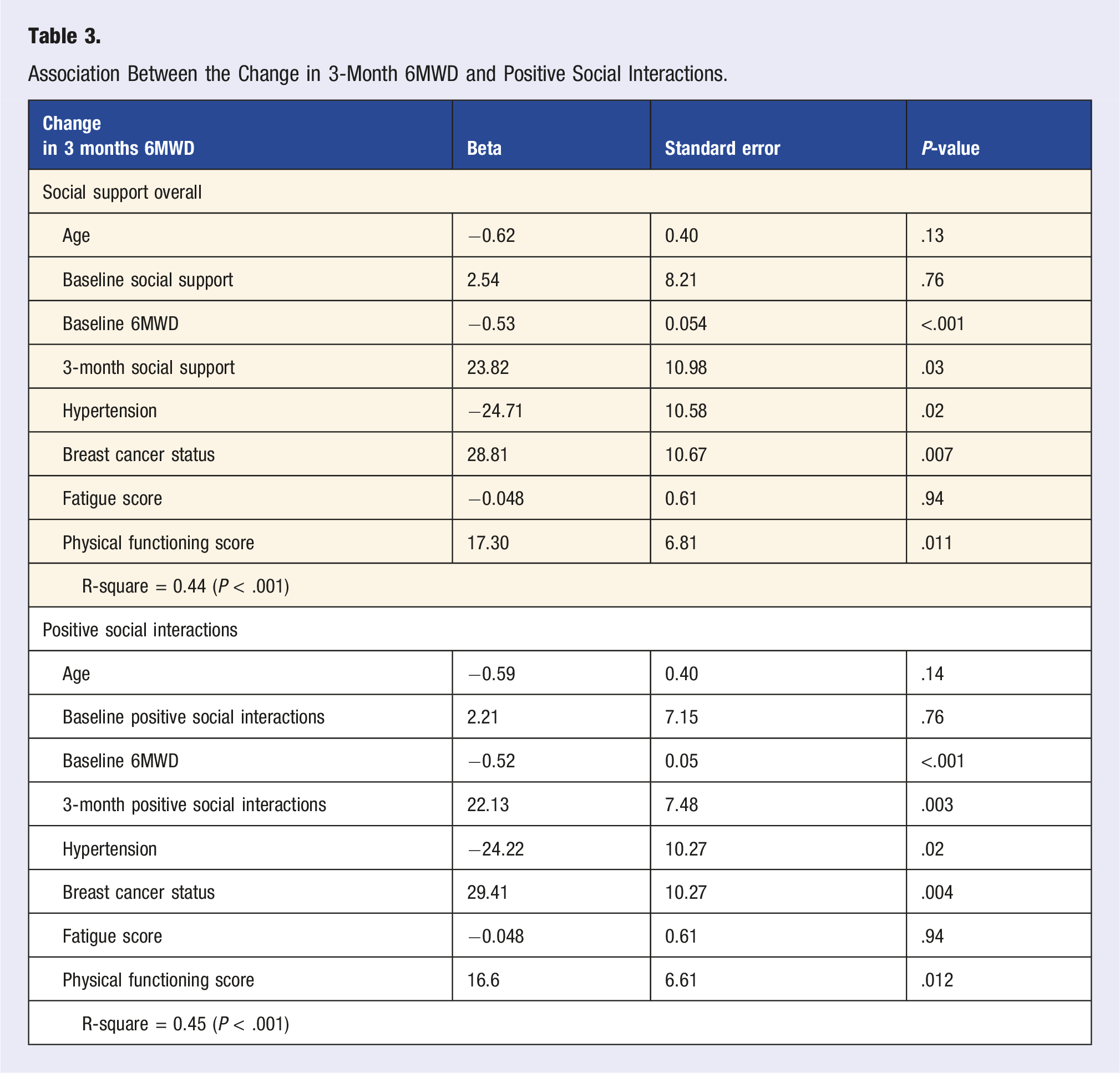
Association Between the Change in 3-Month 6MWD and Positive Social Interactions.
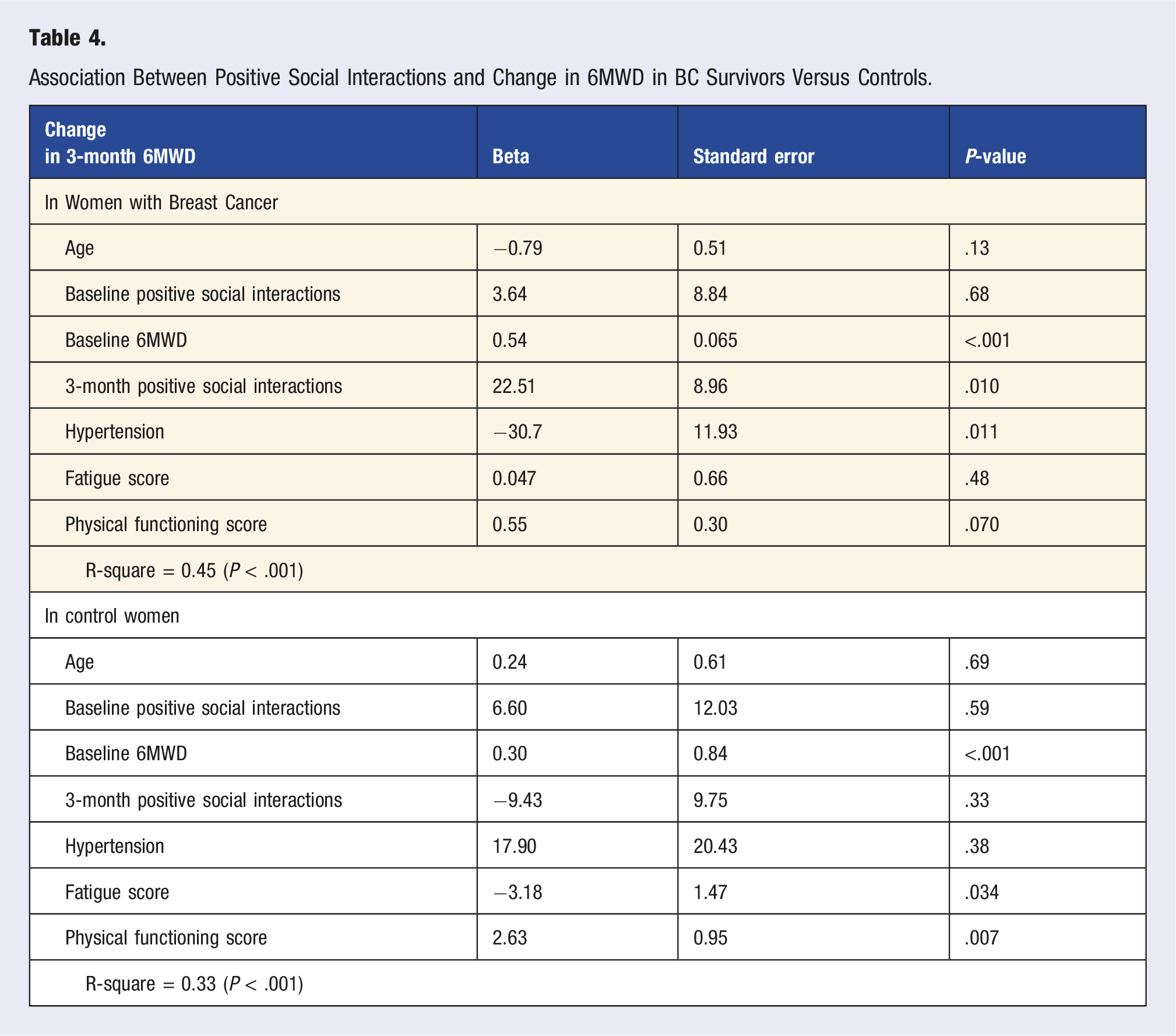
Association Between Positive Social Interactions and Change in 6MWD in BC Survivors Versus Controls.
We did not detect evidence to suggest that the relationship between positive social interaction and 6MWD was mediated by physical activity.
Discussion
To our knowledge, this is the first study to document an association between social support experienced during BC treatment and reduced exercise capacity at 3 months in women treated for BC. This association was predominantly driven by the social support subscale, positive social interaction, a concept that encompasses whether the respondent has someone with whom to do enjoyable activities. The physical, 10 and psychological effects, as well as increased risk of mortality associated with 14 low social support in women undergoing BC treatment has been well documented. 16 However, there is a lack of literature connecting social support to exercise capacity in BC survivors. Though our findings would require testing through a gold-standard randomized control trial which intervenes to increase social support, this observational data suggest the importance of attending to women’s needs for social support with a particular emphasis on positive social interactions during BC treatment.
In the current study, we found that women treated for breast cancer compared to cancer-free controls were more likely to experience a significant decline in overall social support (P = .03), decline in affectionate support (P = .04), and decline in positive social interactions (P = .02) during their cancer treatment. Interestingly, we did not find a significant drop in tangible support, suggesting that this component of social support may persist at similar levels during treatment as to the time of diagnosis. This is conceivable as many women may continue to receive support from family and friends while handling the many logistics required for receipt of cancer treatment. The relationship between social support and improved survival in breast cancer has been discussed in the literature. In addition, associations specifically between positive social interactions and quality of life have been described. Most notably, Kroenke et al’s study found that positive social interactions mediated the relationship between social networks and quality of life. 43 The authors put forth that positive social interactions might allow women with BC the opportunity to distract themselves from the distress of cancer.
Given that submaximal exercise capacity is associated with reduced quality of life and increased cardiovascular disease mortality, it is important to understand factors associated with its reduction during treatment in BC survivors.9,10,44 Here, we found that low social support was associated with reduced 6MWD, after adjustment for confounders. Of note, some of the subscales (i.e., tangible support) did not substantially change over the time of the study, which may account for the lack of association between these subscales at 3 months and 6MWD declines. Of the 4 subscales, we observed that low positive social interactions at 3 months were most strongly associated with reduced 6MWD. We found that the relationship between positive social support and reduced 6 MWD was observed only in BC survivors, likely due to positive social interactions remaining at high levels in control women while decreasing in BC survivors (as shown in Figure 1). Replication in larger cohorts is needed before drawing definitive conclusions about differential effects by cancer status. The decrease observed in positive social interactions during cancer treatment (Table 2) and the strength of the association matching that of overall social support (Table 3) is thus interpreted as low positive social interactions during treatment being most responsible for the association between low social support and 6MWD declines.
The mechanisms by which social support may influence exercise capacity are not clear, though we hypothesized physical activity may mediate this relationship. Existing literature has suggested that social support may be a facilitator in increasing engagement in physical activity. 20 However, when we investigated physical activity as a mediator, our results did not show that physical activity declines experienced during BC treatment explained the relationship between low social support and 6MWD declines; however, our analysis had limited ability to detect mediation by physical activity due to its limited timepoints of data collection. To our knowledge, there is no cancer-related literature on the relationship between social support and exercise capacity. One related study on obese older adults with cognitive impairment found that a social support-based physical activity program resulted in greater submaximal exercise capacity and physical activity participation. 45 Of the literature to examine social support and exercise capacity in cancer survivors, the main focus has been physical activity as an intervention. 22 Future research, such as studies with multiple data collection timepoints is needed to better understand the relationship between social support and exercise capacity with a focus on which factors may serve as mediators.
Multiple studies have investigated factors associated with the various social support constructs among BC survivors, which includes social isolation and positive social interactions.14,43 Research has shown that BC survivors reporting social isolation were more likely to be current smokers, have low physical activity, high alcohol intake, and be obese. 46 The literature suggests that positive social interactions, in particular, was associated with a reduction in pain, nausea, bed rest, and increased energy in BC survivors. 43 We examined how confounders might be involved in the relationship between the various constructs surrounding social support (e.g., affectionate support, emotional support, positive social interaction, and tangible support) and exercise capacity (namely, smoking, obesity, fatigue, and pain). We found that fatigue but not pain, smoking, nor obesity was a confounding factor. In brief, controlling for fatigue attenuated the association between positive social interactions and exercise capacity declines, potentially due to elevated fatigue during BC treatment.
Research around social support has also focused on the logistical support and physiological reactions to the disease in women with breast cancer. 47 In Barth et al’s systematic review, low functional support (e.g., getting tasks done, financial support, helping evaluate a situation) was associated with a higher all-cause mortality (n = 9 studies) with a pooled risk ratio of 1.71 (95% CI: 1.26-2.31). 13 A prospective study conducted by Kroenke et al found that women with less social support experienced greater mortality than those who had close relatives, friends, or living children, which may have been partially explained by their facilitation of access to care. 14 In our dataset, we were unable to examine the role of access to care because all women had access to treatment (by definition of the inclusion criteria in our study designed to examine the role of potentially cardiotoxic treatments). Lack of social support can cause physical stress, increasing inflammation and the immune response which has been measured through biomarkers in past studies. 48 One longitudinal study (N = 647) found that perceived social support was linked to changes in C-reactive protein, interleukin-6, and fibrinogen which are markers of distress and inflammation most often caused by an immune response. 49 This demonstrates the potential buffering effects that social support can exert in response to therapies and overall stress in BC patients.
It is important to note that increasing social support is possible through intervention. Though to our knowledge, no study has examined an intervention to increase positive social interactions specifically among BC survivors. Evidence shows that having someone to listen when needing to talk is associated with a higher quality of life. 48 One social support intervention in particular was shown in chronically ill patients to facilitate improvements in psychological distress as well as increased self-care. 50 Specific to BC survivors, a randomized control trial conducted in 2019 exemplified how interpersonal support and marital communication were able to reduce BC survivor’s anxiety, and depressed mood, as well as increase her self-efficacy. 23 These may be similar constructs to affectionate support and emotional support measured in the MOS. Although we did not detect associations between these variables and reduced 6MWD, we did observe these to significantly decline during cancer treatment. By identifying modifiable factors in women receiving BC treatment, clinicians are able to provide care that addresses the whole person. As such, clinicians may be able to mitigate the loss of exercise capacity during cancer treatment, as we consider the multidimensional characteristics of social support, such as positive social interactions during BC treatment and exercise capacity.51,52
Strengths of our study include the 2 timepoints at which 6MWD and social support were measured, including a timepoint during treatment in BC survivors in which to examine changes in 6MWD, and the inclusion of a cancer-free control group, with whom comparisons of changes in social support and submaximal exercise capacity can be made. Limitations of our dataset include a limited ability to examine mediation by factors, such as physical activity, because we only had 2 timepoints of data collection in this timeframe. In addition, there was a lack of variability on access to care women such that we were unable to evaluate whether these results differed in those with limited access to care. It is also unclear whether these results would be generalizable to people diagnosed with cancer at different sites, such as ovarian or lung cancer.
Conclusion
The results of this study show that reduced social support during BC treatment is associated with reduced exercise capacity. While this requires replication in other studies, our findings suggest this as one potential pathway through which social support may influence mortality, as lower exercise capacity is associated with an elevated risk of cardiovascular disease mortality.9,10,14 The literature showing that BC survivors are receptive to the involvement of professional guidance in their social support indicates the potential for clinicians to provide encouragement of BC survivors to increase positive social interactions during treatment. Though interventions exist to increase the affectionate support and emotional support of caregivers to BC survivors, research is still needed to identify interventions effective at increasing positive social interactions for BC survivors. Overall, this line of research is warranted as evidence in the literature has consistently shown that social support is linked to a breast cancer survivor’s well-being and quality of life.
Supplemental Material
Supplemental Material - Declines in Social Support During Breast Cancer Treatment and Their Association With Exercise Capacity Reductions in Breast Cancer Survivors
Supplemental Material for Declines in Social Support During Breast Cancer Treatment and Their Association With Exercise Capacity Reductions in Breast Cancer Survivors by Johnny Nguyen, Kerryn W. Reding, Ralph D’Agostino Jr, Nathaniel S. O’Connell, Amy Ladd, Warren Szewczyk, Alexander R. Lucas, Giselle C. Meléndez, Shannon Mihalko, Lynne E. Wagner, Bonnie Ky, Kathryn E. Weaver, Glenn J. Lesser, W in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We wish to thank the participants of the UPBEAT trial for their involvement in this study and the research staff at the Wake Forest NCORP Research Base.
Ethical Considerations
This study adhered to the highest ethical principles in the conduct of the study. It received Institutional Review Board approval through the Wake Forest NCI Community Oncology Research Program (NCORP) Research Base.
Consent to Participate
Each participant involved in this study completed an informed consent process in order to enroll in this research study. The consent process was reviewed and approved by the Institutional Review Board.
Author Contributions
WGH, RDJ, GJL, KEW, LEW, SM, KWR: Conceptualization; RDJ, KWR, WGH, JN, WS: Methodology; JN, KWR: Writing—original draft; KWR, RDJ, WGH: Supervision; RDJ, NSO, KWR: Formal analysis; WGH, LEF, KEW, RDJ, GJL, BK, SM: Resources; JN, KWR, RDJ, AL, WS, ARL, GCM, SM, LEW, BK, KEW, GJW, WGH: Writing—reviewing and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIH grants: 2UG1CA189824 and 1R01CA199167-01.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available in accordance with policies developed by the UPBEAT Study P&P to protect sensitive participant information and approved by the Wake Forest NCORP Research Base.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.