
Abstract
“Post-pandemic prevalence of anxiety, depression, and trauma remains elevated in the general population; even clients who seek coaching for lifestyle goals may carry significant mental health burdens in parallel.
Introduction
Health coaching, a profession distinct from traditional mental health roles, has substantial emerging evidence supporting its efficacy for enhancing mental wellbeing.1,2 Clients may reveal symptoms of depression, anxiety, trauma, or other psychological disorders during a coaching session. Coaching helps patients with mental health disorders improve their lifestyle behaviors, which may mitigate the severity of their condition or reduce risky behaviors, even in serious mental illness.3,4 Despite their potential contributions in this area, health coaches currently lack standardized referral protocols, creating practice variation and vulnerabilities for coaches, clients, and primary care providers.
National Board-Certified Health and Wellness Coaches (NBC-HWCs) are credentialed behavior change specialists trained to the profession’s highest standard. NBC-HWCs support self-directed lasting changes that align with client values. 5 Throughout this paper, “health coach/coach” refers to NBC-HWCs and client and patient are used interchangeably congruent with norms in a variety of settings.
Health coaches operate under a defined scope of practice that facilitates client-centered lifestyle behavior and mindset change.6,7 Health coaches may help individuals implement lifestyle medicine recommendations to improve mental health. 8 Clients often experience coaching as therapeutic.9,10 Unlike mental health providers, health coaches do not diagnose or provide psychotherapy or treatment. Coaches serve as collaborative members of the healthcare team, supporting clients in forward-focused growth. The National Board for Health & Wellness Coaching (NBHWC) Code of Ethics requires referral to licensed professionals when client welfare warrants; failure to refer is an ethical breach. 11
The NBHWC Scope of Practice explicitly prohibits health coaches from providing “psychological therapeutic interventions” or any treatment for diagnosed mental health conditions. 6 The NBHWC developed competencies include psychological safety, boundaries, appropriate referrals, and basic mental health symptom understanding 12 (Appendix A). However, research suggests ongoing ambiguity around coach-therapy boundaries, referrals, and coach desire for additional mental health training.4,13
Primary care providers (PCPs) are well-served to partner with health coaches to meet their patient’s lifestyle needs. Providers lack time; a 15-minute appointment cannot meet all the needs a patient brings to the encounter. When coaches are added to primary care teams, patient trust in their PCP increases as does the proportion of patients who would recommend their provider. 14
PCPs managing patients with chronic conditions like diabetes, hypertension, or cardiovascular disease often encounter comorbidities such as anxiety and depression. Depression alone accounts for approximately 10% of primary care visits, 15 yet fewer than half of patients with a mental health disorder are recognized in primary care, and only 12.5% of those are properly treated. 16 Health coaches embedded in primary care teams may find themselves on the front lines of unmet mental health needs.
This paper synthesizes best practices for mental health symptom recognition, referrals, and safety measures. It offers practical recommendations for maintaining clear boundaries while providing ethical service to clients. By strengthening these skills, coaches uphold professional integrity and ethical obligations. By delineating coaches from licensed mental health professionals, coaches protect themselves from legal and ethical breaches. The guidelines presented here are designed to support the integration of coaches in primary care and specialty clinics, while also supporting coaches in private and community-based practice.
Practice Implications
Mental health referral competence is essential to client safety. When clients disclose distress during coaching sessions, coaches must distinguish transient emotional dysregulation from symptoms warranting clinical attention. Prompt action must be taken for the later.
Timely referral for mental health conditions can shorten the duration of suffering by facilitating appropriate treatment before symptoms worsen.17,18 Effective referrals may also enhance the coach-client relationship based on literature from other helping professions. 19 Coaches without training in making referrals may avoid discussing obvious signs of distress, inadvertently invalidating the client’s experience. By contrast, a coach who addresses the issue openly and facilitates support demonstrates true client-centered care. Referring a client to mental health resources can strengthen trust and rapport. Research suggests that referrals normalize mental health care as part of one’s wellbeing journey, reducing stigma, and framing therapy as another resource for growth. 20
Referral practices contribute to the broader vision of integrated whole-person care in lifestyle medicine. Coaches are increasingly working alongside teams of interprofessional health and mental health care providers in collaborative care models. Clear referral processes position coaches as integral team members that improve client outcomes and prioritize safety and wellbeing.
The guiding principles proposed in this paper are rooted in evidence and contextualized within the NBHWC Code of Ethics and Professional Conduct and NBC-HWC Scope of Practice.3,4,6,10,11 These principles are proposed for consideration by the field as the role of NBC-HWCs continues to evolve. Ongoing integration of evidence, experience, and input from interprofessional teams is necessary to continue to shape guidance for NBC-HWCs working at the intersections of lifestyle medicine, primary care, and mental health. The detailed application of these principles with sample language for use in practice appears in Appendix B.
Mental Health Safety & Referral Principles
(1) Remain within the ethical boundaries of the health coaches’ role and scope of practice. (2) Employ health coaching techniques to work through the referral process in non-urgent scenarios. (3) Recognize when a situation requires urgent or emergency action, respond ethically, and collaborate with appropriate professionals. (4) Attend to the needs, boundaries, and wellbeing of the health coach in addition to the needs of the client.
Implementation/Methods
Recognition, Symptom Identification Tools, and Referral
The foundational competency for health coaches is the recognition of symptoms and patterns that signal distress beyond what is experienced with normal life challenges, coupled with the ability to execute timely and appropriate referrals. This recognition and referral skill set (Figure 1) represents the essence of the health coach’s role and scope in mental health support, distinguishing it from the clinical assessment and diagnosis performed by licensed mental health professionals. Exactly how the coach employs recognition and referral in clinical settings is evolving alongside growing complexity of client needs and the integration of coaches into settings with complex individuals. This section also discusses symptom identification tools, which are not yet a standard of care in coaching practice. Recognition and referral process for mental health symptoms.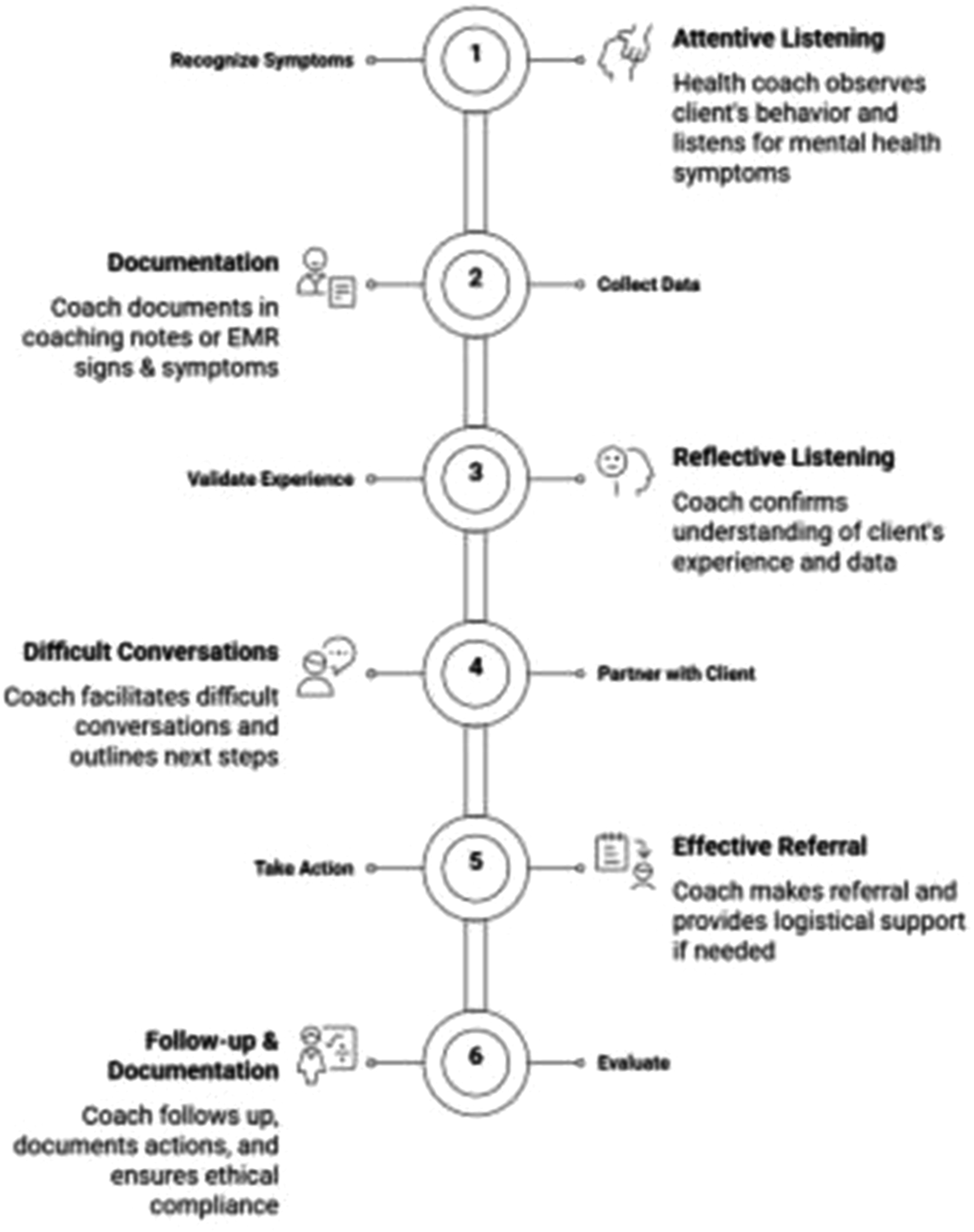
Recognition
Health coaches have a professional responsibility to develop competence in recognizing behavioral, emotional, and cognitive signs that may signal mental health concerns. This includes identifying warning signs of imminent danger or medical urgency and knowing when and how to connect clients with appropriate resources and professionals. Recognition must occur at two levels: at intake, when initial symptom presentation may warrant immediate attention, and longitudinally, as coaches observe changes or emerging patterns across the coaching relationship. Coaches must be grounded in foundational knowledge of mental health symptomatology, remain attuned to shifts that develop or intensify over time, and be familiar with validated symptom identification tools that can support clinical decision making.
Symptom Identification Tools
While symptom identification is a combination of relational observation and client report, standardized screening tools represent another resource for symptom identification. Some health coaches report discomfort with screening instruments, perceiving them as too closely aligned with clinical diagnosis and preferring to defer such activities to licensed providers.13,21 This divergence reflects variability in experience, role, setting, and comfort level.
Tools that rely on self-report rather than professional assessment can help quantify symptom severity and provide objective data to support referral decisions. Appendix C outlines validated tools appropriate for common mental health conditions. How and when these tools are used will vary by setting: coaches working within interprofessional health systems should follow institutional workflows and policies, while coaches in independent or community-based practice may direct clients to reputable nonprofit resources offering free, scientifically validated screening tools available in both English and Spanish. 22 In some settings, it may be most appropriate for clients to complete these tools outside of the session. Clients should have input into how these data points are used in coaching, though responses indicating acute risk, such as suicidality, obligate the coach to refer. Regardless of setting, the decision of whether, when, and which tool to use should be individualized, accounting for client need, coach experience, and practice context.
Referral
Upon recognition of significant, persistent, or urgent mental health symptoms, the health coach must possess the knowledge and the preparedness to execute an appropriate referral. This process requires preparation; health coaches should maintain, or be provided by an employer, a comprehensive, pre-compiled referral network that includes: • Non-urgent community-based mental health resources • Licensed mental health professionals (psychotherapy & psychiatry providers) • Peer support networks and support groups • Substance use treatment • Walk-in or urgent care mental health services (if available) • Crisis intervention resources (suicide hotlines) • Emergency Care
Coaches working with specialized client populations should familiarize themselves with resources specific to those populations. Referral strategies include utilizing national search engines, regional mental health resources, local health systems, low-cost/sliding-scale options, and insurance directories. The referral process requires skillful navigation and firm scope-of-practice boundaries. Health coaches must balance honesty about their concerns with respect for client autonomy. Cultural humility is paramount as coaches must connect clients with resources that honor the client’s identity, language needs, and personal context.
When a referral is offered, clients may resist, disagree, decline, or face structural barriers to accessing care. These scenarios can present ethical complexity and require adherence to guiding principles that prioritize safety. Documentation of these conversations and outcomes is an essential best practice (see Appendix D).
Building Competency Through Training and Supervision
Training
Mental health training designed specifically for health coaches includes symptom identification, simulation of difficult referral conversations, and guidance for ethical decision-making. NBHWC-accredited programs represent the highest standard in health coach training, though competencies will need to evolve alongside the profession. In the interim, continuing education and interprofessional collaboration may fill gaps in education and experience.
Supervision
Health coaches must recognize the limits of their own expertise. Competence means knowing when to seek consultation from a licensed mental health professional or a supervisor. Experience and professional judgment are best shaped by interprofessional practice and formal supervision. The NBHWC and the International Coaching Federation (ICF) reference a supervision/mentoring process for their continuing education options.23,24 The UK & International Health Coaching Association (UKIHCA) requires 4 sessions of health coaching supervision annually. 25 In accordance with other helping professions, such as licensed mental health professions, the NBHWC should consider adopting a formal supervision process as a best practice recommendation. Utilizing interprofessional support systems protects clients and models help-seeking behavior. By maintaining appropriate boundaries, pursuing ongoing education, and leveraging supervision and consultation when needed, health coaches fulfill their role as facilitators of wellbeing who know when, and how, to connect clients with higher levels of care.
Discussion
The process outlined in this paper fills an important gap in the expanding field of health and wellness coaching. Notably, the recommendations align closely with existing guidelines from related domains. The ICF and NBHWC advise health coaches to refer clients to appropriate professionals when psychological issues exceed the coaching scope of practice.12,26 The guidelines discussed in this paper operationalize this guidance with concrete action steps for health coaches collaborating with healthcare professionals. The need extends beyond integrated settings: 41.4% of health coaches report working in private practice, often without direct access to clinical colleagues. 27 This is particularly timely as health coaches face increasing complexity in client cases. Post-pandemic prevalence of anxiety, depression, and trauma remains elevated in the general population; even clients who seek coaching for lifestyle goals may carry significant mental health burdens in parallel. 28 The threshold for referral should remain conservative: when in doubt, refer. Professional bodies such as the NBHWC should consider incorporating stronger accreditation standards related to mental health, building on existing competencies with the detailed recommendations provided in this paper.
Conclusion
Health Coaches must be prepared to navigate the intersection of wellbeing and mental health in a manner that is ethical, safe, and client-centered. This paper presents a structured approach to mental health symptom recognition, referral, and crisis management tailored to the health coaching context. By following the guidelines and their detailed application, health coaches demonstrate the core health coaching values of respecting the client as the expert on their life and expertise in their own health and wellbeing.
Supplemental Material
Suppplemental Material - Mental Health Referrals in Health Coaching: Guidelines for Safe, Ethical Practice
Suppplemental Material for Mental Health Referrals in Health Coaching: Guidelines for Safe, Ethical Practice in Megan E. Voss, Cherie O’Neill, Cynthia Austin, Mary Jo Kreitzer in Practice Brief
Footnotes
Acknowledgments
The authors thank the participating health coaches and licensed mental health professionals for sharing their time and expertise. In addition, to all future professionals in both these groups who chose to collaborate to enhance patient care recognizing the power of these two professions coming together.
Consent for Publication
Submissions containing any data from an individual person (including individual details, images or videos) must include a statement confirming that informed consent for publication was provided by the participant(s) or a legally authorized representative. Non-essential identifying details should be omitted. Please do not submit the participant’s actual written informed consent with your article, as this in itself breaches the patient’s confidentiality. The Journal requests that you confirm to us, in writing, that you have obtained written informed consent to publish but the written consent itself should be held by the authors/investigators themselves, for example in a patient’s hospital record. The confirmatory letter may be uploaded with your submission as a separate file in addition to the statement confirming that consent to publish was obtained within the manuscript text. If this is not applicable to your manuscript, please state “Not applicable” in this section.
Author Contributions
MEV: Conceptualization, Writing-Reviewing, and Editing. CO: Writing-Original Draft, Reviewing, and Editing, Formatting. CA: Conceptulatization, Writing-Reviewing and Editing. MJK: Writing-Reviewing and Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.