
Abstract
In Y-stenting, stabilization of the first stent may be problematic as in some cases it migrates during second stent insertion. This report evaluates the safety and effectiveness of the technique and presents the long-term results of hybrid, Y-configured, dual stent-assisted coil embolization in the treatment of wide-necked bifurcation aneurysms.
We retrospectively evaluated the patients treated endovascularly due to cerebral aneurysms. Twenty patients treated with hybrid Y-stent-assisted coil embolization were enrolled in the study. In hybrid stenting, an open-cell intracranial stent (Neuroform) was used as a first stent to prevent stent migration. A closed-cell stent (Enterprise or Acclino) was used as a second stent and the aneurysm was embolized with coils between the stent struts.
In all patients, hybrid Y-stenting and coil embolization were accomplished successfully. No stent migration occurred. Clinically, neither symptomatic neurologic complication nor death was seen. Of 20 wide-necked bifurcation aneurysms, nine were at the basilar tip, while seven were at the middle cerebral artery and three at the anterior communicating artery. In one patient, the aneurysm was at the A2-3 junction of the anterior cerebral artery. One of the patients had a subarachnoid hemorrhage. The mean angiographic follow-up was 25.6 months. No in-stent stenosis was seen in any of the patients and recanalization in only one.
Hybrid, Y-configured, dual stent-assisted coil embolization is a safe and effective method in the treatment of wide-necked bifurcation aneurysms to prevent stent migration and aneurysm recanalization, and is a viable alternative to microsurgery.
Keywords
Introduction
In the treatment of cerebral aneurysms, the endovascular method is becoming more and more preferable. Recent advances in endovascular techniques and devices let us treat complex aneurysms previously not treatable with either open surgery or endovascular treatment. Stent-assisted coil embolization has been widely used in the treatment of wide-necked cerebral aneurysms for 11 to 12 years and flow diverters for six to seven years.1–7 There are many case reports and case series in the literature on wide-necked bifurcation cerebral aneurysms treated with the Y-stenting technique.8–15 This technique has been preferred in most cases because of the anatomic complexity of the aneurysm and its parent vessels.
In Y-stenting, stabilization of the first stent may be problematic as in some cases it migrates during the second stent insertion. This report evaluates the safety and effectiveness of the technique and presents the long-term results of hybrid, Y-configured, dual stent-assisted coil embolization in the treatment of wide-necked bifurcation aneurysms.
Materials and Methods
Patients
Summary of patients treated with hybrid, Y-configured stent-assisted coil embolization.

Abbreviations: Pat: Patient, F: Female, M: Male, SAH: Subarachnoid hemorrhage, R: Right, L: Left, MCA: Middle cerebral artery, BT: Basilar tip, ACA: Anterior cerebral artery, Acom: Anterior communicating artery, PCA: Posterior cerebral artery, SCA: Superior cerebellar artery, ICA: Internal carotid artery, Pcom: Posterior communicating artery, PICA: Posterior inferior cerebellar artery, N: Neuroform, E: Enterprise.
Hybrid Y-stenting technique
In hybrid stenting, as previously reported in our article,
13
we used two different kinds of stents (open-cell and closed-cell). An open-cell intracranial stent [Neuroform3 or Neuroform EZ: Stryker Neuroendovascular, Kalamazoo, MI, USA (formerly Boston Scientific, Freemont, CA, USA)] was used as a first stent to prevent its migration. A closed-cell stent [Enterprise: Codman Neurovascular, Inc., Raynham, MA, USA (formerly Cordis, Johnson and Johnson Medical, Miami, FL, USA) or Acclino: Acandis GmbH&Co. KG, Pforzheim, Germany] was used as a second stent and the aneurysm was embolized with coils using a microcatheter jailed under the second stent. In all patients, to facilitate second stent deployment, the first stent was placed in the most acutely angled branch (Figure 1).
Sequential representative illustrations of wide-necked basilar tip aneurysm treatment with hybrid Y-stent-assisted coiling: After insertion of the first open-cell stent (Neuroform) in the most acutely angled branch (A), the controlateral branch is catheterized (B). Then a microcatheter to be used for coiling is placed inside the aneurysm (C) before the insertion of the second closed-cell stent (Enterprise). After insertion of the Enterprise (D), the aneurysm is coiled with the microcatheter jailed between the Neuroform and the Enterprise stents (E).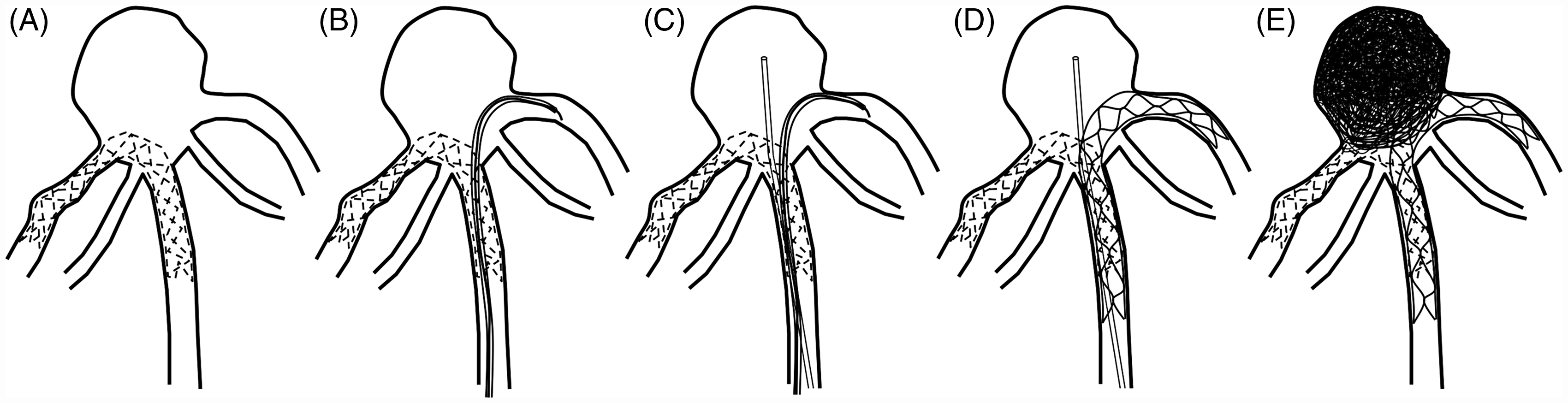
Using long introducers and guiding catheters, access was gained to the internal carotid artery or the vertebral artery after general anesthesia had been administered. First, a Neuroform stent (3 or EZ) was deployed as a first stent after catheterization of the most acutely angled branch. After the Neuroform stent, a Prowler Select Plus (Codman) transport microcatheter of an Enterprise stent was advanced passing the Neuroform stent struts using a microguide wire (0.016 inch, double-angled, 180 cm; Terumo Medical Corporation, Tokyo, Japan) through the other branch. Then the Enterprise stent was deployed in the desired position to configure the Y shape. In one patient (Patient 12), instead of the Enterprise, an Acclino closed-cell stent was placed using its own transport microcatheter with a 0.012 double-angled microguide wire (Terumo).
The aneurysm was catheterized with an Excelsior SL-10 microcatheter (Stryker) jailed under the Enterprise stent after the Neuroform stent deployment or after the second stent insertion. Then the aneurysm was embolized as completely as possible with detachable coils in 17 patients. In one patient, an ACA A2-3 junction aneurysm was treated with only Y-stenting (Patient 8). In another patient treated with stent-assisted coiling (with a Neuroform stent) due to a BT aneurysm, recanalization of the neck of the aneurysm was detected with contrast MR angiography one year later. This recanalization was treated with an Enterprise stent and coiling, making Y-configured hybrid stenting (Patient 4). In one patient with a ruptured BT aneurysm, the aneurysm was embolized with the balloon-remodeling technique [Hyperglide 4x20 mm: Covidien AG, Paris, France (formerly EV3, MTI, Irvine, CA, USA)]. But due to coil protrusion and aneurysmal dilation in the left and right orifices of the posterior cerebral arteries (PCAs), hybrid Y-stenting was applied (Patient 9).
Medication
One or ten days before the treatment, 100–300 mg of acetylsalicylic acid (Aspirin; Bayer Healthcare, Germany) and clopidogrel (Plavix; Bristol-Myers Squibb/Sanofi Pharmaceuticals, NY, USA) were administered. If antiplatelet medicines were started one day before the treatment, 450 mg (six tablets) of clopidogrel was given. If the antiplatelets were begun ten days before, we administered 75 mg of clopidogrel (one tablet) a day and evaluated the sensitivity of Plavix and Aspirin with VerifyNow two days before treatment. Based on antiplatelet sensitivity, doses were increased or clopidogrel was changed to ticlodipin, but treatment was not cancelled. In the patient with the ruptured BT aneurysm, stent usage was not planned and no antiplatelet medicine was administered. But due to coil protrusion and aneurysmal dilation, hybrid Y-stenting was performed after coiling. After stenting, Tirofiban (Aggrastat, Merck&Co., Inc., NJ, USA), the antiplatelet medicine was administered via a 0.5 mg IV. Aspirin and a loading dose of clopidogrel were administered by nasogastric tube one hour after embolization (Patient 9). In another patient, embolization was performed under Aspirin and Coumadin due to mitral valve replacement (Patient 3).
After femoral artery access, 5000–7500 IU heparin was administered IV and the serum-activated coagulation time (ACT) was checked targeting 250–300 seconds. During the procedure, 1000 IU or more of heparin were administered per hour to provide the ACT one to two times higher than the baseline value.
After the procedure, 750–1000 IU/h heparin was infused for 24 hours. Low molecular heparin (2x0.4-0.6 ml) for three to seven days was administered subcutaneously after cessation of IV heparin. Clopidogrel was stopped three to six months later and Aspirin was continued indefinitely.
Follow-up
After the procedure, computed tomography (CT) was performed to detect any hemorrhagic complication that might have occurred during the procedure. All patients were evaluated for any ischemic lesion with conventional and diffusion-weighted magnetic resonance imaging (MRI) one to three hours before the procedure and one day later. After discharge, all patients were checked clinically or by telephone. The first follow-up angiograms were performed after three to seven months. The second and third ones were performed one and three years later.
Results
In this study, 14 of 20 patients were females (70%) and six (30%) were males. Their ages were between 37 and 74 years (mean: 53 years). In all patients, hybrid Y-stenting with or without coiling was accomplished successfully (Figure 2). Complete or nearly complete occlusions were obtained in all patients except one. In that patient, who had an A2-3 junction aneurysm of the ACA, only hybrid Y-stenting was performed (Patient 8, Figure 3).
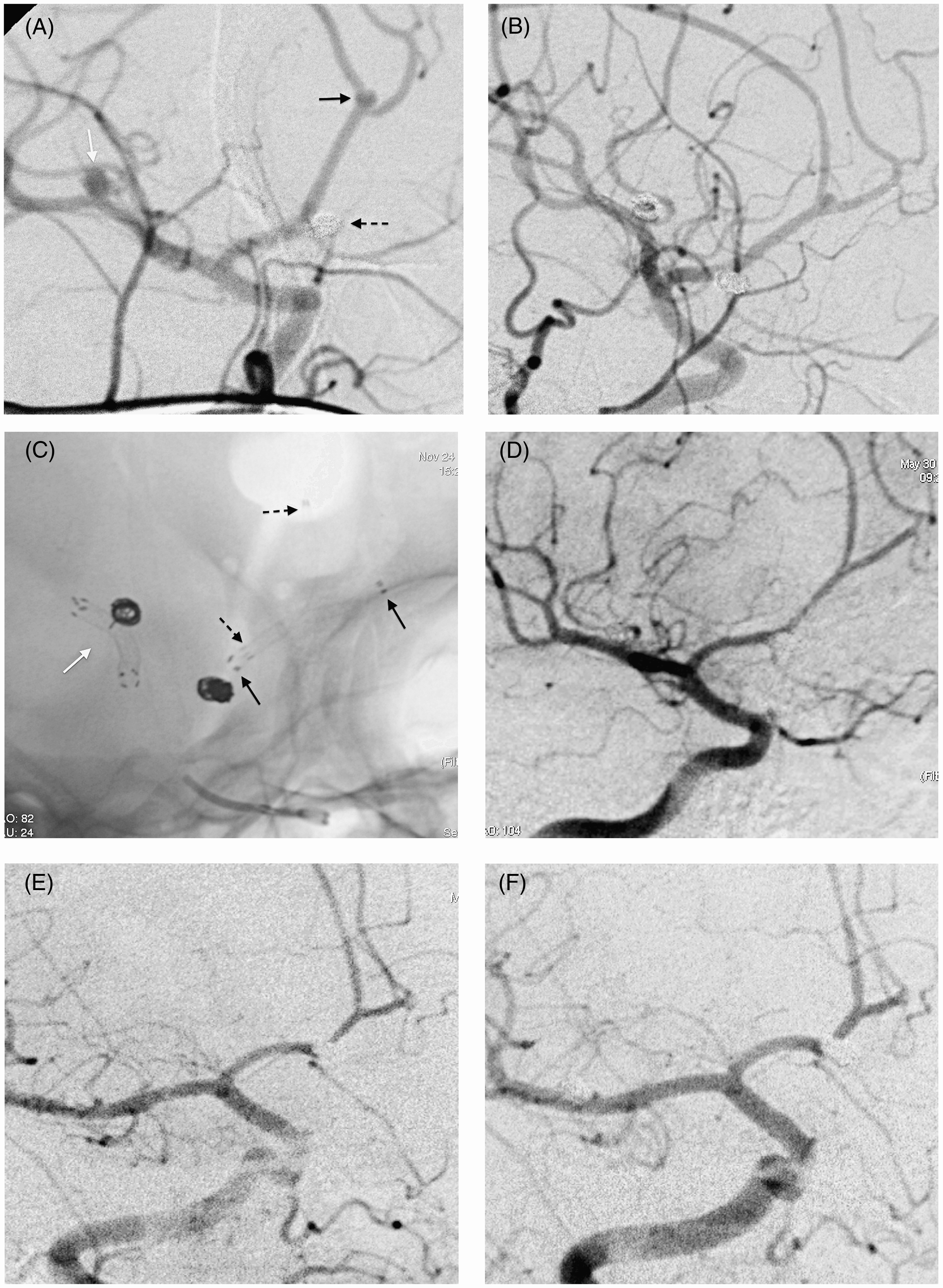
Patient 10. A,B) 3D rotational (A) and digital subtraction angiograms (B) show a wide-necked aneurysm located at the bifurcation of the left middle cerebral artery. C-E) Working (C) and Towne (D) projections show the nearly total occlusion of the aneurysm in the assistance of Y-stenting with the Neuroform (black arrows in E) and the Enterprise (white arrows in E) stents. Follow-up angiograms performed in the 6th (F) and 18th (G) months show the aneurysms totally occluded, no recanalization and no in-stent stenosis. Patient 8. A) Digital subtraction angiography shows the wide-necked aneurysms at the middle cerebral artery bifurcation (white arrow) and A2-3 junction of the anterior cerebral artery (black arrow), and embolized aneurysm of the anterior communicating artery (dashed arrow). The A2-3 junction aneurysm (B) was treated with only hybrid Y-stenting using a Neuroform (black arrows in C) and an Enterprise (black dashed arrows in C) while the bifurcation aneurysm of the middle cerebral artery (B) was coiled with the assistance of the double Neuroform stents (white arrow in C) due to the coil protrusion. The A2-3 junction aneurysm of the anterior cerebral artery was not filling and no in-stent stenosis was seen in the 6th (D), 18th (E) or 31st (F) month follow-up angiograms. In addition, the middle cerebral and anterior communicating artery aneurysms were not filling.
Of 20 wide-necked bifurcation aneurysms, nine (45%) were at the BT, while seven (35%) were at the middle cerebral (MCAs) and three (15%) at the anterior communicating arteries (Acoms). In one (5%) patient, the aneurysm was at the A2-3 junction of the ACA. One (5%) of the patients had a subarachnoid hemorrhage of the basilar artery aneurysm. Hybrid Y-stenting and coil embolization were performed in recanalized aneurysms previously treated with coil embolization in three patients and with surgery in one (Patient 15). The other 16 patients had not been previously treated.
Clinically neither symptomatic neurologic complication nor death was seen. Cranial CT performed urgently after the procedure did not show any intraparenchymal or SAH. In eight (40%) of the patients, one or more small asymptomatic ischemic lesions were detected on diffusion-weighted MRI.
The mean angiographic follow-up was 25.6 months (6-52 months). No in-stent stenosis was seen in any of the patients and recanalization in only one. In that patient (5%) with a BT aneurysm, minimal but stable recanalization in the neck of the aneurysm was seen (Patient 5, Figure 4). No additional neurological problem that might be related with the aneurysm treated was reported at clinical follow-up from ten to 60 months (mean 33.0 months) after the procedure (Table 1).
Patient 5. A-F) The ruptured wide-necked basilar tip aneurysm coiled with the balloon-remodeling technique (A-D) showed progressive recanalization in the neck of the aneurysm in follow-up angiograms performed in the 3rd (E) and 9th (F) months. G,H) The aneurysm neck was coiled with the assistance of hybrid Y-stenting performed with Neuroform (white arrows in H) and Enterprise (black arrows in H) stents. Follow-up angiograms performed in the 3rd, 6th, 18th (I) and 36th (J) months showed stable small recanalization in the neck of the aneurysm.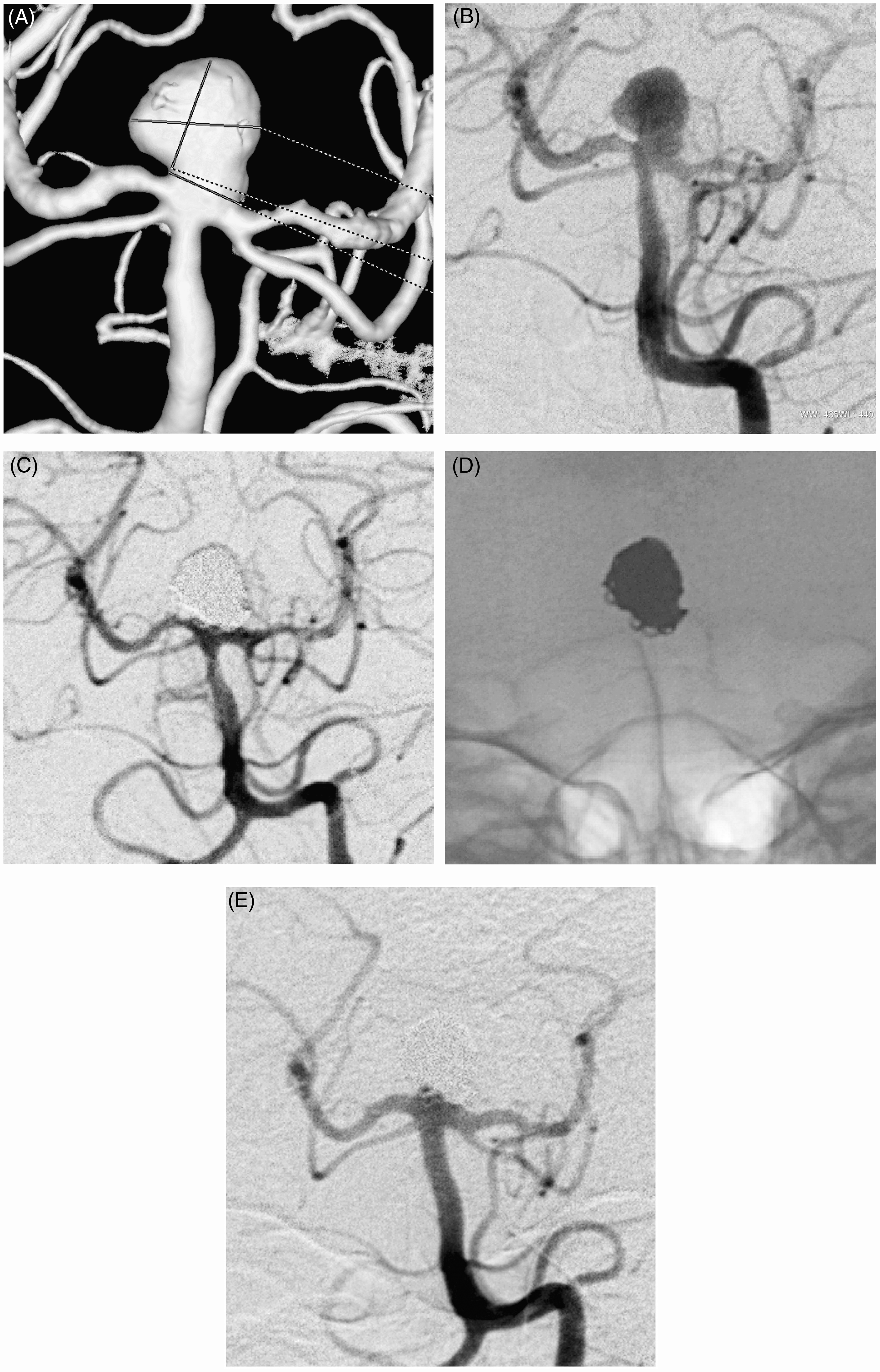
Discussion
Y-stent-assisted coil embolization is a preferable option in the treatment of wide-necked, complex bifurcation, unruptured aneurysms in some centers, ours included. A single stent may not protect the other branch from coil herniation. 10 The Y-stenting technique has been well-defined in our previous and other publications.9–17 In this technique, the second stent partially overlaps the first stent at the proximal part and the aneurysm neck and all parent vessels are reconstructed and protected from coil herniation. This technique was first described by Chow et al. in 2004. 8 They performed the technique without any complications in a patient with a wide-necked unruptured BT aneurysm. They used two self-expanding Neuroform stents to construct the Y configuration.
When we evaluated the articles considering Y-stenting in the treatment of wide-necked bifurcation aneurysms, generally two open-cell Neuroform stents (the first an intracranial, self-expanding stent) were preferred.8–11,14,16–18 In some articles, two identical stents produced by other companies were used for the same purposes. For example, two Enterprises, 12 two Solitaires,19,20 or two LVIS Jr’s (Microvention, Tustin, CA, USA). 15 During some meetings, we saw at least two live cases in which the second Neuroform stent could not be passed between the struts of the first Neuroform stent. In the first wide-necked MCA bifurcation aneurysm we treated with Y-stent-assisted-coiling, we inserted a long Enterprise closed-cell stent as the first stent. But while trying to pass the struts of the first stent with a Prowler Select Plus microcatheter to insert the second Enterprise, the first Enterprise dislodged into the aneurysm. 13 After those experiences, we preferred hybrid stenting in Y-configuration to provide stabilization of the first stent and to pass easily while trying to advance the second stent between struts. In such cases, a Neuroform open-cell stent was chosen as the first stent. When deploying the Neuroform stent, its struts behave as anchors and stabilize the stent due to the open-cell design. Stent migration is nearly impossible while trying to advance the transport catheter of the second stent between the struts of the Neuroform. Another benefit of choosing Neuroform as the first stent is that the spaces between the struts of the Neuroform are wider than other closed-cell intracranial stents. So the second stent can open more between struts at the junction. The reason for choosing Enterprise as the second stent is that the transport catheter (Prowler Select Plus) of the Enterprise is thinner than the transport catheter of the Neuroform3 stent (2.3 F and 2.8 F respectively). So passing the first stent struts with the Prowler Select Plus catheter is easier than with the Neuroform transport catheter. Now thinner stents and transport microcatheters (1.9 F) than Enterprise and Prowler Select Plus are possible. So using thinner microcatheters to insert thinner, closed-cell intracranial stents (Acclino, LVIS Jr, LeoBaby) it is easy to pass between the struts of the Neuroform stent. In one of our cases, we deployed Acclino as the second stent after the Neuroform to obtain Y configuration (Patient 12).
Stent migration is a procedural complication. It is very important to place the first stent in the proper location and the procedure needs experienced hands. Even if the first stent is properly placed, it is possible to encounter stent migration into the aneurysm sac during manipulations for deployment and positioning of the second stent. Since the Neuroform stent has an open cell design, it is very rare to see stent migration when compared to closed cell design of the Enterprise stent. In our first case with an MCA aneurysm (not included in the present series), the Enterprise stent we used first protruded inside the sac while trying to pass the first stent struts. 13 Even though Lozen et al. 11 reported that movement of the first stent did not lead to procedural complications, Thorell et al. 10 reported that they decided against second stent insertion due to displacement of the proximal portion of the first stent (Neuroform) distally into the proximal contralateral PCA, while the second stent was navigated through the struts. Spiotta et al. 14 reported a single Neuroform stent migration in a case series including 19 patients. The migration occurred while attempting to pass the microcatheter between the stent struts into the controlateral PCA. It is obvious that stent migration is more likely while trying to pass the stent struts with a microcatheter and microguide wire complex if the first stent chosen has a closed-cell design. We did not encounter in our cases any first stent migration during manipulation to insert the second stent.
Potential pitfalls of stent placement in endovascular treatment are stent-induced thrombosis and in-stent stenosis. Thromboembolic complications confirming the thrombogenicity of the stent application are the most common adverse events. 21 Stent-induced thrombosis widely depends on hyperactive platelets. 11 To prevent pre- and post-procedural stent thrombosis, it is essential to use anticoagulant and antiplatelet drugs in suitable doses and duration. In their article including seven patients with wide-necked BT aneurysms treated with Y-stent-assisted coiling, Thorell et al. 10 reported that internuclear ophthalmoplegia and partial oculomotor nerve palsy occurred in two patients after the procedure. These resolved in 24 hours with resumption of anticoagulation with heparin infusion. Yahia et al. 22 also reported delayed thromboembolic events associated with the Neuroform stent used in the treatment of intracranial aneurysms in three (4.1%) out of 65 patients. Spiotta et al. 14 reported two cases of mild neurologic symptoms (one resolved in 24 hours and the other in two weeks) due to cerebellar infarcts apparent on post-procedure MRI. They saw asymptomatic emboli on MRI in a third patient. Martinez-Galdamez et al. 20 reported no arterial spasm, rupture or thromboembolic complications in their six cases treated with Y-stent-assisted coiling using two Solitaire stents. Most of the published articles on aneurysms treated with Y-stenting reported no in-stent stenosis on follow-up angiograms.10,11,15,17,20 Spiotta et al. 14 reported only one case of stenosis in their nine cases of aneurysms treated with Y-stent-assisted coiling. In that case, a P1 segment in-stent stenosis not requiring the treatment was seen. In our cases, we did not see any symptomatic thromboembolic complication or arterial rupture, although we detected some ischemic lesions related to the treatment on diffusion-weighted MRI. In addition, we did not see any significant early or late in-stent stenosis.
The treatment of wide-necked or bifurcation aneurysms with balloon remodeling-assisted coiling has not sufficiently prevented the recanalization of the aneurysm. Recanalization rates in aneurysms treated with stent-assisted coiling have been one to three times lower than in those treated with only balloon remodelling-assisted coiling.3,23–26 If wide-necked bifurcation aneurysms are treated with Y-stenting and coil embolization, recanalization rates decrease even more. The placement of two stents in Y configuration alters the flow pattern at the aneurysm neck, redirecting the flow toward the bifurcation vessels to potentially reduce the likelihood of recanalization and thromboembolic events. Recanalization, late thromboembolic events and in-stent stenosis rates are low in articles on aneurysms treated with Y-stenting and coiling. Thorell et al. 10 reported two cases of recanalization coiled with Y-stenting in seven patients. While one required another session of coil embolization, the other did not because the recanalization was very small. In Lozen et al.’s study, 11 one case of recanalization was reported 32 months later. Spiotta et al. 14 reported two delayed thromboembolic complications in two (10.5%) of 19 patients. An angiographic recurrence requiring retreatment developed in only one patient. Lee and Kim 27 also reported a case of late in-stent thrombosis treated with intra-arterial thrombolysis using urokinase. We did not see any recanalization, late thromboembolic events or in-stent stenosis in mid- or long-term angiographic follow-up in our patients except one. In that patient, who had a ruptured BT aneurysm previously treated with balloon-assisted coiling and later treated with Y-stent-assisted coiling due to recanalization seen on angiographic follow-ups performed three and nine months later, we saw a small recanalization in the neck of the aneurysm. However, the recanalization remained stable on angiograms performed later (Patient 5, Figure 4).
Conclusion
Hybrid, Y-configured, dual stent-assisted coil embolization is a safe and effective method in the treatment of unruptured, wide-necked bifurcation aneurysms to prevent stent migration and aneurysm recanalization, and is a viable alternative to microsurgery in view of long-term results. The open-cell design preference for the first stent provides stent stabilization and prevents stent migration while the operator is attempting to pass the microcatheter between the struts of the first stent. The use of two stents preserves the parent circulation and allows more coil compaction, decreasing the recanalization rate. But it must be taken into consideration that the procedure is complex and needs experienced hands.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgment
We thank Lawrence Alan Chambers for help in linguistic corrections of our manuscript.