
Abstract
Background and purpose
Femoral artery injuries are known complications of percutaneous vascular closure devices (VCDs). We studied the incidence of delayed femoral artery angiographic irregularities after neurointerventional procedures in which the EXOSEAL extravascular closure device was used for femoral arterial puncture closure.
Methods
Adult patients who underwent femoral arterial puncture closures with an EXOSEAL VCD and had a follow-up femoral artery angiogram from June 2012 through August 2013 were reviewed. A blinded radiologist compared pre-deployment and follow-up femoral arteriograms for the presence of femoral artery stenosis, dissection, pseudoaneurysm, or development of an arteriovenous fistula. Hospital records were reviewed for major or minor complications of the groin site or femoral artery.
Results
The EXOSEAL VCD achieved hemostasis, without evidence of a groin hematoma or requiring subsequent prolonged manual compression, in 400 of 441 closures following transfemoral arterial access, representing a device success rate of 90.7%. A total of 98 patients underwent 102 repeat angiograms following closure with the EXOSEAL VCD. The average time to the repeat angiogram was 73.5 days (range 0–488, median 28). Follow-up femoral arteriography demonstrated an irregularity in seven cases, all of which were vessel stenoses of <50%. There were no dissections, pseudoaneurysms, infections, or ischemic events in the study population.
Conclusions
Angiographic irregularities were seen in 6.86% of cases after closure with the EXOSEAL VCD. There were no clinically significant vascular complications. Thus, femoral artery closure with EXOSEAL carries a low risk of clinically significant delayed angiographic findings.
Keywords
Introduction
Percutaneous puncture of the femoral artery is the first step in performing the vast majority of diagnostic and interventional neuroradiology (INR) procedures. Subsequent vascular access site management is crucial to safe, efficient, and comfortable procedural completion. A number of vascular closure devices (VCDs) have been recently developed as alternatives to manual compression and extended bedrest for femoral arterial puncture closure. Initial studies posited VCD use as a means to increase closure efficacy, decrease time to ambulation and discharge, facilitate patient throughput, and reduce overall cost.1–8 Moreover, VCD-mediated arterial puncture closure has been shown to increase patient comfort, with patients reporting less pain than those managed with manual compression alone.6,9,10
While VCD use has increased, widespread adoption has been tempered by operator learning curve, cost, impaired or delayed ability to re-access the femoral artery after deployment, and potential for complication development.11–14 An increased frequency of access-site complications inclusive of groin hematomas,15–20 iatrogenic pseudoaneurysm formation, 19 and retroperitoneal hemorrhage21–25 has been noted. Other significant vascular complications relate to the formation of traumatic dissections at the access site with consequent vessel stenosis and limb ischemia21,26–30 as well as intra-arterial sealant deployment, 31 with the potential for local thrombosis and vessel occlusion. 28
At our institution, we use an extravascular closure device in nearly 80% of transfemoral diagnostic or interventional neuroendovascular procedures. The EXOSEAL Vascular Closure Device (Cordis Corporation, Miami Lakes, FL) is an extravascular device that gained Food and Drug Administration (FDA) approval in 2011. With no need for device preparation prior to deployment, the EXOSEAL VCD delivers a conformable, dissolvable, water-soluble polyglycolic acid (PGA) plug into the extravascular space that serves as a physical barrier to close the arterial puncture defect (Figure 1). In addition, there is no arterial compression or need for sheath exchange, and subsequent to deployment, the PGA plug dissolves within 60–90 days. The device has been shown to be safe and effective,32–34 and there have been no reports of intravascular sealant deployment or complications related to femoral artery stenosis and/or limb ischemia. To date, there have been no studies using angiographic evaluation of the femoral artery following EXOSEAL deployment as a surrogate marker for complication outcomes. Herein, we report on the results of follow-up femoral arteriography in patients who had previously undergone EXOSEAL closure following femoral arterial access for INR diagnostic and interventional procedures.
EXOSEAL device deployment, using a dissolvable polyglycolic acid (PGA) plug, involves first inserting the device into the femoral sheath (a) and securing it to the sheath to allow for intraluminal deployment of an indicator wire (b). The sheath and device are pulled back until the indicator wire is at the arteriotomy (c), and the PGA sealant is then delivered to produce permanent hemostasis and the device is removed (d). Images courtesy of Cordis Corporation, http://www.exoseal.com.
Methods
Patient population and outcomes
With approval from the University of Pittsburgh Institutional Review Board (IRB# PR008120394), we retrospectively identified all patients in whom the EXOSEAL VCD was deployed and subsequently underwent repeat angiography at the University of Pittsburgh Presbyterian Hospital from June 2012 through August 2013 (14-month period). The follow-up femoral arteriogram was performed with the introducer sheath within the ipsilateral femoral artery and was compared with the patient’s previous femoral arteriogram. Patients without femoral angiography were excluded from statistical analysis. Collected data included patient demographics and procedural factors, such as femoral sheath size and use of antithrombotic medications. An independently blinded radiologist (CH) retrospectively reviewed each follow-up femoral arteriogram to assess for the presence of a pseudoaneurysm, minor (<50%) or major (>50%) vessel stenosis, or the presence of an intraluminal filling defect. In addition, hospital records were reviewed for major or minor complications of the groin site or femoral artery.
Access and closure technique
Arterial access was gained with the oversight of two attending interventionalists. The common femoral artery was palpated just below the inguinal ligament. A micropuncture needle was used for initial access, followed by introduction of a nitinol Cope wire (B-Braun, Melsungen, Germany). Using the Seldinger technique, a 5-Fr introducer followed by a guidewire was placed and ultimately the femoral sheath was advanced over the guidewire. For diagnostic procedures a 5-Fr sheath was used, while a 6-Fr sheath was used for interventional procedures; as a consequence, a 5-Fr EXOSEAL VCD was used in patients who underwent diagnostic angiography, while a 6-Fr EXOSEAL VCD was used for those who underwent interventional procedures.
The EXOSEAL VCD was used according to the closure protocol provided by the manufacturers; of note, after sealant deployment and removal of the sheath and EXOSEAL, our operators held pressure for 2.5 minutes, while the product instructions mentioned that manual compression was required for a minimum of 60 and 90 seconds following diagnostic and interventional procedures, respectively. In cases of device failure, manual compression was held for 12–18 minutes, or until hemostasis was ensured.
Statistical analysis
Acceptable type I error was set a priori at α = 0.05 for all statistical tests. Continuous demographic characteristics were assessed for normality using the Kolmogorov-Smirnov test; normally distributed data were analyzed by t-test while the remainders were compared using the Wilcoxon Rank-Sum test. Categorical data were analyzed by Pearson’s chi-squared or Fisher’s exact test. Data were analyzed using Stata 11 (StataCorp, College Station, TX).
Results
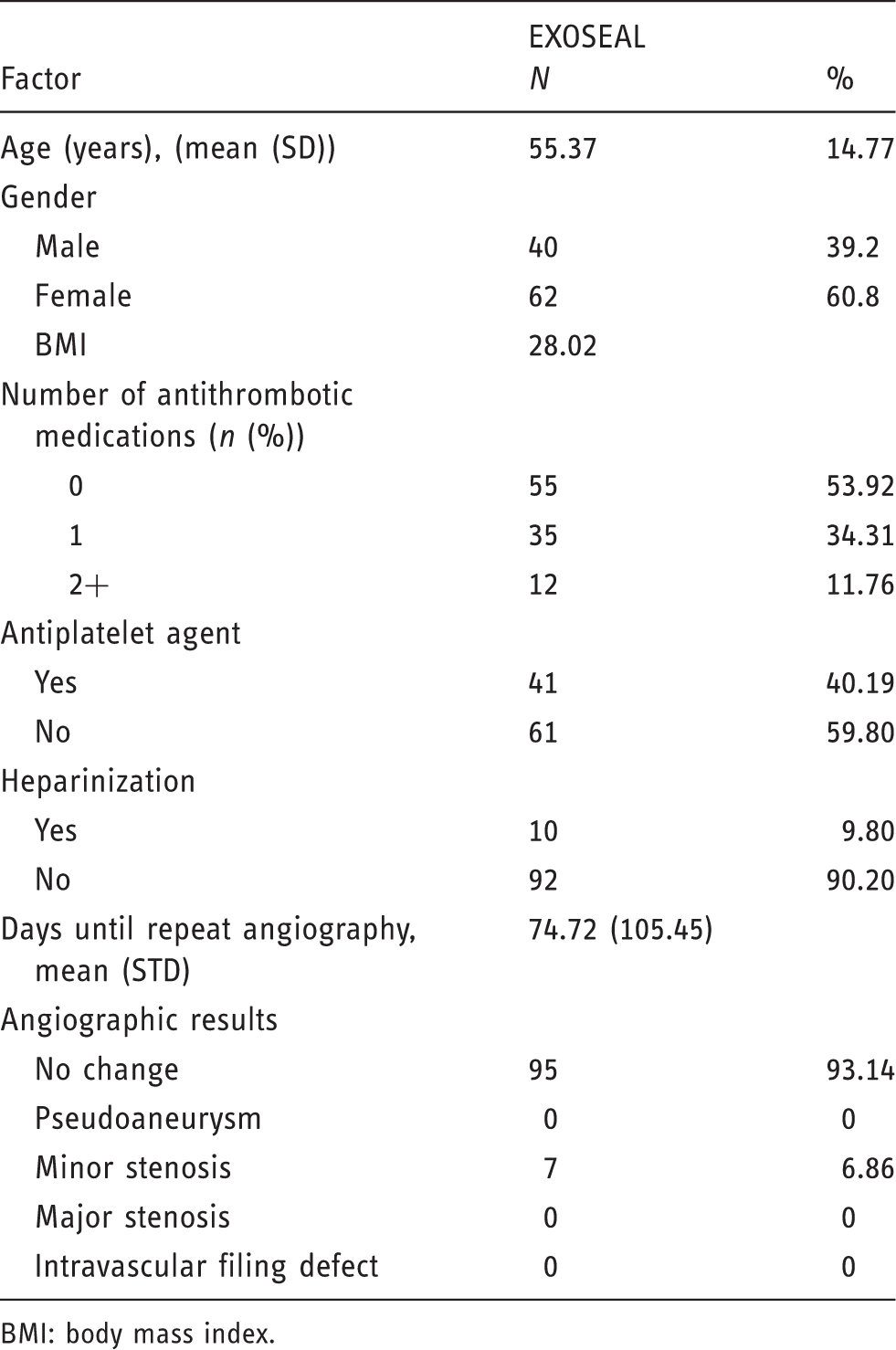
The EXOSEAL VCD achieved hemostasis, without evidence of a groin hematoma or requiring subsequent prolonged manual compression, in 400 of 441 closures following transfemoral arterial access, representing a device success rate of 90.7%. There were no major complications among the cohort, and a minor complication rate of 1.6%, owing to seven patients who developed groin hematomas that did not require transfusion. Ninety-eight patients with 102 repeat angiograms were identified during the study period. The mean age of this cohort was 55.37 ± 14.77; 60.8% were female. Three patients had more than one repeat angiogram. The average time to the repeat angiogram was 74.72 days (range 0–488, median 105.45). Baseline demographic and procedural characteristics as well as angiographic outcomes are included in Table 1. Follow-up femoral arteriography demonstrated an abnormality in seven cases (6.86%), all of which were minor vessel stenosis (average stenosis, 21%) without evidence of intraluminal filling defects (Figure 2). No dissections, pseudoaneurysms, infections, or ischemic events occurred in the study population.
Femoral angiogram of vessel stenosis observed after EXOSEAL vascular closure device (VCD) closure. Figure (a) shows the femoral artery prior to EXOSEAL VCD-mediated closure, with mild stenosis of the artery (red arrow) on follow-up angiography performed 19 days after the initial angiogram (b). Demographic, procedural, and angiographic outcome data. BMI: body mass index.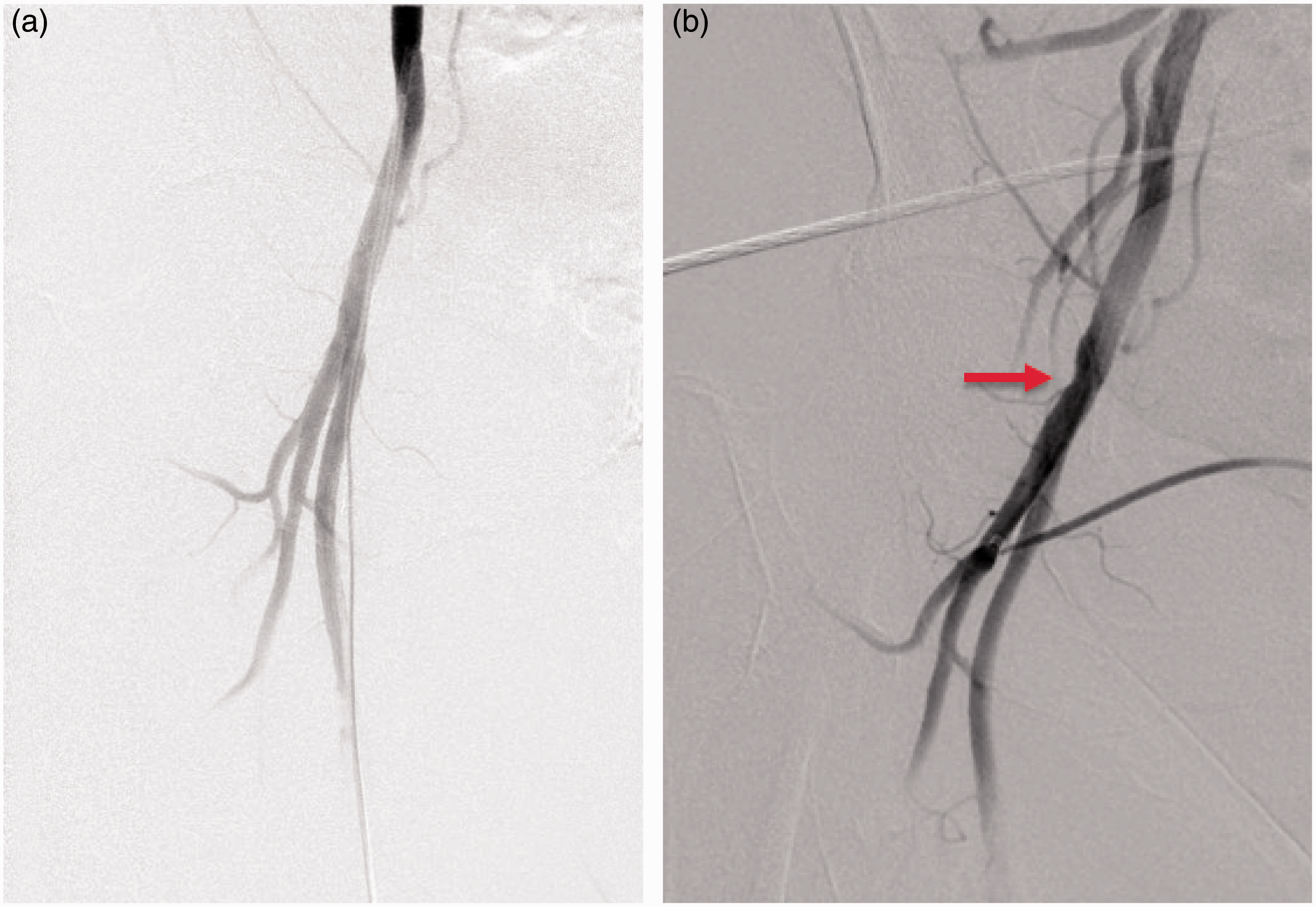
The clinical characteristics of those found to have arterial abnormalities were not significantly different; these included age, body mass index (BMI), sex, and coagulation status (international normalized ratio, platelet count, and peri-procedural antithrombotic use). Procedure-specific characteristics were also not significantly different among those with arterial abnormalities, including sheath size (p = 0.63) and procedure type (intervention vs. diagnostic). Length of time to repeat angiogram also was not significantly different between groups (p = 0.34), and no instances of minor vessel stenosis were observed in patients who underwent repeat angiography greater than 30 days after the initial study.
Discussion
Post-procedural arterial access site management is predicated on achieving hemostasis safely and efficaciously, while also enabling rapid patient ambulation with minimal morbidity or patient discomfort. Our preference has been to use an extravascular closure device in the vast majority of transfemoral diagnostic or interventional neuroendovascular procedures. The 90.7% success rate for femoral arterial puncture closure and 1.6% minor complication rate using the EXOSEAL VCD in our study is congruent with prior reports of the device’s efficacy and complication rates,32–34 and is in line with other plug-mediated closure devices. 35 No patients in our study cohort experienced symptomatic leg ischemia, and seven out of 102 patients (6.86%) with repeat angiograms were observed to have minor vessel stenosis.
The extant literature on the development of ischemic femoral vascular complications associated with the use of extravascular, plug-mediated closure devices is conflicting, and to date has involved the use of the Mynx VCD (AccessClosure, Mountain View, CA), an extravascular, plug-mediated device similar to the EXOSEAL VCD that uses a polyethylene glycol sealant that expands to 300%–400% of its initial size. Islam and colleagues reported on a patient who had previously undergone a percutaneous interventional procedure two days prior for peripheral arterial insufficiency who presented acutely with leg ischemia due to popliteal artery embolization of Mynx VCD sealant. 36 Fields et al. found that 18% of patients who had a follow-up femoral imaging study after Mynx closure demonstrated intravascular filling defects, likely due to intra-arterial sealant deployment; of note, however, with the exception of one patient, all were asymptomatic. 31 In a recent publication from our institution, surgical intervention secondary to symptomatic limb ischemia from vessel stenosis or occlusion occurred in seven out of 937 (0.75%) cases after arterial puncture closure with the Mynx VCD. 35 In contrast, among 31 patients who underwent Mynx-mediated arterial puncture closure, Fargen and colleagues found no occurrences of femoral artery complications on angiography. 37 Similarly, Taha et al. reported no instances of femoral artery complications based on the results of follow-up color Doppler ultrasound studies performed on 55 patients in whom the MynxGrip, the latest iteration of the Mynx VCD, was used. 38
Albeit rare, given the ischemic complication profile associated with the Mynx VCD, an extravascular, plug-mediated closure device similar to the EXOSEAL VCD, we sought to examine repeat angiograms after arterial closure with the EXOSEAL device to assess the rate of subclinical femoral angiographic complications as a surrogate marker for complication outcomes. As noted above, we found seven cases of asymptomatic, minor vessel stenosis. Additionally, there were no cases in which vessel stenosis was observed if repeat angiography was performed more than 30 days after initial device deployment, suggesting that the angiographic abnormalities were the result of the PGA sealant not having undergone complete hydrolysis and, in turn, in vivo dissolution of the PGA plug is likely completed around 30 days after deployment.
The EXOSEAL VCD results in femoral artery hemostasis via the deployment of a dissolvable PGA plug into the femoral sheath tract after a coiled nitinol wire on the distal tip of the device is opposed to the arterial wall. Once deployed, the PGA sealant expands to 15% of its initial size and forms a barrier, preventing blood from exiting the femoral artery. A key theoretical benefit of the device’s design and the minimal plug expansion of the PGA plug is the reduced chance of intra-arterial sealant deployment and lower likelihood of extrinsic arterial compression or deformation from the sealant, and hence, a lower likelihood of stenosis.
The initial clinical results for EXOSEAL were reported by Wong et al. in 2009, after performing a multicenter, non-blinded trial in which patients undergoing transfemoral access for diagnostic or interventional coronary or peripheral vascular procedures were randomized to use of EXOSEAL or manual compression. The device success rate of achieving arterial puncture closure after the use of a 6 F sheath was nearly 92%, with significantly decreased time to hemostasis and time to ambulation among study participants randomized to EXOSEAL closure. There were no major complications in patients on whom EXOSEAL was used, and furthermore, among a subset of patients who underwent duplex ultrasonography at 30 days post-procedure, there were no cases of pseudoaneurysm or arteriovenous fistula formation, with a 6.45% rate of subclinical vessel stenosis, 32 consistent with the findings of the cohort included herein. The subsequent 7 F ECLIPSE trial demonstrated a similar device success rate among the 60 patients studied, with no major complications, and a 0% incidence of partial vessel obstruction on repeat ultrasounds performed roughly 30 days after the index procedure. 33
Potential limitations of our study include lack of randomization or a control group. Given that we did not perform a randomized trial, a potential for selection bias exists. Also, though we discussed our previously reported experience with the Mynx VCD, we did not perform a matched-sample analysis; thus, one is unable to make any direct comparisons between the two devices. Furthermore, no inferences can be made with regards to the utility of manual closure in this setting and no comparison of angiographic outcomes between EXOSEAL closure and manual compression is provided.
Conclusion
The EXOSEAL VCD is well suited for use in most patients in the setting of INR procedures, with a historically high success rate in achieving femoral arterial puncture closure and a 6.86% incidence of minor vessel stenosis based on delayed angiography. Since all instances of stenosis were clinically asymptomatic, with no cases of pseudoaneurysm or intravascular sealant deposition, femoral artery closure with EXOSEAL appears to carry a low risk of significant ischemic complications.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.