
Abstract
In embolization of a cavernous sinus (CS) by transvenous embolization (TVE) for a CS dural arteriovenous fistula (DAVF), selection of embolization coils is difficult owing to the complex anatomical structure of the CS. Moreover, overpacking of the CS with embolization coils may cause permanent cranial nerve palsies. The ED coil-10 (EDC-10) infini is an extremely soft platinum coil without shape-memory that has excellent conformability with surrounding structures. The goal of this study was to evaluate use of the EDC-10 infini coil for embolization of a CS DAVF.
Six patients with a CS DAVF were treated with TVE. Refluxing cerebral and ophthalmic veins were embolized with shape-memory type coils other than EDC-10 infini, and CSs were embolized with the EDC-10 infini coils. In five cases, CSs were loosely embolized with EDC-10 infini coils. In one case, reflux of the cerebral vein worsened from the CS during the procedure, and embolization of the CS tightly using three-dimensional shape-memory type coils other than EDC-10 infini. Overall, three to 19 (average 7.3) coils were used fozr each CS and the total coil volume was 33–284 (average 95.1) mm3 in each CS. Postoperative transient abducens palsy occurred in two cases, but both patients recovered completely. There was no case of recurrence.
The EDC-10 infini coil showed excellent conformability with the complex inner structure of the CS and excellent safety without postoperative permanent cranial nerve palsy.
Introduction
Clinical symptoms of a cavernous sinus (CS) dural arteriovenous fistula (DAVF) arise from an abnormal communication between the arterial and venous systems. The mainstay of treatment for the disease is endovascular therapy using transarterial embolization (TAE) or transvenous embolization (TVE). TAE may be technically and feasibly simple, but is accompanied by a high recanalization rate. For this reason, TVE has become a more desirable option because of its excellent efficacy and durability of occlusion. 1 In TVE for a CS DAVF, the microcatheter generally reaches the CS via the inferior petrosal sinus (IPS) and embolizes the drainage veins that flow back to the cerebral and ophthalmic veins, and also embolizes the CS if the DAVF remains. However, it is difficult to select the proper size and type of coils for packing of the CS owing to the complicated structure and wide individual variations in the CS. Moreover, coil overpacking of the CS can result in cranial nerve palsy (CNP) or exacerbation of preexisting cranial nerve symptoms.2–7
The ED coil-10 (EDC-10) infini (Kaneka Medix Corporation, Osaka, Japan) is a 0.010-inch extremely soft bare platinum coil. Unlike most other commercially available shape-memory-type coils, the EDC-10 infini does not have substantial shape-memory and this unique feature provides excellent conformability with structures contingent to the coil (Figure 1). In this study, we examined the efficacy of the EDC-10 infini for treatment of a CS DAVF in clinical practice.
Visual representation of ED coils with (a) and without (b) shape-memory. The ED coil-10 infini (b) is an extremely soft bare platinum coil and does not have substantial shape-memory. Therefore, when the coil is dangled from the proximal end, it stretches and adopts an approximately linear shape. The ED coil-10 Soft (a) is a two-dimensional coil and maintains the coil shape when dangled.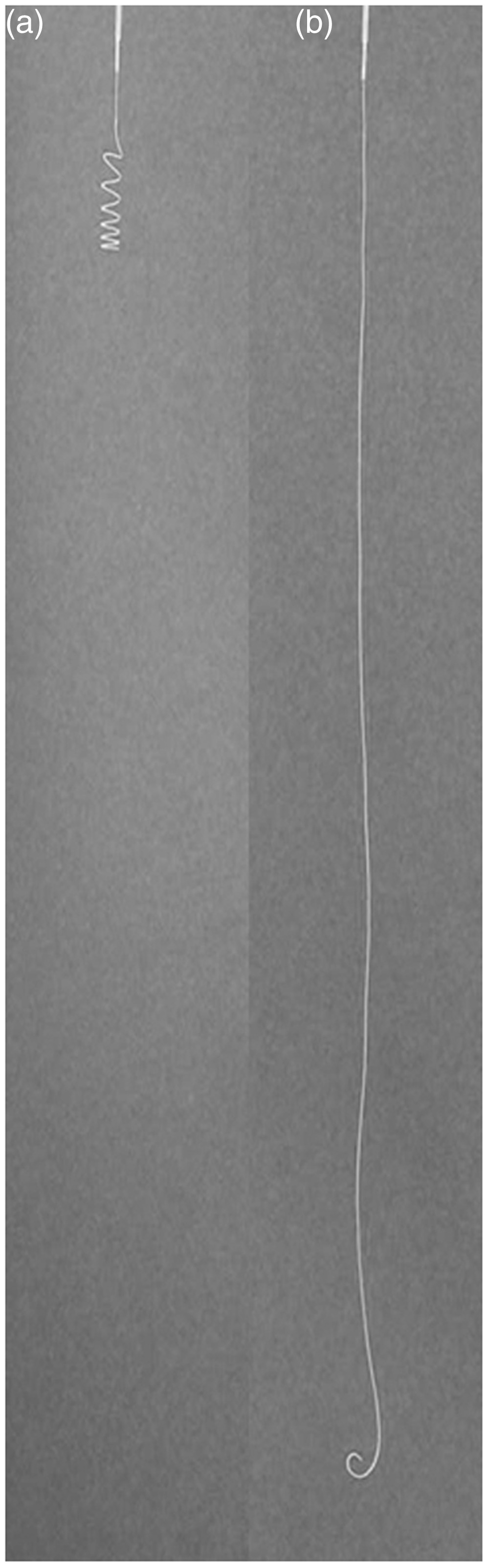
Materials and methods
Summary of patients’ information, clinical symptoms, and angiographic signs.
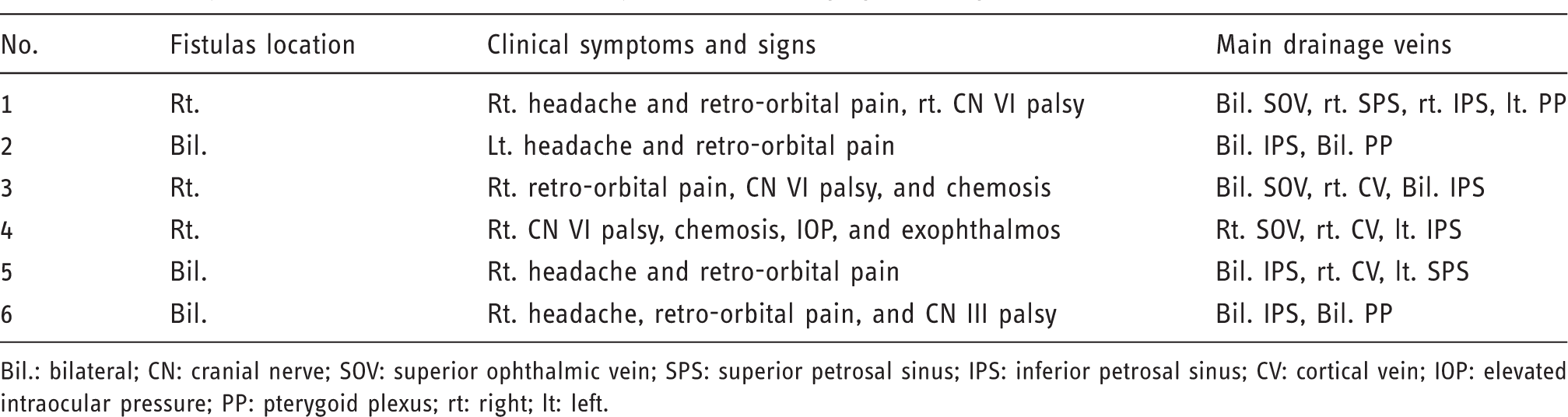
Bil.: bilateral; CN: cranial nerve; SOV: superior ophthalmic vein; SPS: superior petrosal sinus; IPS: inferior petrosal sinus; CV: cortical vein; IOP: elevated intraocular pressure; PP: pterygoid plexus; rt: right; lt: left.
Results
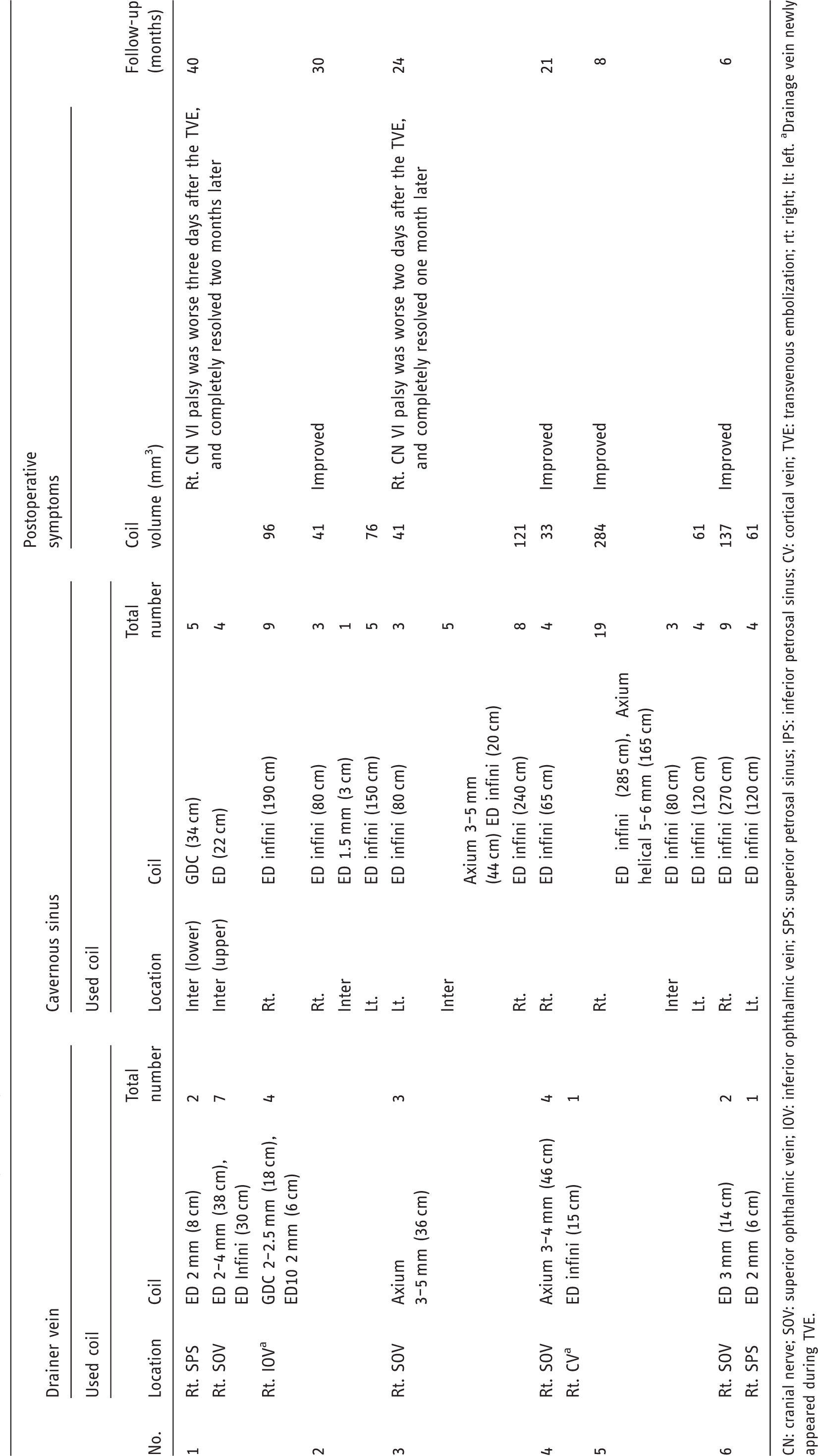
The target region, devices, complications, and clinical courses are summarized in Table 2. Technical success was achieved in all cases. In cases with reflux to the SOV or superior petrosal sinus (SPS), 2D or 3D shape-memory-type coils were used for embolization of the reflux. In those in which new cortical or ophthalmic drainage veins occurred, the drainers were embolized when the microcatheter was able to approach the target region and CSs were embolized when the target region could not be approached. Representative cases (Case 4–6) are shown in Figures 2–4, respectively. Of the six cases, the EDC-10 infini coils were deployed in 10 CSs. Three to 10 EDC-10 infini coils were required for each CS. In one case (Case 5), reflux to the SPS and sphenoparietal vein worsened during packing of the right CS and therefore the inflow zone of the CS from this vein (the lateral portion of the anterior CS where the vein outflowed) was packed tightly with 3D shape-memory-type coils other than EDC-10 infini (Figure 4). Overall, three to 19 (average 7.3) coils were used per CS and the total coil volume was 33 to 284 (average 95.1) mm3. Abducens palsy from before treatment was exacerbated in two cases on postoperative days 2 and 3, respectively, but was cured in one to two months by treatment with corticosteroids, with no residual abducens palsy. Recurrence of clinical symptoms has not been observed during a follow-up period of six to 40 months, (average 24.5 months). In two cases (Cases 5 and 6), follow-up digital subtraction angiography (DSA) was performed, and no residual DAVF were shown. In four cases with more than one year of follow-up, no abnormal findings including cerebral hemorrhage, cerebral swelling due to venous congestion, or enlarged cerebral veins have been detected on brain magnetic resonance imaging (MRI).
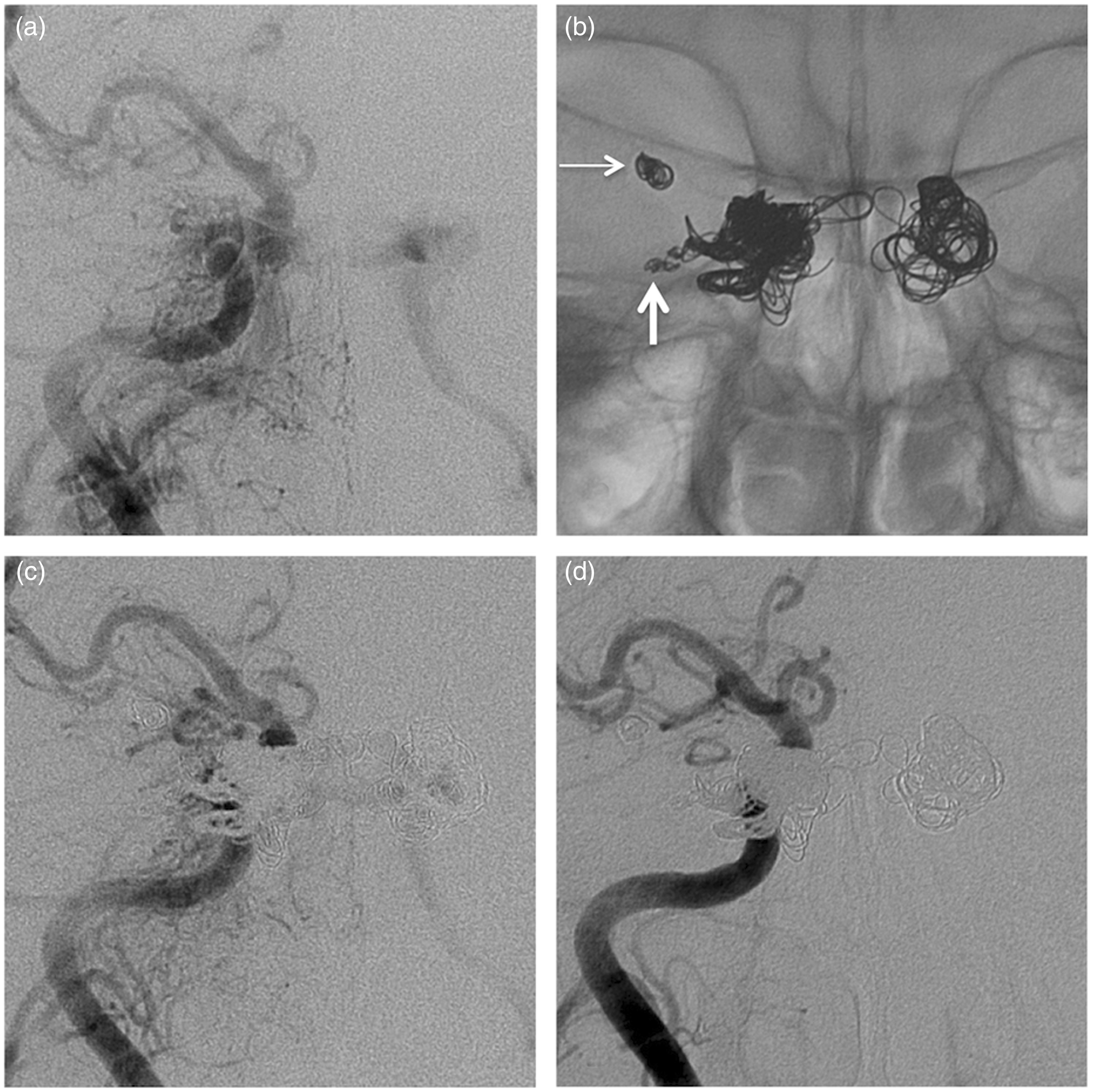
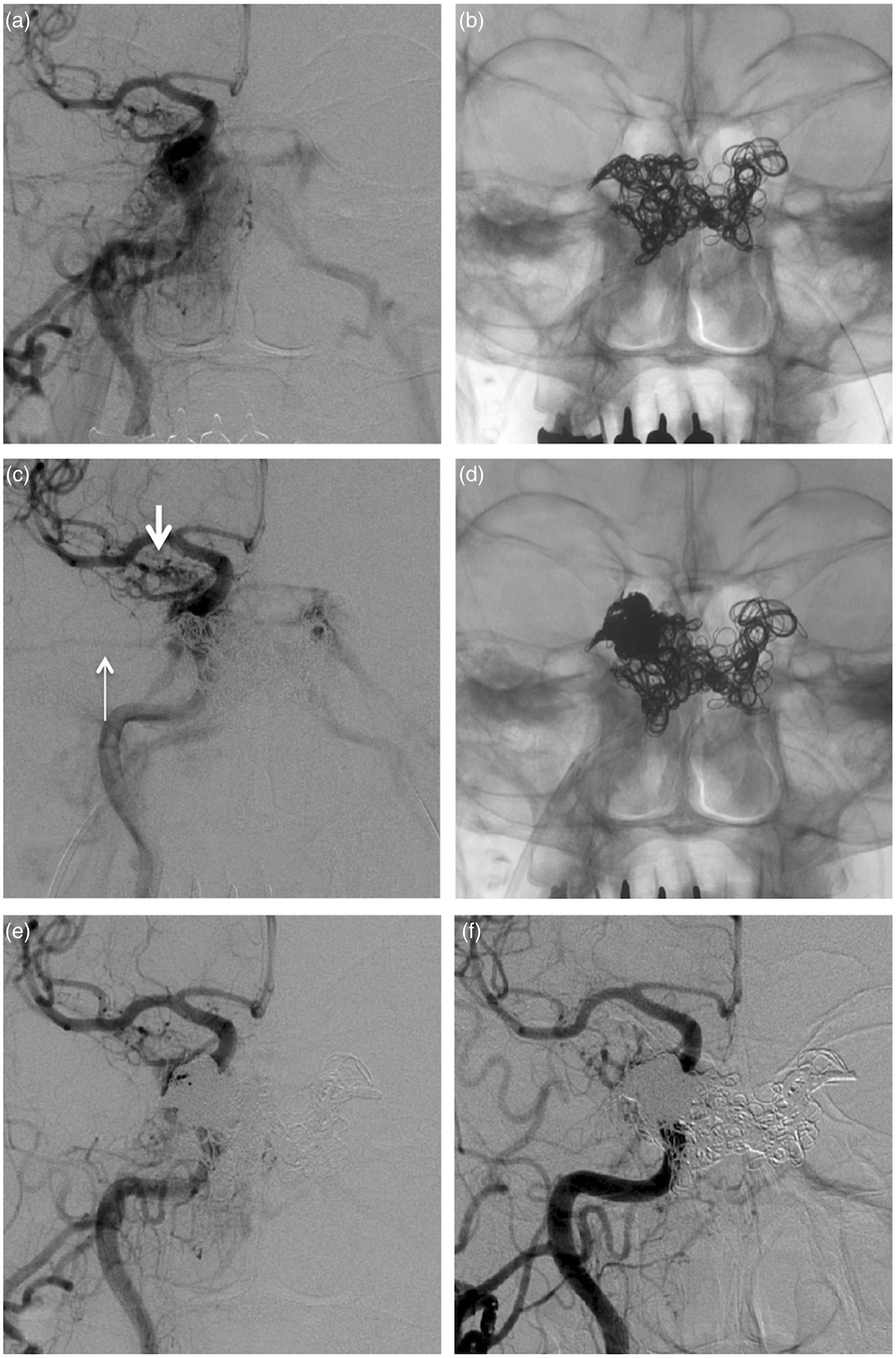
Case 4. Preoperative right common carotid angiography in anteroposterior (AP) (a) and lateral (b) views, showing the right cavernous sinus (CS) dural arteriovenous fistula with drainage roots of the right superior ophthalmic vein (SOV), right sphenoparietal vein, and left inferior petrosal sinus (IPS). Postoperative X-ray in AP (c) and lateral (d) views, showing the SOV embolized with three-dimensional shape-memory-type coils (thin arrow), and the right CS loosely packed with ED coil-10 infini coils (thick arrow). Postoperative common carotid angiography in AP (e) and lateral (f) views, showing that the right SOV was completely occluded, with slight contrast of the right CS and left IPS. Case 6. (a) Preoperative right common carotid angiography in the anteroposterior (AP) view, showing the cavernous sinus (CS) dural arteriovenous fistula (DAVF) with drainage roots of the bilateral inferior petrosal sinus (IPS). (b) Postoperative X-ray showing the right superior ophthalmic vein embolized with two-dimensional shape-memory-type coils (thin arrow), the right superior petrosal sinus embolized with two-dimensional shape-memory-type coils (thick arrow), and the bilateral CS loosely packed with ED coil-10 infini coils. (c) Postoperative common carotid angiography showing slight contrast of the bilateral CS and IPS. (d) Common carotid angiography performed 28 days after the procedure, showing disappearance of the DAVF. Case 5. (a) Preoperative common carotid angiography in the anteroposterior (AP) view, showing the cavernous sinus (CS) dural arteriovenous fistula (DAVF). (b), (c). After the bilateral CSs were loosely embolized by ED coil-10 infini coils, new reflux of the right superior petrosal sinus (SPS) (thin arrow) occurred from the posterior lateral portion of the right CS, and sphenoparietal vein (thick arrow) occurred from the anterior lateral portion of the right CS. (d) The microcatheter was navigated to the posterior lateral portion of the right CS, and this was tightly packed with three-dimensional shape-memory-type coils. Drainers of the right SPS and right middle meningeal vein disappeared. (e) Postoperative X-ray showing tight packing of the right CS with coils. (f) Right common carotid angiography performed 16 days after the procedure, showing marked flow reduction of the DAVF. Location of the embolization, materials, and results of transvenous embolization. CN: cranial nerve; SOV: superior ophthalmic vein; IOV: inferior ophthalmic vein; SPS: superior petrosal sinus; IPS: inferior petrosal sinus; CV: cortical vein; TVE: transvenous embolization; rt: right; lt: left. aDrainage vein newly appeared during TVE.
Discussion
TVEs of CS DAVF are categorized into two groups. One is compact target coil embolization, which is partial compact tight coil embolization at the fistula point with detailed analysis of micro angio-architecture of the DAVF. 6 This targeted TVE was not always indicated for all CS DAVF because of its difference of anatomical structure. In case of non-indicated target TVE such as diffuse fistula type, fistula point to the widely open sinus part, undetectable fistula point or multiple fistula points, the other TVE for CS is indicated, which is the outlet occlusion and total CS coil packing method including the fistula site. In this study, the second method of outlet occlusion and entire CS coil packing was performed in all cases.
The complex structure of the CS makes it difficult to define the precise inner structure and volume. This causes difficulty in selecting the coil size in treatment of a CS DAVF by TVE. Large coils may compress cranial nerves that run along the CS, while small coils are unstable and tend to be unevenly located. Moreover, it is difficult to measure the packing density on the basis of the volume of the CS and the number of coils used. The EDC-10 infini is an extremely soft bare platinum coil with similar mechanical and material traits to those of the ED-coil 10 Extra Soft (Kaneka Medix Corporation). However, unlike other commercially available shape-memory-type coils (including the EDC-10 Extra Soft), the EDC-10 infini does not have substantial shape-memory. This unique feature enables the coil to fit suitably in the irregular structure in the CS, and the deployment point of the coil can be readily changed by controlling the position of the microcatheter. Therefore, the EDC-10 infini is expected to pack loosely in the target region. Indeed, in a case with an embolization site distant from a drainage point in the CS, the coils loosely pack in the entire CS and other regions can then be embolized by repositioning the microcatheter. However, in a case in which the embolization site is close to a drainage point, the coils tend to fold and this results in tight packing due to the unexpected coil behavior, which is probably caused by the complicated structure of the CS. Thus, the behavior of the EDC-10 infini changes markedly depending on the procedure. The EDC-10 infini is a straight-type coil without shape-memory and has size variation up to as long as 30 cm. Therefore, fewer EDC-10 infini should be sufficient to embolize a target region compared with other shape-memory-type coils, which are generally shorter in length. The ED coil series (including the EDC-10 infini) have an audible alarm system to signify the detachment point of coil delivery. This alarm system enables operators to recognize the detachment point even when this is hidden by already deployed coils in a case in which the microcatheter is unintentionally pushed into and/or rolled through the CS.8,9 In Japan, the EDC-10 infini is approved by the Ministry of Health Labor and Welfare for the treatment of neuro-endovascular therapy.
Overpacking of the CS should be avoided because it may lead to a high incidence of CNP.2–7 In previous studies, the rates of post-procedural aggravation of CNP were 10.7%–44% of the cases,3–7 and permanent CNP occurred in 1.8%–10.0%.3,4,6,10 Nishino et al. found that CNP is prone to arise when more than 200 mm3 of coils are deployed into the CS. Embolization of the superolateral part of the anterior CS also often results in oculomotor palsy, while dense packing of the lateral portion of the posterior CS may also cause abducens palsy. 4 Bink et al. reported a significant correlation was found between coil volume and persistent CNP; in patients with unchanged, improved, and cured abducens palsies, mean coil volume in the CS was 324 mm3, 243 mm3, and 116 mm3, respectively. 5 We used the EDC-10 infini for loose packing of the CS by TVE, but the inflow portion of the DAVF in the CS was densely packed. In this way, nine out of 10 lesions were successfully treated and adequate embolization was obtained with 33 to 132 mm3 of coil mass. In one case (Case 5), reflux to the cortical vein from the CS worsened, and therefore other 3D shape-memory-type coils were required for componential tight packing of the CS. In this case, the deployed coil volume reached as high as 284 mm3, but fortunately CNP did not arise because the inner space of the CS might have expanded. Mild transient abducens palsy is likely to be affected by progressive thrombosis in the CS. This complication emerged in two cases (Cases 1 and 3) at two to three days after the procedure, but the symptoms recovered completely in one to two months. In both cases, the complication was thought to be due to thrombus formation 11 rather than a mass effect of excessively inserted coils, because the coil volumes in the two cases were relatively low (96 mm3 and 121 mm3, respectively).
The ED coil-10 infini also has some limitations in treatment of a CS DAVF. The coil tends to proceed straight in the vessel and this results in difficulty in proper embolization for reflux veins such as the SOV, SPS, or cortical veins. Therefore, 2D or 3D shape-memory coils should be used in such cases.
Conclusion
The EDC-10 infini coil has high conformability with surrounding structures and is suitable for embolization of the complicated structure of the CS. The results in this case series show that the coil is effective and safe in clinical practice.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
None declared.