
Abstract
Background
Transbrachial approach is an alternative technique for coil embolization of posterior circulation aneurysms. The purpose of our study was to investigate the anatomical features of the vertebral artery (VA) for transbrachial direct VA cannulation of a guiding catheter (GC) to perform coil embolization of posterior circulation aneurysms.
Methods
Included in retrospective analysis were patients who underwent transbrachial coil embolization of cerebral aneurysms in the posterior cerebral circulation by direct VA cannulation of a GC from 2007 to 2013. Investigated were patient characteristics, preoperative sizes of aneurysms, aneurysms location, the angle formed by the target VA and the subclavian artery (AVS), and the VA diameter at the level of the fourth cervical vertebral body (VAD) in the side of the transbrachial access route.
Results
Thirty-one patients with 32 aneurysms met our criteria. The locations of aneurysms were the VA (n = 16), basilar artery (BA) tip (n = 10), BA trunk (n = 3), BA superior cerebellar artery (n = 1), BA anterior inferior cerebellar artery (n = 1), and VA posterior inferior cerebellar artery (n = 1). The right brachial artery was punctured in 27 cases with 28 aneurysms as transbrachial direct cannulation of a GC, and left was in 4 cases with 4 aneurysms. The average AVS, ranging from 45° to 95°, was 77°, and the average VAD, ranging from 3.18 to 4.45 mm, was 3.97 mm.
Conclusion
For transbrachial direct cannulation of a GC, it seems required that the AVS is about 45° or more and the VAD is about 3.18 mm or more.
Keywords
Introduction
The transfemoral approach is a common technique for coil embolization of cerebral aneurysms in the posterior cerebral circulation. 1 However, it is difficult to advance a guiding catheter into the vertebral artery (VA) through the femoral route in patients with a tortuous aortic arch, an unfavorable supra-aortic takeoff, aortic diseases, or occlusion of the femoral artery, where transbrachial or transradial VA cannulation of a guiding catheter must be attempted. Some previous studies have reported that transbrachial or -radial approach was effective in coil embolization of cerebral aneurysms in the posterior cerebral circulation.2–6 Direct VA cannulation of a 6Fr guiding catheter must enable not only a conventional single-catheter technique but also a stent-assist or balloon-assist technique as adjuvant.7,8 However, there are no reports considering the anatomical features of the VA appropriate to transbrachial direct cannulation. The purpose of our study was to investigate the anatomical features of the target VA appropriate to transbrachial direct cannulation of a 6Fr guiding catheter to perform coil embolization of cerebral aneurysms in the posterior cerebral circulation.
Methods
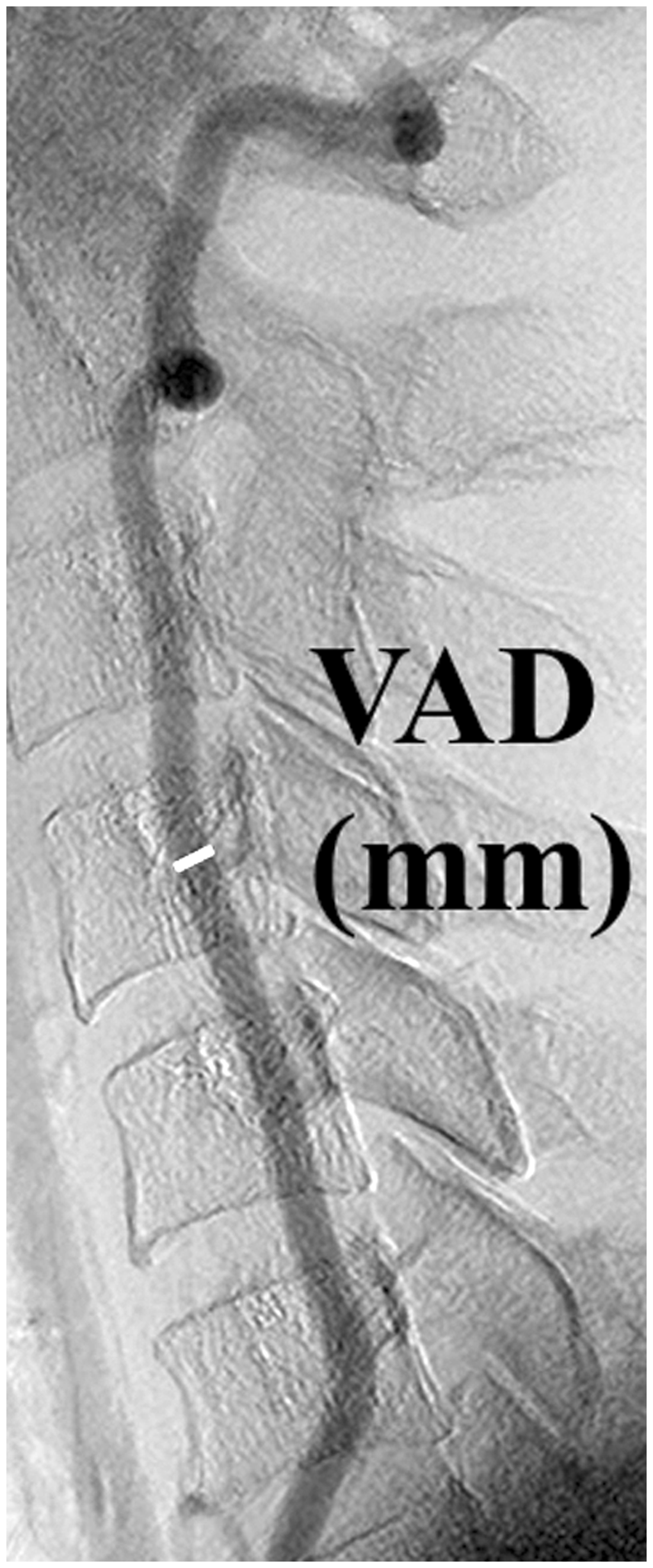
Included in our retrospective analysis were patients in whom we attempted to perform transbrachial coil embolization of cerebral aneurysms in the posterior cerebral circulation by direct VA cannulation of a 6Fr guiding catheter from January 2007 to September 2013. Before endovascular treatment, all patients had undergone transbrachial or transradial diagnostic angiography usually via the right-sided access route with a 3 F sheath, 3.2Fr catheter (125 cm, 3.2Fr MSK catheter, Medikit Co. Ltd) using 0.032 inch and/or 0.025 inch guidewire in our institution. Diagnostic angiography with biplane digital subtraction angiography (DSA) equipment (INFX-8000V, Toshiba Medical Systems Corporation, Tochigi, Japan) provided us with important information of not only three-dimensional (3D) images produced by a Workstation (Zio Station, Amin/Ziosoft, Tokyo, Japan) but also anatomical and morphological features of aneurysms, vertebral and basilar arteries. This information included the dominant sided VA, the appropriate access route to aneurysms and the diameter of the VA as the access route. AVS (the AVS (the Angle formed by the target VA and the Subclavian artery) was defined as the angle formed by the origin of the target VA and the subclavian artery (anteroposterior view) in diagnostic DSA. VAD (VA Diameter at the fourth cervical vertebral body) was defined as the VA diameter at the fourth cervical vertebral body (lateral view) in the target VA in diagnostic DSA.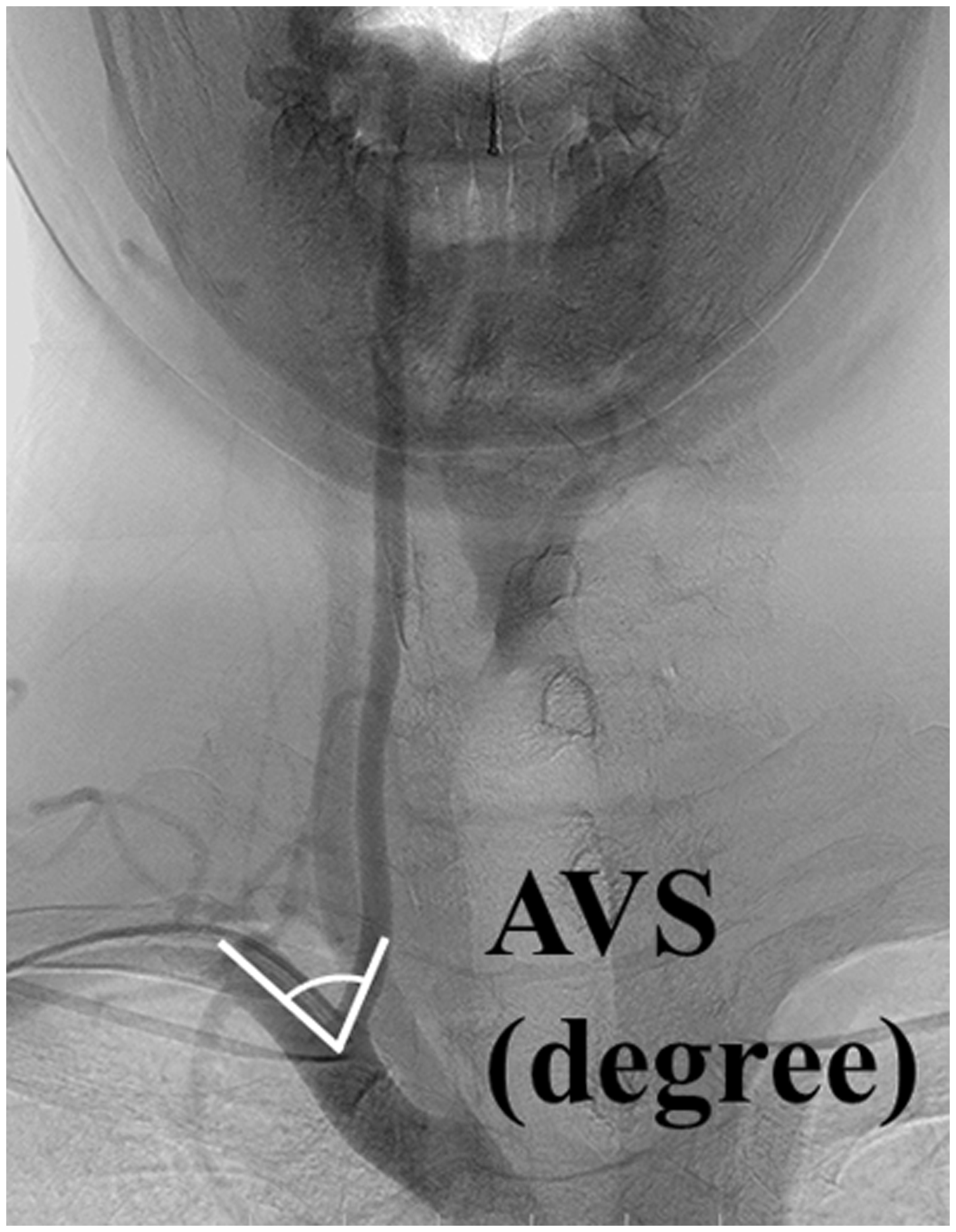
Procedural technique
Transbrachial coil embolization was performed under local anesthesia with oral etizolam. A 6Fr short sheath was inserted into the target-sided brachial artery. A 6Fr Envoy™ guiding catheter (Cordis Neurovascular, Miami Lakes, Fla) (ID (internal diameter) 0.070 inch) or 6Fr Cerulean guiding catheter (Medikit Co. Ltd, Tokyo, Japan) (ID 0.072 inch) was introduced directly into the target VA over 0.035 inch guidewire. Coil embolization was performed by using the detachable coils, i.e. Guglielmi detachable coils (Stryker Instruments, Kalamazoo, MI, USA), Orbit Galaxy detachable coil systems (Codman Neurovascular, Raynham, MA, USA), Micrus coils (Codman Neurovascular, San Jose, CA, USA), or ED coils (Kaneka Medix, Osaka, Japan). We performed embolization with a single-catheter technique for intracranial aneurysms with a narrow neck and used a balloon-assist or a stent-assist technique as adjuvants if necessary, for aneurysm with a wide neck through a 6Fr guide catheter. The balloon-assist technique was performed either with the HyperForm™ (Covidien, Mansfield, MA, USA) or HyperGlide™ balloon microcatheter (Covidien, Mansfield, MA, USA). The stent-assist technique was performed with the Enterprize™ (Codman Neurovascular, Raynham, MA, USA). Initial angiographic results of coil embolization were classified as complete occlusion (98%–100%), near complete occlusion (90%–98%), or incomplete occlusion (<90%).
Pre- and post-coil embolization management
Patients gave written informed consent to undergo coil embolization. For at least 3 days before coil embolization, they took aspirin (100 mg/day) and clopidogrel (75 mg/day) in elective cases. They continued to take aspirin (100 mg/day) and clopidogrel (75 mg/day) for three months after coil embolization. They took etizolam (3 mg t.i.d) orally on the previous day and just before the coil treatment. After the placement of the guiding catheter via brachial artery, they received intravenous heparin 5000 IU. A 6Fr sheath was removed when activated clotting time value was less than 150 seconds and hemostasis was obtained by manual compression.
Evaluation
We firstly evaluated either unsuccessful or successful direct annulation to the target, and secondly either unsuccessful or successful coil embolization procedure.
Results
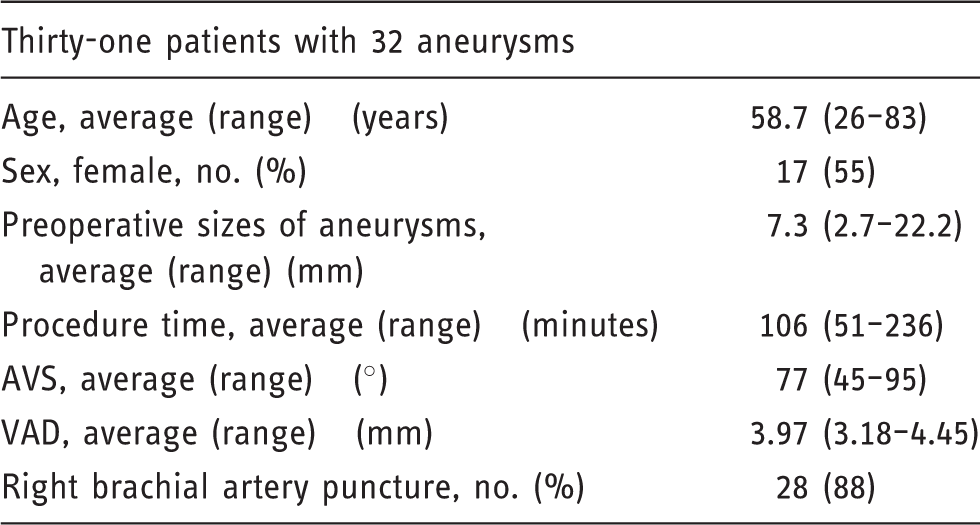
Thirty-one patients with 32 aneurysms met our criteria (Table 1). Their ages ranged from 26 to 83 years (average, 58.7 years). Seventeen patients (55%) were women. The sizes of aneurysm ranged from 2.7 to 22.2 mm (average, 7.3 mm). The locations of aneurysms were the VA (n = 16), basilar artery (BA) tip (n = 10), BA trunk (n = 3), BA superior cerebellar artery (n = 1), BA anterior inferior cerebellar artery (n = 1), and VA posterior inferior cerebellar artery (n = 1). By using information from diagnostic DSA, we performed transbrachial procedures in patients who had anatomical and morphological features suitable to transbrachial rather than transfemoral access. We measured AVS and VAD and then determined either right or left brachial artery as an access route. The right brachial artery was punctured in 27 cases with 28 aneurysms and the left one in 4 cases with 4 aneurysms. No transbrachial approach was abandoned or switched to transfemoral approach. We were successful in direct transbrachial cannulation of the 6Fr guide catheters to the VA and subsequent coil embolization in all cases (Figures 3 and 4). The average AVS, ranging from 45° to 95°, was 77°, and the average VAD, ranging from 3.18 to 4.45 mm, was 3.97 mm (Table 1). The stent-assist technique was used in 4 patients and balloon-assist techniques in 11 patients. The mean procedure time was 106 minutes (range 51–236 minutes). At the end of the coil embolization, complete occlusion was in 20 aneurysms and near complete in 12. Therefore, procedural success rate was 100%.
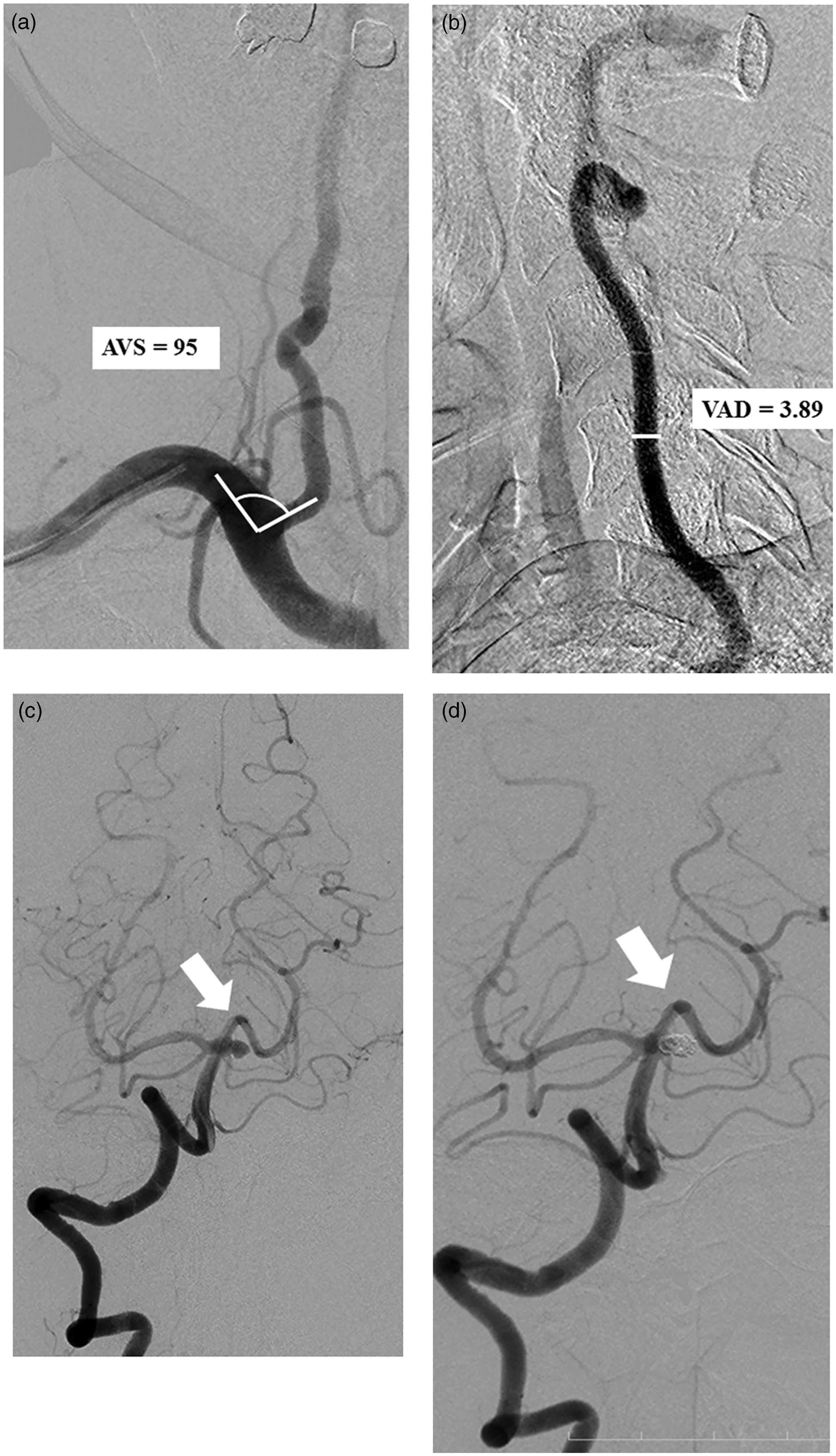
(a) Right subclavian angiogram demonstrated no stenosis of the right VA origin and the AVS was 45° in diagnostic DSA (anteroposterior view). (b) The VAD was 4.41 mm in diagnostic DSA (lateral view). (c) Right vertebral angiogram showed a dissecting fusiform aneurysm in V4 segment (arrow). (d) Final control angiogram showed successful stent-assisted coil embolization of the VA aneurysm (arrow). (a) Right subclavian angiogram demonstrated no stenosis of the right VA origin and the AVS was 95° in diagnostic DSA (anteroposterior view). (b) The VAD was 3.89 mm in diagnostic DSA (lateral view). (c) Right vertebral angiogram showed a saccular aneurysm at BA/superior cerebellar artery bifurcation (arrow). (d) Final control angiogram showed successful balloon-assisted coil embolization of the BA superior cerebellar artery aneurysm (arrow). Summary of patients.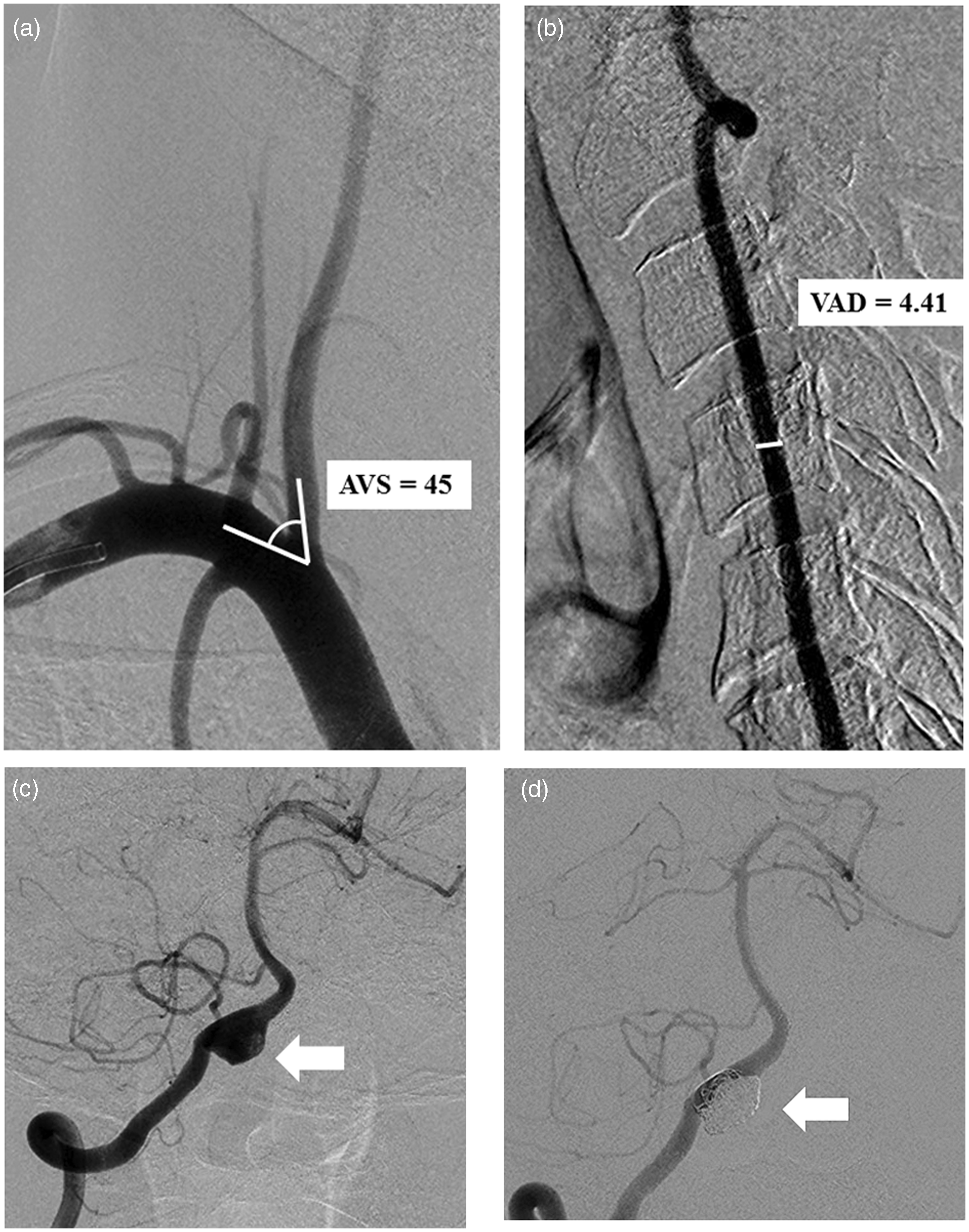
Discussion
Our results suggested that when the angle formed by the target vertebral artery and the ipsilateral subclavian artery was 45° or larger and the target vertebral artery diameter at the fourth cervical vertebral body was 3.18 mm or larger, successful transbrachial direct cannulation of a 6Fr guiding catheter to the target VA was achieved.
Cardiac interventional procedures via the brachial or radial approach are widely performed.9,10 However, transbrachial or -radial neurointerventional procedures have yet to become common.11–13 There have been no reports considering the anatomical and morphological features of the target VA appropriate to transbrachial direct cannulation. Our results demonstrate that diagnostic DSA provides useful information such as AVS and VAD to determine a suitable access route. Even though patients undergo transfemoral diagnostic angiography, it can give beneficial information of the target AVS and VAD. Not only diagnostic DSA but also aortic arch computed tomography angiography probably provides with useful information of the AVS and VAD. When interventional procedures in the posterior circulation starts through the femoral artery and transfemoral cannulation of a guiding catheter must be abandoned, information of the VSA and VAD must be important to determine switching to a transbrachial access of either the right or left access route.
A systematic review of studies involving coiling for more than 400 posterior circulation aneurysms reported that coils were able to be deposited in the target aneurysms for a high intent-to-treat success rate of 97.6% not 100%. 11 Some treatment failures might occur secondary to unfavorable anatomy. Transbrachial VA cannulation of a guiding catheter might improve an intent-to-treat success rate. Transfemoral cannulation may be appropriate to the VA with AVS smaller than 45° and its investigation is required. Our results show anatomical and morphological features of the VA where transbrachial direct cannulation to the VA can be achieved, but not where transfemoral access is problematic.
Brachial artery spasms may likely occur compared to the femoral artery because the brachial artery is smaller.9,12,13 Transradial approach is an alternative one. There are three probable risks in transbrachial approach.12,13 The first is pseudoaneurysm of the brachial artery, the second is median nerve palsy and the third is brachial artery occlusion. To the best of our knowledge, our study is the first report considering the anatomical and morphological features of the VA appropriate to transbrachial direct cannulation. A larger number of cases are required to confirm our results because of the small number in our study.
Conclusions
When the angle formed by the target vertebral artery and the ipsilateral subclavian artery was 45° or larger and the target vertebral artery diameter at the fourth cervical vertebral body was 3.18 mm or larger, transbrachial direct cannulation of a 6Fr guiding catheter to the target VA was achieved.
Footnotes
Acknowledgments
We acknowledge secretary assistance of Nozomi Chiba, BA, and the specialized assistance of nurses and radiological technicians in our neuroendovascular catheterization room.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
We have no association with any individual, company, or organization with a vested interest in the subject matter mentioned in the manuscript. Dr Iwata reports no disclosures. Dr Mori serves on the editorial board of American Journal of Neuroradiology, advises Toshiba Medical and Kaneka Medix and receives royalties from Medikit. Dr Miyazaki reports no disclosures. Dr Tanno reports no disclosures. Dr Kasakura reports no disclosures. Dr Aoyagi reports no disclosures.