
Abstract
Background
Staged endovascular embolization of large arteriovenous malformations (AVMs) is frequently performed to gradually reduce flow and prevent abrupt hemodynamic changes. While feeding artery aneurysms have been associated with increased risk of hemorrhage in the setting of AVMs, decisions regarding if and when to treat these aneurysms vary. Acute, fatal rupture of a feeding artery aneurysm following embolization of a large, unruptured AVM has been infrequently reported in the literature.
Case description
A 69-year-old female presented with headache and mild left hemiparesis referable to a 5 cm right fronto-parieto-temporal AVM with surrounding vasogenic edema. The AVM was associated with numerous bilateral feeding artery aneurysms (the largest was a 2 cm right middle cerebral artery (MCA) bifurcation aneurysm). There was also a large, partially thrombosed venous varix. Staged embolization of the AVM was performed. Several hours after the third stage of her embolization, she became obtunded, with a fixed and dilated right pupil. Head computed tomography (CT) showed a large intraparenchymal hemorrhage with midline shift in the right sylvian fissure, remote from the AVM nidus. She was taken to surgery for a decompressive craniectomy and hematoma evacuation. The MCA aneurysm was confirmed to be the source of hemorrhage and it was clipped. Despite aggressive medical and surgical treatments, the patient died.
Conclusions
An increase in AVM feeding artery pressure following endovascular embolization may contribute to the rupture of a feeding artery aneurysm. For this reason, treatment of large arterial aneurysms on feeding pedicles should be considered prior to embolization of the AVM nidus.
Keywords
Introduction
Given the unpredictable hemodynamic changes following occlusion of large arteriovenous malformations (AVMs), staged endovascular embolization is frequently performed in an effort to gradually reduce flow through the fistula and prevent untoward treatment effects. Notably, in 3–58% of cases, concomitant arterial aneurysms—whether on the feeding vessel, within the nidus, or on an unrelated artery—are found in patients harboring AVMs.1–3 Multiple lines of evidence support the notion that feeding artery aneurysms in particular increase the risk of AVM-related hemorrhage.1,4–6 It is likely that AVM-associated arterial aneurysms may not themselves be the source of hemorrhage in such instances, but may represent an indicator of a hemodynamically tenuous system that is more predisposed to hemorrhage. However, significant disparity exists regarding the treatment strategy for patients with AVM-related feeding artery aneurysms. While some authors propose that treatment of the AVM itself should be the principal goal of therapy.7,8 other authorities advocate prompt, aggressive treatment either of the arterial aneurysms9,10 or of both lesions concurrently.8,11 Certainly, a unified recommendation for the management of AVM-associated arterial aneurysms is presently lacking.
In this report, the authors present the case of a 69-year-old woman who presented with signs and symptoms referable to a 5 cm, unruptured, right frontal-parieto-temporal AVM with numerous feeding artery aneurysms and a large, partially thrombosed venous varix. Significant vasogenic edema surrounding the lesion was seen on neuroimaging. Following the third stage of a multi-tiered endovascular treatment strategy to reduce flow within the AVM, a 2 cm feeding artery aneurysm ruptured. Despite aggressive medical and surgical interventions, the patient died. Here, we review this complex case and propose potential mechanisms to explain the acute rupture of the feeding artery aneurysm following endovascular AVM embolization.
Case report
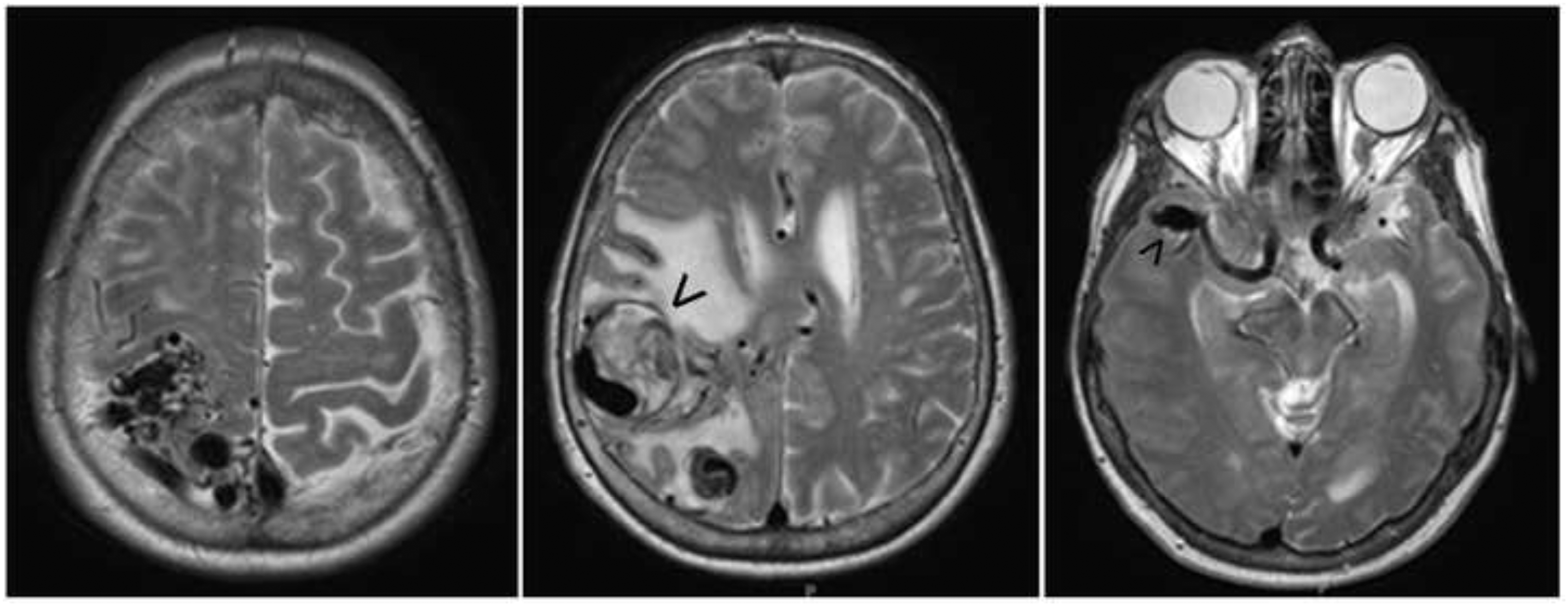
A 69-year-old female with a history of hypertension and chronic obstructive pulmonary disease was referred to our institution with a 2–3-week history of worsening headaches and mild left hemiparesis (upper > lower extremity). A non-contrast head CT showed a large, partially calcified, iso- to hyperdense mass in the right fronto-parieto-temporal region with surrounding edema and midline shift (Figure 1). Magnetic resonance imaging (MRI) revealed a complex vascular lesion which was iso- to hyperintense to gray matter on T2-weighed imaging and had numerous dilated vascular channels and flow voids (Figure 2). Also noted was a large, partially thrombosed vessel (Figure 2, large arrowhead) and a right middle cerebral artery (MCA) bifurcation aneurysm (Figure 2, small arrowhead).
Axial sections of a non-contrast head CT demonstrate a large, iso- to hyperdense mass in the right fronto-parieto-temporal region with scattered areas of calcification and significant surrounding edema, mass effect, and right-to-left midline shift. Axial sections from a T2-weighted MRI demonstrate a large, iso- to hyperintense lesion in the right fronto-parieto-temporal area with numerous dilated vascular channels and flow voids. A large, partially thrombosed venous varix (large arrowhead) and right MCA bifurcation aneurysms (small arrowhead) are also well visualized.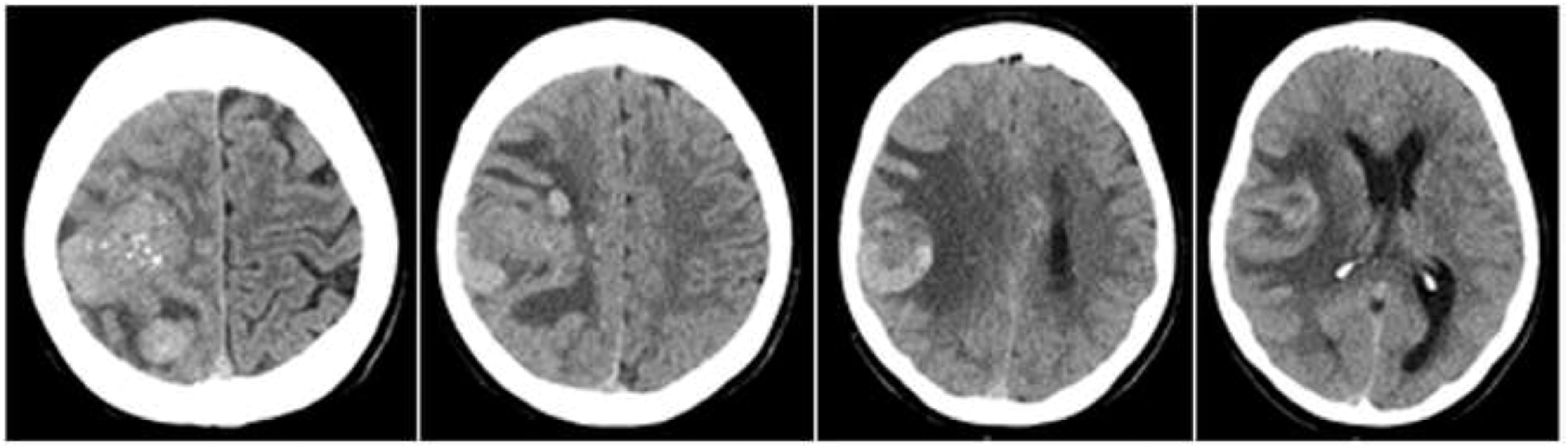
Cerebral catheter angiography verified a large fronto-parietal-temporal AVM (nidus = 5 × 4 × 4 cm) supplied by hypertrophied right MCA and anterior cerebral artery (ACA) branches (Figure 3). Venous drainage was predominantly superficial into the superior sagittal sinus through cortical veins, but also included a smaller deep venous component via the vein of Galen (Figure 3(H), small black arrowheads). There was a large (3 cm), partially thrombosed venous varix arising from a draining parietal cortical vein (Figure 3, large white arrowhead). The Spetzler-Martin grade was 4 (Size = 2, Eloquence = 1, Drainage = 1).
12
Multiple, bilateral feeding artery aneurysms were identified (eight in total), the largest of which was a 2 × 1 × 1 cm right MCA bifurcation aneurysm (Figure 3(B), small white arrowhead). The other aneurysms (Figure 3, small white arrowheads) involved the distal right MCA (3 mm, Figure 3(B)), right ophthalmic artery (3 mm, Figure 3(B)), right pericallosal artery (7 mm, Figure 3(E)), left cavernous carotid artery (2 mm and 1 mm, respectively, Figure 3(J)), and anterior communicating artery complex (7 mm and 2 mm, respectively, Figure 3(L)). The patient was started on dexamethasone therapy for the vasogenic edema that was believed to be responsible for her hemiparesis.
Anteroposterior (A–D) and lateral (E–H) views of the cerebral vasculature following a right common carotid artery contrast injection. Early arterial (A, E), mid to late arterial (B, F), early to mid venous (C, G), and late venous (D, H) phases are depicted. Anteroposterior (I), lateral (J), and oblique (K) views of the cerebral vasculature after a left common carotid artery contrast injection are also shown, as well as a three-dimensional rotational angiogram (L). As shown, there is a 5 × 4 × 4 cm AVM that receives arterial supply from the right MCA and ACA and drains into the superior sagittal sinus and vein of Galen. There is a large, partially thrombosed venous varix arising from a parietal cortical vein (large white arrowhead) and multiple, bilateral AVM-associated arterial aneurysms (eight in total; small white arrowheads). The largest aneurysm (2 × 1 × 1 cm) resides on a feeding artery pedicle at the right MCA bifurcation.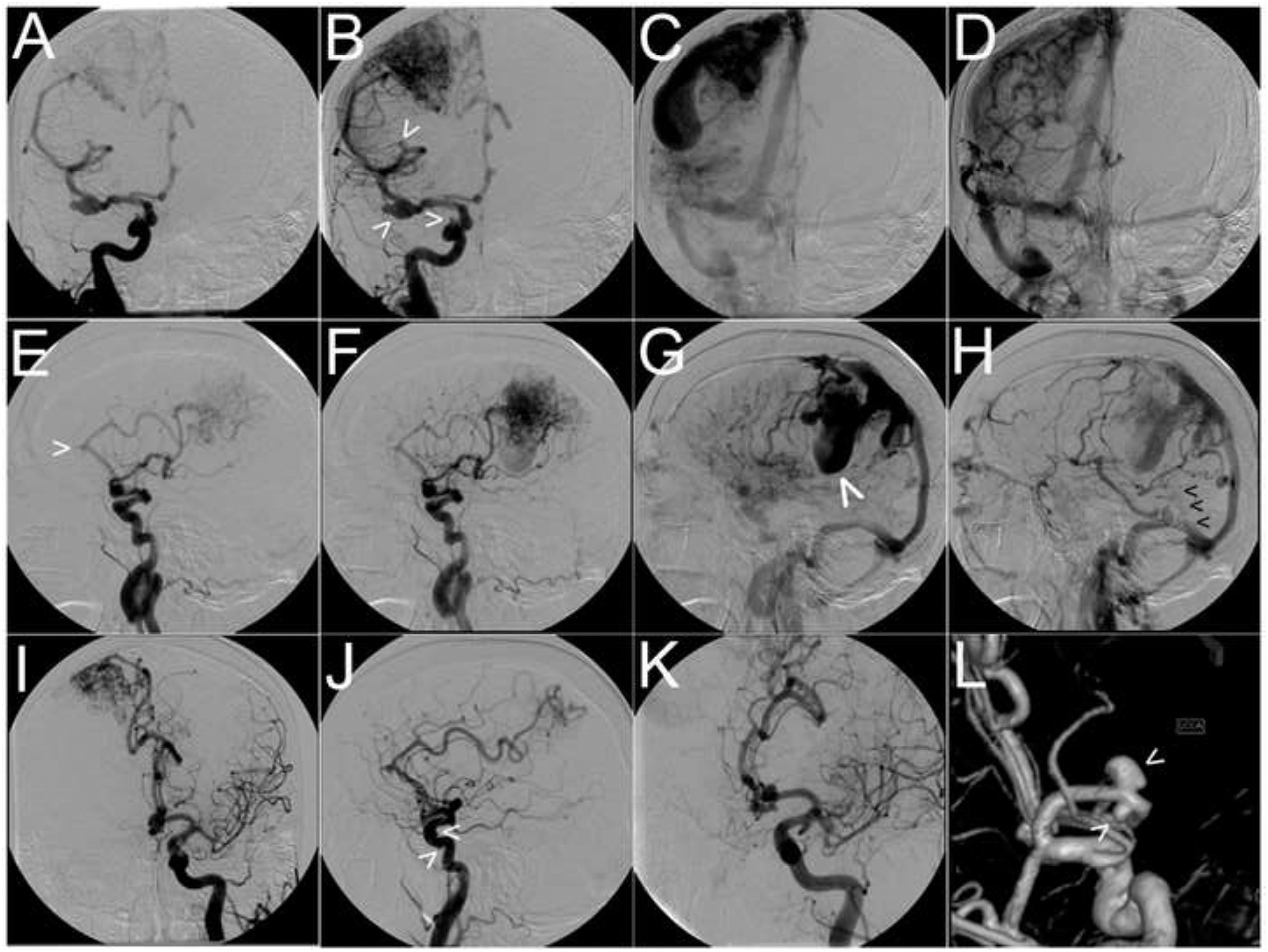
During the next 6 months, she developed progression of her headaches and left-sided weakness. Her case was discussed at a multi-disciplinary neurovascular conference and the group consensus was for staged endovascular embolization to reduce the AVM nidal volume for gamma knife radiosurgery.
Stage 1 of the embolization was performed using n-butyl cyanoacrylate glue to target the posterior feeding pedicles arising from the right pericallosal artery. This resulted in a 75% reduction of nidal volume supplied by the right ACA and 20% reduction in overall AVM nidal volume (Figure 4(A, B)).
Lateral views of the cerebral vasculature (early to mid arterial phase) following a right internal carotid artery contrast injection. Pre-procedural (A, C, E) and post-procedural (B, D, F) arteriograms are depicted for each stage of embolization to demonstrate the progressive decrease in the size of the AVM nidus.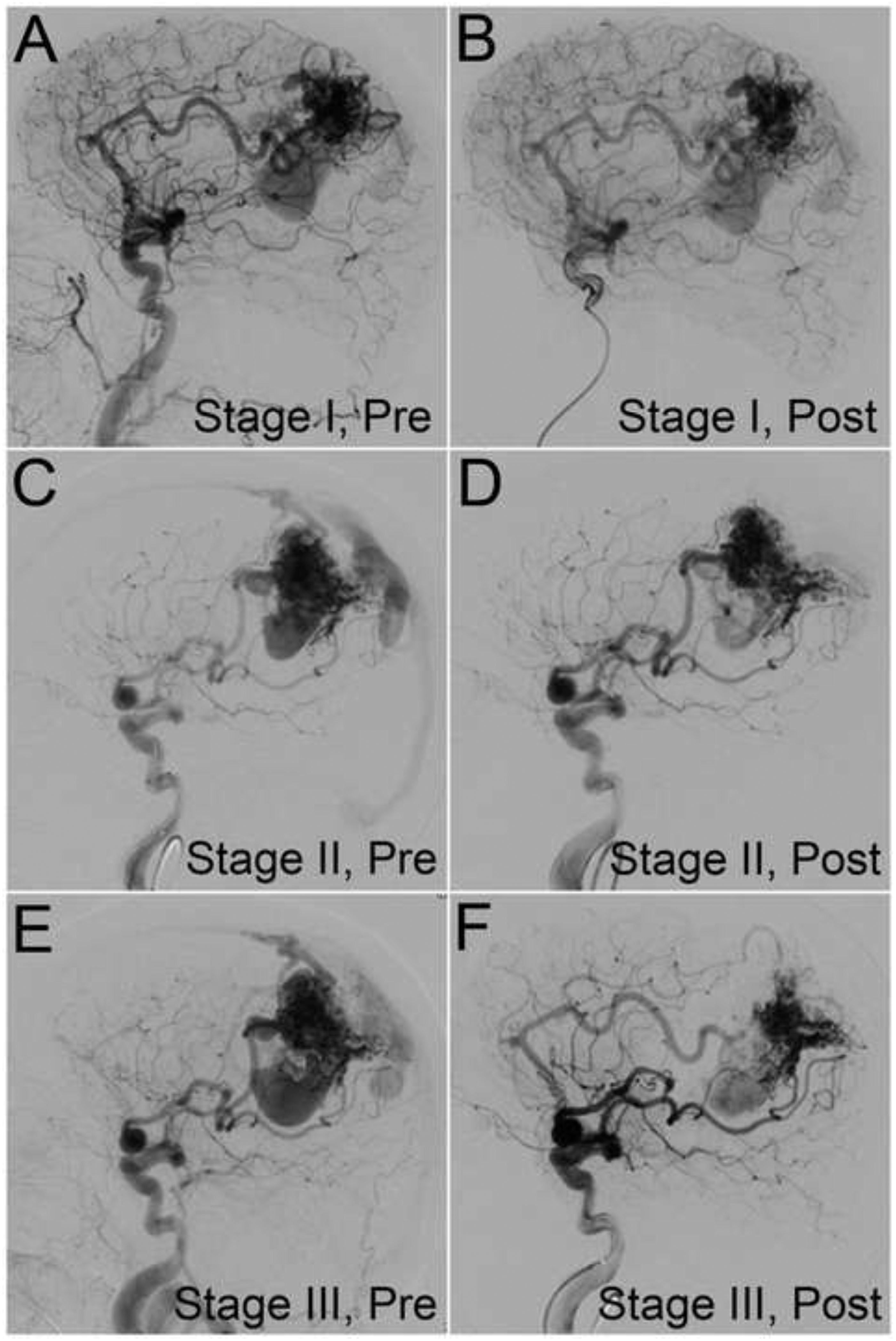
The patient’s left hemiparesis continued to progress due to worsening edema surrounding the AVM and partially thrombosed venous aneurysm. Three months later, she underwent stage 2 of the embolization, which consisted of Onyx embolization of the distal right MCA branches with elimination of a large venous fistula and reduction of some nidal volume (∼10%) at the inferior-most aspect (Figure 4(C, D)). Three months after the stage 2 embolization, she underwent a third embolization consisting of Onyx delivery to two distal right MCA branches, with a 30% further reduction in the AVM nidal volume (Figure 4(E, F)). Immediately following this procedure, the patient was extubated and at her neurological baseline.
Several hours after the procedure, she became acutely unresponsive and was noted to have a fixed, dilated right pupil. Re-intubation and mannitol therapy were performed. Head CT revealed a large right intraparenchymal hematoma in the sylvian fissure with significant mass effect and midline shift (Figure 5(A–C)). The epicenter of the hemorrhage was remote from the AVM nidus (Figure 5(D)). The source of the bleeding was presumed to be from the right MCA bifurcation feeding artery aneurysm.
Axial (A–C) and coronal (D) sections of a non-contrast head CT demonstrate a large intraparenchymal hemorrhage centered in the right sylvian fissure with significant mass effect and right-to-left midline shift. The epicenter of the hemorrhage (D) is well inferior to the AVM nidus.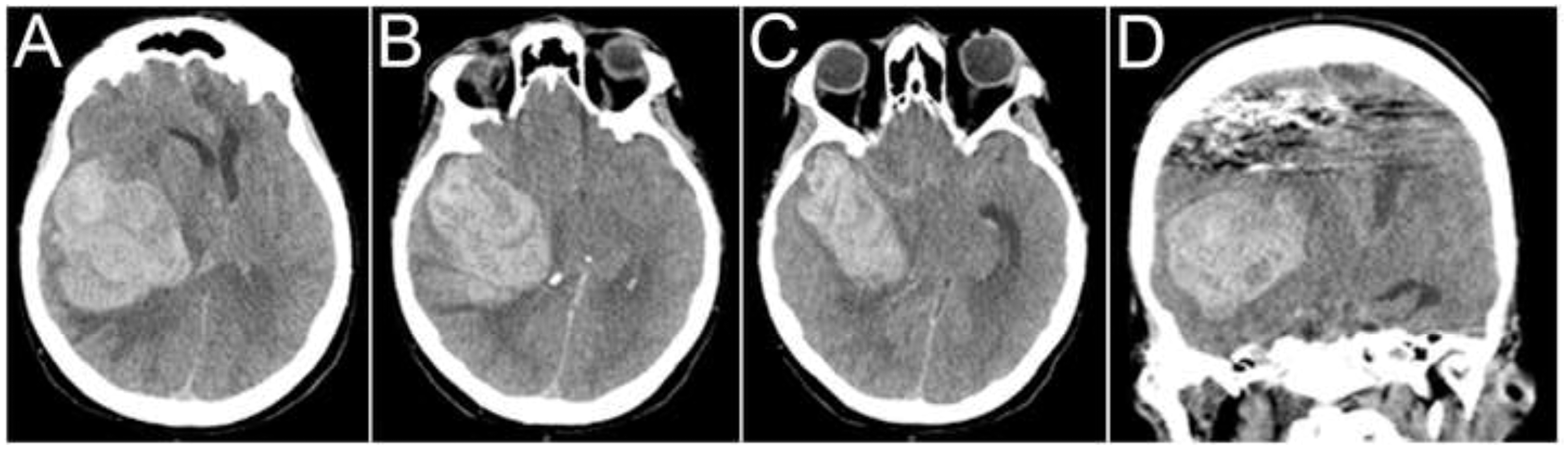
The patient was taken emergently to the operating room for a decompressive craniectomy, hematoma evacuation, and microsurgical clipping of the right MCA bifurcation aneurysm, which was confirmed intra-operatively to be the source of the hemorrhage. Shortly after treatment of the MCA aneurysm, however, brisk bleeding was observed from multiple deep portions of the AVM. Hemostasis was attempted, but was ultimately unsuccessful given the diffuse nature of the bleeding. The procedure was abandoned after packing of the surgical cavity and scalp closure. Given her persistent poor neurological status after this event, the family elected to withdraw care and she died.
Discussion
During surgical or endovascular obliteration of large AVMs, significant hemodynamic derangements can occur (with potentially devastating clinical consequences) due to the chronic loss of autoregulatory capacity in the arteries adjacent to the AVM, coupled with acute increases in arterial pressure upon AVM removal. 13 Adding a further degree of complexity to the treatment of these lesions, AVM-related feeding artery aneurysms are considered by some authorities to be a high-risk lesion for hemorrhage1,4 and should be promptly treated at the same time as, or preceding, treatment of the AVM.8,9 The precise hemodynamic impact of AVM obliteration—either partial or complete—on the natural history of feeding artery aneurysm rupture, however, remains enigmatic. 14
To the authors’ knowledge, there are few if any reports in the existing literature documenting acute rupture of a feeding artery aneurysm following a technically uncomplicated, staged embolization of a large AVM. Pollock and colleagues 15 reported on the management of a patient with a ruptured, de novo, intranidal aneurysm following staged embolization of a large right fronto-parietal parasagittal AVM. Similar to our case, the patient recovered well from the initial procedure, but the following morning rapidly progressed to obtundation with fixed and dilated pupils. The patient was managed successfully with cerebrospinal fluid diversion and endovascular embolization of the remaining pedicle feeding arteries (including the intranidal arterial aneurysm responsible for the bleeding). While other instances of acutely ruptured AVM-associated arterial aneurysms either during or following staged endovascular embolization have been reported,10,16–19 the preponderance of these cases was related to a recognized technical complication during the procedure.
Acute increases in AVM feeding artery perfusion pressure following treatment of large AVMs is well recognized as a potential precipitant for rupture of arterial aneurysms.20,21 In support of this, multiple lines of evidence have shown that elevated arterial perfusion pressure positively correlates with spontaneous AVM hemorrhage.22,23 Pressure measurements directly obtained via superselective catheter angiography in patients harboring AVMs show that arterial pressures are greater in the proximal feeding artery pedicles than in the more distal AVM nidus. 24 Moreover, using similar methodologies, other groups have demonstrated that feeding artery aneurysms are subjected to significantly higher pressures than the more distal AVM nidus and associated intranidal aneurysms following embolization.25–28
Certainly, given the complexity of this patient’s AVM (i.e., large, high-pressure, high-flow, with a partially thrombosed venous aneurysm and multiple, bilateral flow-related arterial aneurysms), the decision of which arterial feeding pedicle to embolize first was a topic of intense discussion prior to the initial stage of her embolization. While the precise pathobiology of AVM-associated arterial aneurysm rupture following embolization is unknown, it is likely that embolization of feeding pedicles not harboring flow-related arterial aneurysms may redirect flow—and, consequently, hemodynamic stress—toward those residual pedicles containing aneurysms. This situation could potentially lead to rupture of an AVM-associated arterial aneurysm. Given that our patient harbored numerous flow-related aneurysms (the largest being a 2 cm right MCA aneurysm and a 7 mm anterior communicating artery aneurysm), an argument could have been made to initially embolize either the ACA or MCA feeding pedicles. While we elected to embolize the distal anterior cerebral artery pedicle for the initial stage of the procedure, we cannot rule out the possibility that this intervention redirected flow into the right MCA feeding pedicle, thereby predisposing the large MCA aneurysm to rupture during a subsequent embolization.
Utilizing a quantitative computer model of the intracerebral circulation, Gao et al. 29 estimated the magnitude of changes in arterial perfusion pressure along the vascular tree during stepwise AVM obliteration. Interestingly, they observed that in large AVMs (flow = 1 L/min) the feeding artery pressures increased from 18 to 68 mmHg, and the percent occlusion at half-maximal pressure increase was 92%. For medium-sized AVMs (flow = 0.5 L/min), feeding artery pressures increased from 37 to 66 mm Hg, and the percent occlusion at half-maximal pressure increase was 71%. The authors concluded that scenarios in which the risk of feeding artery aneurysm rupture might be higher are (a) during the final stages of staged endovascular embolization; (b) in the presence of a small, residual AVM after surgery; and (c) during the final stages of stereotactic radiosurgery. 29
While the model proposed by Gao and colleagues 29 does have limitations, our patient’s clinical scenario would most closely resemble that of a large, high-flow AVM. As such, an increase in the feeding artery perfusion pressure of approximately 3.7 times the baseline value—as proposed by the authors—may well be sufficient to increase the transmural pressure gradient across a feeding artery aneurysm wall and facilitate rupture. Furthermore, our patient exhibited a large, partially thrombosed venous varix with significant surrounding vasogenic edema on her initial neuroimaging studies. It is known that partial venous outlet thrombosis is a common cause of vasogenic edema and progressive neurological deficit in patients with unruptured brain AVMs. 30 Given these findings, it is not unreasonable to assume that our patient exhibited higher baseline feeding artery perfusion pressures and that the calculations proposed by Gao et al. 29 may well be an underestimate of the actual arterial pressure changes following embolization.
Conclusions
We believe that in the present case an abrupt increase in pressure in the MCA following transarterial embolization of a large brain AVM led to a fatal rupture of a large MCA aneurysm. Strong consideration should be given to treating such aneurysms before, or during, the first stage of transarterial embolization to prevent this type of complication.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.