
Abstract
Background
Endovascular coil embolization of pial arteriovenous fistulas (AVF) has been reported as an effective treatment. However, venous thrombosis and intracranial hemorrhage developing after endovascular occlusion of a pial AVF have not been adequately reported.
Case description
A 37-year-old man presented with left middle cerebral artery (MCA) AVF and right posterior cerebral artery (PCA) AVF with giant venous pouches. Staged endovascular coil embolization was performed. The MCA AVF was completely occluded by coils at the first stage. Intravenous heparin (3000 IU) was administered during the procedure, and then low molecular weight heparin (subcutaneous injection, 0.4 mL/12 hours) was administered for two days. The PCA AVF was near completely occluded by coils without anticoagulation therapy at the second stage. Rapid progressive venous thrombosis and intracranial hemorrhage were confirmed by computerized tomography brain scan postoperatively, and the patient was then transferred to the neurological intensive care unit for further treatment. Finally, the patient recovered well at the five-month follow-up.
Conclusions
Endovascular occlusion of a high-flow pial AVF with a giant venous pouch resulting in significant blood stasis could precipitate thrombosis in the venous system. Further studies are required to establish whether anticoagulation therapy is necessary.
Introduction
A pial arteriovenous fistula (AVF) is a direct communication between the pial or cortical artery with the cortical or deep vein without an intervening nidus, and accounts for 1.6% of all intracranial vascular malformations. 1 Pial AVFs can cause hemorrhage and neurologic deficits secondary to local venous congestion, brain edema, or ischemia. Most require some kind of intervention.2,3 Microsurgery, endovascular treatment, and multidisciplinary approaches are the main treatment options for pial AVFs.2,4 Endovascular coil embolization has been reported to be an effective treatment for pial AVFs.5–11 However, venous thrombosis and intracranial hemorrhage developing after endovascular occlusion of pial AVFs are rare but devastating complications that have not been adequately reported.
Case report
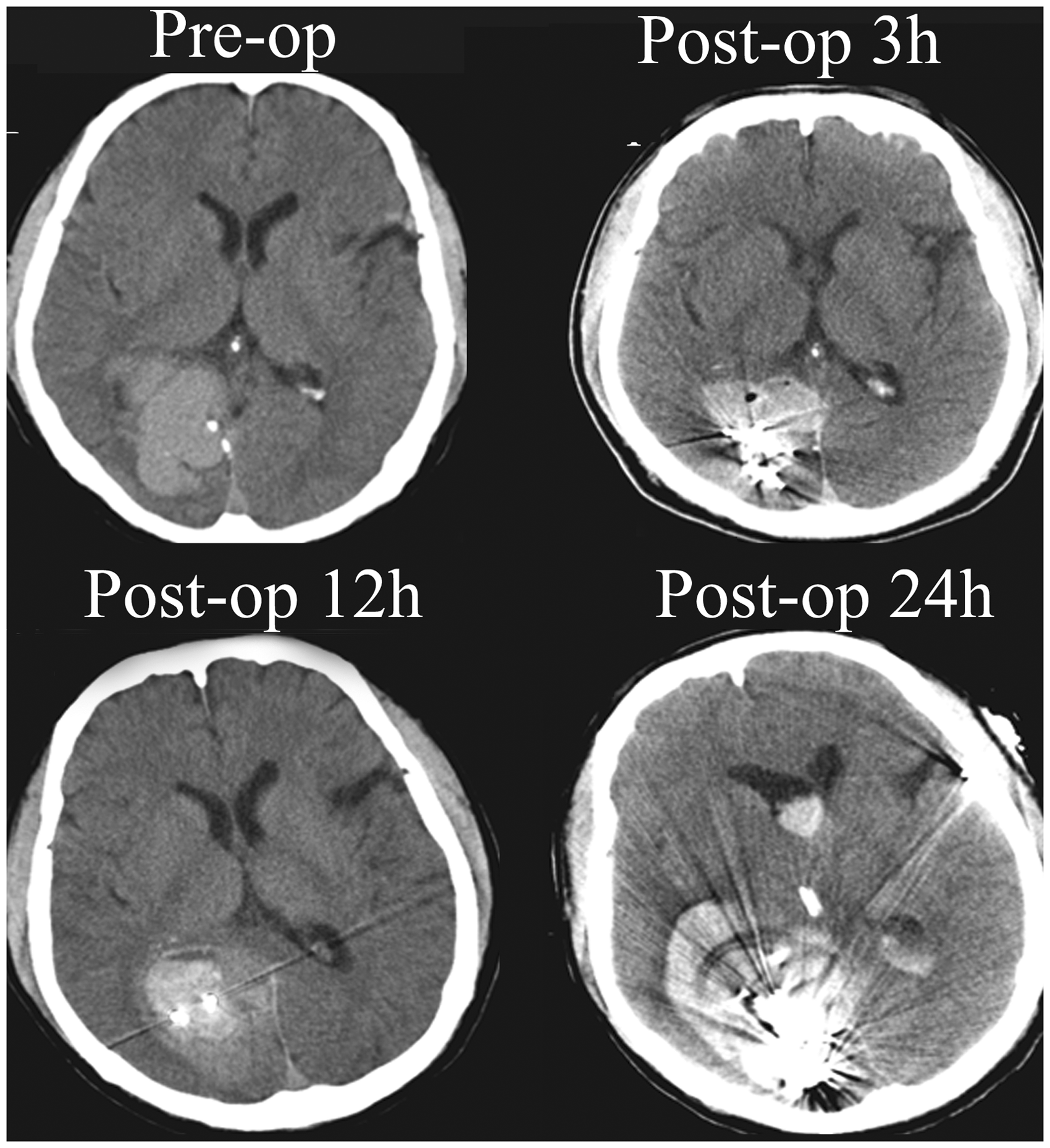
A 37-year-old right-handed man presented to our institution suffering with seizures for four months. His cognitive function had decreased, but other neurological examinations were intact. Family and clinical history of vasculopathy (hemorrhagic hereditary telangiectasia disorder) were negative. Laboratory analysis for coagulation was normal. Digital subtraction angiography (DSA) showed two high-flow pial AVFs with giant venous pouches. One pial AVF (Figure 1) was located in the left frontal motor area supplied by the left middle cerebral artery (MCA). Venous drainage was predominantly superficial into the superior sagittal sinus through cortical veins, the Trolard vein, and other cortical veins that used the same venous outlet (Figure 1). The other pial AVF (Figure 2) was located in the right occipital lobe supplied by the right posterior cerebral artery (PCA). Venous drainage was predominantly superficial into the right transverse sinus through cortical veins, and no cortical veins connecting the venous outlet were identified (Figure 2). Staged endovascular coil embolization was performed. First, the left MCA AVF was completely occluded (Figure 1) and treated with loose packing of the giant venous pouch using big and long coils (eV3, Irvine, CA) followed by tight packing of the fistulous portion with small coils (eV3). The patient’s blood pressure (120–100/80–60 mmHg) was controlled at approximately 80% of the basal blood pressure for three days after the procedure. Intravenous heparin (3000 IU) was administered during the procedure, and then low molecular weight heparin (subcutaneous injection, 0.4 mL/12 hours) was administered for two days. The patient was discharged uneventfully. Three months later, the right PCA AVF was treated with coils. The treatment strategy and materials used were the same as for the first embolization, and finally the PCA AVF was nearly completely occluded (Figure 2). Anticoagulation therapy was not administered due to incomplete occlusion, and no other normal veins were using the same venous outlet (Figure 2). However, the patient’s blood pressure was controlled (120–100/80–60 mmHg). The patient had a headache, and a computerized tomography (CT) brain scan was performed at 3, 12, and 24 hours postoperatively. The scan showed progressive venous thrombosis and intracranial hemorrhage (Figure 3). The patient was then transferred to the neurological intensive care unit, and underwent external ventricle drainage with intracranial pressure monitoring. The patient was back to baseline at the five-month follow-up after the second treatment. A follow-up CT brain scan showed no evidence of intracranial hemorrhage, and DSA showed complete occlusion of the two pial AVFs (Figures 1 and 2).
Pre- and postoperative cerebral angiogram of the left MCA AVF. Arrows show where normal cortical veins use the same venous outlet. AVF, arteriovenous fistula; MCA, middle cerebral artery. Pre- and postoperative cerebral angiogram of the right PCA AVF. PCA, posterior cerebral artery. Pre- and postoperative computed tomography (CT) brain scans of the right PCA AVF.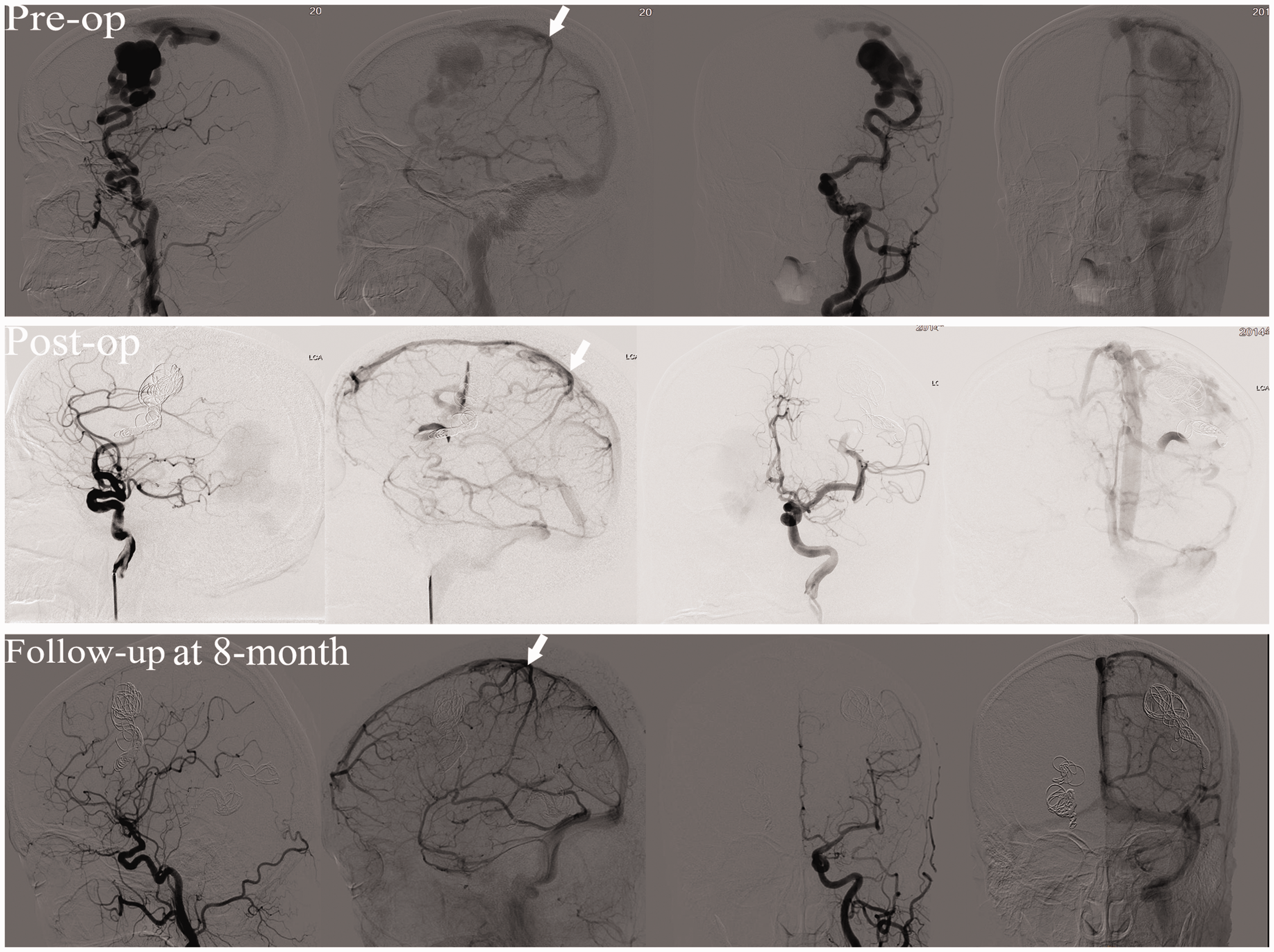

Discussion
Simple disconnection of pial AVFs is considered enough in most cases, by either microsurgery or endovascular embolization. 2 We selected endovascular coil embolization rather than microsurgery for the following reasons. First, microsurgery can carry an increased risk of neurologic morbidity. Second, the MCA AVF is located in the cerebral motor area, and the PCA AVF is relatively deep, with the fistulous portion accessible beyond the giant venous pouch. Moreover, several embolic materials such as coils, balloons, onyx, and glue can be used to disconnect the AVFs.5–11 Detachable coils have some advantages with regard to the embolization of high-flow pial AVFs because they are controllable before detachment, and migration of embolic materials to the distal draining vein can be prevented.
Venous thrombosis is a challenging complication after endovascular occlusion of pial AVFs. Complete occlusion may produce extensive thrombosis of the draining veins, causing venous infarction or hemorrhage. 7 However, very few cases of venous thrombosis have been reported after treatment of pial AVFs. Lv et al. 7 reported three cases of venous thrombosis after endovascular occlusion of pial AVFs without anticoagulation therapy. The outcomes were that one patient presented with seizures, one with blindness, and another with Parinaud syndrome and right hemiplegia. At the six-month follow-up, the last patient was back at baseline. Gonzalez et al. 12 reported one case of rapid progressive venous thrombosis after surgically clipping a high-flow pial AVF without anticoagulation therapy 24 hours later. Although acute surgical management was performed, the patient died 72 hours later. Yang et al. 13 reported a case of insidious onset of peri-lesional edema formation after abrupt disconnection of pial AVF shunting using surgical arterial ligation. The patient received antiplatelet and anticoagulation therapy and recovered well. They concluded that antiplatelet and/or anticoagulation agents seem to be necessary in the case of abrupt disconnection of single- or dual-channel pial AVF to prevent postoperative venous thrombosis. In our case, anticoagulation therapy was not administered after taking into consideration the incomplete occlusion, the fact that no other normal vein was using the same venous outlet, and the bleeding at 12 hours after surgery. The blood stasis due to near-complete occlusion may be a trigger for venous thrombosis, and coils in the venous pouch as a scaffold may accelerate the course. Both complete and incomplete (near complete) occlusions may lead to venous thrombosis. Therefore, the clinical option is not clear. Close clinical and imaging follow-up is warranted in these patients. The state of hypercoagulation should also be examined preoperatively.14,15 Therapeutic anticoagulation for 2–15 days may be a strategy for preventing venous infarction or hemorrhage in patients who present with headaches after embolization.3,7,12,13,16 Staged procedures to occlude pial AVFs are necessary for high-flow shunting, 17 and multimodal treatment strategies for complex pial AVFs should be considered. 4
Conclusions
Endovascular occlusion of a high-flow pial AVF with a giant venous pouch resulting in significant blood stasis could precipitate thrombosis in the venous system. Further studies are needed to establish whether anticoagulation therapy is necessary.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the National Natural Science Foundation (grant numbers 81441038 and 81371314).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.